BIO 225 Exam 3
1/292
Earn XP
Description and Tags
Exam 3, Duan, W26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
293 Terms
Four Questions to Always Think About With Hormones
What are they?
Where and how are they made?
What do they do?
How do they work mechanistically?
Endocrine disorders with growth hormone
Can cause dwarfism or giantism
Some families have a recessive gene for growth hormone receptor malfunction and their children can be homozygous recessive and have growth defects.
Hormone Regulation Quick Rule
Too much or too little of any hormone is not good for our bodies, we manage a tight ship when it comes to hormones because any imbalance can cause severe damage.
There are hormones in our body that regulate every process from nutrient usage and storage, to growth, to maternal behaviors, etc. They affect our behavior and physiology.
Classical Definition of Hormones
Chemical Substances produced by specialized organs called endocrine glands and transported through the bloodstream to other tissues where they act to elicit a specific physiological response.
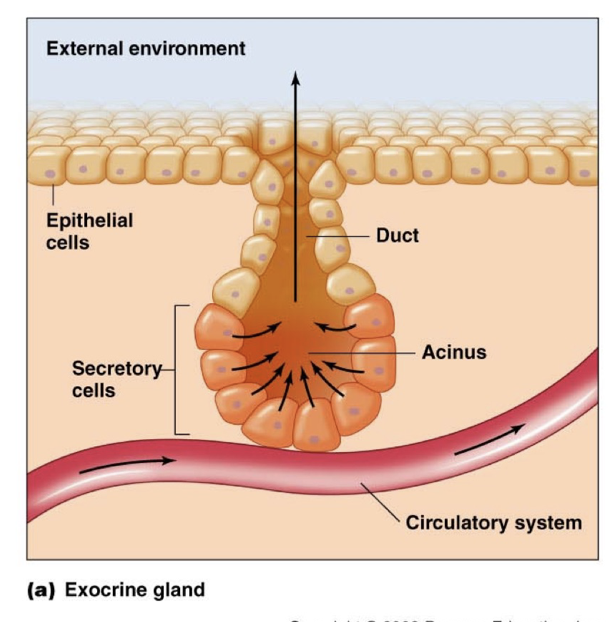
Exocrine Glands
Release their chemicals to the external environment
Have ducts to pass material to surface
Poorly Vascularized
Exocrine Glands Examples
Salivary
Mammary
Mucosal
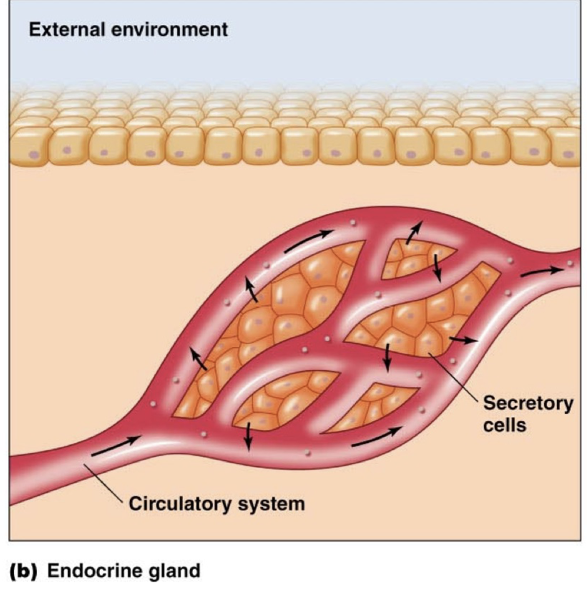
Endocrine Glands
Secrete Chemicals to Internal Environment
Usually secrete hormones into the blood stream
No Ducts
Highly Vascularized
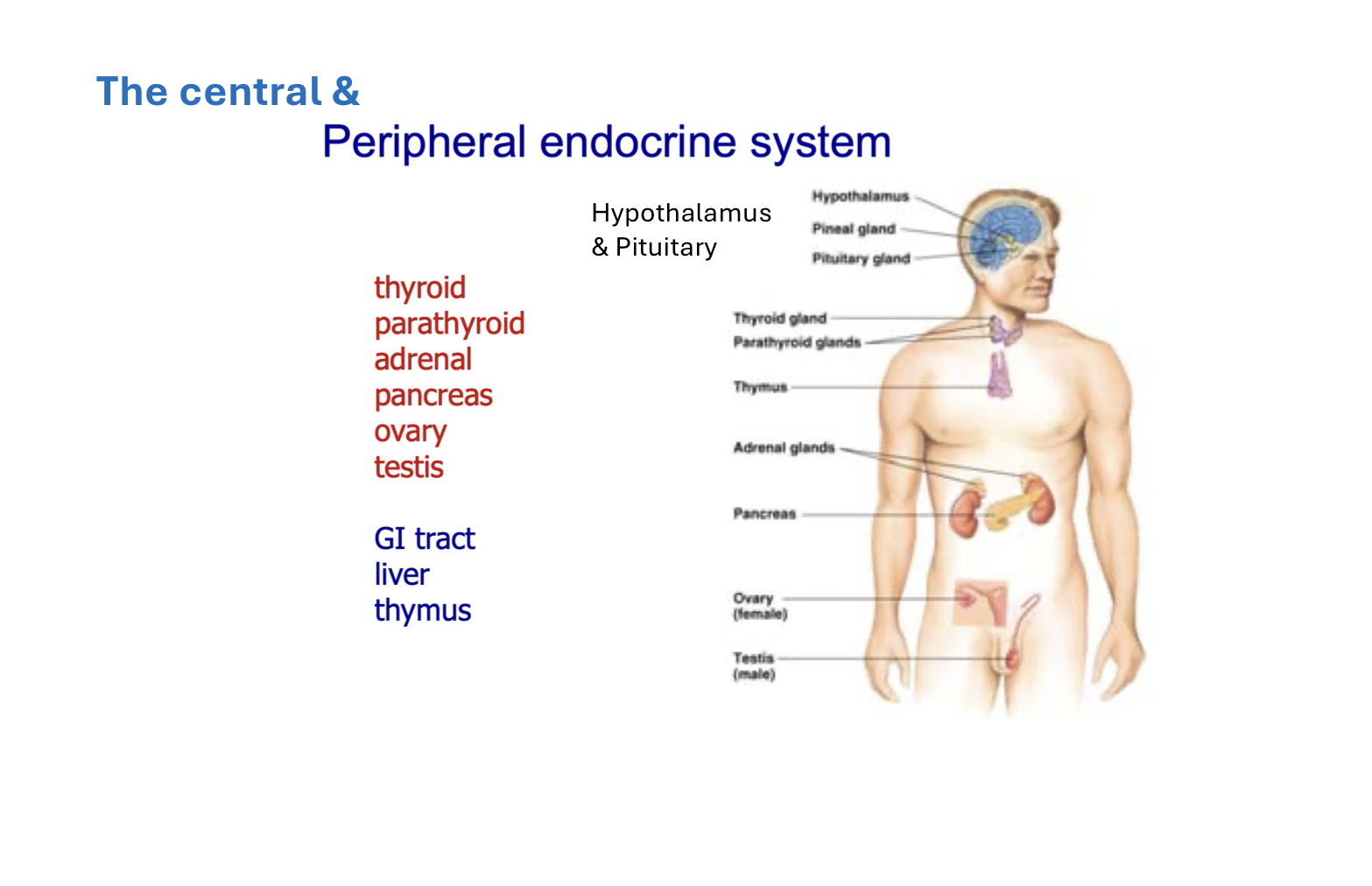
Major Endocrine Glands
Pineal
Hypothalamus
Pituitary
Thyroid
Parathyroid
Adrenal
Pancreas
Ovaries
Tested
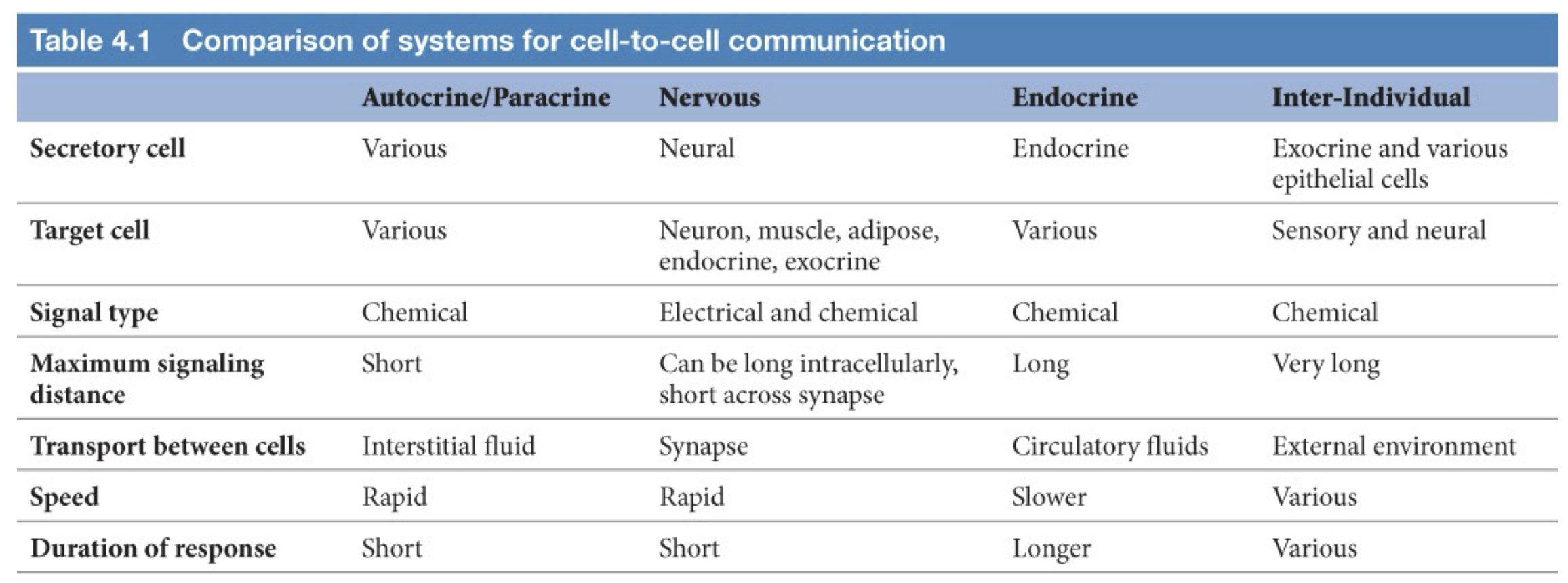
Types of Cell Signaling
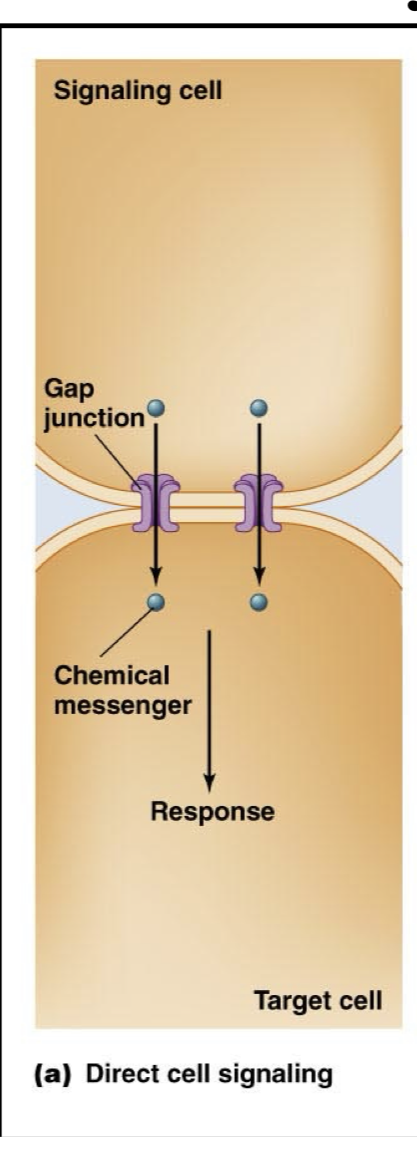
Direct Cell Signaling (General Definition)
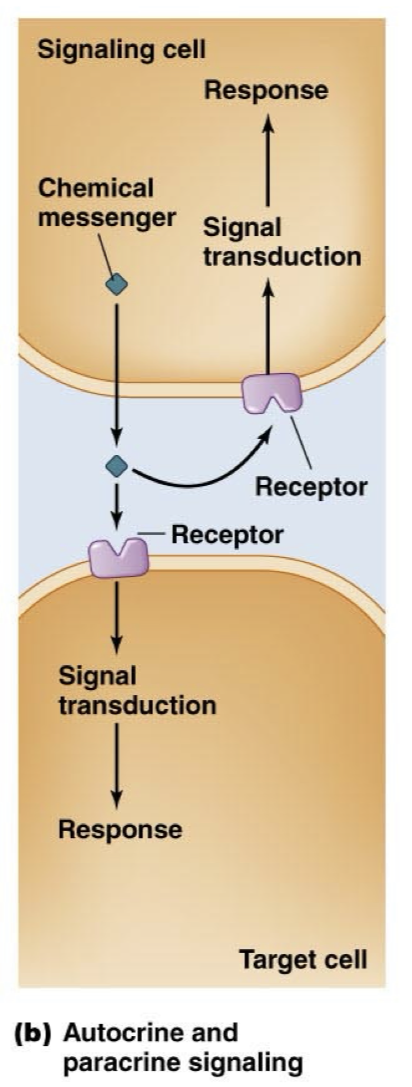
Autocrine and Paracrine Signaling (General Definition)
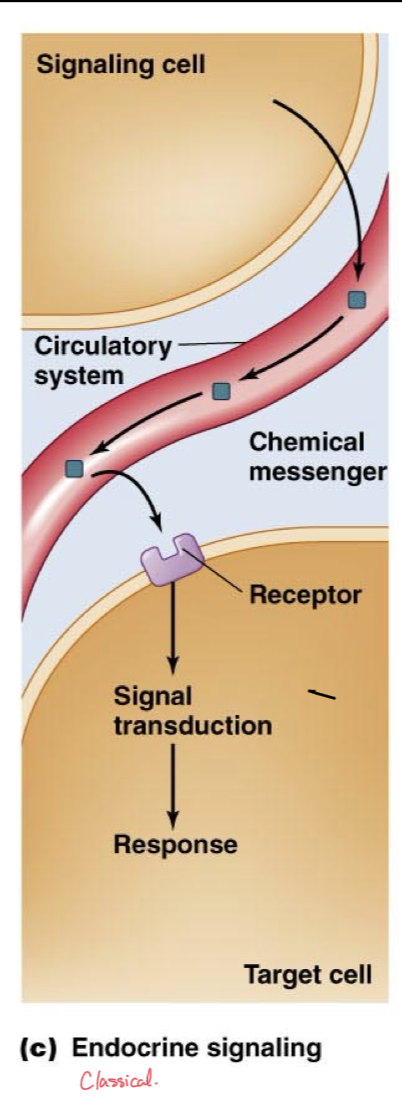
Endocrine Signaling (Classical Definition)
Neural Signaling (General Definition)
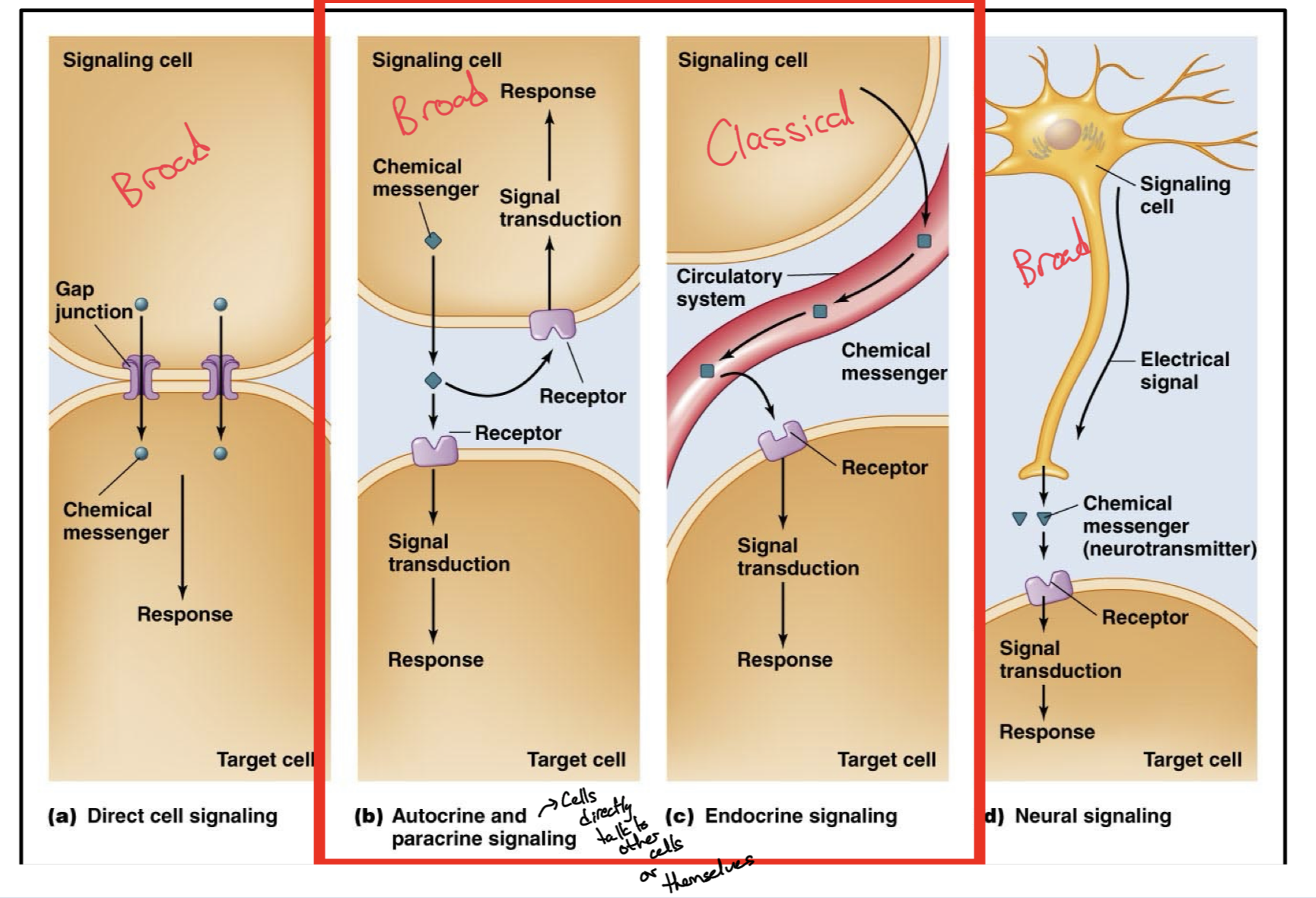
Direct Cell Signaling
Two cells connected through gap junctions to rapidly and directly pass chemical messengers to each other, no need to pass messenger through extracellular space.
