Eating Disorders 1: Presentations, theories, causes, and maintaining factors
1/132
Earn XP
Description and Tags
Define an eating disorder, and understand the diagnoses involved Detail how many cases of eating disorders exist in the population Distinguish and detail theories of causation and of maintenance Use this understanding of causation and maintenance to explain cases
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
133 Terms
internal balance mechanism in body
homeostasis
homeostasis function
keep eating evenly and diversely, ensure well nourished
what two concepts r being balanced by homeostasis in eating
hunger
satiety
problems w homeostasis
hunger and satiety influenced by interfering factors
influences on hunger - problems for homeostasis
genetics
learning
social learning
influence on satiety- problems for homeostasis
social pressures
food industry
toxic environment
eating disorders (Fairburn & Walsh, 2002)
a persistent disturbance of eating behaviour or behaviour intended to control weight, which significantly impairs physical health or psychosocial functioning
ed diagnoses- over time
change over time, suggesting not rly there yet
icd tends to follow dsm
what
bmi
weight in kg) / (height in m)²
healthy range bmi
19-25
bmi- how is it determined
not biologically
varies w factors like ethnicity
bmi and younger ppl
not very meaningful for them
use expected weight for height, adjusted for age
bmi underweight categories for u18s
< 85% underweight
< 70% dangerously underweight
overweight bmi
> 25 < 30
obese bmi
> 30
anorexia nervosa - diagnostic criteria, meet all of these features:
persistent restriction of energy intake leading to significantly low body weight
either: intense fear of gaining weight or becoming fat or persistent behaviour that interferes w weight gain (even tho signif low weight)
anorexia nervosa- diagnostic criteria, meet at least one of these features:
disturbance in the way one’s body weight or shape is experienced
undue influence of body shape and weight on self-evaluation
persistent lack of recognition of the seriousness of the current low body weight
subtypes of anorexia nervosa
restricting
bing-eating/ purging
critical thought re anorexia definition
ppl differ in set point for weight- limitation of using weight/bmi
various suggestions for bmi marker over years- e.g.: atleast 15% below, under 17.5, adjust for ethnic groups- all have conceptual and practical problems
athletes tend to count as overweight (more muscle)
ballerina and gymnasts sanctioned to b underweight
weight not a surefire indicator
weight and anorexia
better at spotting extreme examples
esp when seen b4 and after states
or weight loss is way beyond bmi of 17.5
hwvr might be starvation for other reasons e.g. the Dutch Hunger Winter
The Dutch Hunger Winter
1944-1945
famine
german occupied netherlands
esp in densely populated western provinces north of great rivers
bulimia nervosa- diagnostic criteria
recurrent episodes of binge eating
recurrent inappropriate compensatory behaviour in order to prevent weight gain
binges and compensatory behaviours both occur, on avg, at least 1x week for 3mo
self-eval unduly influenced by body shape/weight
not occur exclusively during episodes of AN
binge eating definition
eating, in a discrete period of time, more than most wld eat during similar period and under similar circumstances
a sense of lack of control, overeating
inappropriate compensatory behaviour in BN
self induced vomiting
misuse of laxatives, diuretics, other meds
fasting
excessive exercise
issues w bulimia nervosa definition
limitations of binge definition
-subjective (loss of control)
-objective (loss of control + excessive intake)
-what counts as excessive? over 2-3000?
defining compensatory behaviours
-is vomiting always self-induced?
