Looks like no one added any tags here yet for you.
Specialties within audiology
Medical audiology
Educational audiology
Pediatric audiology
Dispensing/rehabilitative audiology
Industrial audiology
Recreational and animal audiology
Tele-audiology
Forensic technology
Medical audiology key features
Diagnose, manage, and treat hearing and balance disorders
Work in hospitals, clinics, and ENT practices
Diagnostic testing — audiometric evaluations, auditory brainstem response (ABR), and vestibular assessments
Medical collaboration
Rehabilitation
Tinnitus management
Balance disorder treatment
Play a role in the interdisciplinary approach to diagnosing and managing auditory and balance disorders, ensuring patients receive comprehensive care and support
Educational audiology key features
Provide audiological services in educational settings (schools) to ensure students with hearing impairments can access appropriate accommodations and support
Hearing assessments
Classroom acoustics
Hearing aid and assistive technology management
Collaboration with educators
IEPs
Training and education
Advocacy
Help students achieve academic success and fully participate in the school environment
Pediatric audiology key features
Diagnose and manage hearing disorders in infants, children, and adolescents
Work in various settings like hospitals, clinics, schools, and private practices
Early Hearing Detection and Intervention (EHDI)
Diagnostic testing — behavioral audiometry, otoacoustic emissions (OAEs), auditory brainstem response (ABR)
Management
Family counseling and support
IEPs and 504 plans
Collaboration with other professionals
Ensure early and effective intervention for children
Dispensing/rehabilitative audiology key features
Diagnosing and managing hearing loss through the selection, fitting, and adjustment of hearing aids and other assistive devices
Assessment
Device selection
Fitting and customization
Counseling and education
Follow-up and support
Aural rehabilitation — improve listening skills
Combines clinical expertise with patient-centered care to improve QOL
Industrial audiology key features
Focuses on preventing and managing hearing loss in workplace environments, particularly in industries with high noise levels
Noise assessment
Hearing conservation programs
Hearing protection devices
Regulatory compliance
Employee training and education
Data management
Research and development
Protect workers’ hearing, prevent NIHL, and promote safe auditory environments
Tele-audiology key features
Using telecommunication technology to deliver audiological services remotely, enhancing accessibility and convenience
Remote hearing assessments
Hearing aid fitting and adjustment (virtual)
Consultations and counseling
Hearing rehabilitation
Accessibility
Integration with traditional care (in-person visits)
Expands access to audiological care for those with mobility challenges, residing in remote areas, or having busy schedules
Animal audiology key features
Focuses on the hearing health and management of auditory issues in animals (pets and working animals)
Hearing assessments (brainstem auditory evoked response)
Diagnosis and treatment