Autocrine/Paracrine Signaling
Releasing a chemical messenger into the extracellular fluid to bind/target a nearby cell or the same cell which released the messenger.
Causes signal transduction and response in the neighboring cell or in itself, but not through a direct connection, still travels through the extracellular fluid.
Endocrine Signaling
More classical version of chemical signaling with hormones
Chemical messenger is released by one cell to affect a target cell at a far distance, with the messenger using the circulatory system as a freeway to reach its target
Chemical messenger then leaves the bloodstream and binds to the target cell.
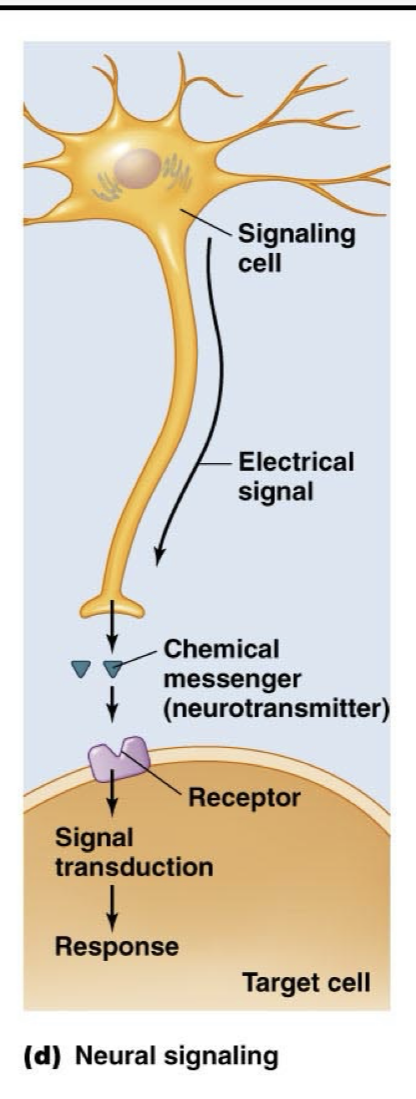
Neural Signaling
A more unorthodox way of thinking about endocrine system and hormones, but still counts
Neuron carries an action potential after being triggered by an integrating center or sensory neuron and at its synapse, it releases neurotransmitters to either affect another neuron or a cell, depending on the target cell and which chemical messenger is used.
Limitations of Classical Definition
Not all substances that have hormonal activity are produced from specialized tissues
Many Hormones have multiple sources
Some hormones act locally without releasing into circulation
Broader Definition of Hormones
Hormones are chemical substances released by one cell to act on another cell. They are not nutrients and are usually effective in very low concentrations.
Six Classes of Chemical Messenger (3 to focus on)
Peptides
Steroids
Amines
Lipids
Purines
Gases
How does structure of chemical messenger affect signaling?
Structure of the chemical messenger being used, especially whether it is hydrophobic or hydrophilic affects the signaling mechanism, how and when it is produced, and how it is transported.
Hormone Subdivision
Hormones can be divided into either being hydrophobic or hydrophillic and this leads to changes in function.
Hydrophobic Hormones
Synthesized on demand or else would diffuse whenever
Diffuse easily across the membrane
Can travel short distances by dissolving, otherwise need a carrier in the blood
Can bind to intracellular or transmembrane receptors, slow or rapid effects.
Hydrophilic Hormones
Stored inside the cells in vesicles,
Secreted via exocytosis from their vesicles,
Can easily dissolve and transport through extracellular fluids, especially blood because they are polar.
Rapid effects.
Peptide/Protein Hormones
Hydrophilic: Can easily dissolve in bloodstream, soluble in aqueous solutions, target to target cell dissolved in extracellular fluid.
Bind to transmembrane receptors, cannot pass through cell membranes to bind intracellularly.
Rapids Effects on Target Cell
3-200 Amino Acids Long
Synthesized on the Rough ER, as larger preprohormones
Later cleaved and stored in vesicles as prohormones
Cleaved once more and secreted by exocytosis as active hormones.
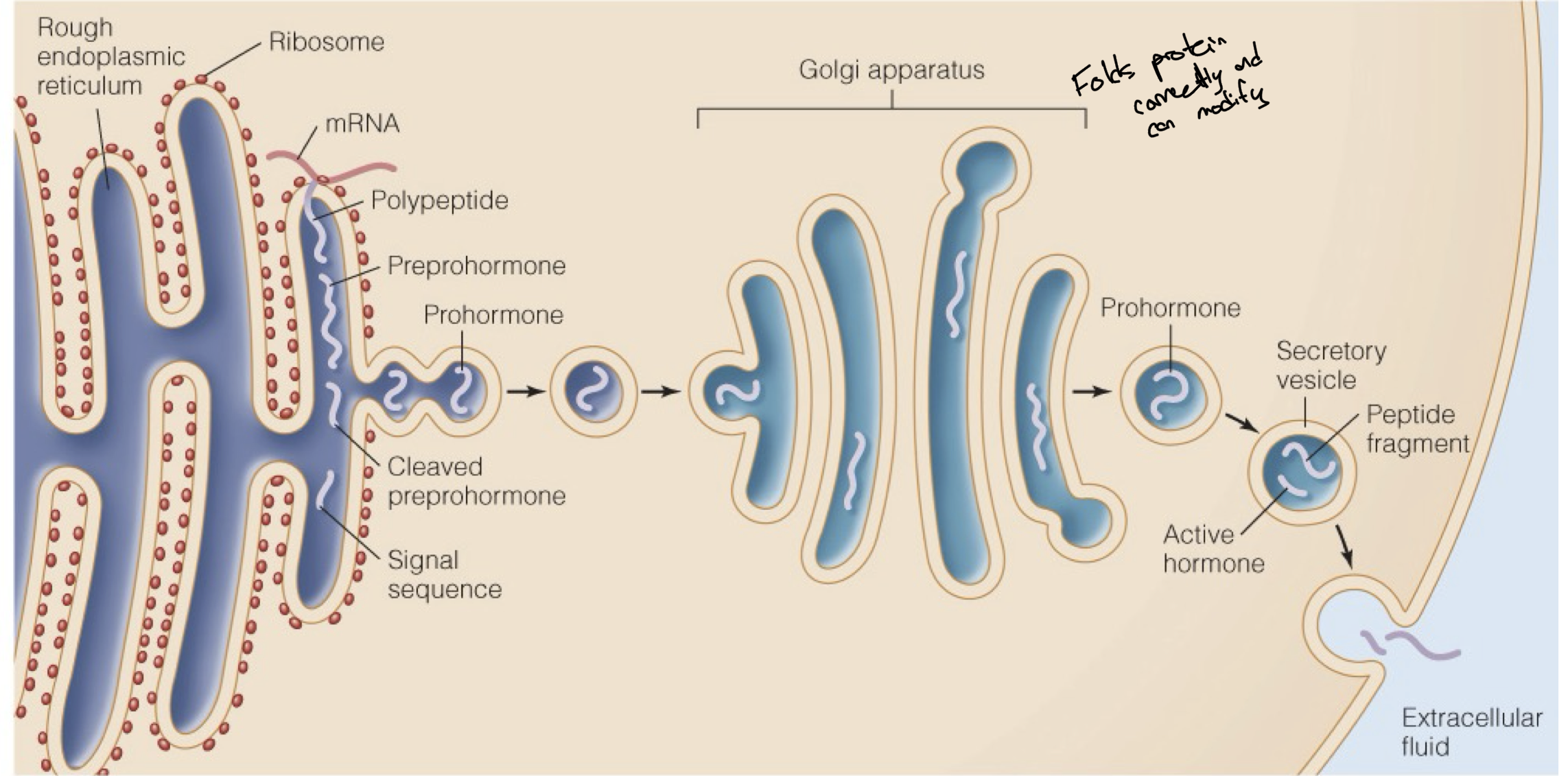
Peptide Hormone Production/Transformation
Peptide hormones are produced in the rough endoplasmic reticulum
Then they are cleaved from preprohormones into prohormones when they are packaged into vesicles.
Then the golgi apparatus takes the proteins in these vesicles and properly folds them into their functional structure.
Before being released from the cytoplasm, the prohormones are cleaved once more into the active peptide hormone and then released via exocytosis.
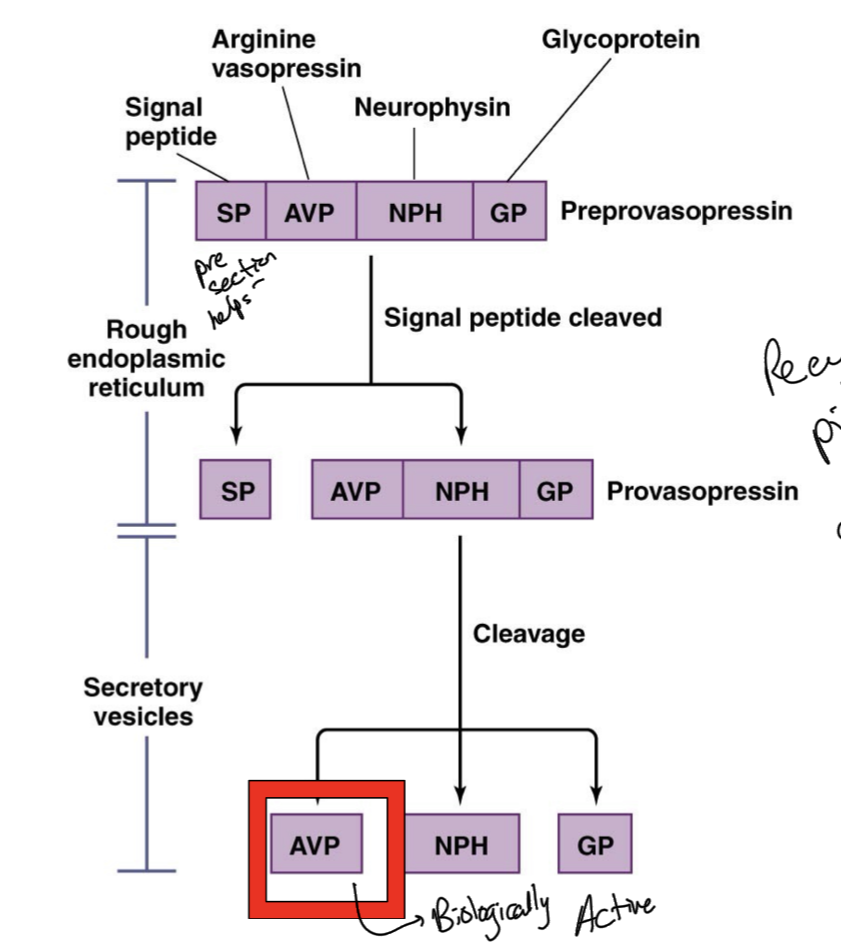
Synthesis and Secretion of AVP
AVP is arginine vasopressin hormone
As a preprohormone, it holds a signal peptide chain and other pieces to help its transport and proper functioning.
Signal peptide chain tells us where the hormone should go, like an ID tag.
In the Rough ER, the signal peptide is cleaved from the protein
Once these prohormones are packaged into vesicles, it is once again cleaved and only the active from of the protein is left, while the other cleaved pieces are reused when more of this hormone is produced.
Amine Hormones
Chemicals that posses an Amine Group (-NH2)
Examples are catecholamines (dopamine, NE, E) serotonin, melatonin, histamine, and thyroid hormones.
Also known as biogenic amines
Some are “true” endocrine hormones while others are neurotransmitters, and some can work as both.
Most are hydrophillic, with one of the most notable exceptions being thyroid hormones which are hydrophobic.
Diverse Effercts.
Steroid Hormones
Derived from cholesterol
Synthesized by the smooth ER or mitochondria
Synthesized on Demand
3 Major Classes: Mineralocorticoids, glucocorticoids, and reproductive hormones
Hydrophobic, can diffuse through plasma membrane so cannot be just stored in cell
Transported to target cells via carrier proteins like albumin
Can bind to intracellular or transmembrane receptors
SLOW effects on target (like gene transcription) but cortisol has rapid, non-genomic effects.
Mineralocorticoids
Electrolyte Balance, Control our water-ion balance
Glucocorticoids
Mainly Stress hormones like cortisol
Control our stress response
Reproductive Hormones
Testosterone, Estrogen, Etc.
Regulate seggs-specific characteristics, male and female characteristics.