-exercise for health or to control weight?
keep changing freq/often/amount of behaviours
binge eating disorder- diagnostic criteria
recurrent episodes of binge eating
marked distress re binge eating
bingeing at least 1x per week for 3mo (mean)
no purging or compensatory behaviours
episodes associated w 3 or more of 6 behaviours
binge eating
•eating, in a discrete period of time more than most people would eat during a similar period and under similar circumstances
•a sense of lack of control over eating during the episode
what must episodes be associated w in BED
at least three of the following:
•eating much more rapidly than normal
•eating until feeling uncomfortably full
•eating large amounts of food when not feeling physically hungry
•eating alone because of feeling embarrassed by how much one is eating
•feeling disgusted with oneself, depressed or very guilty afterward
when was binge ED first proposed
1980s, took many years to be adopted
accessibility of treatment w BED
most towards AN and BN so may be more difficult to access
critical thghts of BED definition
same as BN- issues defining binge
recent formal diagnosis (only formalised in 2013 w DSM-5) → so still some debate re definitions (number of binges, over how long)
need to understand motivation for bringing in this category
motivation for bringing in BED category
genuine distress and need for treatment
access to insurance funding for clinicians as way of treating a lot of overweight/obese patients
name for eating disorders which are atypical
other specified feeding and eating disorders (OSFED)
what was OSFED previously known as
EDNOS
OSFED definition
present w many symptoms of other EDs but do not meet full criteria for diagnosis
significant EDs
why were OSFED introduced
clinical reasons in USA- need diagnosis for insurance to pay for treatment and services
also to help progress research by better defining group
OSFEDs
atypical anorexia nervosa
atypical bulimia nervosa
atypical binge eating disorder
purging disorder
night eating syndrome
atypical anorexia nervosa
despite significant weight loss, individual’s weight is within or above normal range
atypical bulimia nervosa
of low frequency and/or limited duration
atypical binge eating disorder
of low frequency and/or limited duration
ARFID
avoidant/restrictive food intake disorder
ARFID- who
primarily but not exclusively children and young ppl
ARFID- criteria
disturbance in eating or feeding
-substantial weight loss/lack of weight gain
-nutritional deficiency
-dependence on supplements
absence of typical ed beliefs abt food or fear of weight gain
replacing and extending what was called selective or fussy eating
subtypes of ARFID
sensory-based avoidance
lack of interest
food associated w fear-evoking stimuli
refusal of food intake based on smell, texture, colour, brand, presentation
sensory based avoidance ARFID
what is the lack of interest in in ARFID
in consuming food or tolerating it nearby
how have fear evoking stimuli developed in ARFID
thru a learned history
effective ARFID treatments
primarily behavioural, focusing on anxiety/exposure
Fairburn et al (2003): criticism of eating disorder diagnosis
diagnosis of specific eating disorders does not do what it should
evidence for Fairburn et al . (2003)’s criticism
diagnosis of specific EDs does not do what it shld:
40-50% of cases do not fit neatly into diagnoses
atypical cases (OSFED) are single largest group
many fail to stay in one diagnosis
does not even indicate best treatment
as consequence to Fairburn et al. (2003)’s criticism, what is happening?
something of a shift away from rigid diagnoses- transdiagnostic model
Fairburn et al., (2003), Waller, 1993: eating disorders
transdiagnostic model
the underlying biological causes and consequences of EDs mean the following must be considered:
co-occuring psych problems
anxiety disorders (ocd, social)
depressed mood (low serotonin)
complex emotional and relational needs (personality disorders (anxiety and impulsivity based))
alcohol and substance use (alc as higher risk)
high mortality rates of EDs due to range of problems, incl:
•cardiac complications
•muscular weakness (including cardiac failure)
•osteoporosis
•liver damage
•oesophageal tearing
•fainting
incidence definition
number of new cases in set window of time
prevalence definition
number of current cases (point …) or number of people who have had the problem over the past year (annual …) or case over lifetime (lifetime …)
types of prevalence
point
annual
lifetime
why is it hard to calculate ed incidence
slow onset + secrecy + slow diagnosis
do we focus on prevalence or incidence of EDs and why
hard to calc incidence
can take a while to detect new cases
so focus on prevalence
prevalence rates- Beat (2012)
est about 750,000 in UK
c.1% of population
prevalence rates- Beat (2012)
prevalence - issues
depends on assumptions made
most focus on young, female population (14-30yo)
lifetime prevalence of AN (van Eeden et al., 2021)
4% women
0.3% men
lifetime prevalence of BN (van Eeden et al., 2021)
3% women
1% men
lifetime prevalence of BED (Galmiche et al., 2019)
2.8% women
1% men
what does Galmiche et al., 2019 indicate
OSFED highest lifetime prevalence
highest lifetime prevalence
OSFED Galmiche et al., 2019
Silen & Rahkonen, 2022
in western cultures, binge eating lifetime prevalence up to 6.1% in women and 0.7% of men
medical records revises and case numbers of EDs- can they tell us number of cases?