Hearing protection
Rehabilitation
Education and counseling
Research
Enhance QOL for animals
Forensic audiology key features
Involves the application of audiological principles and practices in legal contexts
Expert witness testimony
Evaluation and documentation
Noise exposure analysis
Hearing loss verification
Causation analysis
Consultation with legal teams
Rehabilitation and compensation recommendations
Ensure accurate assessment and interpretation of hearing-related issues in legal disputes
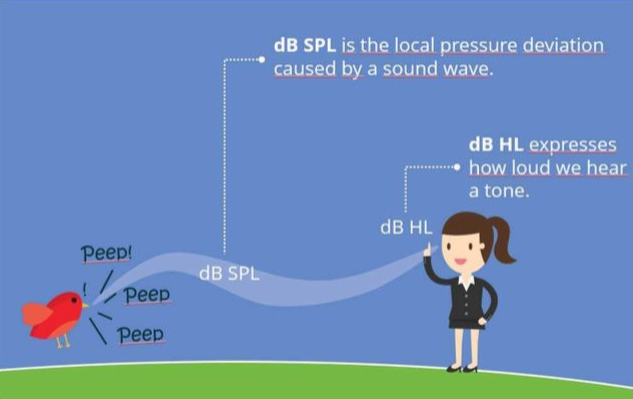
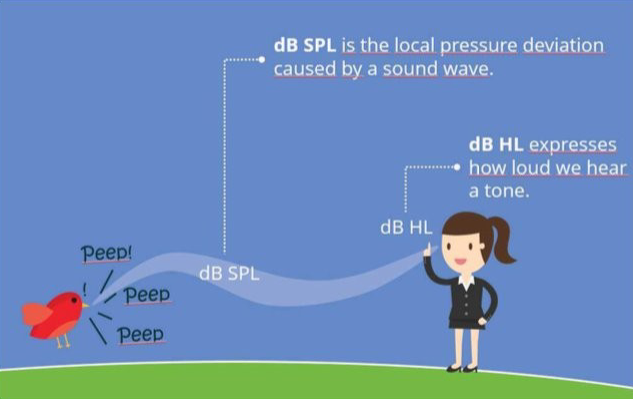
dB HL
How loud we wear the tone… the hearing ability of a person that gives a statement about the severity of hearing loss
“Audiometric normal zero”
HL = hearing level
dB SPL
Sound pressure level — the log scale when referencing the reference level of sound pressure, the local pressure deviation caused by a sound wave
dB SPL = 20 x log (P0/Pr)
Sound pressure: the amplitude level of sound at a specific location in space
dB SL
Sensation level — dB HL amount relative to the individual’s threshold, the difference between person’s threshold and the level observed
If a person’s threshold is 23 dB HL, then a 33 dB HL sound is __ dB SL this person
10
A patient’s threshold is 20 dB HL, then a 50 dB HL sound is __ dB SL to this person?
30
dB IL
Intensity level — refers to the log scale when referencing the reference level of intensity
Sound intensity is the amount of energy transmitted per second over an area of one square meter
dB IL = 10 x log (I0/Ir)
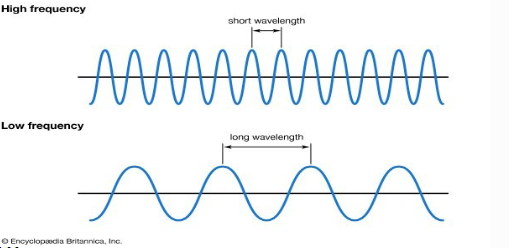
Relationship between frequency and wavelength
The higher the frequency, the shorter the wavelength
The lower the frequency, the shorter the wavelength
λ = c / f
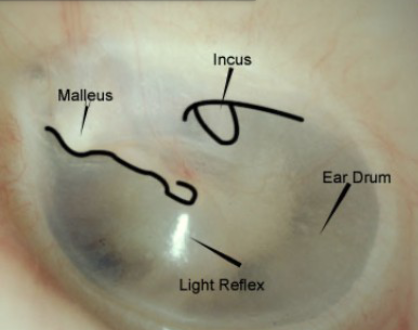
Overview of otoscopy
Hand-held otoscopes are used for inspection of the outer ear, ear canal, and tympanic membrane
Some disorders may be suggested by the appearance of the tympanic membrane
Shining a light allows some of the structures of the middle ear to become visible (because the tympanic membrane is semitransparent) — cone of light
Malleus, Incus, ear drum… want to see these and the light reflex
How to perform otoscopy in infants/children
The pinna is pulled downward and back to better straighten the canal for a more direct view of the tympanic membrane.
The examiner’s fingers brace the head to prevent injury to the ear canal if
the patient should suddenly move
How to perform otoscopy in adults
The pinna is pulled upward and back to better straighten the canal for a more direct view of the tympanic membrane.
The examiner’s fingers brace the head to prevent injury to the ear canal if
the patient should suddenly move
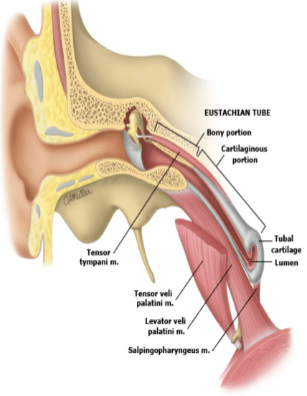
Eustachian tube
The eustachian tube enters the middle ear anteriorly at a 30-degree
angle in adults and passes down into the nasopharynx for 36 mm.
In adults, the tube is normally kept closed by the spring mechanism of
cartilage and is opened by the action of four sets of muscle.
Levator veli palatini
Salpingopharyngeus
Tensor tympani
Tensor veli palatini
When does the eustachian tube open?