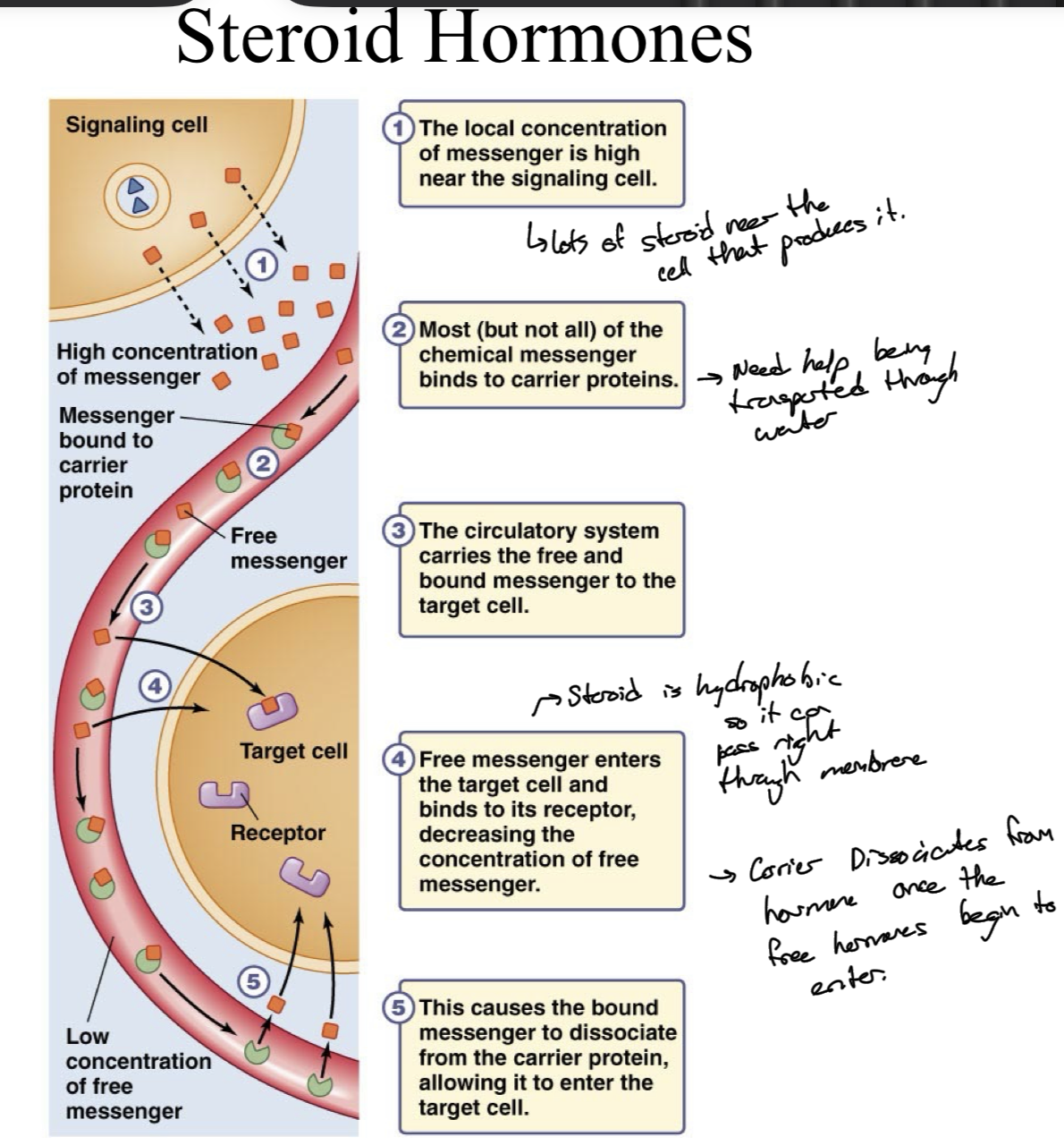
Steroids being carried to Target Cell
Messenger concentrations are high near the signaling cell
Most but not all of the messenger binds to carrier proteins
Circulatory system carries the free and bound messengers to the target cell, and free messengers leave the blood stream to the target, this decrease in unbound messenger causes some of the bound messengers to unbind, increasing release to the target cell in a cascade.
Receptors on Target Cell
Hydrophilic Messengers bind to transmembrane receptors, because they cannot just cross the membrane, so settle for the cell surface.
Hydrophobic messengers bind to intracellular receptors, can caross the membrane of cells, fat soluble.
Ligand
Chemical messenger that can bind to a specific receptor
Receptor Changes shape when ligand binds
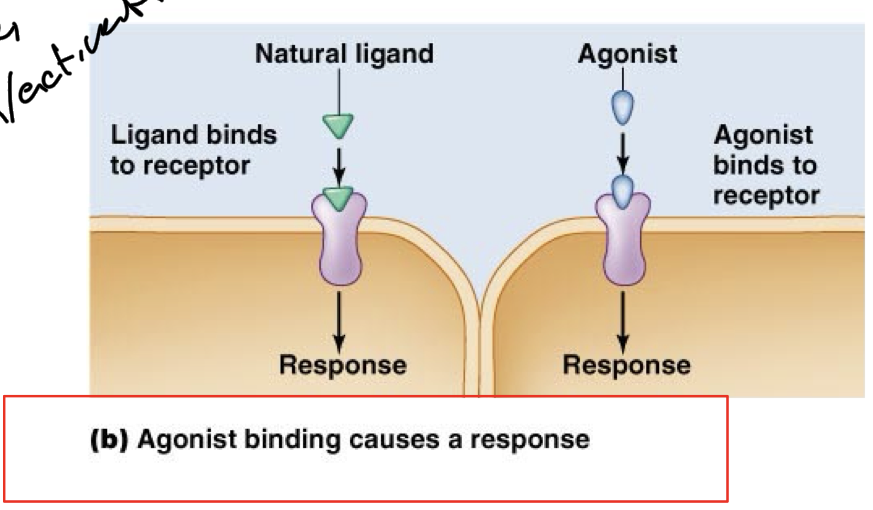
Agonist
Compound that can bind to the same receptor as the natural messenger/hormone and activates/triggers the same functions.
Mimics natural effects.
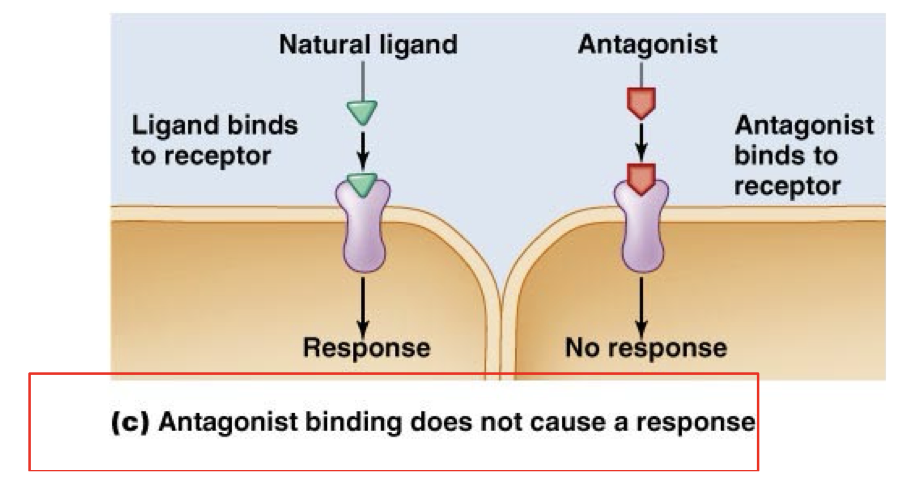
Antagonist
Binds to the same receptor as the natural hormone but blocks any response from happening.
Prevents the natural response.
Ligand-Receptor Specificity
Ligands can activiate different types of receptors but each receptor will only respond to one type of ligand
This specific interaction is what helps trigger specific responses.
Only cell tissues that express the correct receptors will respond to different hormones.
Hormones and receptors have particular shapes like puzzle pieces, fit together.
Law of Mass Action
Formation of the Ligand-Receptor complex causes the response.
Receptors and ligands meet by chance. When there is more of either a ligand or receptor or both, there is a stronger response, more complexes.
If you only increase the ligands, there will be a stronger response until all of the receptors are bound/saturated, and the response is maximal.
Saturation is an important point in the law of mass action, you can increase response by increasing ligand until a certain point when all receptors are bound. Even increasing receptors, they can all be saturated eventually.
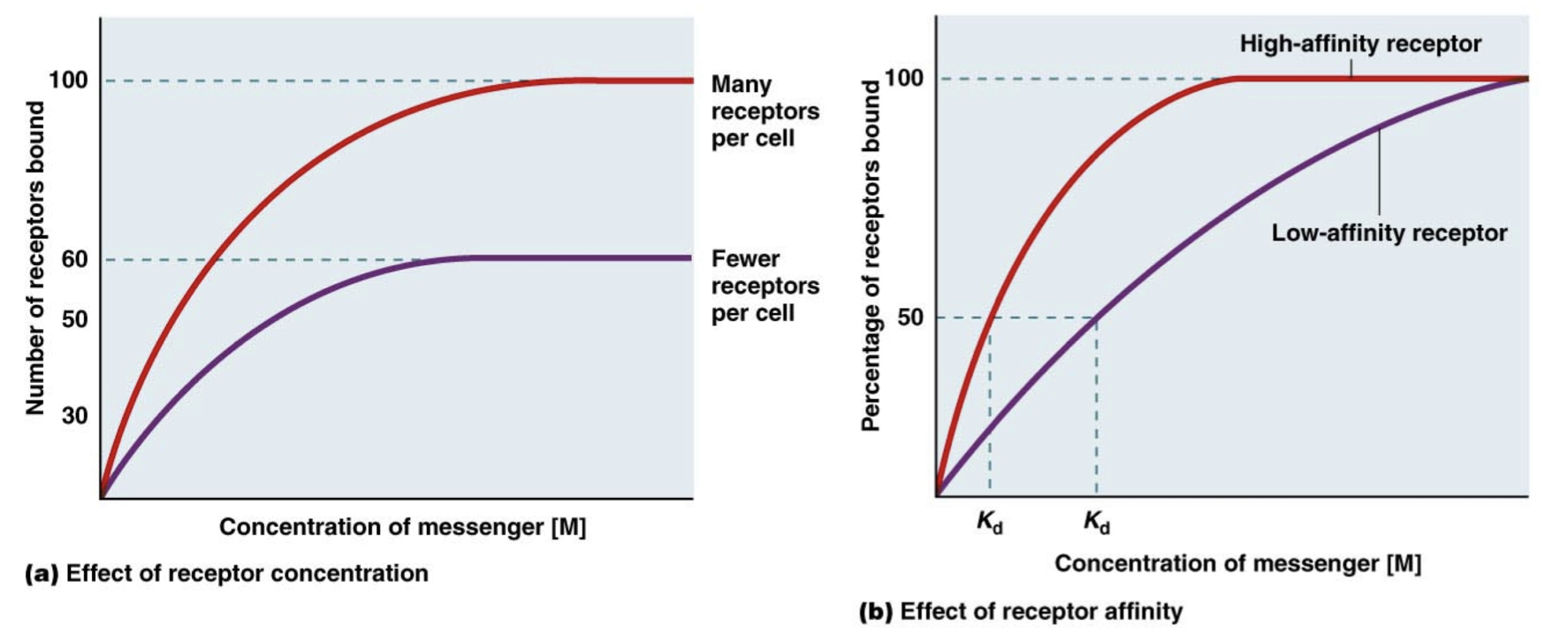
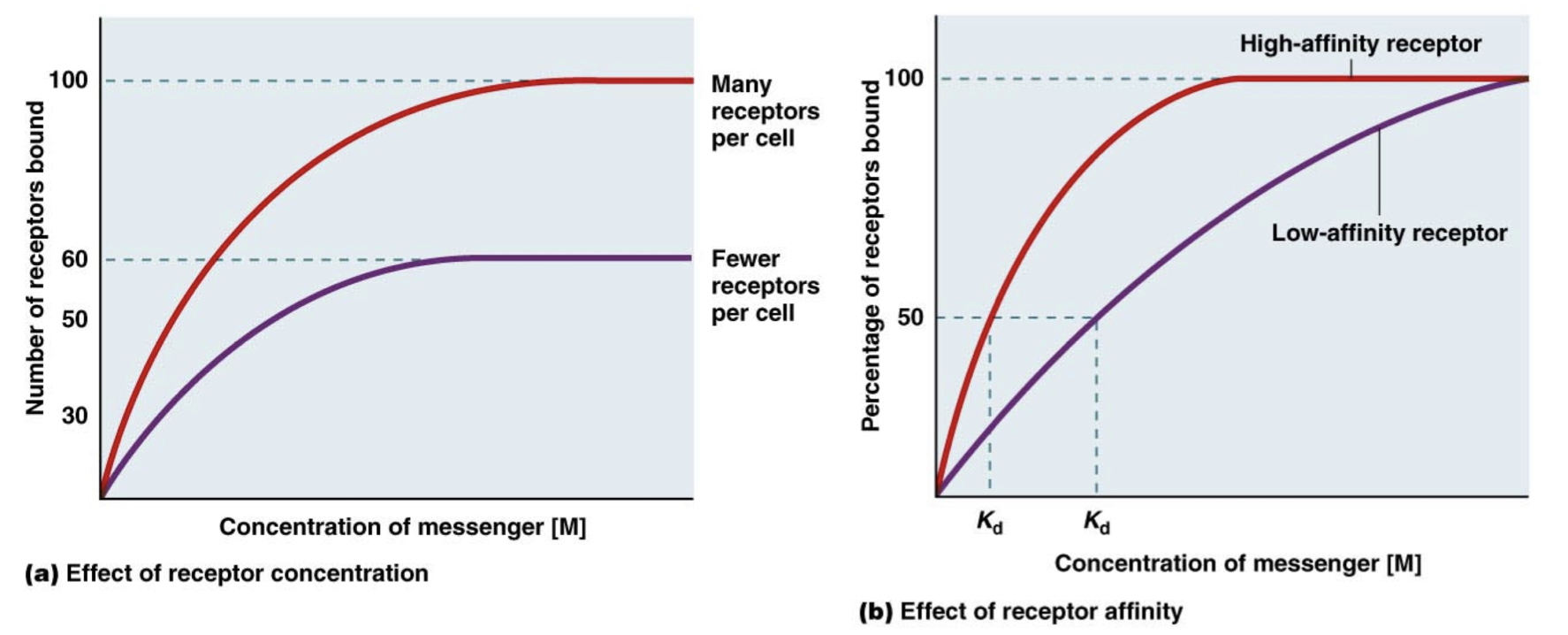
Receptor Affinity
Kd is the messenger concentration required to get half of the receptor population responding/bound/active.
A lower Kd indicates that these receptor populations have a higher affinity for the messenger because it takes less messenger to get to the 50% response.
Different cells can respond to the same hormone but have different affinity receptors for that hormone or have different numbers of receptors, causing a difference in response.
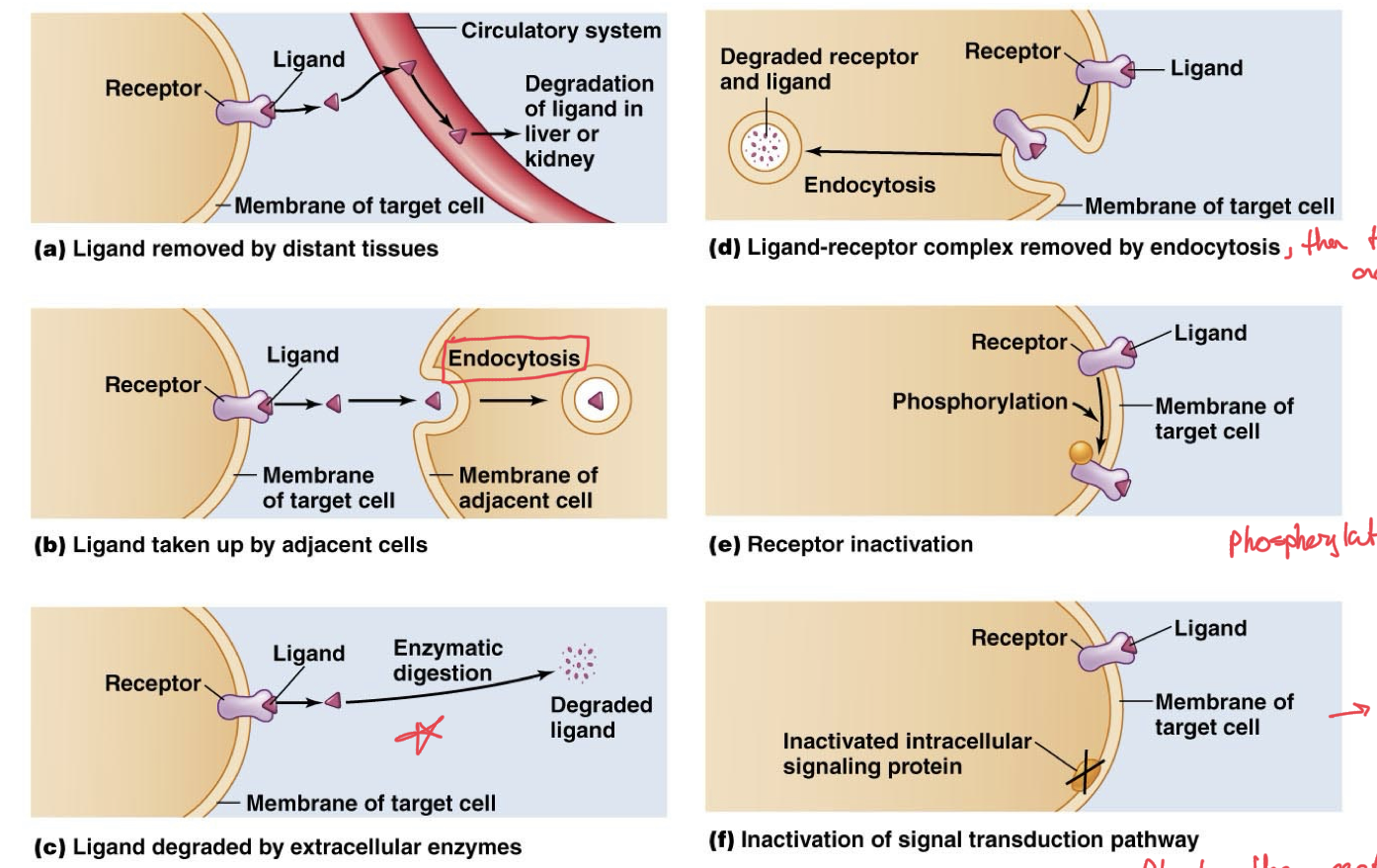
Inactivation of Ligand Receptor Complex
We need deactivation of these complexes, cannot be constantly activated, their on/off function is what makes them effective.