no, only say how many were spotted not how many there were
beware reports re epidemics and rocketing numbers- cld be raised awareness
gps miss cases even where v undeweight and esp if person is not young, white, and female
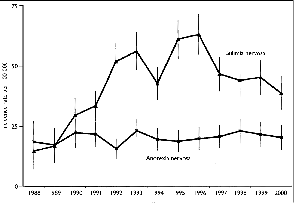
what is happening year
seems like epidemic of EDs
acc bc more awareness being raised (Currin et al., 2005)
not abt new cases
what is related to increasing identifcation and prevalence of EDs
westernisation
Curacao study
showing more cases among non-whites in recent years (Hoek, 2006)
Fiji study (Becker et al., 2011)
clear link w prevalence to introduction of western media
both TV and more social network based exposure e.g. home DVD
objective of Curacao study
AN once thght to only occur in affluent societies, cases now been documented globally so, to examine whether AN emerges in societies undergoing socioeconomic transition
what did authors study in Curacao study
incidence of AN on Caribbean island Curacao
method Curacao study
contacted full range of community health service providers, incl dieticians, school counsellors, all 82 GPs
studied inpatient records for 84,420 admission to Curacao General Hospital and two private hospitals in 1995-1998
probable incident subjects were interviewed
results of Curacao study
incidence rates in 1995–1998 per 100,000 person-years for AN were 1.82 (95% confidence interval [CI]=0.74–2.89) for the total population
were 17.48 (95% CI=4.13–30.43) for the high-risk group of 15–24-year-old females.
no cases were found among the majority black population.
for mixed and white population, the incidence rate per 100,000 person-years for anorexia nervosa was 9.08 (95% CI=3.71–14.45)
Curacao study: incidence rates in 19__-____ per 100,000 person-years for AN were ____ for the total population
1995-1998
1.82
Curacao study: incidence rates in 1995-1998 per 100,000 person-years for AN were ____ for the high-risk group of __________
17.48
15-24 yo females
Curacao study: how many cases of AN found in majority Black population?
zero
Curacao study: incidence rates in 1995-1998 per 100,000 person-years for AN were ____ for the mixed and white population
9.08
Curacao study: conclusions
overall incidence of AN much lower than in affluent societies of USA and Western Europe
sociocultural factors appear to be associated w differential incidence rates of AN
incidence of AN amongst majority black population is zero
incidence among minority mixed and white ppl similar to that of USA and Netherlands
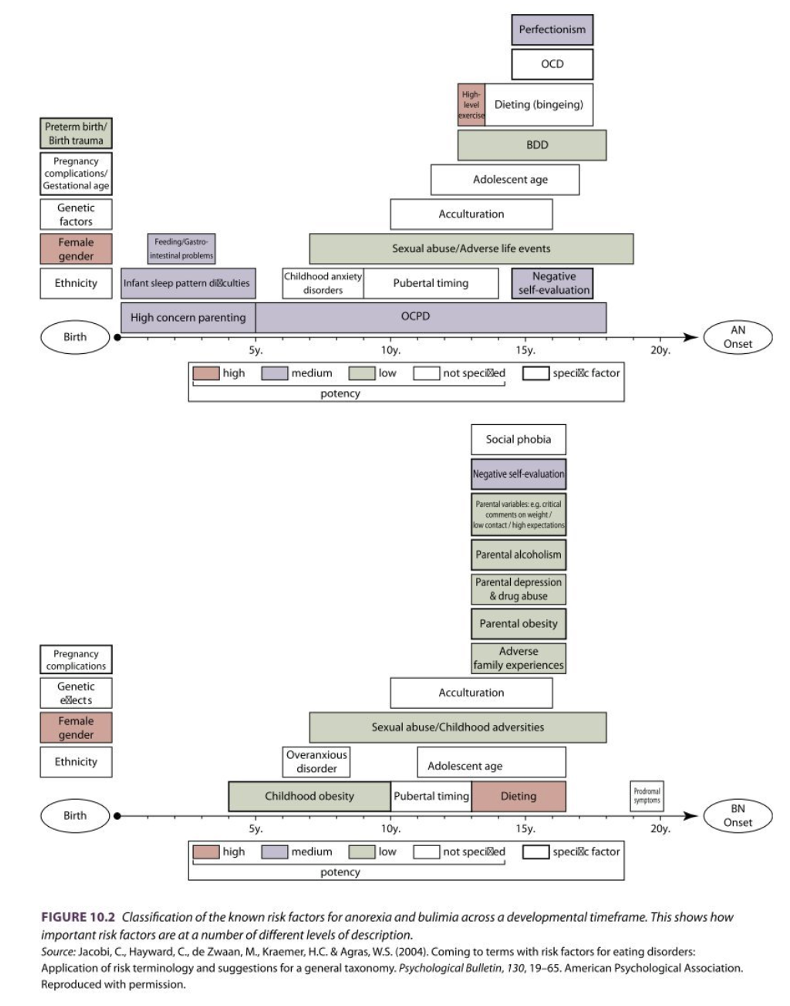