Opening of the tube occurs during yawning, sneezing, or swallowing, or when excessive air pressure is applied from the nose
Eustachian tube in infants
In infants, the eustachian tube is shorter and wider in relation to its length and in a more horizontal plane than it is in adults.
The orifice of the eustachian tube in the nasopharynx tends to
remain open in infants until the age of about 6 months.
Functions of the eustachian tube
1. Balance pressure in the middle ear (commonly felt as your ears popping)
2. Drain fluid from the middle ear
3. Protect the ear from both hearing sounds your body causes and nasal drainage
Overview/steps of hearing
Sound waves enter the outer ear and travel through the ear canal, which leads to the eardrum.
The eardrum vibrates from the incoming sound waves and sends these vibrations to three bones in the middle ear.
The bones in the middle ear amplify the sound vibrations and send them to the cochlea.
When the sound goes into the cochlea, hair cells send a wave of energy to the auditory nerve and then to the brain
Disorders of the outer ear
Microtia
Atresia
Growths in the external auditory canal
Cerumen impaction
External otitis
Perforation of the tympanic membrane
Microtia
Birth defect of the ear in which the external ear is small and not properly formed
Atresia
Absence or underdevelopment of the ear canal and middle ear structures
Osteomas
Bony tumors in the external auditory canal
Exostoses
Outward projections for the surfaces of bone, known as swimmer’s/surfer’s ear, as a result of exposure to cold, wet, windy conditions
Cerumen impaction
Excessive wax in the ear
External otitis
Inflammation of the external ear canal, itching, may cause pain
Tympanic membrane perforation
The tympanic membrane may become perforated in several ways:
• Excessive pressure buildup during a middle ear disorder
• Direct trauma from a pointed object
• Sudden pressure in the ear canal
• Rapid changes in ear canal pressure such as in scuba diving
Myringoplasty — surgical repair
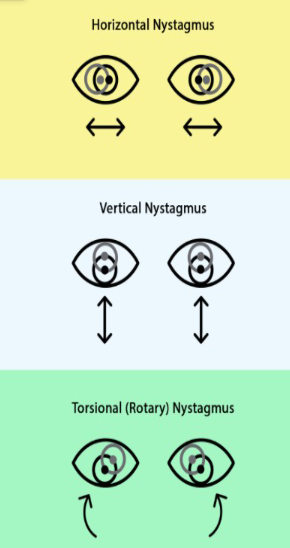
Nystagmus
The reflexive eye responses during head rotation
Dizziness vs. vertigo
Dizziness — a general term to describe unsteadiness, lightheadedness, or feeling foggy
Vertigo — a spinning sensation; you’re spinning or the room is spinning
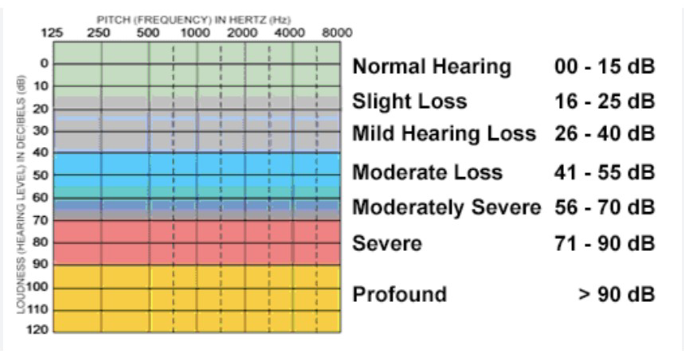
Degrees of hearing loss
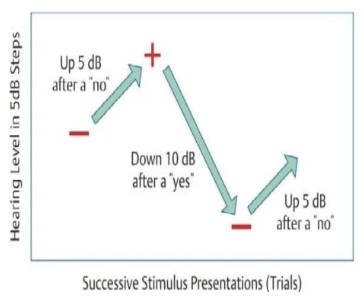
Hughson-Westlake Method
If the patient responds, decrease stimulus intensity by 10 dB.
If the patient does not respond, increase stimulus intensity by 5 dB.
Threshold is determined to be the level where 2 out of 3 correct responses are obtained at the lowest ascending test level.