Ligand can be removed by distance tissues like liver or kidney through circulatory system
Ligand can be taken up by adjacent cells, inactivating the current cell receptors being activated by that ligand
Ligand can also be degraded by extracellular enzymes, like acetylcholinesterase
Ligand-receptor complex can be absorbed entirely by the cell via endocytosis, so no more ligand triggering it and then degrades it in the cell.
Receptors can be deactivated, for example by simply phosphorylating to inactivate them, make them dormant.
Inactivation of the signal transduction pathway altogether, so that even when ligand is bound to receptor, the signal cannot go any further than that.
Ligand Promiscuity
A ligand may bind to more than one receptor
There are many receptor isoforms, which are NOT the same receptor, respond through entirely different pathways for different effects.
Different receptors for the same ligand expressed on different target cells, causing different responses to the same ligand.
A single cell may have receptors for many different ligands, allowing very diverse effects under different conditions.
IGF1R and IGF2R receptors are a good example, function very differently but they share the same hormone, IGF-2.
Receptor Subdivisions
Receptors can be broken down into two types based on their location, either transmembrane or intracellular.
Most are transmembrane, such as ligand-gated ion channels, receptor-enzyme receptors, and g-protein couples receptors.
Transmembrane receptors usually bind the water-soluble ligands
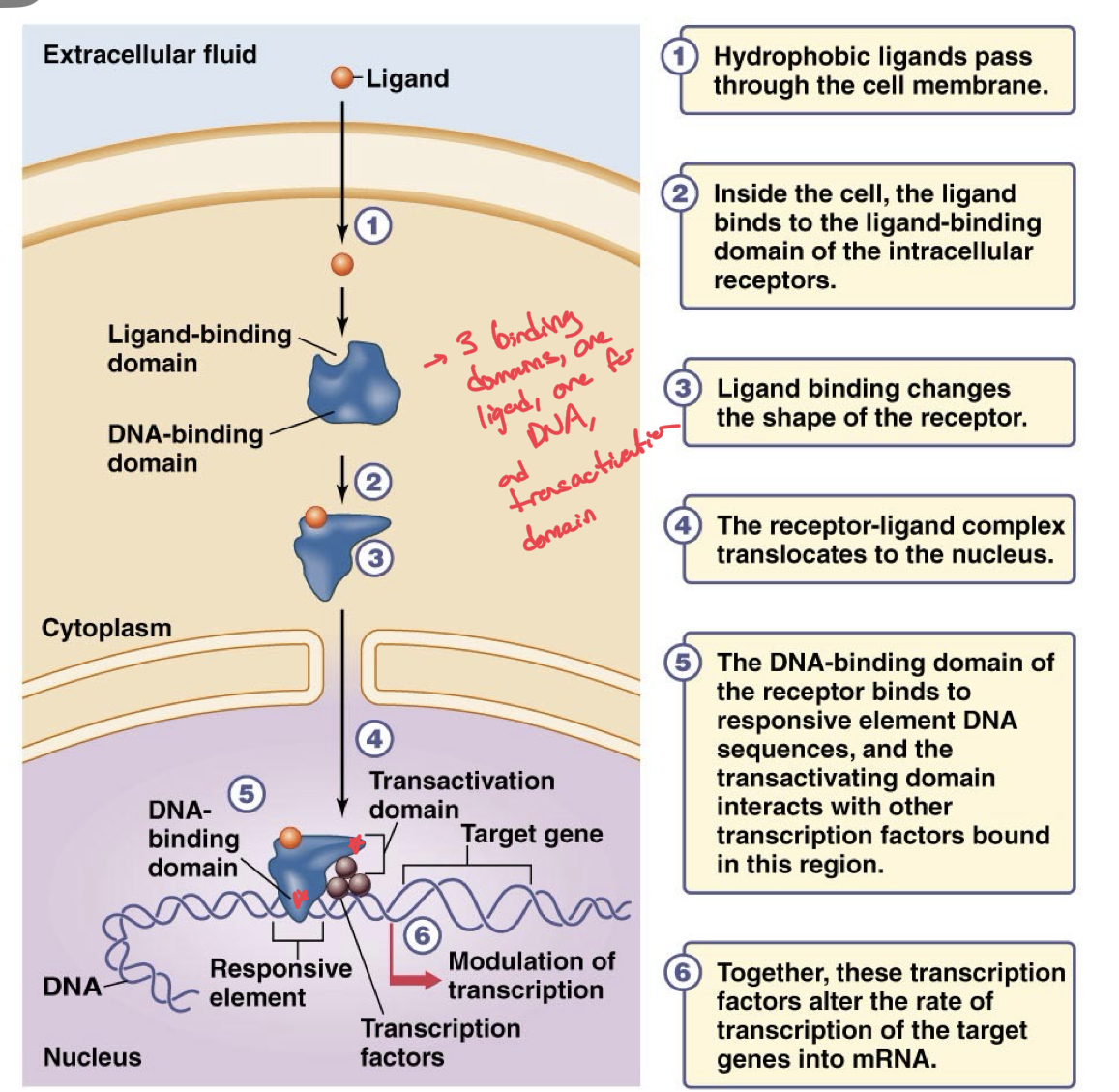
Intracellular Receptors
Ligand Diffuses across the cell membrane
Binds to receptor in cytoplasm or nucleus. If in the cytoplasm, the binding causes the receptor to move into the nucleus.
This formed L-R complex binds to a DNA region known as the responsive element via the DNA-binding domain
Triggers the activation of different transcription factors which will regulate gene expression of a nearby gene.
Increases or decreases production of specific mRNA
Signal Amplification
Amplification of signals from one trigger/stimulus is key to getting our body to function as one well-oiled machine and to get many diverse responses from one ligand-receptor complex.
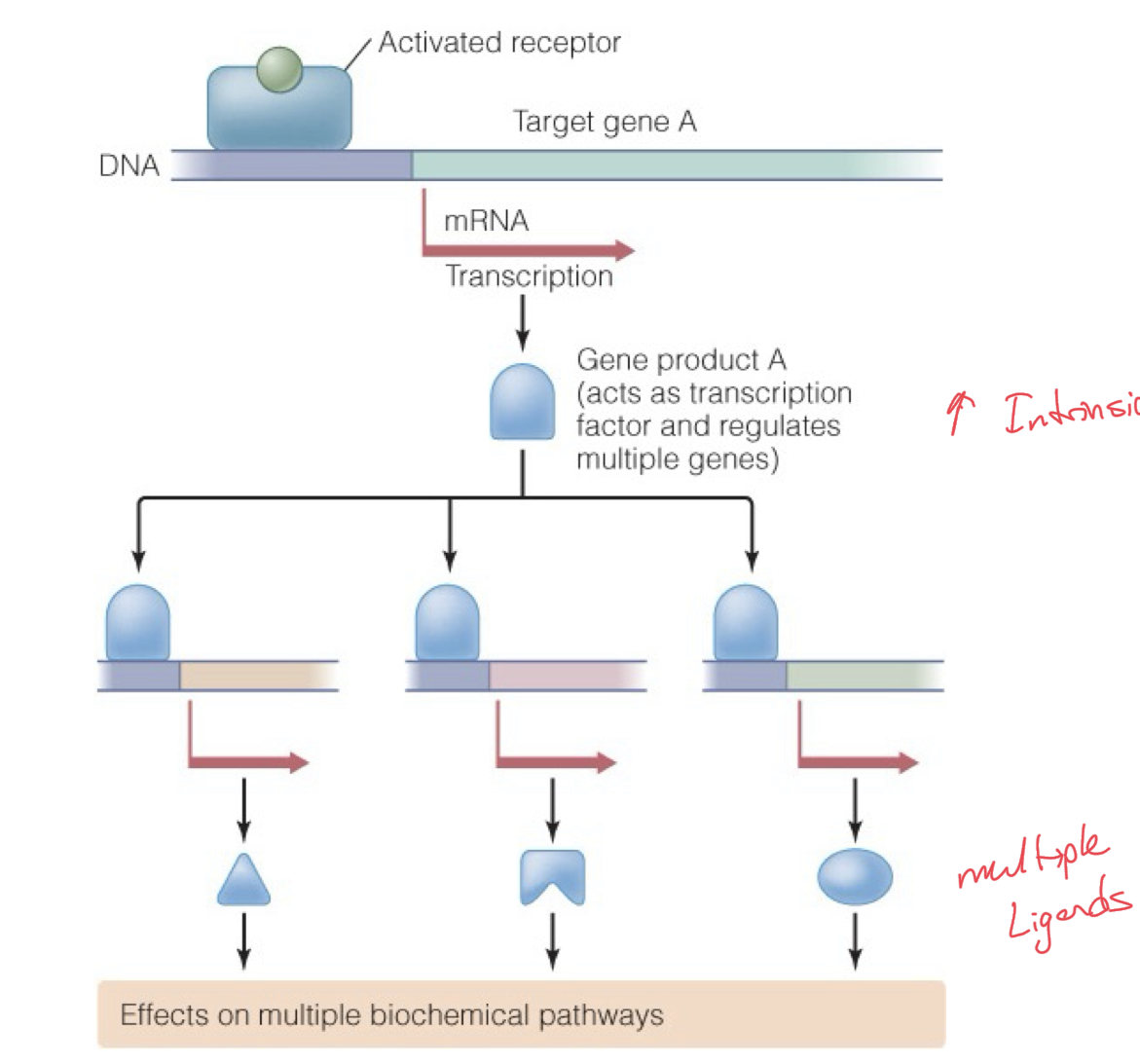
Intracellular receptors and transcriptional cascades, a closer look
An activated intracellular receptor will trigger transcription factors which could increase gene expression of a gene.
This gene could in turn be transcribed into mRNA for more transcription factors, which will then go on to regulate transcription of even more diverse regions of DNA.
This could continue or they could end up producing multiple ligands.
Widespread effect of transcription from one DNA region.
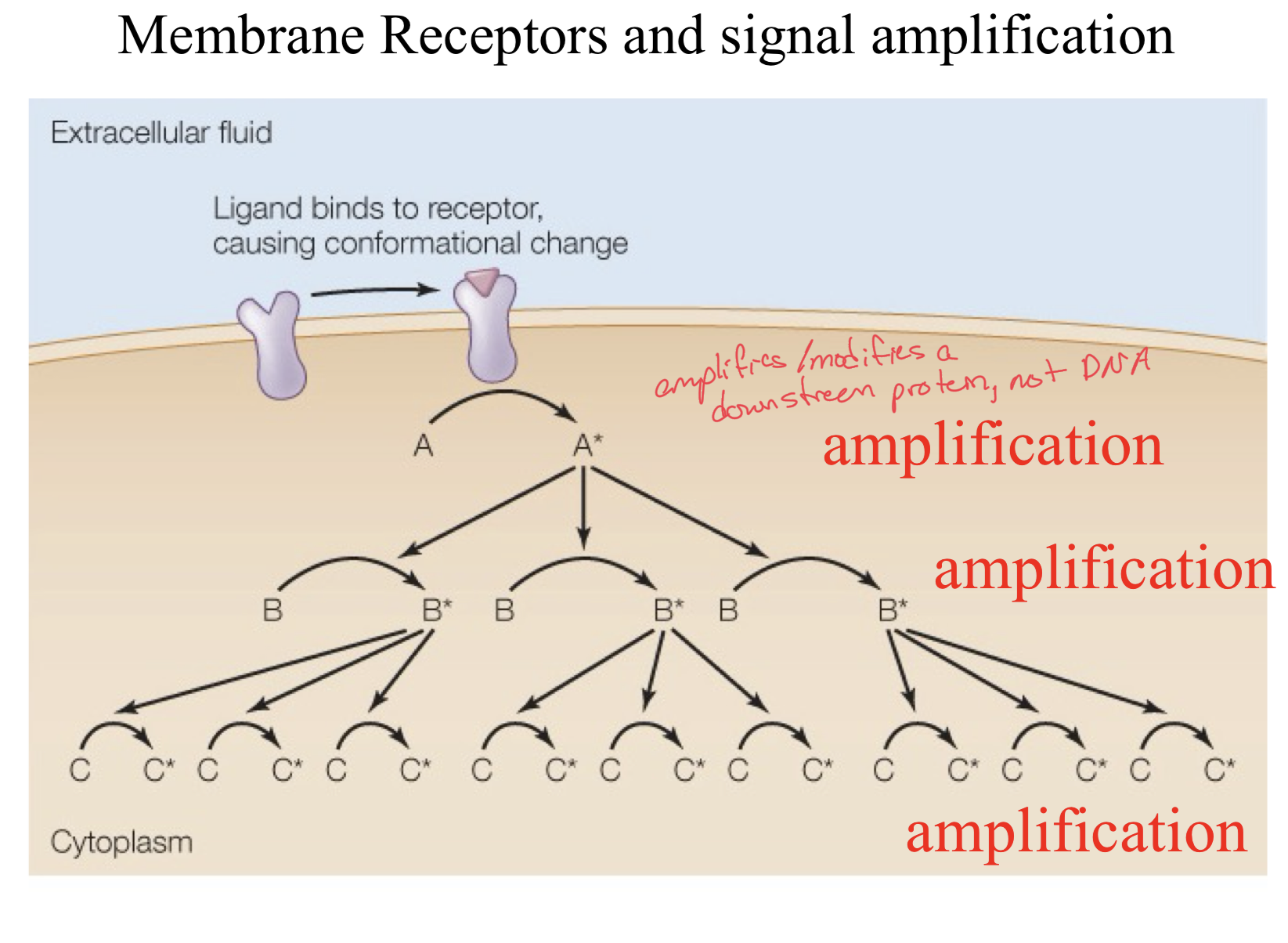
Transmembrane Receptors and Signal Amplification
When a ligand binds to a receptor, a conformational change is triggered.
This in turn causes product A to be activated.
This activated A then in turn activates many of product B
These many activated product B’s activate even more Product C molecules and this is how signals get amplified through a cascade of activation, increasing in targets every time.
Membrane Receptors with Enzymatic Activity
3 Major Cases of Pathways for Enzymatic Activity of Receptors, with some variation within but a rather stable framework
Every Enzyme Receptor has a ligand binding domain, a transmembrane domain, and a catalytic domain.
The 3 classes are Guanylate Cyclases, Tyrosine Kinases, and Serine/Threonine Kinases.
