cerebral cortex
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
overview of function:
cerebral cortex:
cognition:
***what is cognition? what functions are considered part of cognition? what is metacognition? what is functional cognition?
cerebral cortex: “the seat of intelligence” (considered the highest level of the CNS)
basic sensorimotor, visual and auditory processing
***cognition: ***information-processing functions carried out by the brain that include:
***attention
***memory
***executive functions: planning, problem solving, self-monitoring, self-awareness, & meta-cognition
*** meta-cognition= ***higher order thinking: enabling ***understanding, analysis, and control of one’s cognitive processes
***comprehension of language and ***formation of speech
***calculation abilities
***visual perception
***praxis (engaging, applying, exercising, realizing, or practising ideas)
can be conscious or unconscious
***functional cognition: how an individual ***utilizes and integrates his or her thinking and processing skills to ***accomplish everyday activities in clinical and community living environments.
overview of structure:
***know the structure of the cerebral cortex, including the types of fibers and what they connect (e.g., projection fibers connect the cortex with subcortical structures such as the spinal cord and brainstem, etc.)
***know the general functional categories of the cerebral cortex
***what areas of the cortex are considered motor areas?
review:
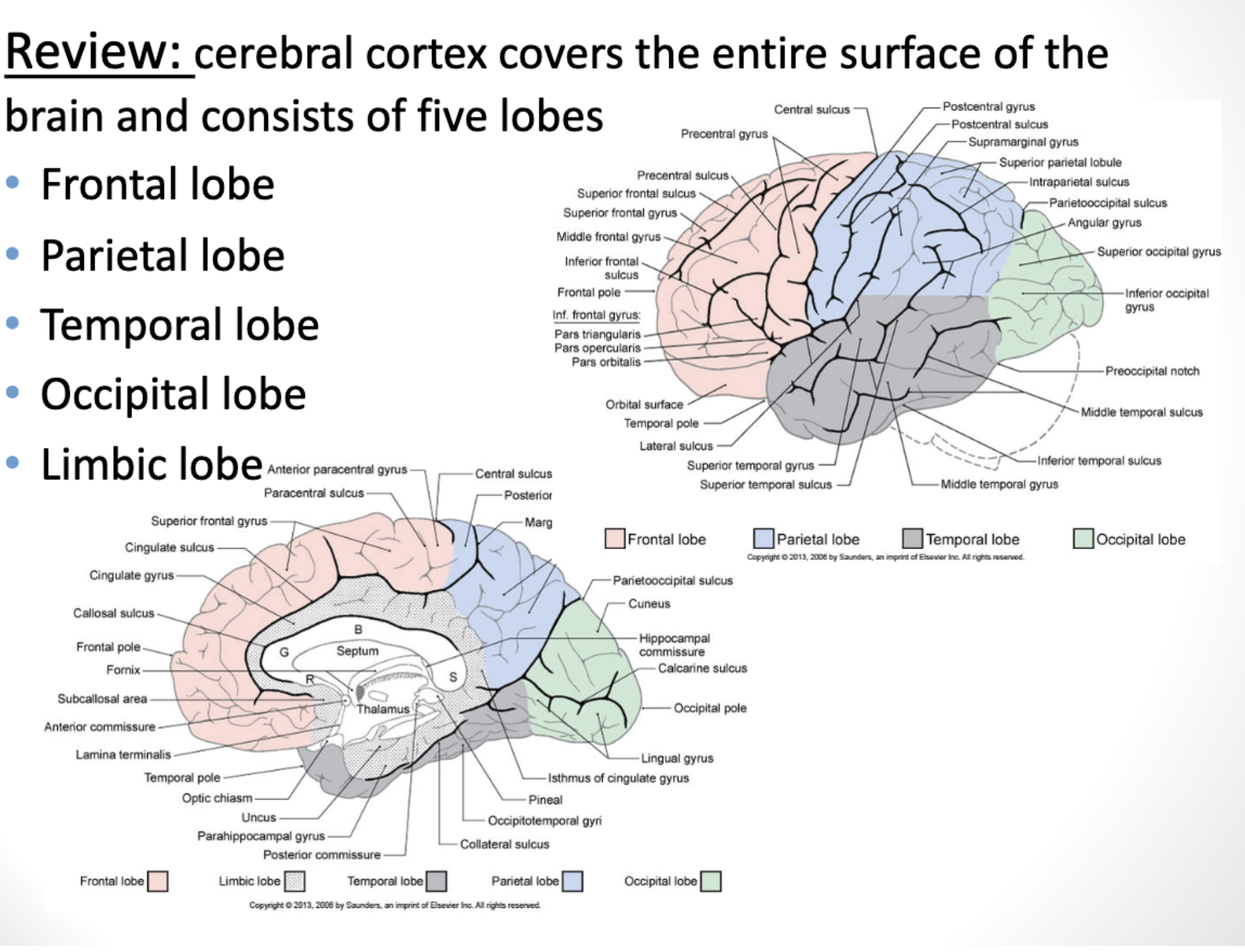
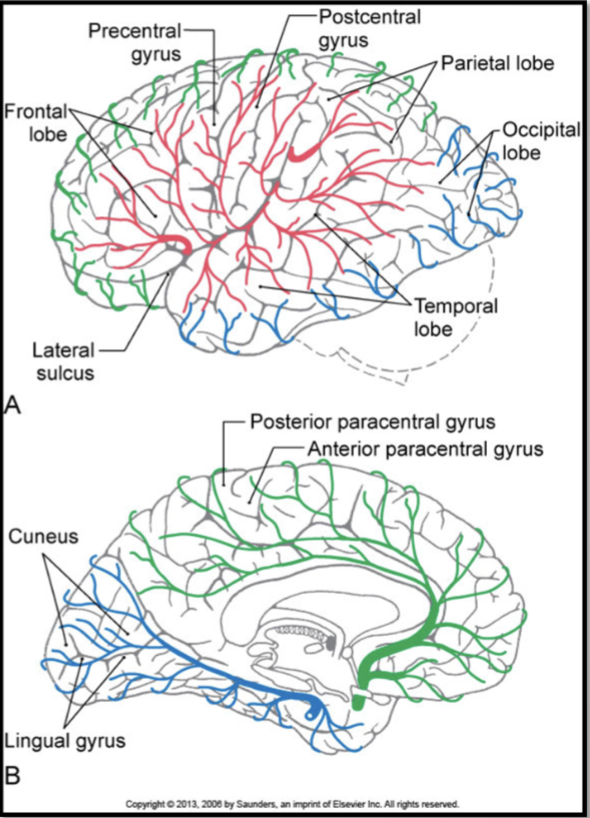
cerebral cortex ***covers the entire surface of the brain and consists of ***five lobes
***frontal lobe (red)
***motor!!! and ***executive functions
the ***motor areas of the cortex are primarily located in the ***frontal lobe, specifically in the areas surrounding the ***precentral gyrus
areas include…and are responsible for ***planning, ***initiating, and ***executing movements
***primary motor cortex
***premotor cortex
***supplementary motor area
***parietal lobe (blue)
***somatosensory processing and ***sensory integration
***temporal lobe (grey)
basic ***auditory processing
***emotional processing
***memory formation
***occipital lobe (green)
***visual functions
***limbic lobe (lighter gray when brain is opened up)
***memory learning and ***emotional processing
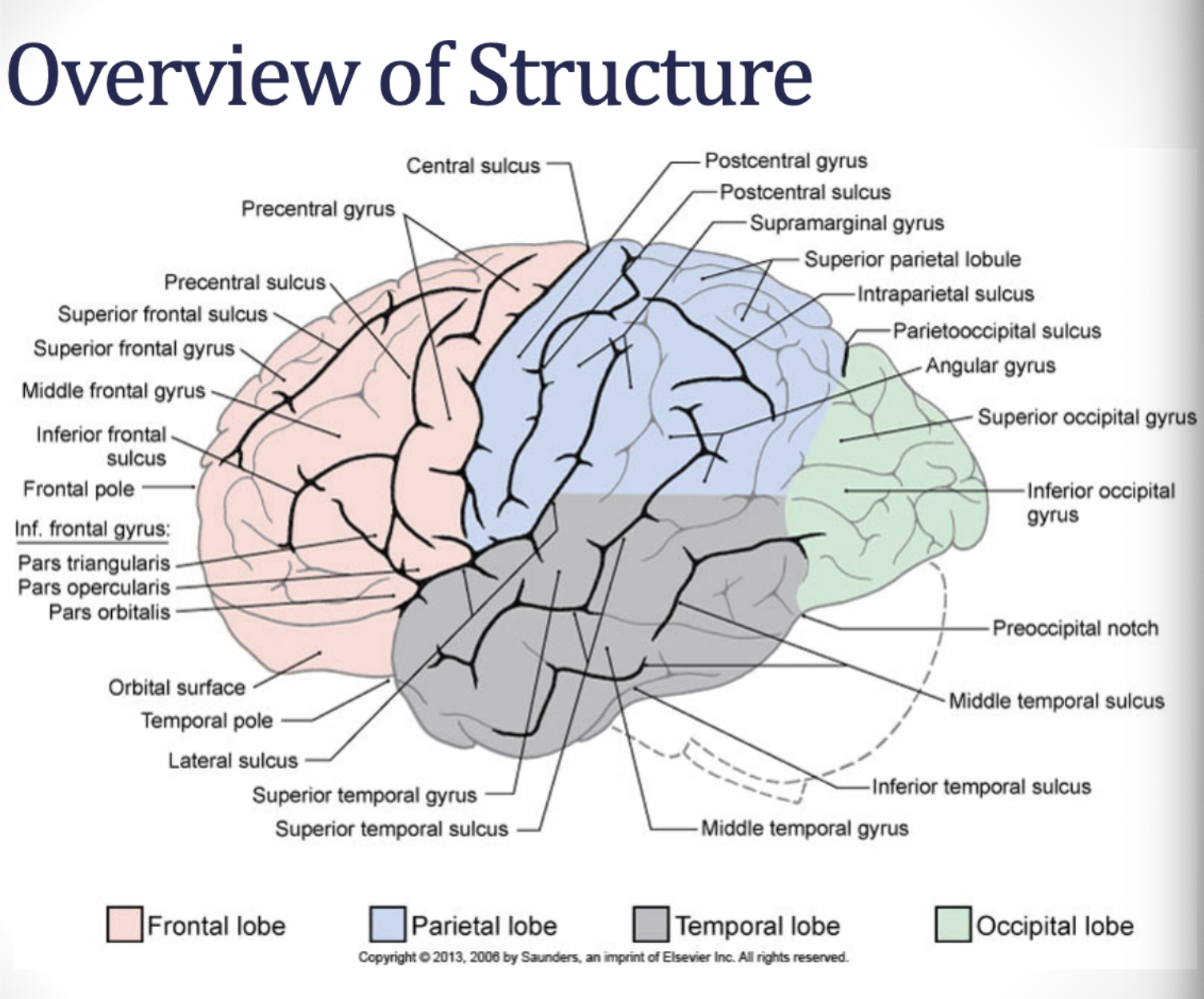
***central sulcus
***divides the ***frontal and ***parietal lobes
***precentral gyrus
in the ***frontal lobe
***postcentral gyrus
in the ***parietal lobe
***lateral sulcus
***divides the ***temporal lobe ***from the frontal and parietal lobes
parietooccipital sulcus
***divides the ***parietal lobe from the ***occipital lobe
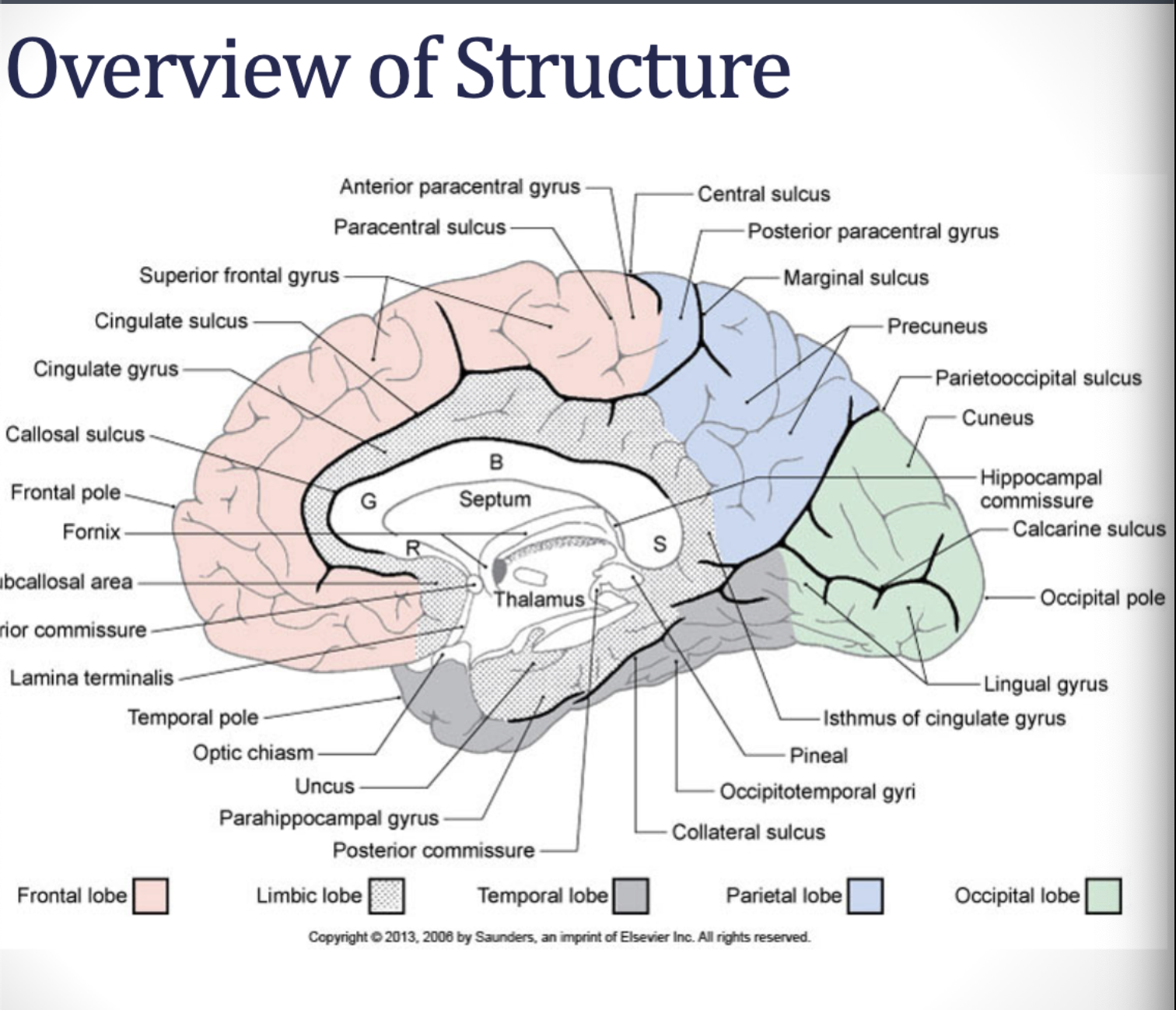
limbic structures
lobe is key for ***emotional processing