The starting intensity for the subsequent frequency will be your previous frequency’s threshold + 10 dB.
Ascending
Starting inaudibly and ascend in intensity.
Difficulty conditioning patient to task, responses may be more of
a minimal response level than threshold.
Descending
Starting above threshold and turn the volume softer until barely
audible.
Patient becomes familiar with stimulus and what to listen for, but
can also give more false positives, especially if patterning.
Disorders of the middle ear
Otitis media
Tympanostomy tubes (PE tubes)
Middle ear effusion
Cholesteatoma
Patulous eustachian tube (PET)
Otosclerosis
Otitis media
Most common disorder of the middle ear
Infection that causes inflammation and behind the eardrum
Eustachian tube becomes swollen, mucus can build up
Ear pain, trouble hearing, pressure in the ear, drainage from the ear
Usually clear up within 3-5 days
Tympanostomy tubes (PE tubes)
PE tubes might help individuals who have repeated, long-lasting
ear infections.
During a tympanostomy, a physician inserts a small tube into a tiny incision in the ear drum.
The tubes help let air into the middle ear and allow fluid to drain.
Middle ear effusion
There is thick or sticky fluid in the middle ear but no signs of acute infection
Places pressure on the tympanic membrane
May result from a cold, sore throat, or upper respiratory infection
More common in children due to immature eustachian tube
Difficulty hearing, tugging at ears, loss of balance, delayed speech development
Resolves on its own within 4-6 weeks
If it persists more than 2-3 months, ear tubes may be placed
Cholesteatoma
Benign growth (skin-lined cyst) that begins at the eardrum and invades the middle ear and mastoid
Can retain bacteria and cause infection
Can eat away at the bones and erode the ossicles
First sign is discharge
Almost always needs surgery to treat
As the cyst grows it can become infected
Primary acquired cholesteatoma
Occurs when the ear doesn’t drain or doesn’t even equal out pressure properly (eustachian tube)
Secondary acquired cholesteatoma
Develops when skin cells collect behind the eardrum after a rupture
Congenital cholesteatoma
Forms when skin cells become trapped in the middle ear before birth
Patulous Eustachian Tube (PET)
Disorder of the valve of the eustachian tube that causes it to remain open
Pressure in the ears, ability to hear your own voice/bodily functions loudly
Can be caused by great weight loss, immune disorders, acid reflux, stress/anxiety, chronic nasal allergy
There are medical treatments to avoid dehydration and surgical treatments to fill surrounding areas
Otosclerosis
Abnormal hardening of body tissue — abnormal extension of sponge-like bone growing in the middle ear cavity
Prevents ossicles from vibrating normally in response to sound
Progressive disorder
Runs in families, more common in women
Surgery is often required — stapedectomy (prosthetic device used to allow sound waves to travel to inner ear)
Inner ear disorders
Inner ear hearing loss (general)
Presbycusis (age-related hearing loss)
Noise-induced hearing loss (NIHL)