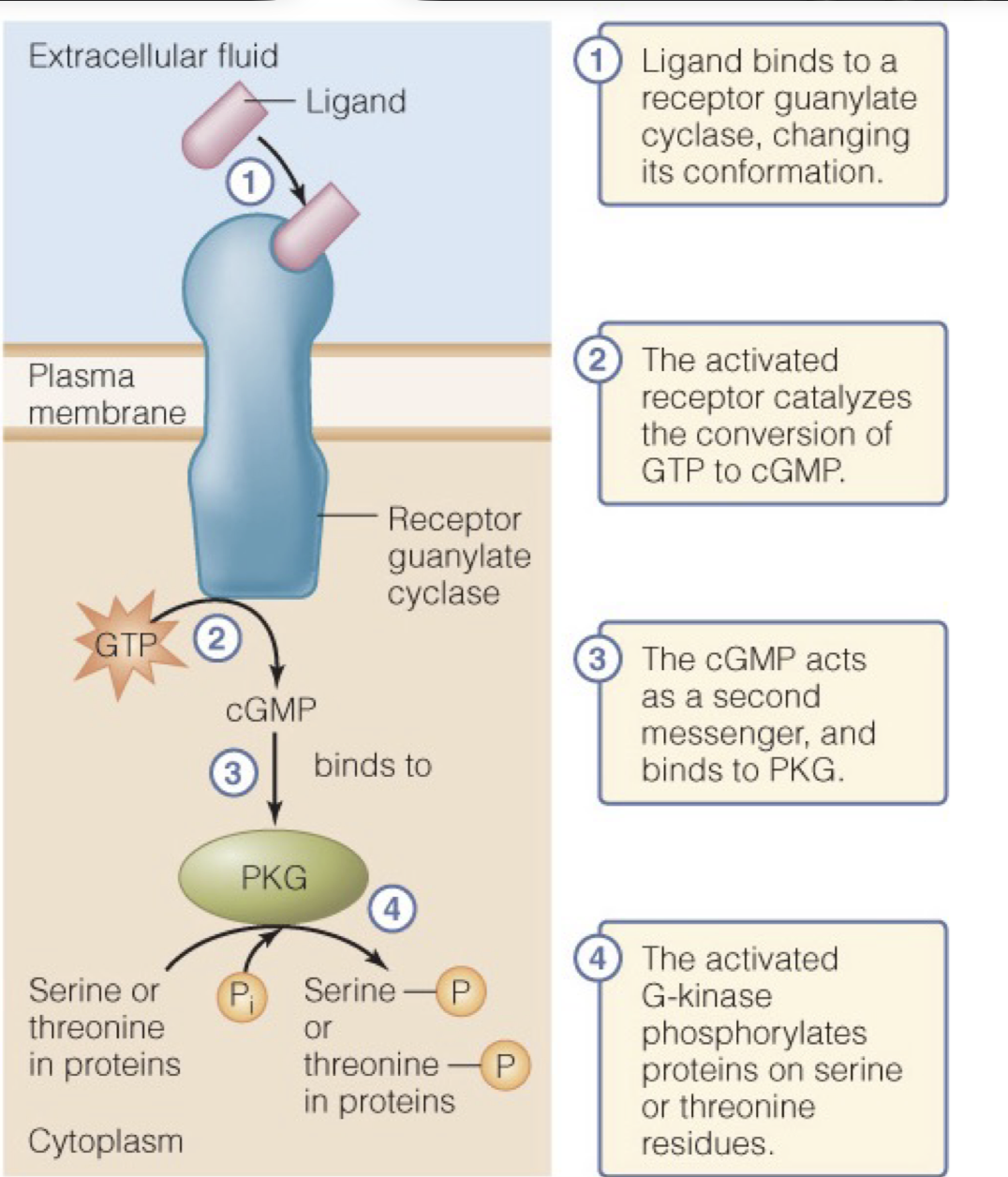
Guanylate Cyclases
In a guanylate cyclase, a ligand will bind the ligand-binding domain changing the conformation of the receptor.
This activated receptor then acts as a catalyst for the conversion of GTP to cGMP
The cGMP is a secondary messenger which binds to and triggers PKG to become activated and in turn begin phosphorylating serine or threonine residues in proteins, activating these proteins.
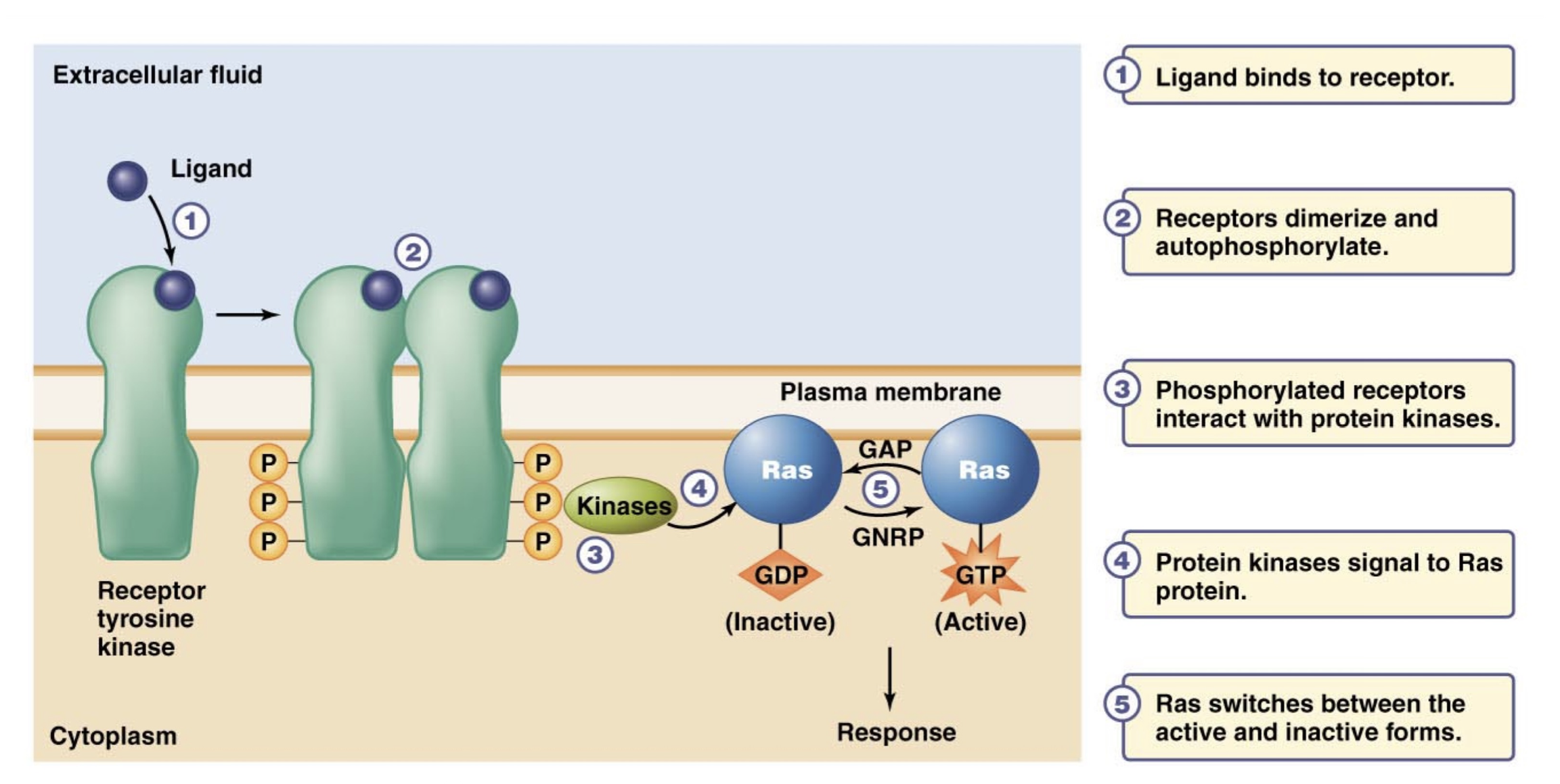
Receptor Tyrosine Kinases
When a ligand binds to a tyrosine kinase receptor, it triggers this recpetor to dimerize and once dimerized, it autophosphorylates.
Now that the dimer is phosphorylated, it is in its active form and it interacts with and activates protein kinases
In turn, these protein kinases signal to Ras proteins to become active by binding GTP instead of GDP, which is their inactive signal. GTP as a secondary messenger.
Ras continues switching between active and inactive forms.
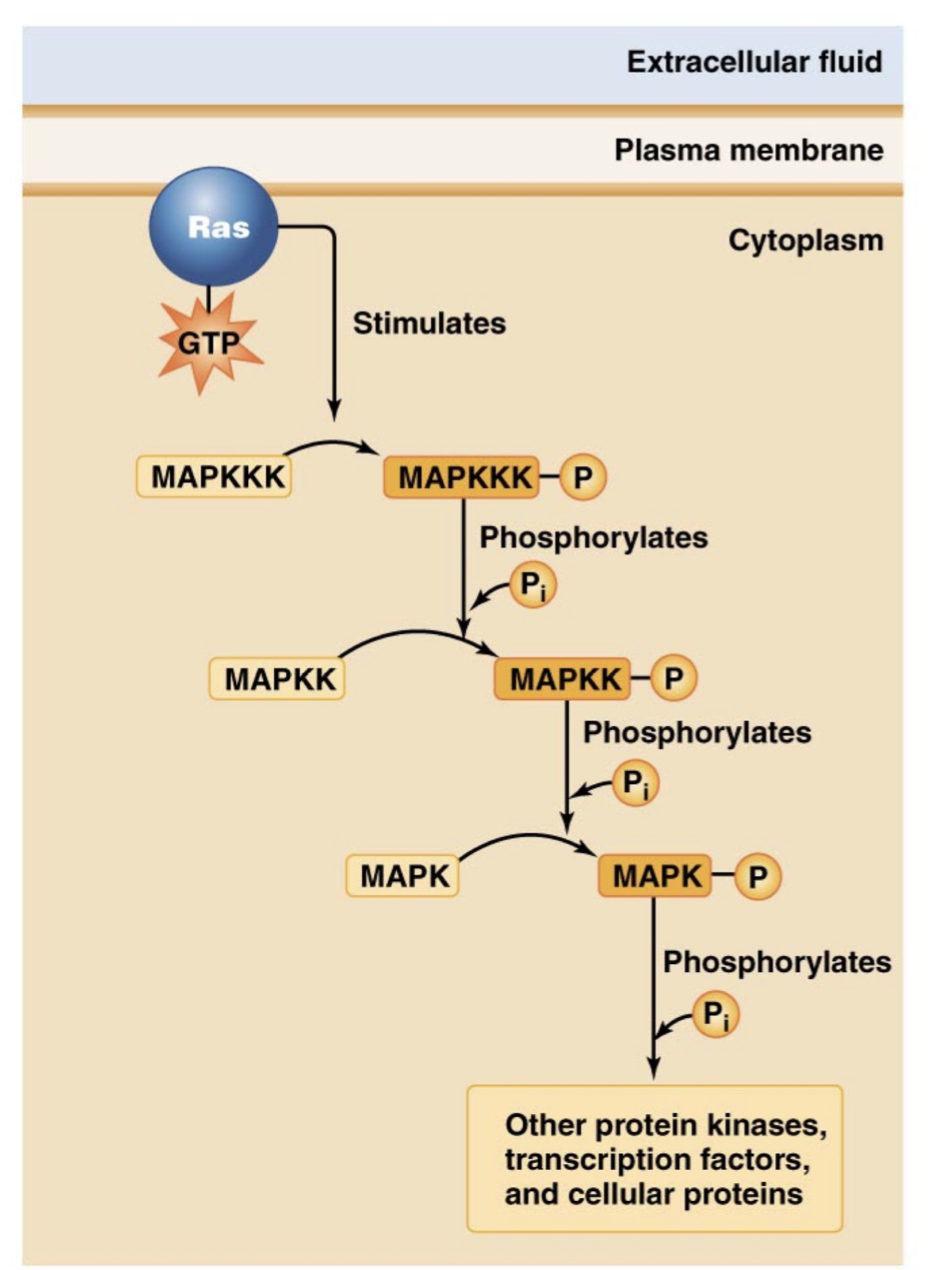
However, when Ras is active it triggers a phosphorylation cascade response.
Ras proteins activate and phosphorylate MAPKKK proteins which will in turn phosphorylate MAPKK proteins,
Phosphorylated MAPKK will phosphorylate MAPK proteins, which will then phosphorylate other protein kinases, transcription factors, and proteins for the response.
Ras Active v Inactive
When Ras is active, it is bound to GTP
When Ras is inactive it is bound to GDP
Protein kinases triggered by the RTK make Ras switch between active and inactive, but there are other enzymes that help
GAP: GTPase activating proteins, help the deactivation by dephosphorylating GTP
GNRP/GEF: Guanine nucelotide exchange factors, helps phosphorylate GDP into GTP
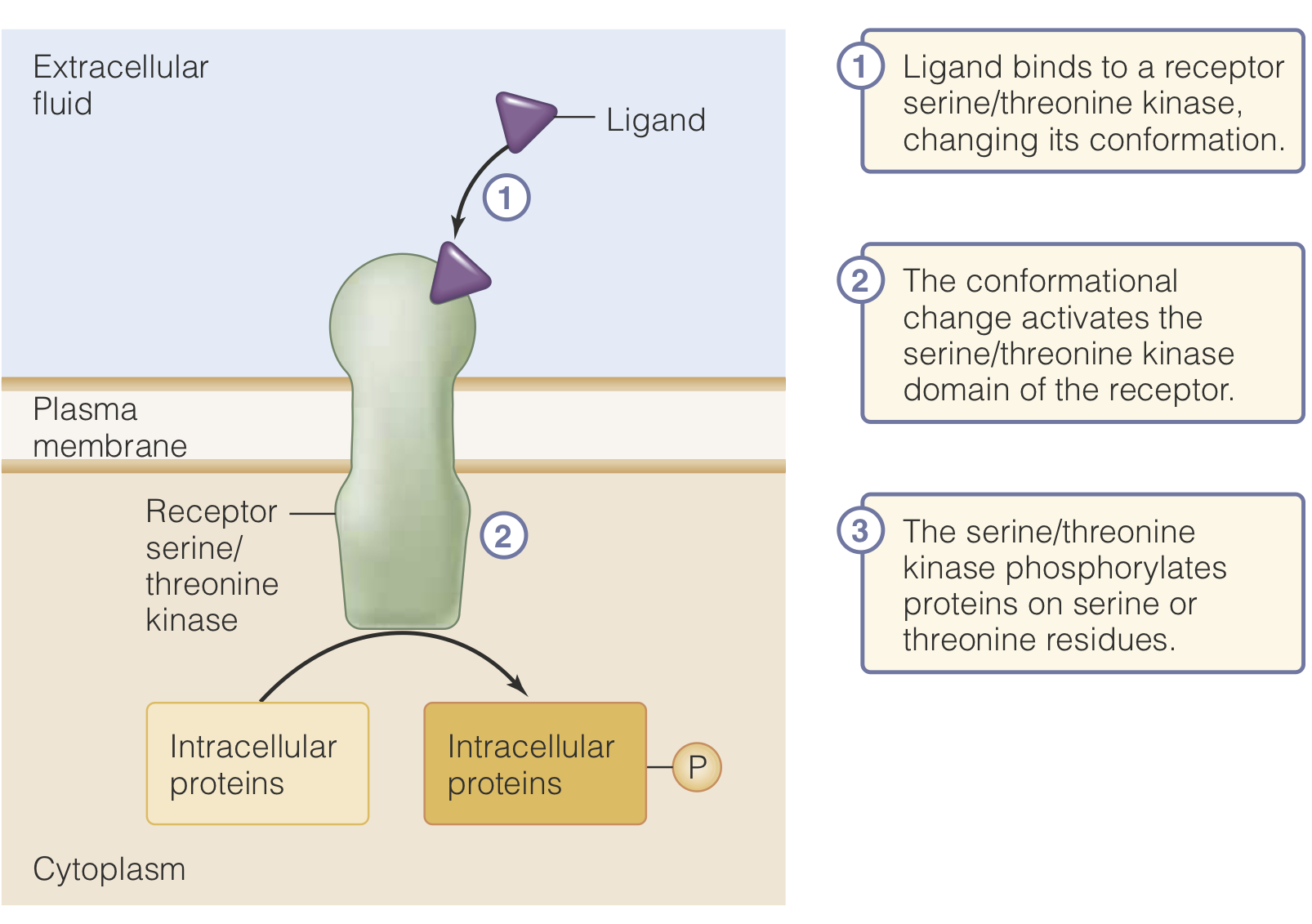
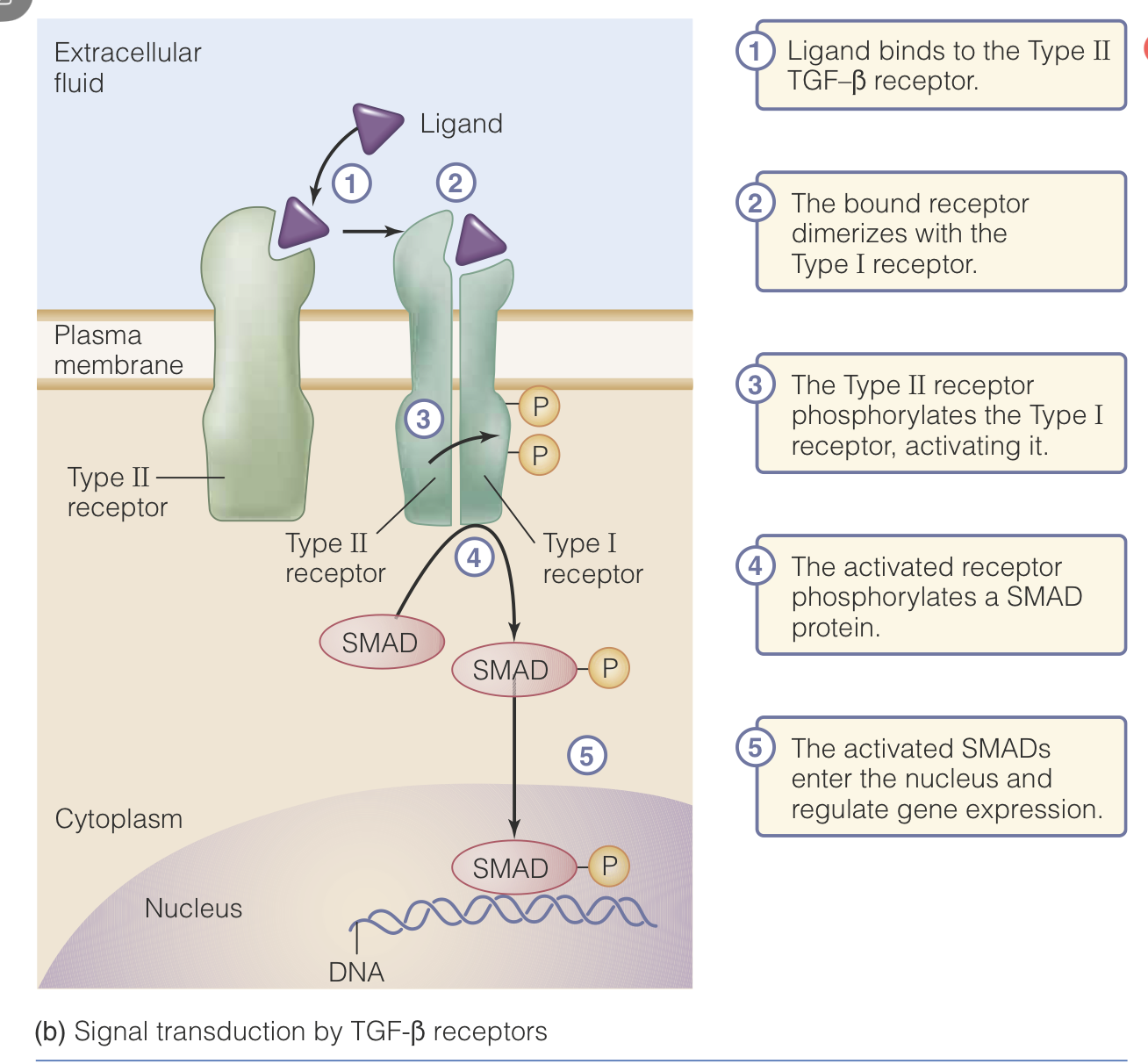
Serine/Threonine Kinase Receptors
In this case, a ligand binds to a Type II TGF-Beta receptor (Tissue Growth Factor Beta Receptor)
Once this receptor is bound, it dimerized with its Type I receptor. This dimer can then carry out the full reaction of the receptor.