***cingulate gyrus
***parahippocampal gyrus
***uncus
***subcallosal area
overview of structure: ***know the structure of the cerebral cortex, including the types of fibers and what they connect (e.g., projection fibers connect the cortex with subcortical structures such as the spinal cord and brainstem, etc.)
projection fibers:
callosal/commissural fibers:
association fibers:
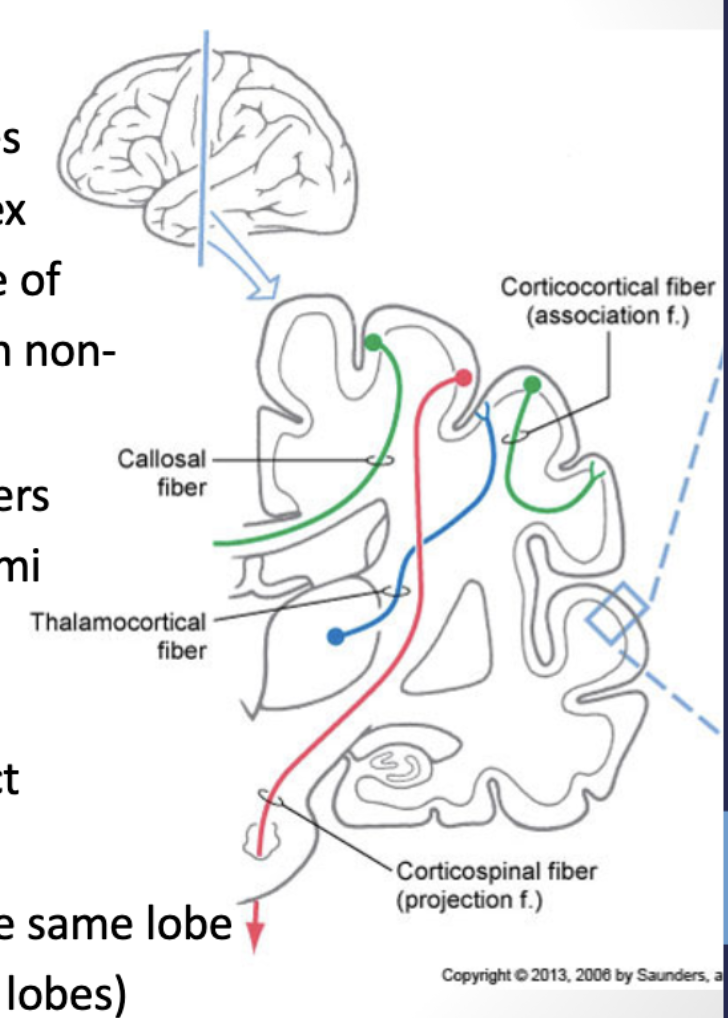
white matter: areas of the cortex are ***connected to each other and ***to subcortical structures via fiber bundles
***projection fibers: (ascending (blue) & descending (red))
these fibers ***project from cortical areas ***to subcortical structures (descending tracts, e.g., corticospinal tract, corticonuclear tract, etc.)
or from ***subcortical areas to the cortex (ascending fibers, e.g., thalamocortical fibers from the VPL, VPN, VA)
***thalamocortical fibers: main source of ***input to the cortex ***originating from non-cortical structures
***thalamocortical tract brings information ***from the thalamic nuclei ***to the association cortex- the ***main source of information to the cortex
***callosal/commissural fibers: (green)
these fibers connect areas of the cortex in ***one hemisphere with areas of cortex ***in the opposite hemisphere
e.g., ***corpus callosum: major neural pathway that connects homologous cortical areas of the ***left and right hemispheres
*studies show support for both theories, saying the cerebral cortex can serve both inhibitory and excitatory influences on the contralateral hemisphere
*some say they can also inhibit the other hemisphere (e.g., using right hand to reach, the left hemisphere is active and inhibits the right hemisphere transcollosal fibers)
after a stroke, it’s thought that there is excessive inhibition of the ipsilesional (affected) hemisphere by the contralateral (non-affected) hemisphere, resulting in poor functional outcomes
*some say the corpus callosum integrates information across hemispheres, serving as an excitatory function in inter-hemispheric communication
***anterior commissure connects the ***frontal and ***temporal areas
***hippocampal commissure connects the ***hippocampal structures
***posterior commissure connects the ***areas of the diencephalon
***association fibers:
these fibers connect ***areas of cortex ***within the same hemi-sphere
***short fibers connect ***cortices of gyri of the ***same lobe
e.g., premotor cortex with the motor cortex and the frontal lobe
& ***long fibers connect ***cortices gyri of ***adjacent/different lobes
e.g. visual system has dorsal and ventral streams of vision
dorsal stream: connects occipital to parietal lobes
ventral stream: connects occipital to temporal lobes
overview of structure: ***know the structure of the cerebral cortex, including the types of fibers and what they connect (e.g., projection fibers connect the cortex with subcortical structures such as the spinal cord and brainstem, etc.)