Perinatal causes of inner ear hearing loss
Anoxia (deprivation of oxygen to the body), prolapse of umbilical cord, premature separation from placenta, toxic substances in bloodstream
Head trauma through violent contractions or forceps during delivery
Treatment for inner ear hearing loss
Watchful waiting
Amplification
Implantable devices — cochlear implants
Aural rehabilitation
Postnatal causes of inner ear hearing loss
Infections — mumps, measles, chicken pox, meningitis
Most caused by virus are bilateral but some can be unilateral (mumps)
Presbycusis (age-related hearing loss)
A gradual decrease in hearing sensitivity in both ears due to increase in age
1/3 of people between 65-74 have hearing loss
Causes: age-related changes in middle ear, complex changes along nerve pathways from ear to brain, long-term exposure to noise, medical conditions like diabetes, genes, medications that are toxic to hair cells in cochlea
Symptoms: muffled speech sounds, trouble understanding speech, often asking others to speak louder
Causes of noise-induced hearing loss
Being around loud noises over a long period of time
Exposure to loud noise in a short period of time, such as gunshot or explosion
Shooting and hunting
Listening to music at high volume through earbuds
Lawn mowing
Symptoms of NIHL
Decreased hearing
Inability to hear high-pitched sounds
Muffled or distorted speech
Tinnitus
Aural fullness
Otalgia: pain in the ear
Prevention of NIHL
Earplugs
Earmuffs
Degree of hearing loss
Severity
Configuration of hearing loss
Shape of hearing loss on an audiogram
Type of hearing loss
Location of hearing dysfunction (outer, middle, inner ear)
3 types of hearing loss
Conductive
Sensorineural
Mixed
Conductive hearing loss
Due to disorders in the outer and/or middle ear
Outer ear:
Cerumen obstruction
Microtia
Atresia
Middle ear:
Otitis media
Eardrum perforation
Exostoses
Sensorineural hearing loss
Due to disorders in the inner ear (sensory cells or neural region)
Inner ear (sensory)
Age-related hearing loss
NIHL
Drug-induced hearing loss
Genetic-mutation induced hearing loss
Inner ear (neural)
Acoustic neuroma
Auditory neuropathy
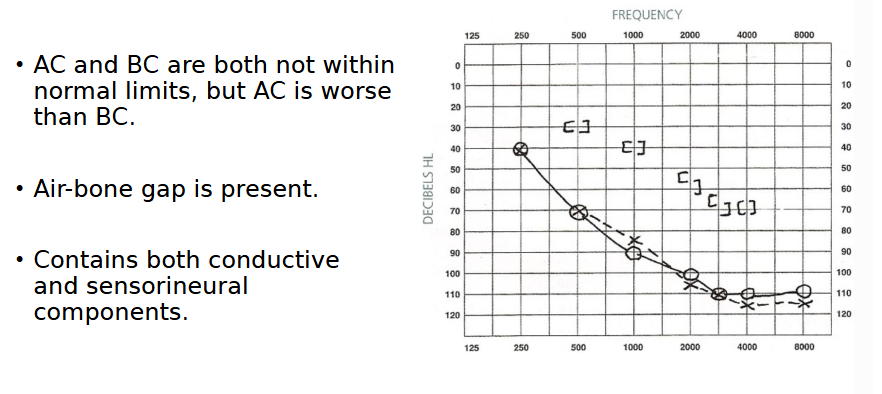
Mixed hearing loss
Has both conductive and sensorineural components — due to disorder in outer and/or middle ear AND inner ear
Ex. an older person with age-related hearing loss and an ear infection.
Air conduction testing
Identifies patient’s hearing sensitivity at different frequencies — if there is a loss of hearing, the test can specify the degree/severity but not the type (conductive, mixed, or sensorineural) of hearing loss
Evaluates the outer, middle, and inner ear
Bone conduction testing
Determines the patient’s sensory/neural sensitivity
Only evaluates the inner ear
By using results of both tests you can determine the type of hearing loss (conductive, sensorineural, or mixed)
Order of frequencies for air conduction testing
1000 Hz - 2000 Hz -3000 Hz -4000 Hz -6000 Hz -8000 Hz -500 Hz -250 Hz
Order of frequencies for bone conducting testing
1000 Hz - 2000 Hz - 4000 Hz - 500 Hz - 250 Hz
Which ear do we start with when testing?