Once the dimer has formed, the Type II subunit phosphorylates the Type I subunit.
This phosphorylation activates the Type I receptor and it phosphorylates a SMAD protein.
These activated SMAD proteins will then enter the nucleus and regulate gene expression.
More generally, these receptor bind ligand and then phosphorylate intracellular proteins, to trigger further effects.
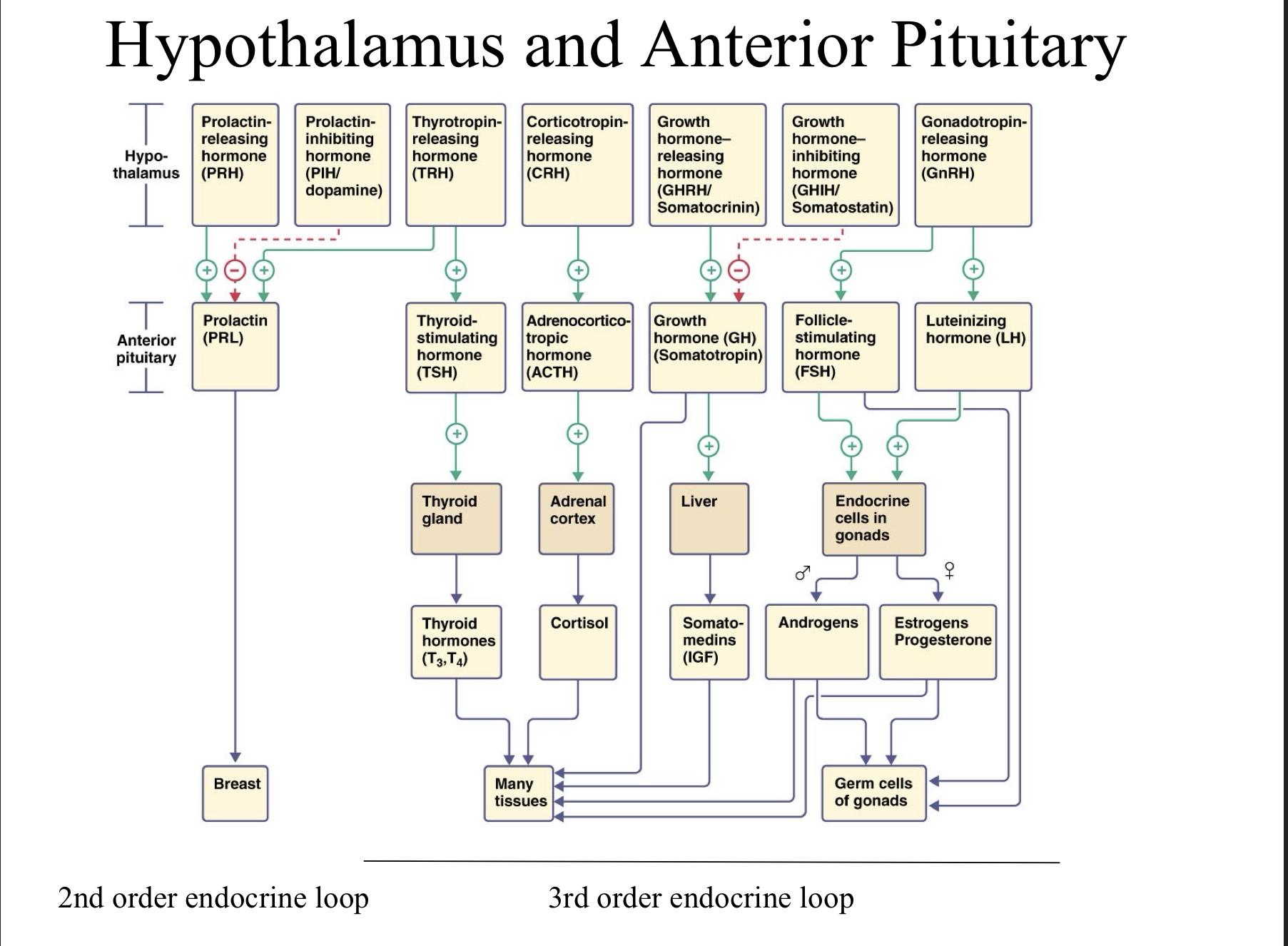
Pituitary Gland + Hypothalamus
These two regions are like the top of the endocrine system, they run the whole show from the CNS.
Pituitary Gland
The pituitary gland secretes many hormones.
It has two distinct anatomical sections: The anterior pituitary (blood vessel) and the posterior pituitary (physical)
It is in direct communication with the hypothalamus through blood vessels and neuronal connections, depending on which section.
Anterior Pituitary
Also known as the adenohypophysis
Has the portal vein system to transport neurohormones from the hypothalamus to the anterior pituitary
When hypothalamus receives some stimulus, it’s neurons releases neurohormone into the portal vein system and does not directly synapse onto the anterior pituitary
As the neurohormone reaches the anterior pituitary, it triggers the secretion of tropic hormones, which then gets carried down the blood stream to its target organs and the neurohormone is removed from circulation.
Neurohormone from hypothalamus only circulates around the anterior pituitary gland

Anterior Pituitary Mechanism
Hypothalamus synthesizes and secretes neurohormones
These neurohormones travel via the hypothalamic-pituitary portal vein system
Then, the anterior pituitary is stimulated by the neurohormones to release tropic hormones to target organs.
This triggers the beginning of a third order endocrine pathway.
Tropic Hormones
Tropic hormones are hormones which cause the release of another hormone.
Posterior Pituitary
For the posterior pituitary, it is a first-order endocrine loop, as the neurons from the hypothalamus extend all the way to the posterior pituitary and release neurohormones into the blood vessels surrounding the posterior pituitary.
Posterior pituitary technically releases these hormones into circulation but in reality, they are directly from the hypothalamus via a physical neural connection.
AVP
Arginine Vasopressin, also known as Anti-Diuretic Hormone
Peptide hormone that regulates water retention, blood pressure, and urine production. Aids in retention of water in the kidneys to conserve water
First order endocrine loop, via the posterior pituitary.
Oxytocin
Peptide hormone that regulates uterine contractions during labor, stimulates milk let-down (NOT MILK PRODUCTION- Prolactin)
Promotes social bonding (Love hormone)
Important for bonding between mothers and offspring as well as for partners.
Works via positive feedback, during labor the release of oxytocin causes further release of oxytocin until labor is over.
First order endocrine loop via the posterior pituitary.
Hypothalamic control of adenohypophysis
The hypothalamus secretes various hormones which trigger the anterior pituitary to release tropic hormones
These hypothalamic hormones include TRH, GnRH, and CRH
Thyrotropin Releasing Hormone (TRH)
First hypophysiotropin together with GnRH being isolated in 1969.
Stimulates the release of Thyroid stimulating hormone (TSH) from the anterior pituitary.
Tripeptide hormone composed of pyroglutamyl-histidyl-prolineamine chains.
Short 3 amino-acid peptide
Gonadotropin-Releasing Hormone (GnRH)
10 amino acid decapeptide, highly conserved through species
Stimulates the release of follicle stimulating hormone (FSH) and leutinizing hormone (LH) from the anterior pituitary.
Corticotropin Releasing Hormone (CRH)
Stimulates the release of Adrenocorticotropic Releasing Hormone (ACTH) from the anterior pituitary.
41 amino acid peptide
Structurally related to urotensin secreted by frog skin and fish urophysis
Hormones produced by the anterior pituitary
Growth Hormone
Prolactin
Thyroid Stimulating Hormone via TRH
Adrenocorticotropic hormone via CRH
Leutinizing Hormone via GnRH
Follicle stimulating hormone via GnRH
Growth Hormone (GH)
Peptide hormone that is involved in the growth of tissues
Released by the anterior pituitary after receiving signals from hypothalamus.
Hypothalamus releases either GH-releasing hormone or GH-inhibiting hormone, which dictates what the anterior pituitary does.
Gigantism
Increased levels of GH early in life
Acromegaly
Increased GH later in life
Abraham Lincoln had this condition
Shorter lifespan because heart cannot keep up with the growing tissues/increased circulatory needs
GH Deficiency
Leads to short stature or just dwarfism
Receptor Insensitivity
GH-receptors do not respond, even though growth hormone is produced normally
Leads to Dwarfism.
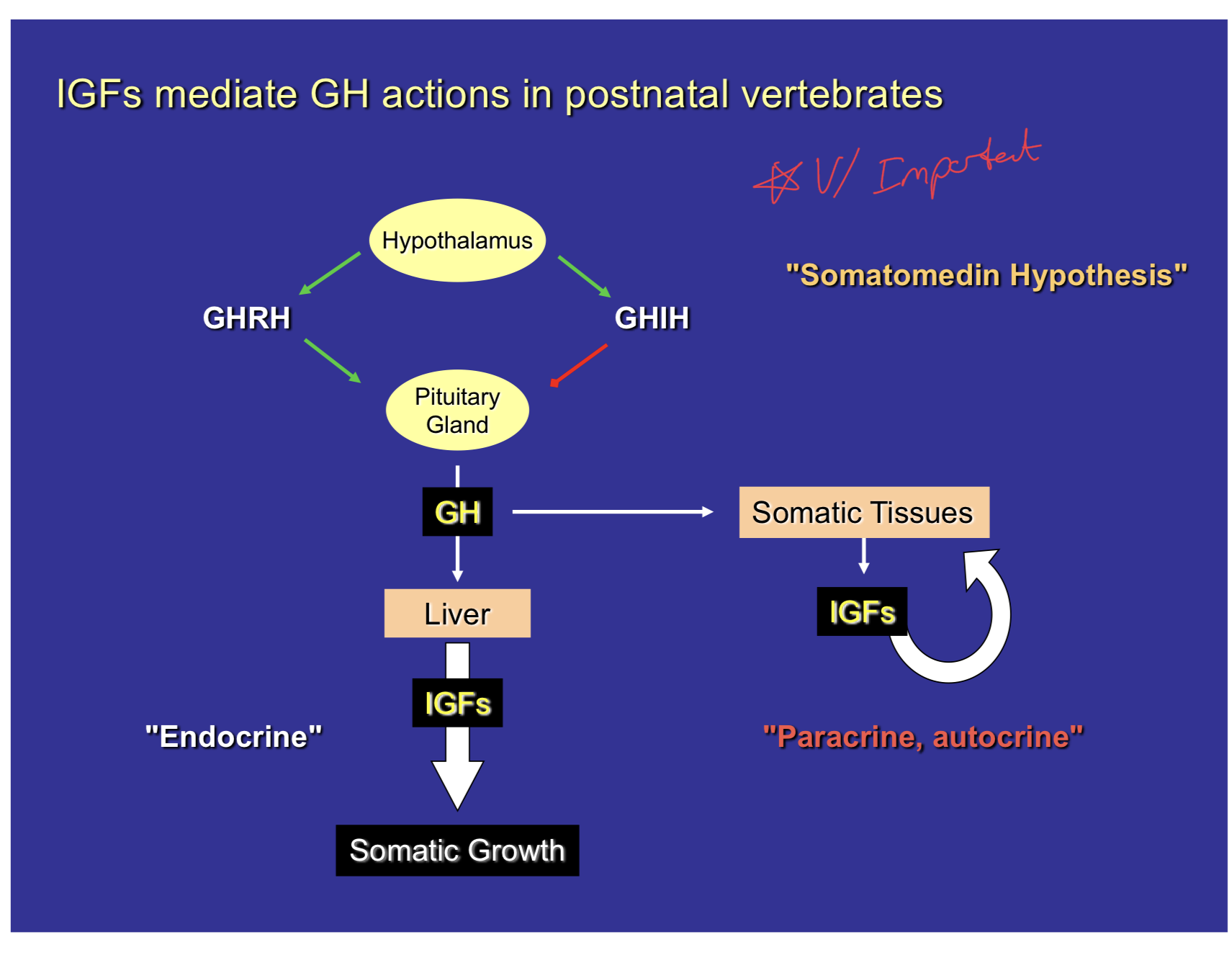
Somatomedin Hypothesis
Pathway proposed to explain the course of growth hormone throughout our bodies.
Begins at the hypothalamus, where it either releases GHRH or GHIH depending on the existing levels of growth hormone in our bodies.
These hormones then travel through the portal vein system to the anterior pituitary to trigger the release or inhibition of growth hormone.
When growth hormone is released, it travels to the liver and to somatic tissues.
At both the liver and somatic tissues, Insulin-like growth factors, another class of peptide hormones, is released which can trigger somatic growth in both.
In the somatic tissues, the IGF works through a paracrine/autocrine system, as it is released by those tissues and affects those tissues
In the liver, the IGF travels through the circulatory system in an endocrine pathway to trigger growth of somatic tissues.
There is negative feedback on this system, when there is lots of IGF present, negative feedback on pituitary and on the hypothalamus. Also, when there is too much GH detected, negative feedback occurs on the hypothalamus to release GHIH or decrease GHRH.
Insulin-like Growth Factor
Peptide hormone that is heavily involved in somatic growth.