neocortex-
2 major cell types
***neocortex – consists of six layers (I-VI)
***majority of the cortex
***2 major cell types
***pyramidal neurons:
***one apical dendrite and ***multiple dendritic trees; these ***project OUT of the cortex ***to other regions of the brain and ***to the spinal cord
***granular neurons:
***smaller dendritic trees and ***shorter axons;
***REMAIN in the cortex – considered interneurons and are responsible for ***communication between the cell layers
neocortex: ***know the structure of the cerebral cortex, including the types of fibers and what they connect (e.g., projection fibers connect the cortex with subcortical structures such as the spinal cord and brainstem, etc.)
layer:
composed of:
role:
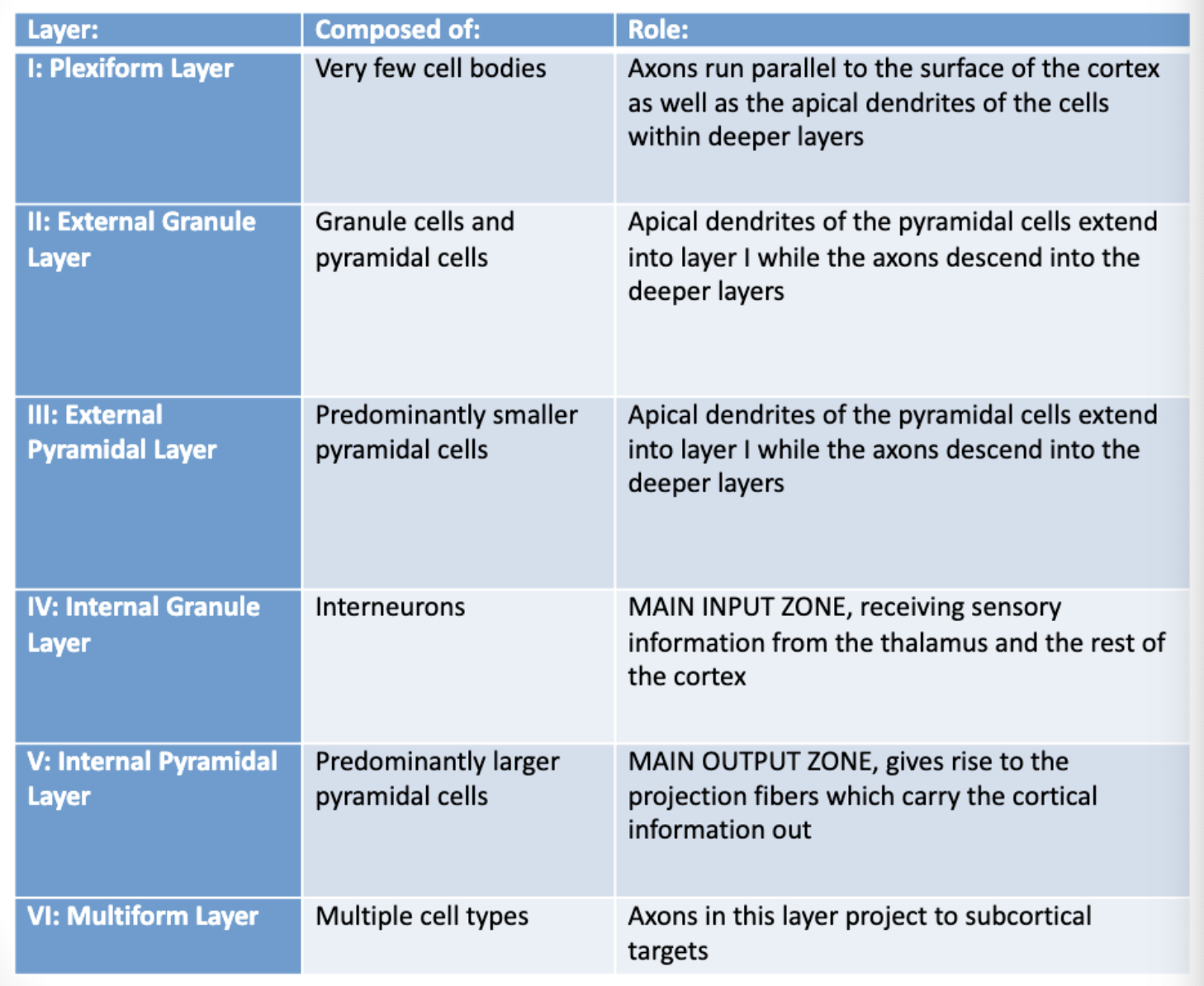
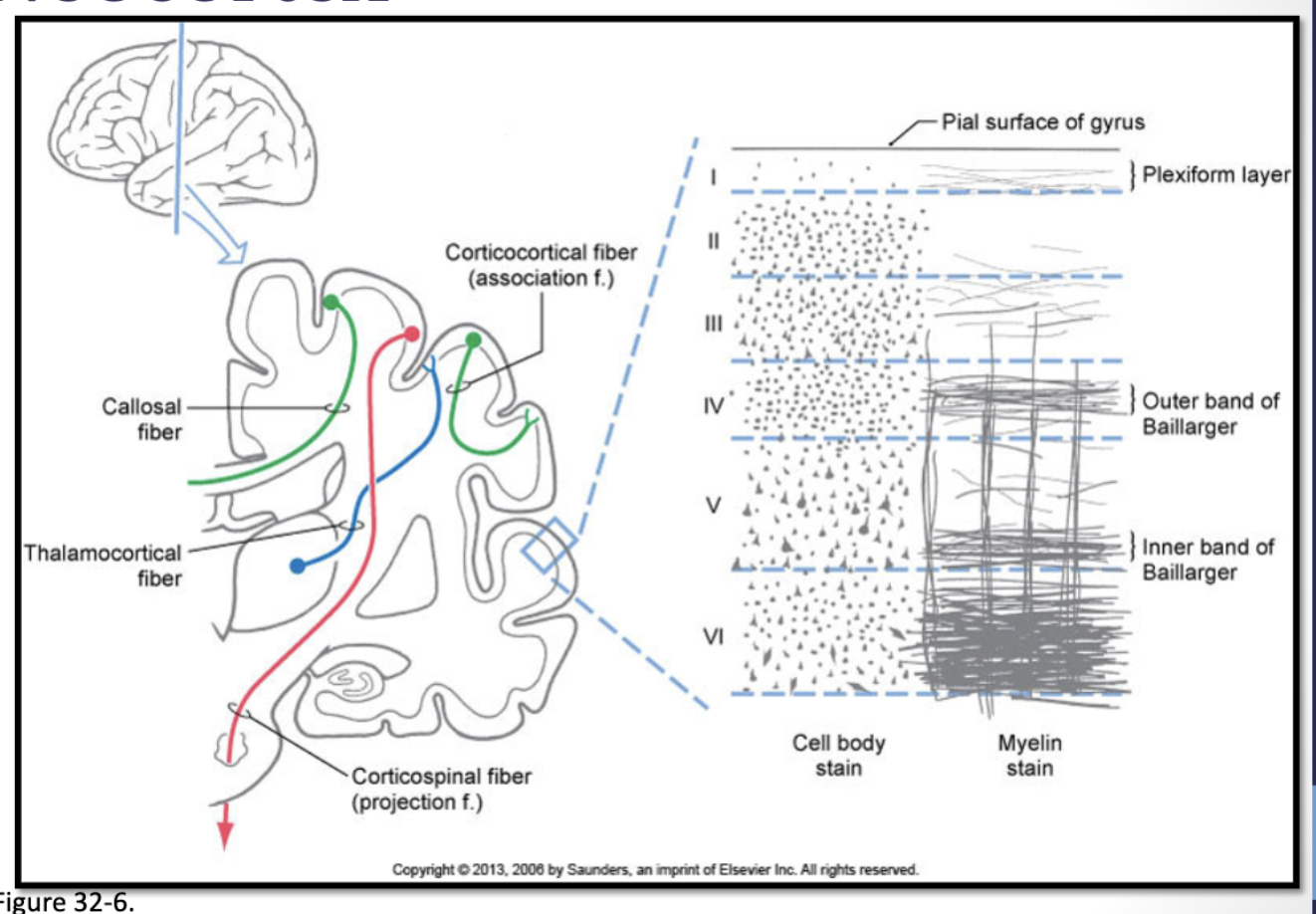
6 layers of the neocortex
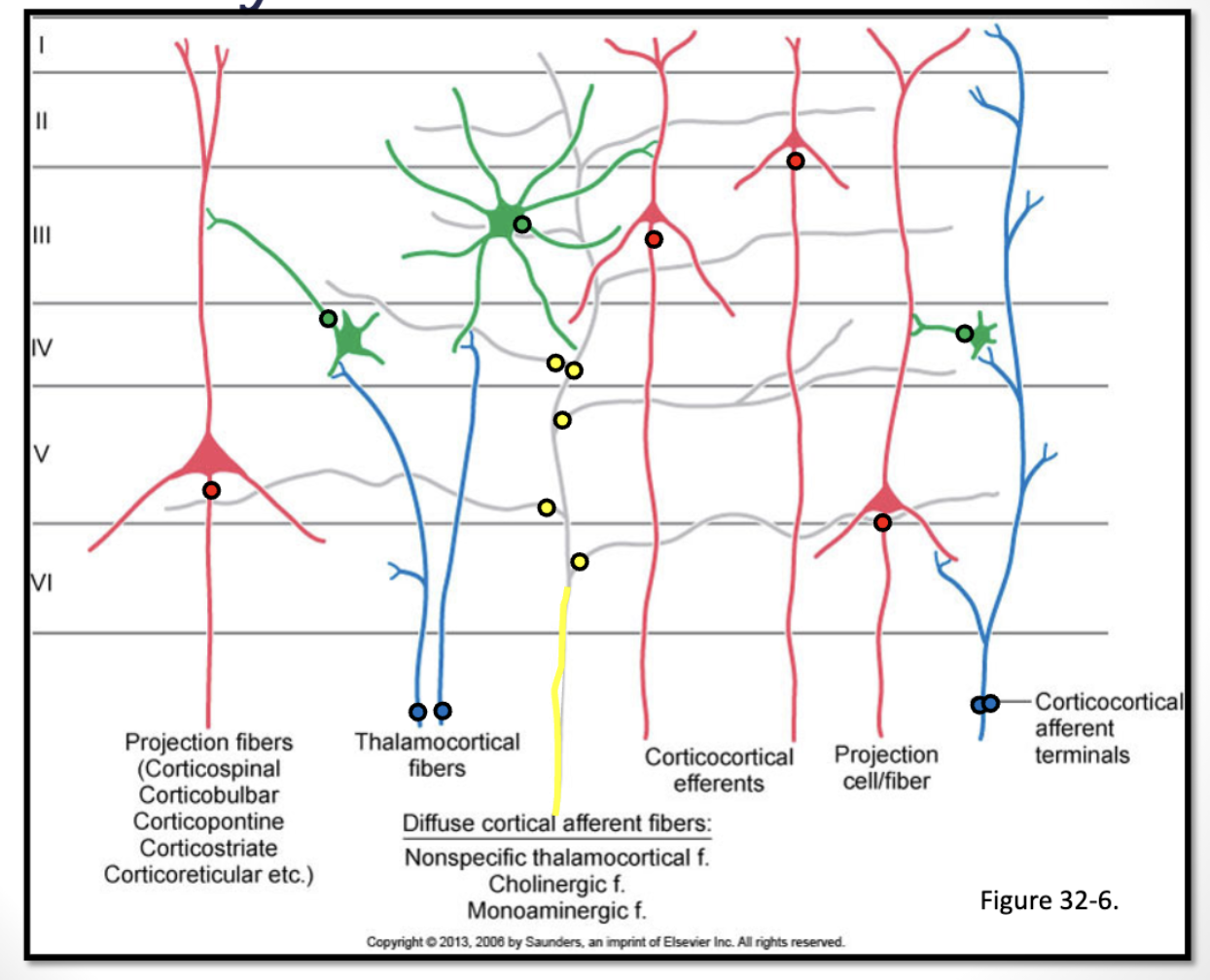
circuitry
intrinsic circuitry
afferent fibers:
local circuit neurons:
efferent fibers:
***know the structure of the cerebral cortex, including the types of fibers and what they connect (e.g., projection fibers connect the cortex with subcortical structures such as the spinal cord and brainstem, etc.)