Always start with the better ear — if there is not a better ear, or if the thresholds are same for both ears, start with the right ear
Testing frequency for normal hearing
Start at 1000 Hz around 30-40 dB HL
If they do not respond, increase intensity by 10 dB
Testing frequency for hearing loss
1000 Hz around 50-60 dB HL
If they do not respond, increase intensity by 10 dB
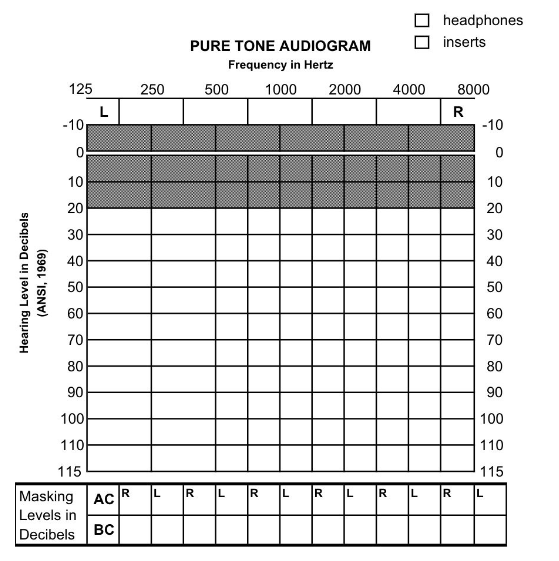
Audiogram axes
X-axis: frequency (Hz)
Y-axis: hearing level (dB HL)
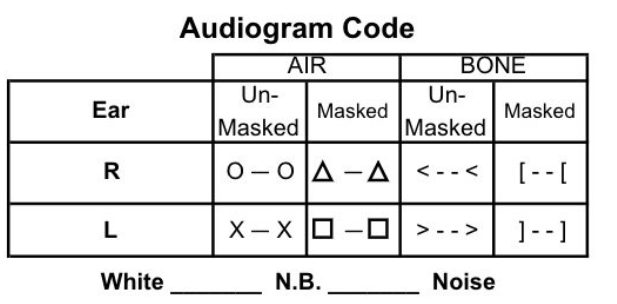
Audiogram key
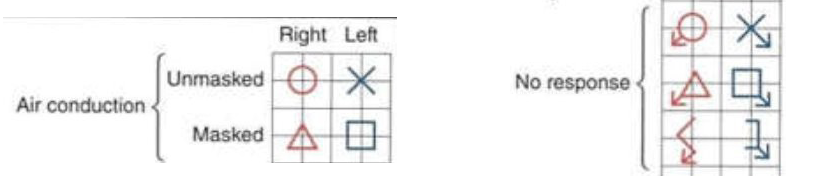
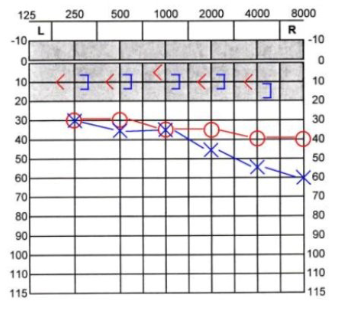
How to record air conduction results on an audiogram
Left ear: blue X
Right ear: red O
Symbol placed at the intersection of frequency and intensity that represents the threshold
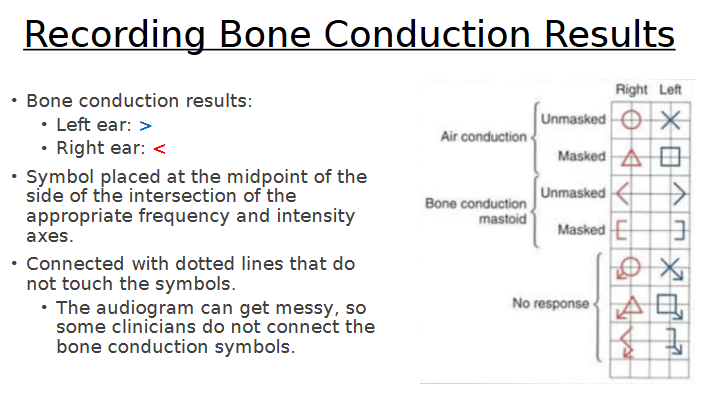
How to record bone conduction results for audiogram
Pure tone average
Average of hearing threshold levels at a set of specified frequencies: 500, 1000, and 2000 Hz
Shows hearing level in each ear