Involved in somatic growth but also invlved in brain and ear hair cell development
IGF-1 Abnormality
Severe/profound deafness and mental retardation
Patients were unresponsive to injections of GH, due to the IGF-1 hormone being abnormal, a shorter peptide, so it was not functioning correctly.
Prolactin
Peptide Hormone secreted by the anterior pituitary
Main job of this hormone is to stimulate milk synthesis
Also promotes maternal behavior through effects on the brain.
Found in all vertebrates, even those without mammary glands.
DOES NOT control milk secretion, only production.
Human Mammary Gland
Has 3 lobules and 4-5 ducts with which to control milk secretion.
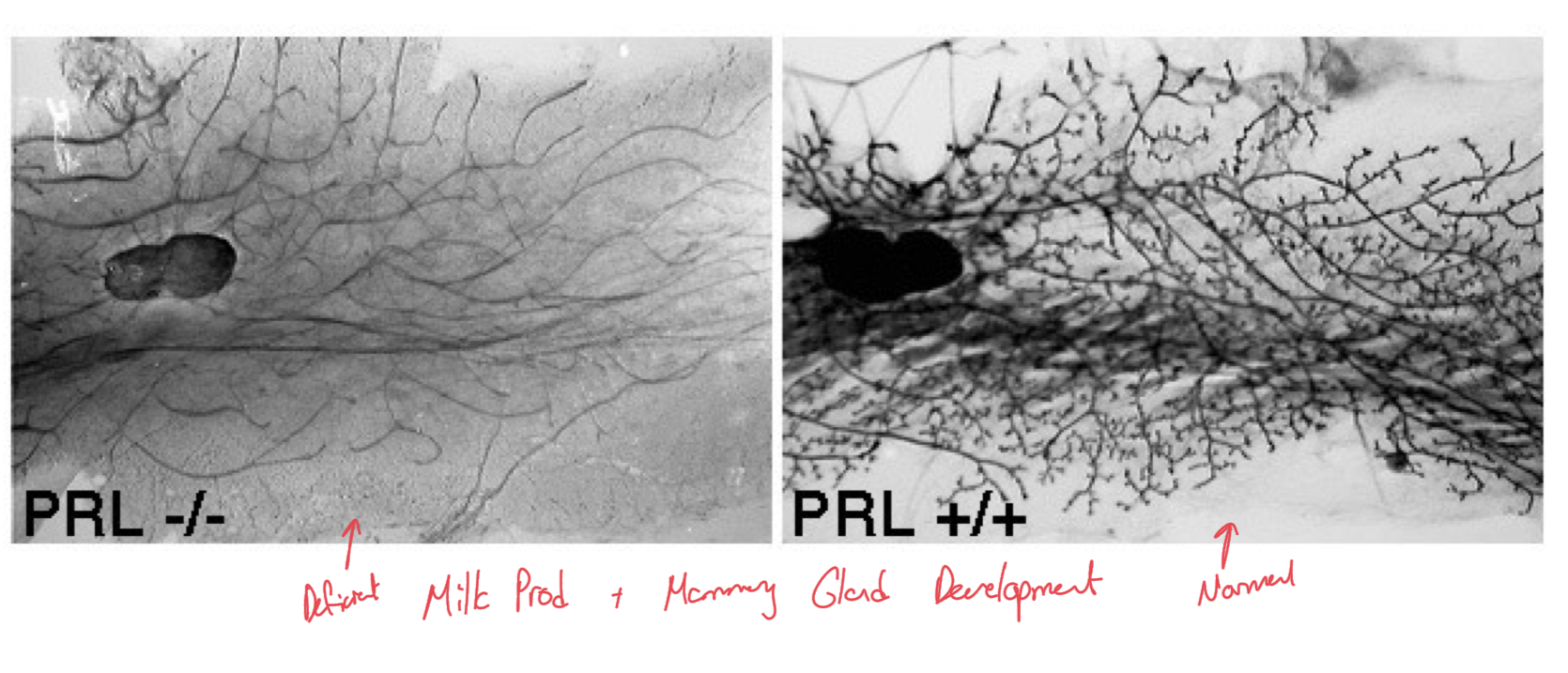
PRL in Mammary Gland Development
When PRL hormone has been knocked out, removed, there is deficient milk production and mammary gland development as compared to individuals with normal prolactin production/secretion.
Other actions of PRL in vertebrates
1. Osmoregulation- most primitive action of PRL. In fish, it served as a fresh-water adapting hormone.
2. Reproduction- Concerned with the consequences of reproduction, like development of mammary gland, development of crop sac in pigeons. Inhibitory to GtH (gonadotropin hormone) secretion
3. Development- Considered a larval(tadpole) growth hormone, anti-metamorphic. This feature is mainly studied in amphibians
4. Metabolism- Affects lipid and glycogen metabolism
5. Integument (Skin)- Affects hair growth, sebaceous glands, feather patterns in birds, and pigmentation
6. Behavioral Effects- Maternal behavior.
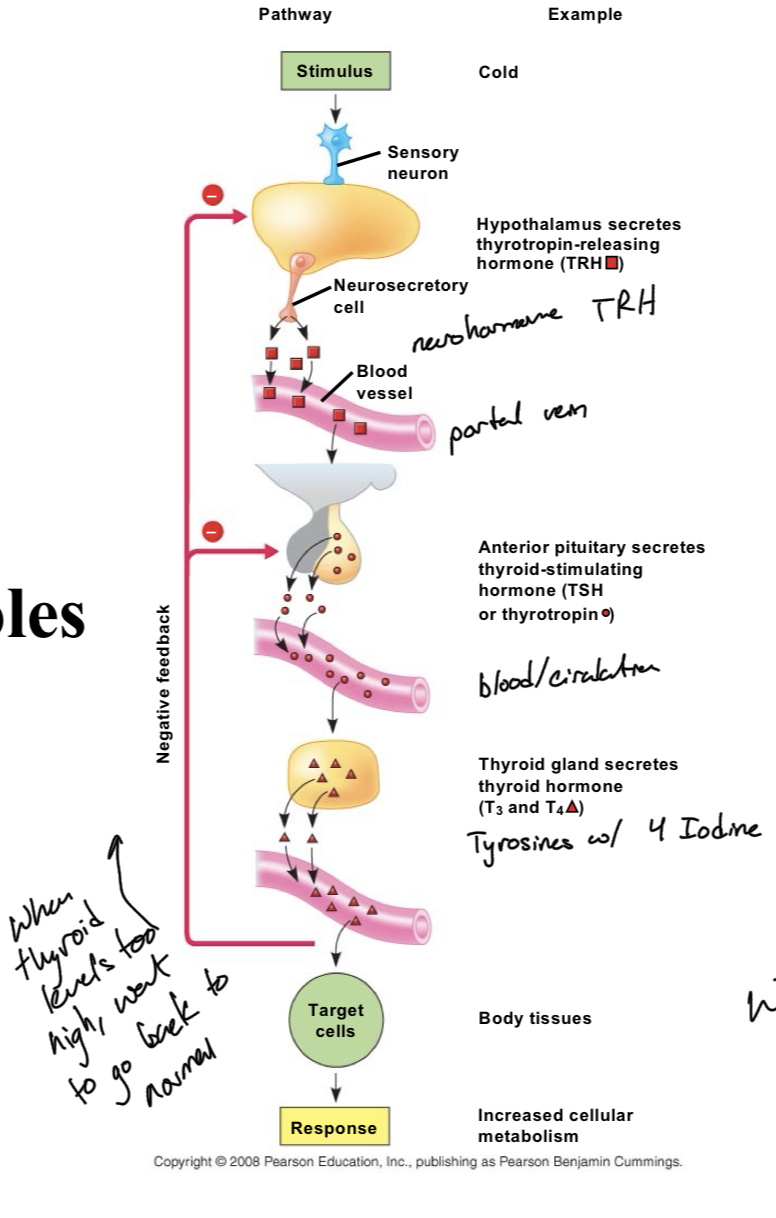
Thyroid Stimulating Hormone (TSH)
Controls the secretion of thyroxine (T3/T4) by the thyroid gland
Secreted by the anterior pituitary in response to Thyrotropin Releasing Hormone (TRH) from hypothalamus
Thyroid
The word means “shield” in Greek
Names for the shield-shaped cartilage of the larynx.
Structure of Thyroid Hormones
T4 Thyroid Hormone: Known as tetraiodothyronine, contains 4 Iodine atoms
T3 Thyroid Hormone: Known as triiodothyronine, contains 3 Iodine atoms. 10x more active than T4
Amines but they are hydrophobic
Role of Thyroid Hormone
Thyroid hormone is mainly involved in metabolism and thermogenesis, creating heat and increasing energy production.
Can also be involved in a negative feedback loop when there is too much thyroid hormone. This loop inhibits the secretion of TRH (hypothalamus) and TSH(adenohypophysis)
Low thyroid hormone levels lead to low energy and weight gain because metabolism is so slowed.
Cretinism
Caused by insufficient thyroid hormone during fetal and neonatal development
Condition of severe mental retardation and growth defects
Occurs when our body is not producing enough thyroid hormone.
Goiter
Caused by a dietary iodine deficiency
Iodine is necessary for proper production of T3 and T4 as it is embedded in the molecules
Iodine must come from food because it is essential, we do not produce it in any way.
When we lack iodine, the pituitary gland releases more TSH in response to these decreased levels of T3/T4.
Solution was adding iodine to our table salt.
Hashimoto Disease
Autoimmune disease where there are TPO antibodies which destroy the machinery which makes thyroid hormones.
People with this condition thus have low thyroid hormone levels.
Solution is to inject people with thyroid hormone.
Graves Disease
An immune system disorder that results in the overproduction of thyroid hormones (hyperthyroidism)
Accelerated metabolic processes such as heart rate, protein breakdown, neural activity, and heat generation.
Using lots of energy because metabolism is at full speed, engine running at top speed.
Leads to anxiety, irritability, fine tremor in hands/fingers, heat sensitivity, enlargement of thyroid gland because excess thyroid hormone but still functions properly, change in menstrual cycles, ED or reduced libido, bulging eyes aka Graves’ opthalmopathy, fatigue, thick red skin aka Graves’ dermopathy, and rapid/irregular heartbeat.
Adrenocorticotropic Hormone (ACTH)
Regulates the secretion of corticosteroids by the adrenal cortex.
Part of our stress response system known as the HPA axis
Triggered release when the hypothalamus secretes Corticotropin Releasing Hormone (CRH)
Gonadotropins
Leutinizing Hormone (LH)
Follicle Stimulating Hormone (FSH)
Both Peptide Hormones
Connections Between Hormones, Hypothalamus, and Anterior Pituitary
Tropic Hormones come from the Hypothalamus
Be aware of activating and inhibiting hormones for PRL and GH.
Endocrine Glands in the Central and Peripheral Nervous System
Pancreas
Located near the small intestine
Accessory of digestive tissue
Acts as an endocrine and exocrine gland
Pancreas an an Exocrine Gland
Produces pancreatic enzymes and sodium bicarbonate which gets released into the small intestine via the pancreatic duct
Produces the pancreatic amylase, peptidases, etc.
Pancreas an an endocrine gland
Produces insulin and glucagon, which are both necessary for glucose regulation
Islets of Langerhans
Clusters of endocrine cells within the pancreas that serve as the endocrine pancreas
Made up of 4 cell types, the alpha cells, beta cells, delta cells, and acinar cells
Have capillaries running through them to keep them healthy.
Act as the bodies primary glucose regulator via secretion of endocrine hormones
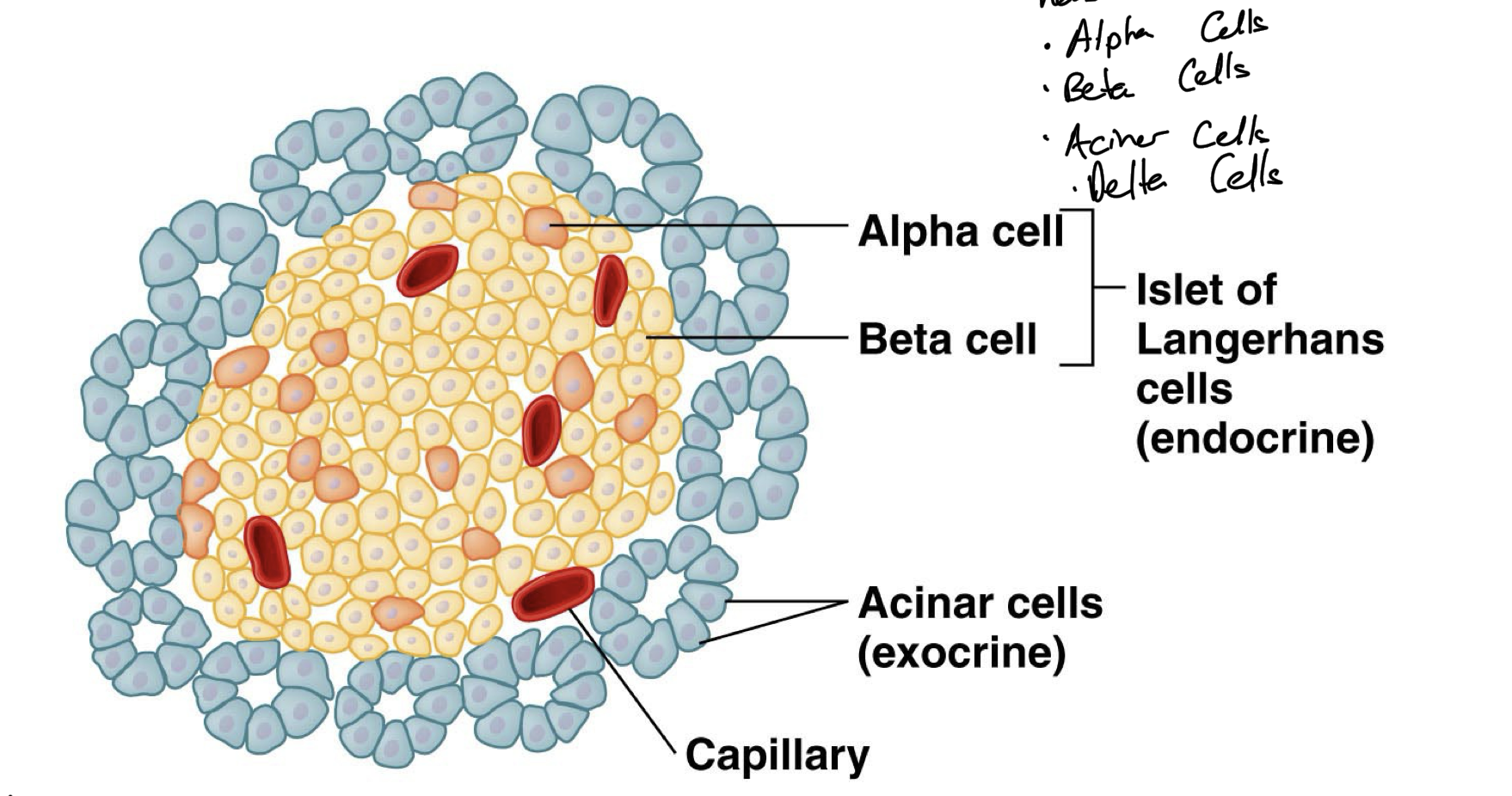
Insulin
Lowers our blood glucose level and moves it to storage, promotes uptake of glucose from blood. Anabolic.
Peptide hormone secreted by the beta cells of the Islets of Langerhans
Regulates the metabolism of carbs, fats, and proteins
Promotes the absorption of glucose from the blood.
Promotes glycogenesis and lipogenesis to store the excess glucose in our blood
Triggered by high blood glucose
Glucagon
Raises blood glucose levels by breaking down glycogen. Catabolic
Peptide hormone secreted by the alpha cells of the Islet of Langerhans.
Works when our body is hypoglycemic.
Regulates the metabolism of carbohydrates
Promotes glycogenolysis, lipolysis, and gluconeogenesis
Triggered by low blood glucose
Somatostatin
Hormone produced by the delta cells of the Islet of Langerhans
Major inhibitory hormone which inhibits GH, TSH, Adenelyl Cyclase, Prolactin
Inhibits the release of insulin and glucagon
Suppresses the exocrine secretions of the pancreas.
Gastrin
Hormone which triggers the stomach cells to produce HCl
Vasoactive Intestinal Peptide (VIP)
Hormone that stimulates the intestine to release water and salts back into the intestinal tract
Amino Acid Makeup of Insulin
51 amino acid chain,
A chain is 21 a.a.