intrinsic circuitry: high degree of convergence (where information comes into a neuron) and divergence (information gets transmitted out of the neuron) within the neural circuitry of the cerebral cortex – allowing for complex integration of information
afferent fibers: bring input to the cortex
thalamocortical fibers (input from thalamic nuclei) – excitatory
cortico-cortical fibers – excitatory or inhibitory
diffuse inputs (e.g., ascending reticular activating system; raphe nuclei) – excitatory (contain projections concerned with the regulation of cortical excitability, arousal, sleep, and wakefulness)
e.g., raphe nuclei, which deals with serotonin, helps modulate the brain under stressful conditions
local circuit neurons: processing & integrating information (layer IV)
excitatory and inhibitory interneurons
efferent fibers: pyramidal cells – excitatory output from the cortex
cortico-cortical fibers (i.e., association or callosal – layers II & III)
e.g., “what” stream of vision: connections between the visual cortices and the temporal cortices
e.g., “where” stream of vision: connections between the visual cortices and the parietal cortices
projection fibers (layer V)
e.g., corticospinal, corticonuclear, corticorubral, corticopontine, corticoreticular tracts
image
***6 layers
***layer II & ***layer III: have ***pyramidal cells that ***output to the ***cortico-cortical projections
***layer IV: major ***input zone of the cortex
***thalamocortical fibers and ***cortico-cortical fibers come in here
***layer V: major ***output zone
***gives rise to the projection fibers
blue
information comes in from afferent thalamocortical and cortico-cortical fibers
yellow
diffuse input from modulatory systems that can alter the excitability levels of the cortex
—> they synapse on the pyramidal cells in…
…green,,,
—> ,,,which output to the cortico-cortical connections; those synapse onto the,,,
red
,,,efferent projection fibers
—> which output the information from the cortex
== this ^ is constantly happening all over the cortex
histological organization: ***know the structure of the cerebral cortex, including the types of fibers and what they connect (e.g., projection fibers connect the cortex with subcortical structures such as the spinal cord and brainstem, etc.)
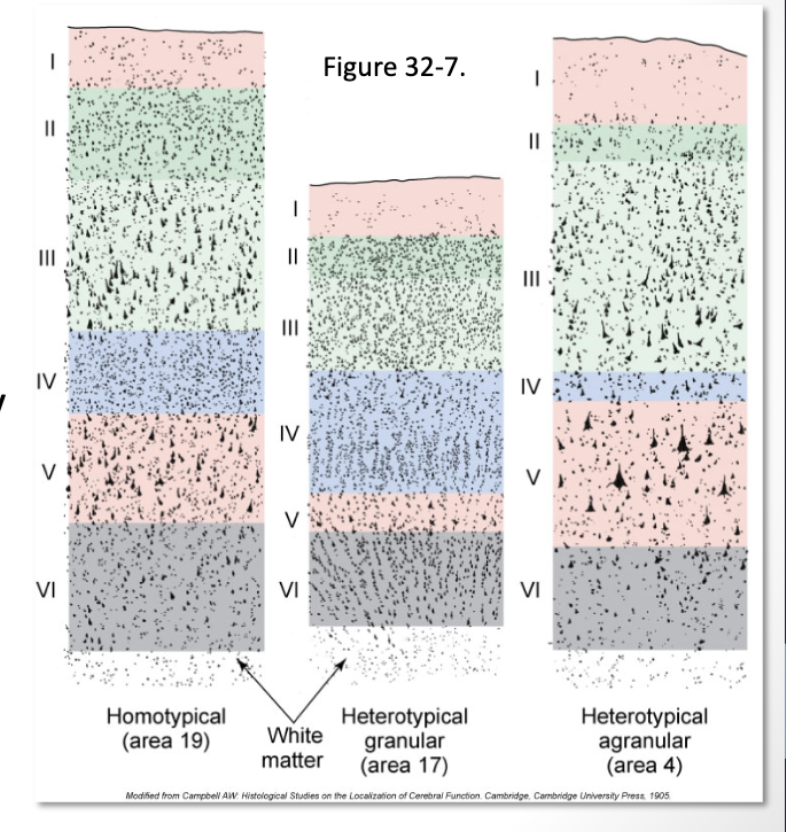
cytoarchitecture:
homotypical:
heterotypical:
cytoarchitecture: ***not every area of cortex has the same makeup- ***differs based on ***function
homotypical: all six layers are clearly and evenly represented- most areas of the cortex (1st column)
heterotypical: layers vary in thickness (2nd and 3rd columns)
granular cortex:
***layer IV (*where ***all the information is coming in) is especially ***thick
& ***layer V is ***thin
==> this is the ***primary sensory cortex
*the ***sensory cortex ***always gets a lot of information in
agranular cortex:
***layer V (*where ***all the information is getting sent out) is especially thick
& ***layer IV is ***thin
==> this is the ***primary motor cortex
*this ***primary motor cortex ***always gets a lot of information out
brodmann’s areas
47 different areas based on the cytoarchitecture of the cortex
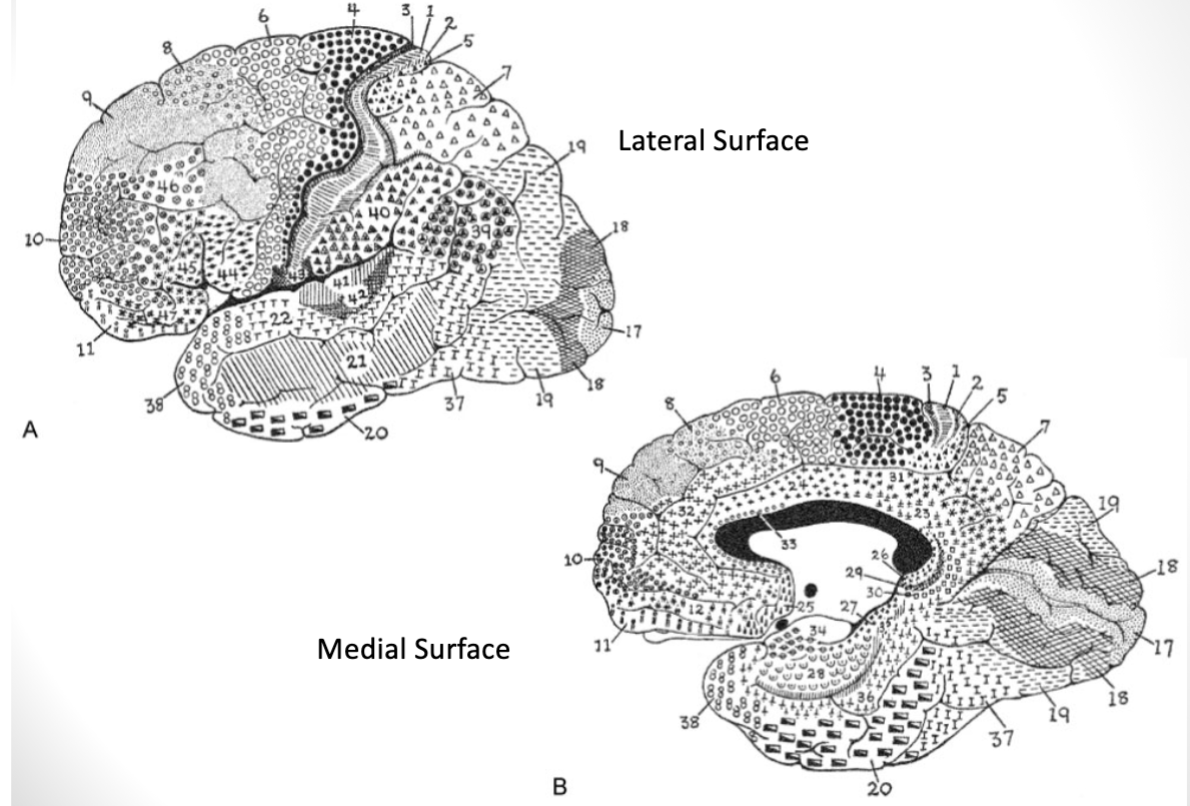
brodmann’s areas
***frontal lobes:
***know the location and function of the following:
***primary areas of the cortex
areas 4, 6, 8-12, 32, & 44-47
***primary motor cortex: area 4
***what areas of the cortex are considered motor areas?
***premotor & SMA (motor planning): area 6
***what areas of the cortex are considered motor areas?
***frontal eye fields: area 6 & 8
***broca’s area (speech): areas 44 & 45
***prefrontal and ***orbitofrontal 8-12; 32; 45-47
brodmann’s areas
***parietal lobes:
***know the location and function of the following:
***primary areas of the cortex
areas 3, 1, 2, 5, 7, 39, 40, & 43
***primary somatosensory cortex: areas 3, 1, 2
***posterior parietal cortex:
***visuospatial functions
***superior parietal cortex:
areas 5 (***somatosensory association cortex),
7 (***dorsal stream of vision – “where” & “how” stream of vision)
***inferior parietal cortex: areas 39 (angular gyrus) & 40 (supramarginal gyrus)
associated with ***wernicke’s area
brodmann’s areas
***temporal and ***occipital lobes:
***know the location and function of the following:
***primary areas of the cortex
areas 17-22, 36-38, 41 & 42
***primary auditory cortex: area 41 & 42
***primary visual cortex: area 17
***visual and ***auditory association cortices: areas 18-22
***wernicke’s area: 22
***ventral stream of vision (“what” and “who” stream of vision): area 37
brodmann’s areas
***limbic lobes:
***know the location and function of the following:
***primary areas of the cortex
areas 23-31 and 33-35
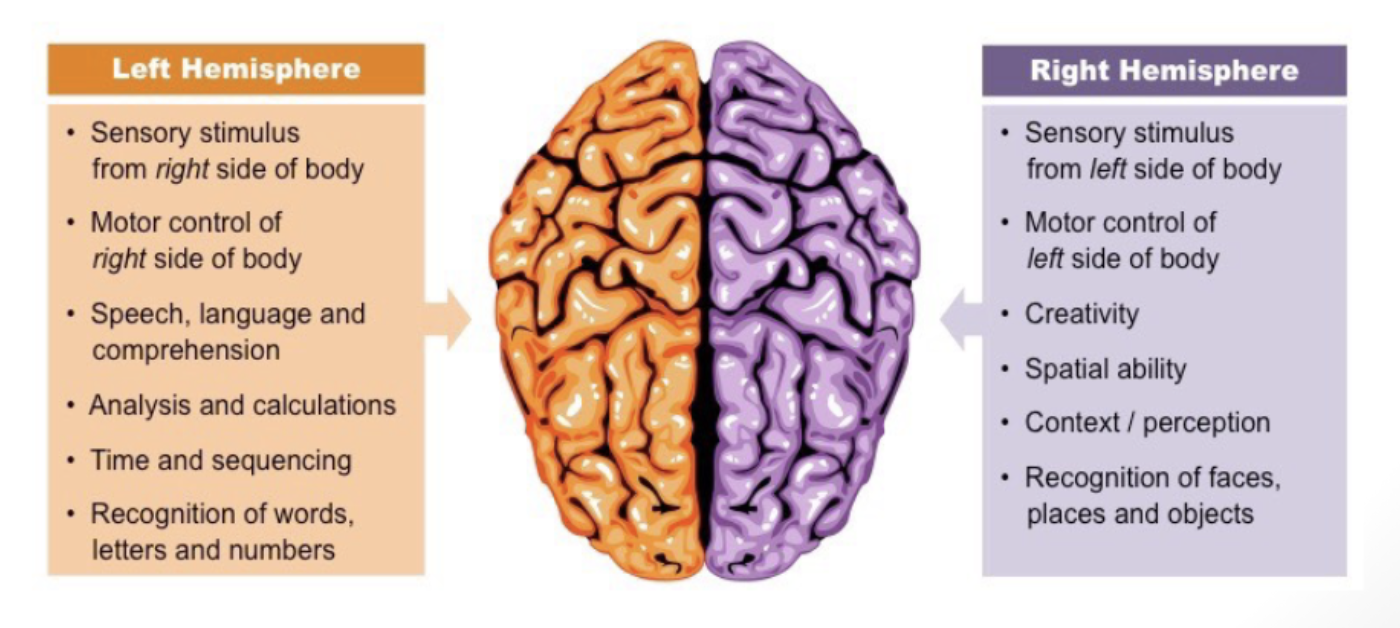
lateralization
***what is lateralization? what is the right hemisphere specialized for? what is the left hemisphere specialized for?
generally speaking, ***RIGHT BRAIN is big picture; ***LEFT BRAIN is detail-oriented
***right brain is going to help explain context
***left brain is going to help more with the ***routines of your day but ***not necessarily the full understanding
***motor and sensory functions pertaining to one side of the body ***are controlled by the opposite hemisphere (right side of brain controls the left side of the body)
***information from one visual field is ***processed by the opposite hemisphere (right side of the brain processes visual information from left side of environment)
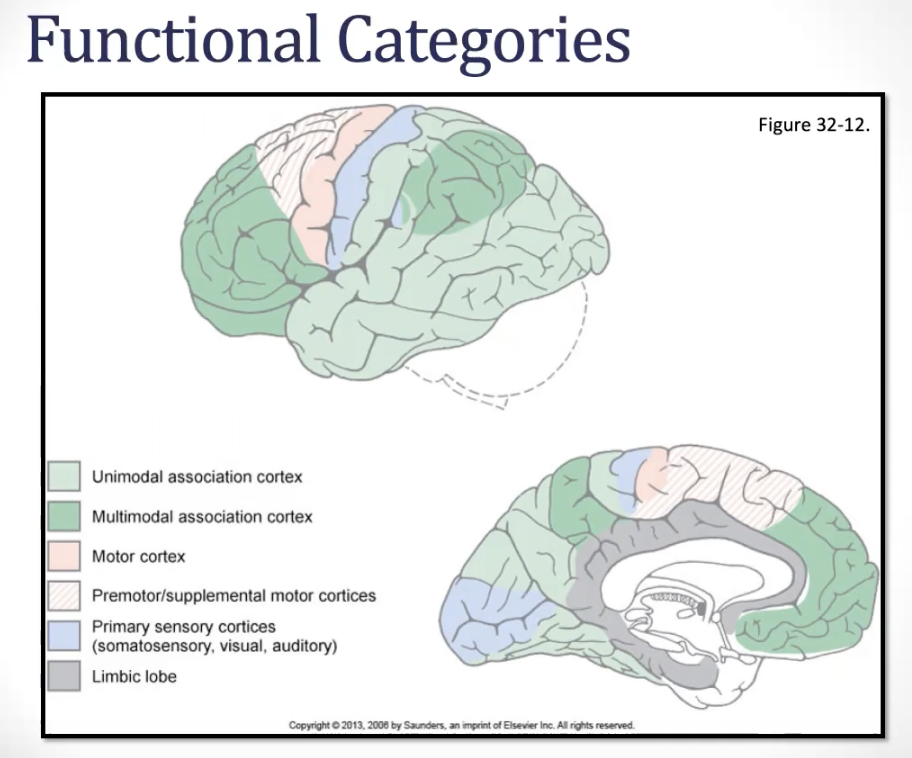
functional categories: ****know the location and function of the following:
motor:
primary sensory:
association areas:
***unimodal association:
***multimodal association:
***primary motor:
***primary motor cortex,
***supplementary motor area and the
***premotor cortex
***primary sensory:
***primary somatosensory cortex,
***primary visual cortex and
***primary auditory cortex
association areas: (majority of the cortex)
***unimodal association= ***areas that are adjacent and ***related to primary areas/primary sensory cortices
***information is processed from a single sensory modality (like sight or sound) in the primary region and is ***conveyed to the association areas via cortico-cortical fibers
***location:
***near the primary sensory cortices
e.g., ***visual association cortex, which surrounds the ***primary visual cortex in the ***occipital lobe & ***inferior temporal gyrus- it’s here that the basic elements of ***visual perception are integrated into an ***overall perception of the visual world
e.g., ***auditory association cortex near the ***primary auditory cortex in the ***temporal lobe
e.g., ***somatosensory association cortex
***function:
***process sensory inputs from the primary areas, ***integrating information within a single sensory modality (e.g., different visual characteristics like color, shape, and movement)
***multimodal association= these are ***large areas of cortex that ***receive information from several different sensory modalities and ***create a broader, more complete ***understanding of ourselves and our environment
***location:
***generally located more posteriorly in the cortex, such as the…
***posterior parietal cortex
and ***prefrontal cortex
***function:
***integrate information from ***different sensory modalities and other brain areas, contributing to…
e.g., ***…higher cortical functions, such as ***language, ***visuo-spatial relationships, ***praxis, ***executive functions
also play a role in ***planning and ***executing motor actions
primary cortices: ***know the location and function of the following: primary areas od the cortex
***primary motor cortex (PMC)
***localized to the ***precentral and ***anterior paracentral gyri of ***frontal lobe
somatotopic organization: motor homunculus
***function: ***sends motor output to the ***opposite side of the body (via the corticospinal and corticonuclear tracts)
lesions of this area would result in upper motor neuron signs- contralaterally
primary cortices: ***know the location and function of the following: primary areas od the cortex
***primary somatosensory cortex (PSC)
***localized to the ***postcentral and ***posterior paracentral gyri of ***parietal lobe
somatotopic organization: sensory homunculus
***function: ***receives sensory input from the ***opposite side of the body (via the PCMLS and ALS)
lesions of this area result in decreased awareness of sensory stimuli &/or poor localization of sensory stimuli - contralaterally
primary cortices: ***know the location and function of the following: primary areas od the cortex
***primary visual cortex (PVC)
***localized to the ***upper and lower banks of the ***calcarine sulcus in the medial ***occipital lobe
retinotopic organization in PVC
***function: receives ***visual input from the ***contralateral visual field
lesions of this area result in visual field deficits – contralaterally; the nature of which depend on the exact location of the lesion
primary cortices: ***know the location and function of the following: primary areas od the cortex
***primary auditory cortex (PAC)
***localized to the ***transverse temporal gyri located deep in the ***lateral sulcus
tonotopic organization in PAC
***function: ***receive auditory input from both ears
lesions of this area result in decreased perception of sound but not a complete loss of hearing limited to one side or the other
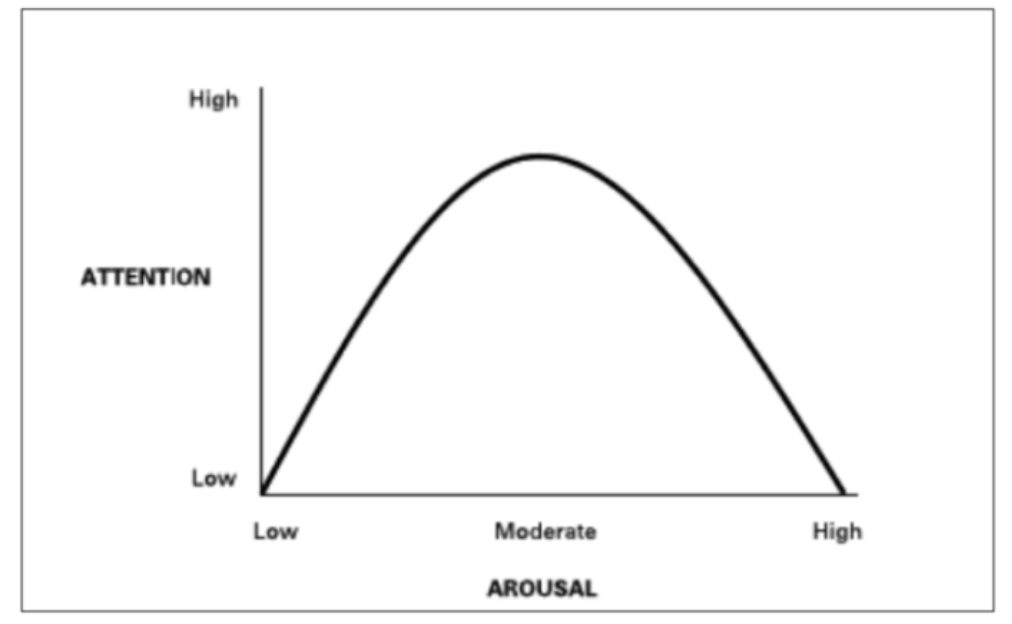
higher cortical functions: ***what is attention?