How to calculate pure tone average
dB level at 500 Hz + dB level at 1000 Hz + dB level at 2000 Hz = X/3 = PTA
Example: 45 + 35 + 30 = 36
How to report pure tone/audiogram results
Use a sentence or describe the right and left ear separately if there is an asymmetry
Need to include all 4 aspects of the hearing loss
Degree
Configuration
Type (conductive, mixed, sensorineural)
Lateralization (bilateral or unilateral, symmetrical or asymmetrical)
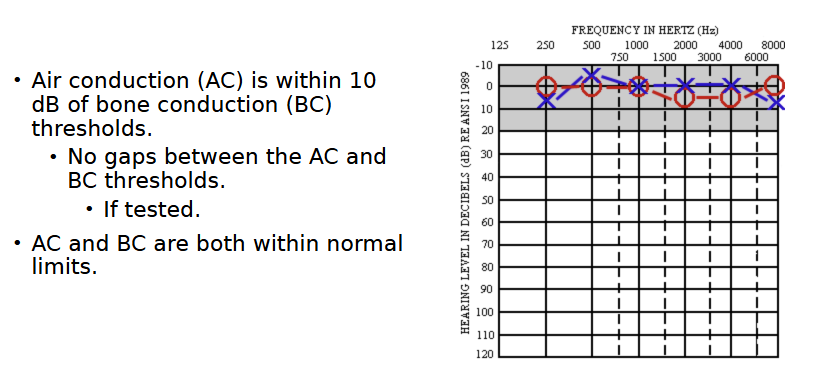
Audiogram characteristics for normal hearing
“Normal hearing sensitivity bilaterally”
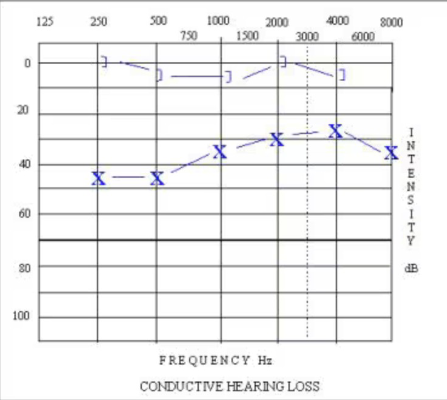
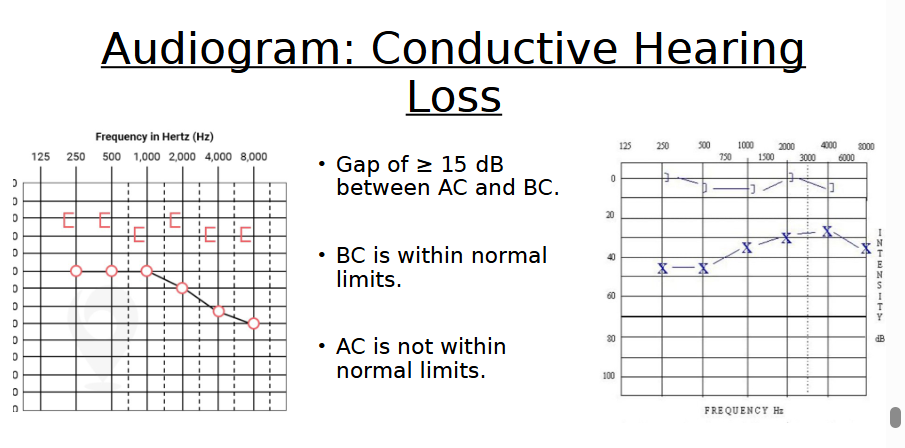
Audiogram characteristics for conductive hearing loss
“Mild sloping to severe conductive hearing loss in the right ear”
“Moderate rising to mild conductive hearing loss in the left ear”
Audiogram air-bone gap
The difference between the air and the bone conduction thresholds.
The gap should be 10 dB or less in subjects without a conductive component (sensorineural hearing loss or normal hearing).