causation of EDs
lots of sociocultural and neurobiological factors
neurobiological factors + clarity
unclear
hypotheses more common than acc evidence
genetics
- some evidence e.g. twin studies
-dk where responsible genes r
-are genes responsible for ed.s directly or for other risk factors. e.g. perfectionism, serotonin mechanisms that predispose to impulsivity or compulsivity
hypothalamic damage, preventing hunger?
-but AN patients report lots of hunger
issues underpinning identification of neurobiology in EDs
exacerbated by issue of causality
does dysfunctional biology result in ED or does ED result in dysfunctional biology
which starvation effects seem to go away when a person eats
mood deficits
cognitive deficits
social isolation
behavioural inactivation
→ important re treatment planning
important questions re ed maintenance
•If we cannot identify clear, universal pattern of predictors, can we identify what keeps the problem going once it has started?
•Eating disorders can and do last for years, so how to stop them as soon as possible?
•If we identify maintaining factors, can we interrupt them?
cognitive patterns common in EDs
low self esteem
negative self attribution
perfectionism
what do cognitive patterns each have in EDs
self-maintaining cycle
self maintaining cycle, low self esteem
means do not look for positive things about ourselves. so remains that way
self maintaining cycle, high perfectionism
meaning we avoid things wrong, rather than we are good at anything, so have to keep striving
two main central belief systems/ cog patterns
broken cognitive link
overvaluation
broken cognitive link between…
eating and weight; driving restriction, then binging, then gaining weight, then restricting
what does broken cog link have
strong cognitive dissonance element
Waller and Mountford (2015)
assumption even a small amount of eating will lead to disproportionate weight gain
assumption that any weight gain will be uncontrollable and unstoppable
therapeutic task is help rebuild broken cog link
assumptions re broken cog link by Waller and Mountford 2015
even small amt of eating will lead to disproportionate weight gain
any weight gain will be uncontrollable and unstoppable
what do Waller and Mountford 2015 say the therapeutic task is
help rebuild the link
overvaluation…
of appearance and weight as defining ourselves as being acceptable people
what are safety behaviours
behaviours that calm us temporarily when we are anxious but where the long term consequence is that we feel worse