arousal and attention
== ***ability to focus on and selectively process specific information from the environment while filtering out irrelevant details
***arousal/alertness is the first step
starts with the reticular activating system; if a person is ***not alert
enough, there can be ***no attentionconversely, if a person is ***over-aroused/hyper-alert, ***attention will also be affected
attention is ***highest at moderate levels
higher cortical functions:
***what is atttention?
***what are the different types of attention?
***what areas of the brain are thought to be important for mediating attention?
arousal and attention- attention (__ and __ association areas)
attentional capture
selective attention
sustained attention
divided attention
alternating attention/task-switching
***frontal; ***parietal
***attentional capture – ***automatic or reflexive orienting to a stimulus
***selective attention – ***goal-directed focus of attention with the ability to ***ignore irrelevant stimuli
e.g. listening to lecture even if there are loud car noises outside
show increased activity of the ***anterior cingulate, ***right dorsolateral, ***prefrontal, and ***right parietal cortices
***sustained attention – ability to ***maintain vigilance over time
e.g. listening to lecture over the course of an hour
***divided attention – ability to ***perform two or more tasks at the same time, or ***process two or more sources of information at the same time
e.g. listening to lecture and shopping online at the same time
***alternating attention/task-switching – ***rapidly switching between different skills/tasks/cognitive sets
e.g. reading a recipe while cooking- back and forth
higher cortical language
***where are expressive and receptive language functions localized in the cortex?
***know the cortical structures (including hemisphere) involved in the processing of language comprehension and expression
***know all the types of aphasia presented in lecture- damage to which areas of the brain causes which types of aphasia? what is the blood supply to each of these regions?
language (__ and __ ***association areas)
***frontal; ***temporal
language is the faculty of communication to describe things, events, and to express ideas
language is a function of multimodal sensory and motor processing areas and includes speaking, reading and writing
when we talk about hemispheric dominance of language, the hemisphere that controls language is considered the dominant hemisphere
***almost all right-handers (~98%) and 50-70% of left-handers are ***left-cerebral dominant
in brain lesions, ***which impact language, ~95% of those cases are ***left-hemisphere involvement
***right hemisphere is involved in language in regards to the ***prosody of speech (rhythm, tone, stress, etc.)
aphasia is a disturbance in the understanding or the formulation of language not due to hearing/vision/motor impairments
***where are expressive and receptive language functions localized in the cortex?
***know the cortical structures (including hemisphere) involved in the processing of language comprehension and expression
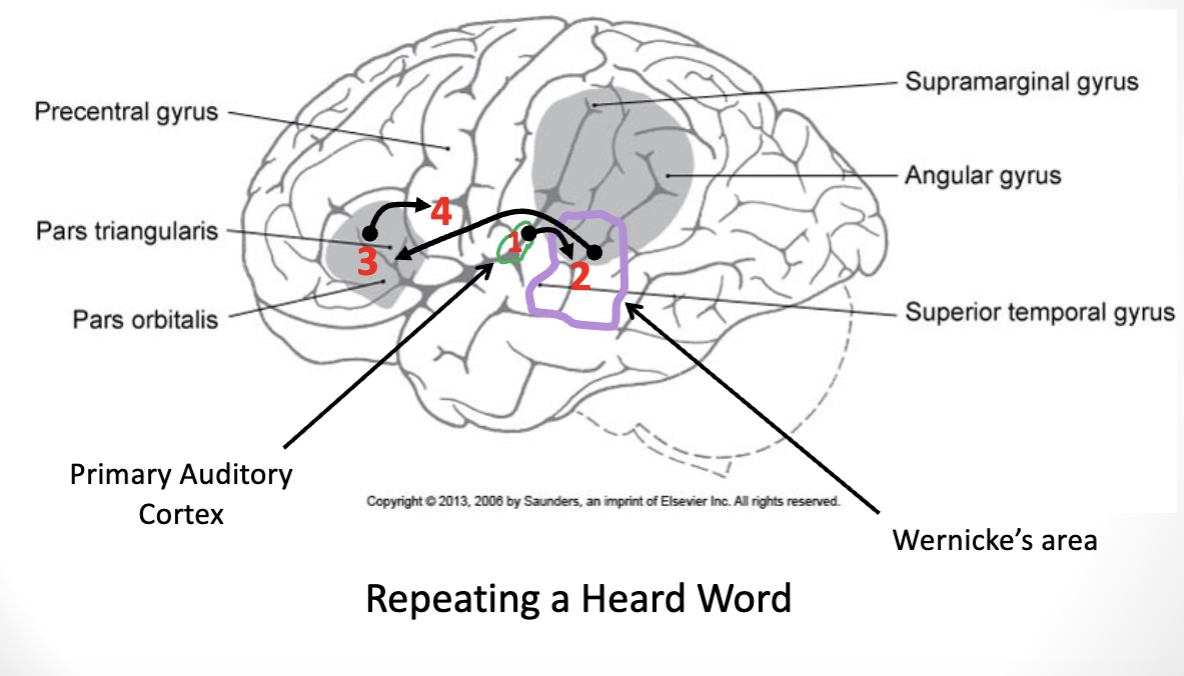
repeating a heard word
upon ***hearing a spoken word, the ***primary auditory cortex receives the information
information ***travels to wernicke’s area, in the ***temporal lobe (***where speech is understood)
***information gets sent via the ***arcuate fasciculus ***to the pars orbitalis, in the ***inferior frontal gyrus of the frontal lobe (i.e., ***broca’s area)
where ***motor plan for speech is formed and ***delivered to the,,,
,,,***primary motor cortex, where ***speech is produced
***where are expressive and receptive language functions localized in the cortex?
***know the cortical structures (including hemisphere) involved in the processing of language comprehension and expression
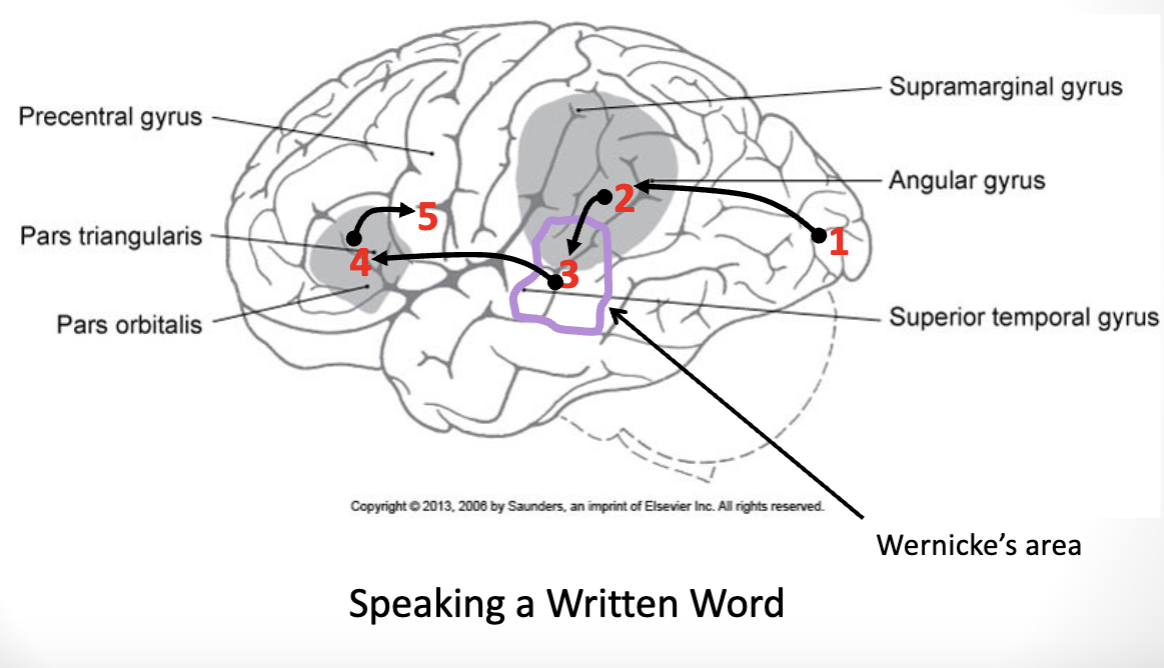
speaking a written word
***primary visual cortex receives the information
—> travels to the ***inferior parietal lobe
—> travels to ***wernicke’s area for comprehension
—> travels to ***broca’s area for the motor plan
—> travels to the ***primary motor cortex to ***generate execution commands to speak
higher cortical language: ***know all the types of aphasia presented in lecture- damage to which areas of the brain causes which types of aphasia? what is the blood supply to each of these regions?