B chain is 30 a.a.
C chain is 21 a.a. but has no physiological role
Proinsulin is 86 amino acids long but the pro region gets cleaved off
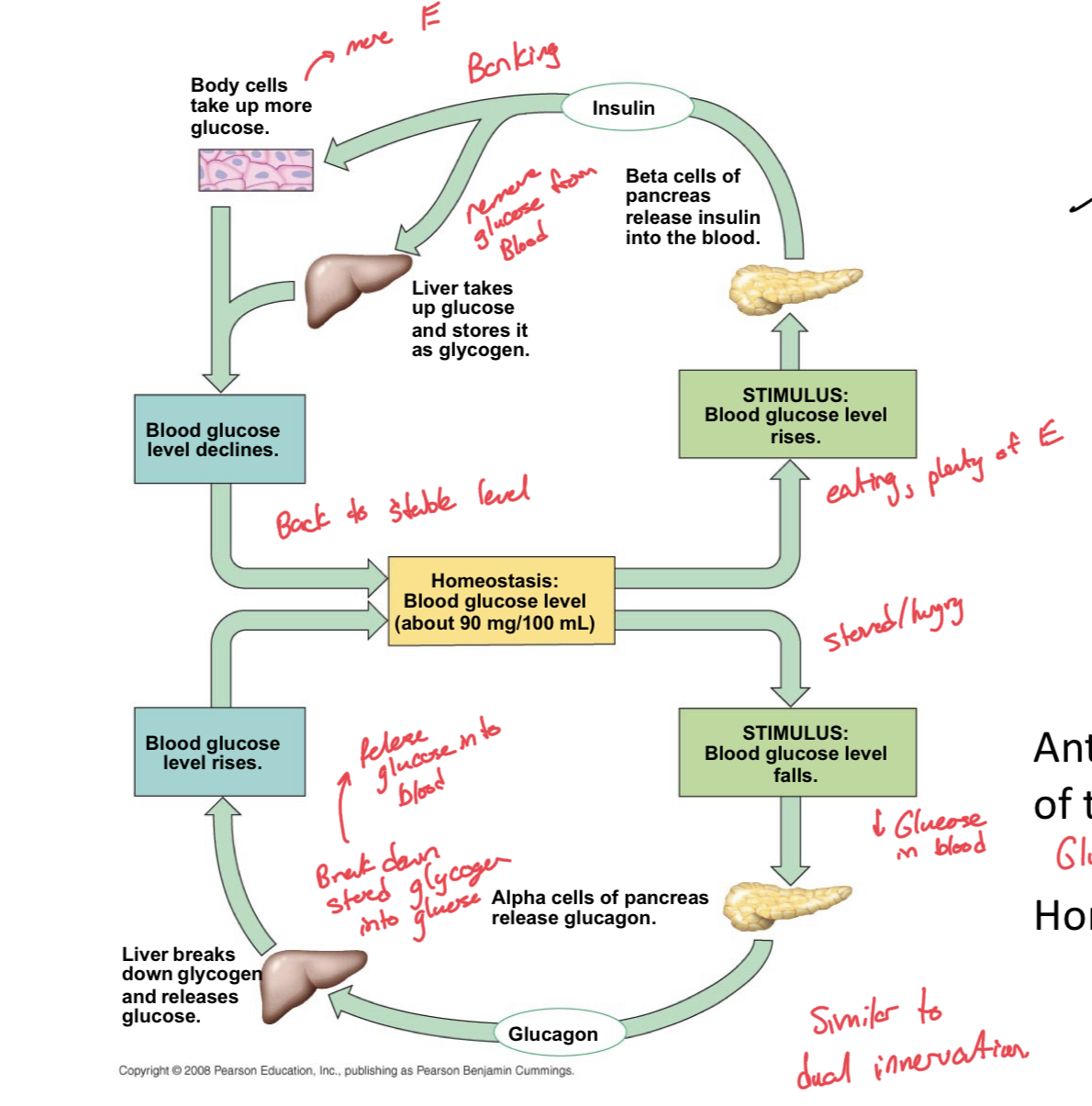
Relationship between Insulin and Glucagon and Homeostasis
When we have high blood glucose (stimulus), then the beta cells of the pancrease release insulin into the blood, which triggers both the body cells to take up more glucose and the liver to take up glucose and store it as glycogen, at which point, blood glucose levels drop back to a homeostatic level
When we have low blood glucose (stimulus) then the alpha cells of the pancreas release glucagon. Glucagon then travels to the liver to trigger the breakdown of stored glycogen and it releases glucose. Then, blood glucose levels rise and return to homeostatic level.
Glucagon and Insulin are like yin and yang, manage an antagonistic relationship for homeostatic regulation.
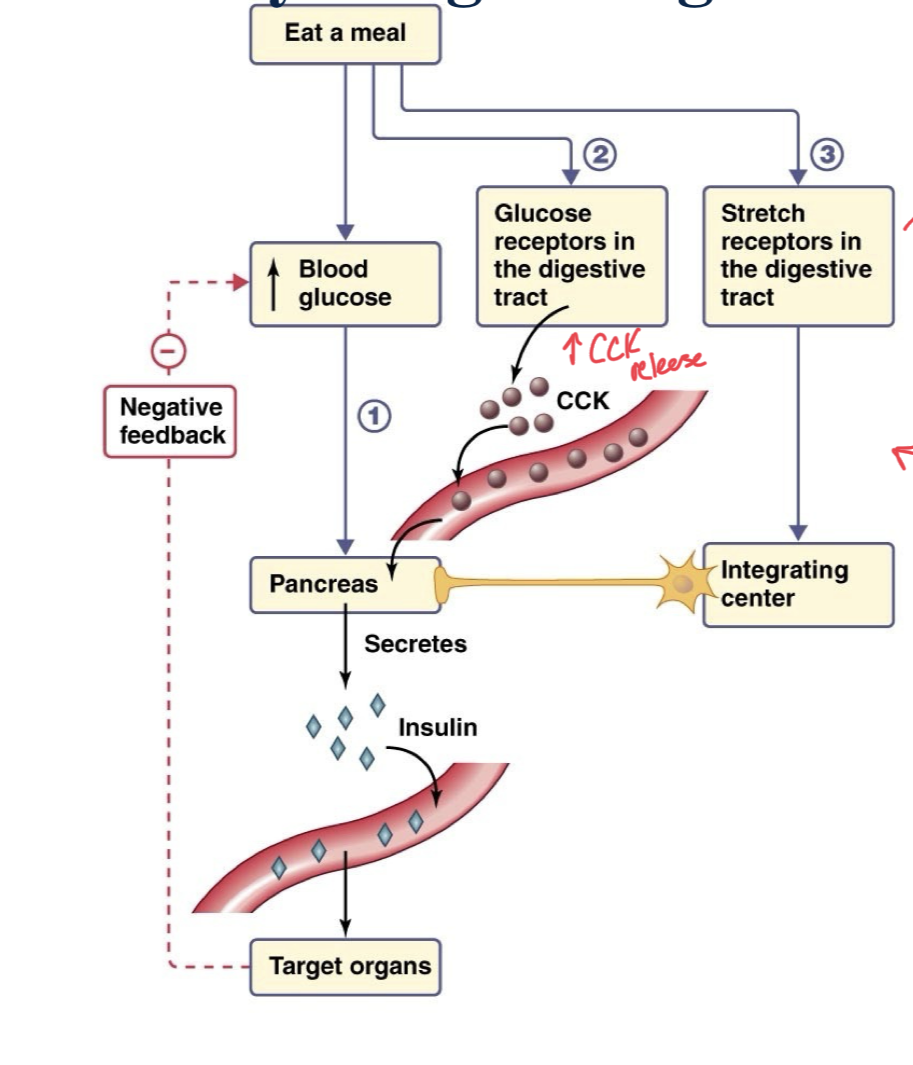
Pathway for regulating Insulin Secretion
Involved feedback as well as feed forward mechanisms
When we eat a meal, there are feed forward mechanisms that trigger the pancreas to secrete insulin before blood glucose levels actually rise.
When we eat, glucose receptors in our digestive tract trigger the release of CCK into the circulatory system which triggers insulin release at the pancreas, fat breakdown, and inhibits hunger. (Feed Forward)
Additionally, stretch receptors in the digestive tract communicate with an integrating center of CNS to communicate with pancreas to secrete insulin into the blood to the target organs.
Mechanism for hormones to work together
Antagonistic Relationships
Additive
Synergistic
Feedback
Feedforward
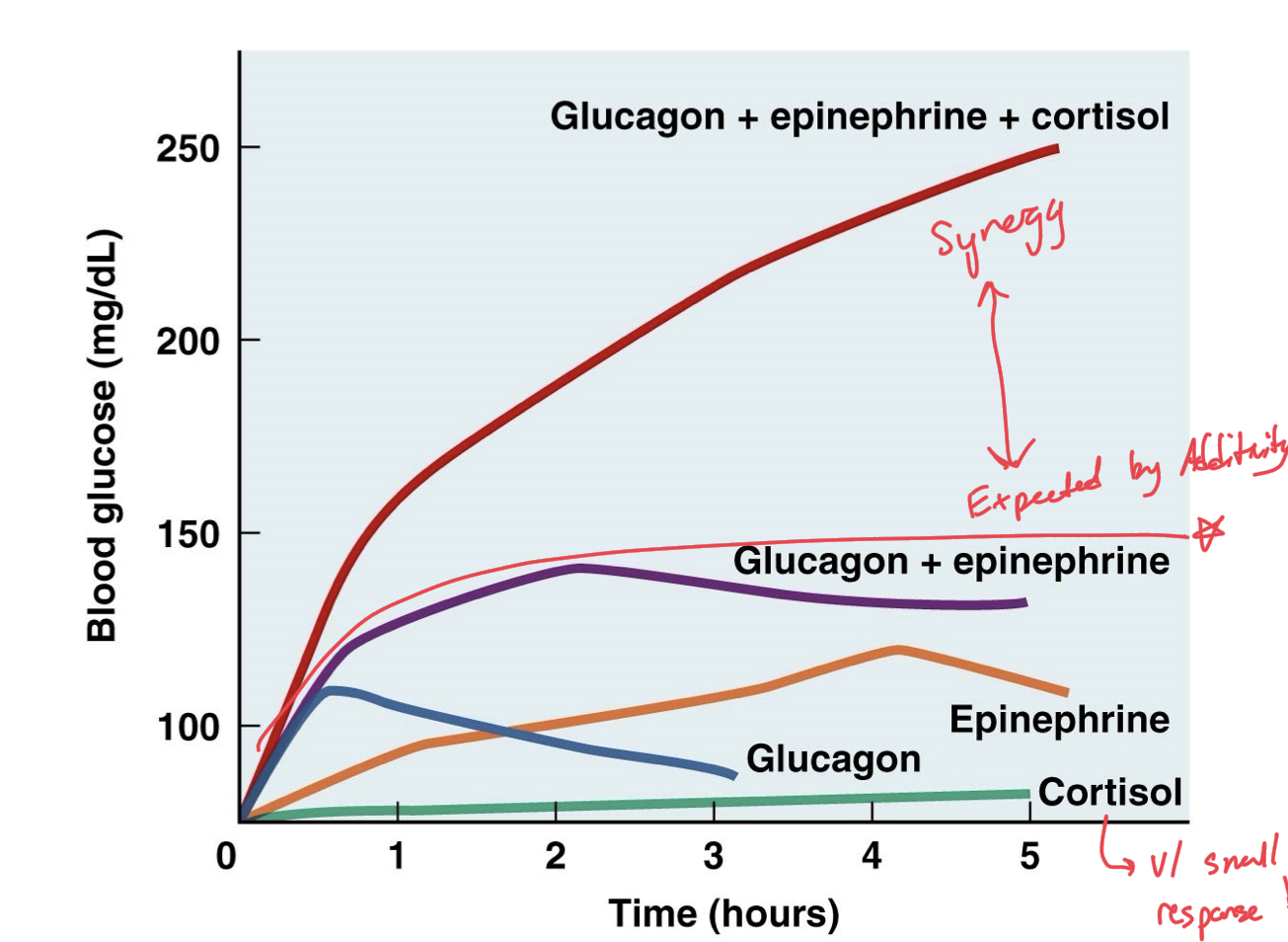
Additivity
When two or more hormones work in the same way on the same target, work together to produce a combined effect of their two individual efforts.
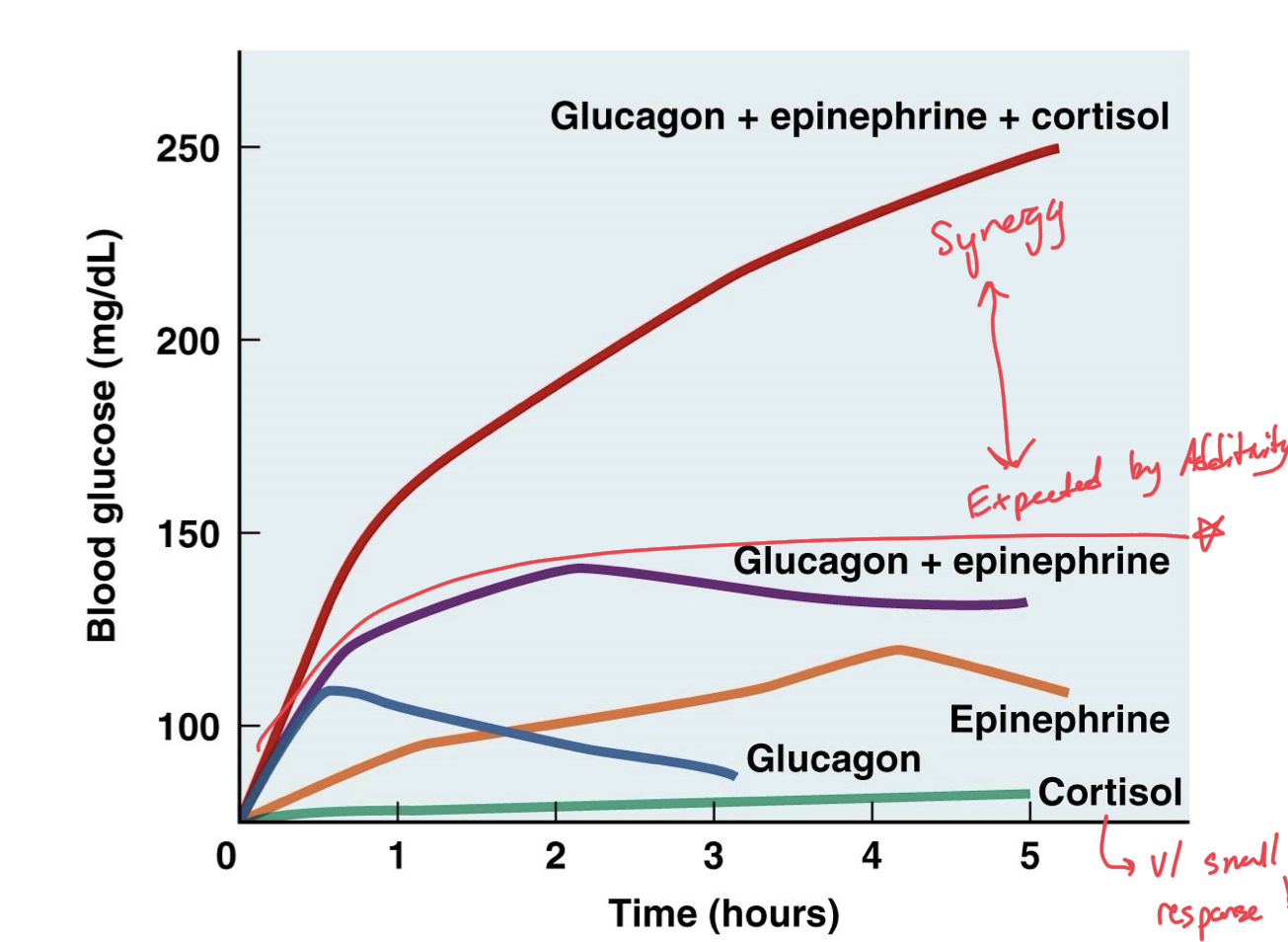
Synergism
When two or more hormones work together to increase the target cell response much more than is expected by just their additivity, by just combined individual efforts, push beyond combination effects.