language: ***aphasia:
***fluent aphasia
***non-fluent aphasia
***any disturbance in language, affecting the ***production of speech, the ***comprehension of speech, the ***ability to read or the ***ability to write
usually due to a ***lesion of the left hemisphere
***fluent aphasia: can ***still produce speech, but the ***meaning is impaired (usually a ***Wernicke’s aphasia)
***non-fluent aphasia: ***difficulty communicating orally and with written words, as it is the ***production of speech, but ***comprehension is usually intact (usually ***Broca’s aphasia)
higher cortical language: ***know all the types of aphasia presented in lecture- damage to which areas of the brain causes which types of aphasia? what is the blood supply to each of these regions?
language: ***broca’s aphasia
“***expressive aphasia”
as a result of lesions in the ***left inferior frontal gyrus, aka ***Broca’s area, or Brodmann’s areas 44 and 45
***frontal lobe tumors and occlusions of the ***frontal branches of the ***Middle Cerebral Artery
often seen with a contralateral hemiparesis (b/c the location of Broca’s area is very close to motor)
might ***still be able to get keywords out, but the ***grammar is off
might ***have problems with repeating words
***might have agraphia (***impairments in writing)
usually able to ***understand spoken and written words
these patients are ***usually aware of the deficits – they can ***UNDERSTAND they are not saying what they want to say, and are frequently frustrated by the deficit
higher cortical language: ***know all the types of aphasia presented in lecture- damage to which areas of the brain causes which types of aphasia? what is the blood supply to each of these regions?
language: ***wernicke’s aphasia
“***receptive aphasia”
lesions in the ***left inferior parietal lobe, Brodmann’s areas 39 and 40, as well as in the ***posterior superior temporal gyrus, aka ***Wernicke’s area, or Brodmann’s area 22
as a result of occlusions of ***temporal and/or ***parietal branches of the ***Middle Cerebral Artery
might have ***agraphia (***impairments in writing)
might have ***alexia (inability to read)
usually present with ***clear speech, ***normal prosody, but the ***content is unintelligible (paraphasic speech)
these patients usually have an ***impaired awareness of the deficits as they cannot comprehend what they are saying; usually less frustrated than patient’s with expressive aphasia
higher cortical language: ***know all the types of aphasia presented in lecture- damage to which areas of the brain causes which types of aphasia? what is the blood supply to each of these regions?
language: ***conduction aphasia
this is a disruption of the ***arcuate fasciculus, which is a ***bundle of long association fibers that connect Wernicke’s to Broca’s areas
***impaired communication between these 2 areas
it is a type of fluent aphasia where ***spontaneous expression is intact and ***comprehension is functional, but these patients will have ***trouble ***repeating phrases or ***translating/interpreting what they have heard into an appropriate reply
higher cortical language: ***know all the types of aphasia presented in lecture- damage to which areas of the brain causes which types of aphasia? what is the blood supply to each of these regions?
language: ***global aphasia
this is damage to ***both Broca’s and Wernicke’s areas
usually due to occlusion of the ***internal carotid artery, which results in very ***gross left hemispheric damage
***loss of virtually all language
may be able to use some gestures
higher cortical functions
motor control
praxis
apraxia
forms of apraxia:
ideomotor
ideational
***what is praxis? what is apraxia? what brain structures (including hemisphere) are involved in praxis?
***ideational apraxia- know what it is and what you would see clinically during engagement in activity/occupation
***motor (ideomotor) apraxia- know what it is and what you would see clinically during engagement in activity/occupation
motor planning (motor and parietal association areas)
***praxis – the ***conception and planning of a new action in response to environmental demand
***apraxia – the ***inability to execute learned purposeful movements despite having the desire to perform them, as well as the motor/sensory capabilities required to execute them
usually secondary to lesions of the ***left hemisphere (***premotor cortex, ***supplementary motor area, and/or ***parietal association cortex)
forms of apraxia:
***ideomotor – most common; ***impaired motor performance in ***response to a verbal cue despite intact sensory/motor/language, usually with tool use or gesturing
more of a ***performance problem
***deficits with timing, sequence, amplitude, configuration, limb position in space and
often ***able to perform the same acts normally during their daily life- but ***issue comes after you force/ask them to produce the motion
e.g., them brushing their teeth in the morning vs asking them to brush their teeth
***ideational – ***inability to coordinate activities with multiple,
sequential steps or movementsmore of a ***conceptual problem
may be able to ***name the tool or ***verbally tell you what the tool is used for, but ***cannot execute what to do with it
e.g., tell you that an object is a toothbrush + what a toothbrush is, but cannot show you how to use it
higher cortical functions:
***know the examples provided for spatial relations dysfunction (e.g., position in space, depth/distance, etc.). damage to which area of the brain will likely cause these deficits? what would you clinically see during engagement in activity/occupation with each of these deficits?
***know the neglect syndromes (e.g., unilateral spatial neglect; unilateral body neglect). damage to what areas of the brain will likely cause neglect syndromes? why is left unilateral spatial neglect more common than right unilateral visual spatial neglect? what would you see clinically during engagement in activity/occupation with each of these deficits?
***posterior parietal cortex:
critical for attention and awareness of self and extra-personal space
spatial relations: how objects are located in space with reference to other objects
e.g., understanding your glass of water is to your right, as is the wine and champagne glasses
visual-spatial attention: directing attention to a location in space
e.g., what captures your visual view first when looking at a picture
detecting the movement of people or objects in space
body schema
understanding your body in relation to itself
damage to the ***right (*non-dominant hemisphere) ***parietal association cortex (***posterior parietal lobe) can cause the following
***unilateral spatial neglect: patient is ***unaware of objects and events in the ***left half of visual space
***unilateral body neglect: ***decreased awareness of the ***left side of the body
*most people’s right hemispheres is the non-dominant hemisphere, showing as less people being left-handed

higher cortical funcions:
***know the examples provided for spatial relations dysfunction (e.g., position in space, depth/distance, etc.). damage to which area of the brain will likely cause these deficits? what would you clinically see during engagement in activity/occupation with each of these deficits?
***know the neglect syndromes (e.g., unilateral spatial neglect; unilateral body neglect). damage to what areas of the brain will likely cause neglect syndromes? why is left unilateral spatial neglect more common than right unilateral visual spatial neglect? what would you see clinically during engagement in activity/occupation with each of these deficits?
differences in attentional processing of the brain
***left unilateral spatial neglect is more common than having a right unilateral spatial neglect
***b/c right visual field information is controlled by both hemispheres
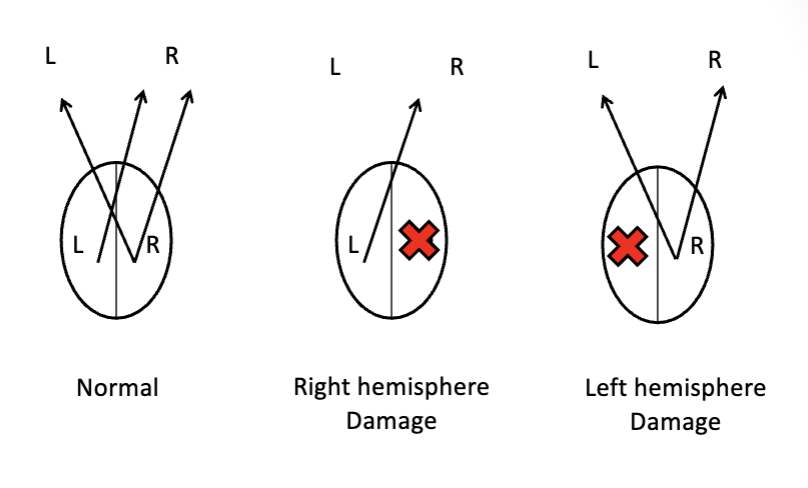
normal visual attention
***right hemisphere of the brain is controlling visual attention to ***both the ***left and ***right visual fields
***left hemisphere of the brain is controlling visual attention to ***just the right visual fields
if you had ***damage to the right hemisphere, which ***perceives information from the left visual fields
***you’d be left with right visual field information
if you had ***damage to the left hemisphere, which ***perceives information from the right visual fields
***you’d be left with both visual fields information
higher cortical functions: ***what is agnosia? what are the different types of agnosia (e.g., visual agnosia, etc.?) damage to what area of the brain will likely cause these types of deficits? what would you see clinically during engagement in activity
agnosia:
***inability to ***know, name, identify, or extract meaning from visual, auditory, or tactile information – ***parietal and ***temporal association areas
***visual agnosia: ***inability to visually recognize objects, although sensory function is generally normal
***social-emotional agnosia: ***inability to correctly ***perceive or comprehend ***social-emotional information conveyed by ***voice, ***gesture, or ***facial expression
***prosopagnosia: ***inability to recognize faces
higher cortical functions: ***what are executive functions and what structures of the cortex are important for executive functions? what deficits might be seen with damage to these structures? how might these deficits impact daily functioning?
***executive functions:
damage to the ***prefrontal cortex
***executive functions: ***prefrontal cortex
***organization: attention, planning, sequencing, problem solving, cognitive flexibility, abstract thinking, etc.
***regulation: initiation of actions, self-control, emotional regulation, moral reasoning, decision-making, etc.
***damage to the prefrontal cortex
deficits in attention
planning deficits: inability to anticipate or predict future events based on current information
disorganized
perseveration
lack of judgment
socially inappropriate behavior
higher cortical functions
the mirror neuron system: (MNS)
distributed network of neurons located throughout the…
frontal (e.g, ventral premotor cortex, inferior frontal gyrus),
parietal (e.g., inferior parietal lobe),
temporal (e.g. superior temporal gyrus),
cingulate
& insular cortices
network is active when we perform a particular action and when we observe another individual perform an action
this distributed network is thought to allow us to understand the actions performed by another person and to predict the consequences of their actions by using mental simulation (“simulation theory”)
plays a role in motor learning
plays a role in empathy
deficits in the functioning of this network have been implicated in autism spectrum disorders and schizophrenia
higher cortical functions
Theory of Mind (ToM): “Theory—Theory”
ToM neural network(??)
Theory of Mind (ToM): “Theory –Theory”
how we develop theories about other peoples minds; cognitive capability to consider the wants, needs, knowledge, and mental states of another person
ToM neural network (??)
medial prefrontal; Precuneus (Superior Parietal Lobule)
temporal/Parietal junction (right hemisphere)
cingulate cortex/amygdala
brain networks:
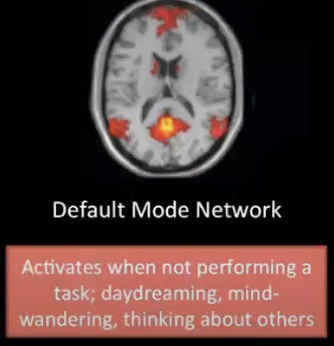
default mode network:
consists of discrete cortical areas (bilateral and symmetrical)
medial prefrontal cortices
posterior cingulate cortices
medial and lateral parietal cortices
medial and lateral temporal cortices
typically more active when we aren’t engaged in attention-demanding or goal-directed tasks
thought to allow emotional processing, self-referential mental activity, and the recollection of prior experiences
e.g., introspection about oneself
e.g., thinking about others
brain networks:
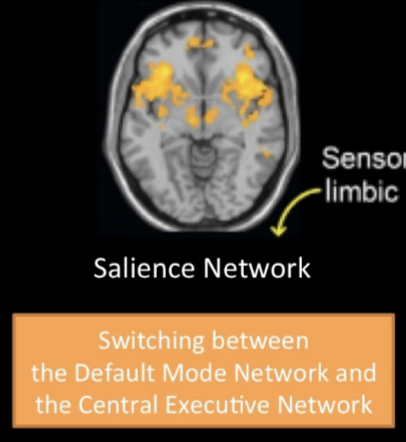
salience network:
highly involved in processing sensory stimuli with visceral, autonomic, and hedonic pleasure information
anterior cingulate cortices
deals with attention and processing of pain and reward
anterior insula cortex
interoceptive signals
subcortical nodes involved in affect and reward processing
integrates internal and external stimuli
plays a key role in identifying the most relevant stimuli in order to guide attention and behavior for adaptive purposes – important for “switching” between the default mode and central executive networks
e.g., gut reaction and increases awareness of subjective feeling states
brain networks:
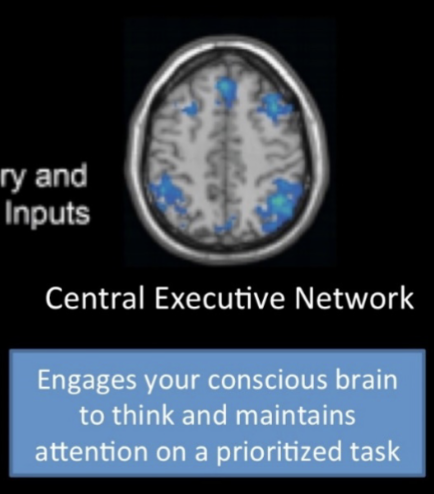
central executive network:
dorsolateral prefrontal cortex
planning, problem solving, abstract thinking, verbal and design fluency, maintaining shifting cognitive sets
anterior cingulate
emotional drive and integration, motivated behavior, decision making, inhibiting of inappropriate responses
orbitofrontal cortex
impulse control, maintaining cognitive set, monitoring outgoing behavior, inhibiting socially inappropriate behavior, valuing rewards based on sensory stimuli, subjective emotional evaluations
lateral posterior parietal cortex
sensory integration, perception, and problem-solving
operates during all goal-directed activities and filters out distractors that might interfere with performance (allowing us to stay focused and achieve our goals)
plays a key role in working memory, cognitive processing, reasoning, task flexibility and decision making
review of blood supply: ***review the blood supply to the cerebral cortex and know which of the cortex are supplied by these arteries (MCA, ACA, PCA)
blood supply to the cerebral cortex
*anterior cerebral:
serves majority of the ***medial surface of the hemispheres (green)
*middle cerebral:
serves majority of the ***lateral surface of the hemispheres (red)
**posterior cerebral:
serves the ***inferior temporal lobe and the ***medial occipital lobe (blue)
*branches of the internal carotid artery
**branch of the basilar artery
review of blood supply: ***review the blood supply to the cerebral cortex and know which of the cortex are supplied by these arteries (MCA, ACA, PCA)
***anterior cerebral artery
supplies the following key functional areas:
***primary motor cortex for ***LE
***primary somatosensory cortex for ***LE
***motor planning areas in the ***medial frontal lobe (dominant hemisphere)
***prefrontal cortex
review of blood supply: ***review the blood supply to the cerebral cortex and know which of the cortex are supplied by these arteries (MCA, ACA, PCA)
***posterior cerebral artery
supplies the following key functional areas:
***optic radiations and ***primary and visual association cortices
***hippocampal formation and ***fornix
review of blood supply: ***review the blood supply to the cerebral cortex and know which of the cortex are supplied by these arteries (MCA, ACA, PCA)
***middle cerebral artery
supplies the following key functional areas:
***primary motor & ***somatosensory cortex for ***face, ***trunk, & ***arm/hand
deep white matter (corticobulbar & corticospinal tracts)
***broca’s area (superior cortical branch) and ***Wernicke’s area (inferior cortical branch) in the ***language-dominant (L) hemisphere
***frontal eye fields
parts of ***frontal and ***parietal lobes important for ***lateralized attention, ***visuospatial analysis & ***emotional expression (body language/tone of voice) (specifically in R hemisphere)
***optic radiations (inferior cortical branch)
stroke syndromes: ***describe common impairments seen in MCA stroke, including main stem, superior cortical branch, and inferior cortical branch. what different impairments would you likely see between left MCA vs right MCA strokes in each of these locations?
***middle cerebral artery (MCA)
main stem:
superior cortical branch:
inferior cortical branch:
most common location of stroke
***main stem: key deficits
***contralateral ***hemiplegia;
***contralateral somatosensory loss;
***contralateral homonymous hemianopia;
***head and eye deviation ***toward the side of the lesion (acutely)
***right hemisphere lesion: ***denial, ***neglect, ***disturbed spatial perception, & emotional flatness is possible
***left hemisphere lesion: ***global aphasia
***superior cortical branch:
***contralateral ***hemiparesis impacting the ***face and ***UE;
possible ***contralateral ***somatosensory loss impacting the ***face and ***UE;
***head and eyes deviated ***toward the side of the lesion (acutely)
***right hemisphere lesion: ***neglect and ***disturbances in spatial perception
***left hemisphere lesion: ***broca’s aphasia
***inferior cortical branch: key deficits
possible ***mild weakness of the contralateral face & arm and
possible ***contralateral somatosensory loss;
***contralateral ***superior quadrantanopia
***right hemisphere lesion: ***denial, ***neglect & ***disturbed spatial perception
***left hemisphere lesion: ***Wernicke’s aphasia
stroke syndromes
anterior cerebral artery (ACA) key deficits
ACA-MCA cortical border zone: key deficits
anterior cerebral artery (ACA) key deficits
contralateral hemiparesis involving the leg
contralateral somatosensory loss involving the leg
frontal lobe behavioral abnormalities
ACA-MCA cortical border zone: key deficits
weakness of the proximal limb girdles of the arm, leg, or both
stroke syndromes
posterior cerebral artery (PCA)
penetrating branch supplying thalamus:
unilateral cortical branches of PCA:
bilateral cortical branches of PCA:
penetrating branch supplying thalamus:
may produce loss of all somatic sensation in the contralateral face and body – this initial hemianesthesia may later develop into thalamic pain syndrome (pain that is not in conjunction with sensory input)
unilateral cortical branches of PCA:
contralateral homonymous hemianopia
bilateral cortical branches of PCA:
inability to form new semantic or episodic memories; cortical blindness (complete loss of vision in a normally appearing eye- not a structural issue, but a processing issue!)
stroke syndromes:
lacunar strokes:
common lunar stroke syndromes:
lacunar strokes: (aka small vessel disease)
these strokes are a consequence of blockage of blood flow to a single small deep penetrating vessel supplying the subcortical white matter region, basal ganglia, internal capsule, corona radiata, thalamus, or paramedian pons
blood vessels responsible for these areas:
lenticulostriate arteries of the MCA,
thalamogeniculate arteries of the PCA
paramedian perforating arteries of the basilar artery
common lunar stroke syndromes:
pure motor hemiparesis
the most common lacunar syndrome (33-50%)
usually involves the internal capsule, corona radiata, or basis pontis;
presents clinically with contralateral hemiparesis
pure sensory:
typically involves the thalamus (VPL), internal capsule or corona radiate;
presents clinically with contralateral sensory loss
sensory-motor stroke
typically involves the thalamus and posterior limb of internal capsule;
presents clinically with a combination of contralateral motor and sensory loss
ataxic hemiparesis:
typically involves the internal capsule, pons or corona radiate;
presents clinically as a combination of cerebellar and motor symptoms, including weakness and clumsiness, on the ipsilateral side of the body; typically leg > arm
dysarthria-clumsy hand:
usually involves the pons, anterior limb, or genu of internal capsule;
presents clinically with dysarthria and contralateral paresis/clumsiness of the arm and hand