“Right mild flat conductive hearing loss”
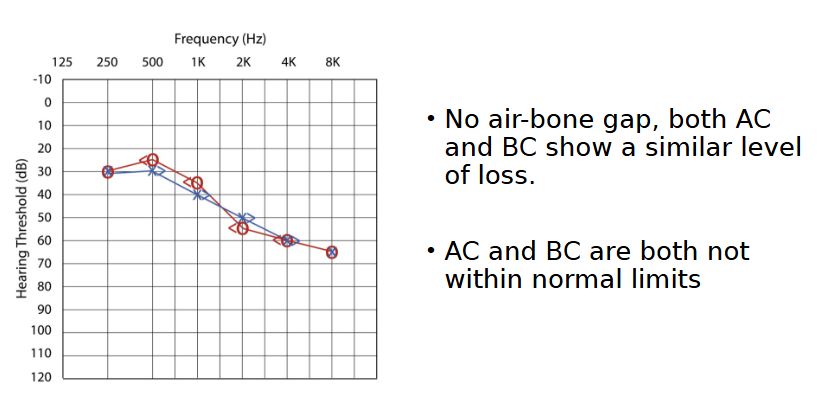
Audiogram characteristics for sensorineural hearing loss
“Mild sloping to moderately severe sensorineural hearing loss bilaterally”
Audiogram characteristics for mixed hearing loss
“Mild precipitous sloping to profound mixed hearing loss bilaterally”
Types of lateralization
Bilateral (both ears)
Symmetrical
Both ears have the same level and configuration of hearing loss
Asymmetrical
≥ 15 dB difference at 1 frequency
≥ 10 dB difference at 3 consecutive frequencies
Unilateral (one ear)
Left or right
Configurations of audiograms
Flat
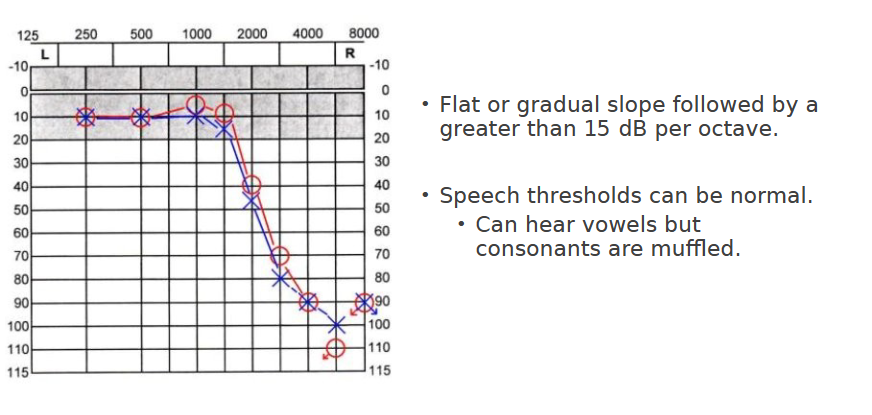
Sloping
Precipitous
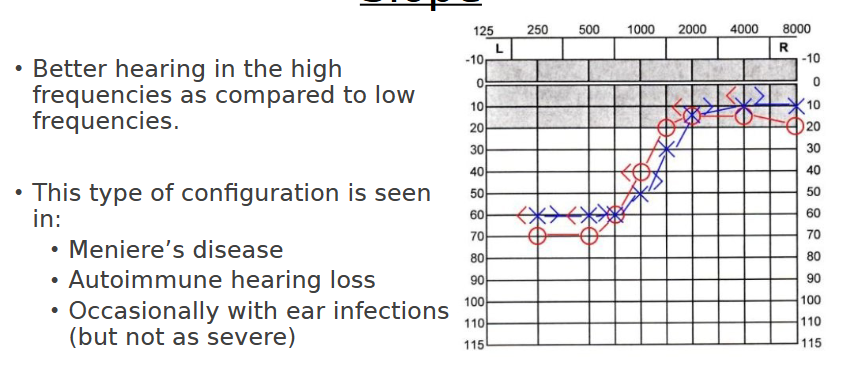
Rising or reverse slope
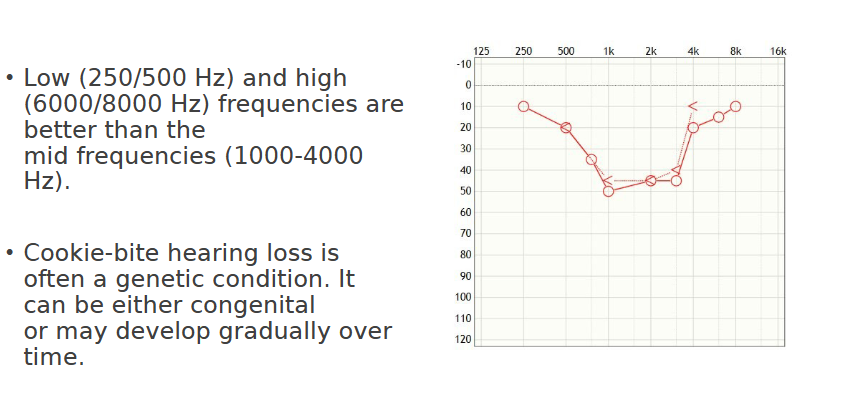
Cookie-bite or trough
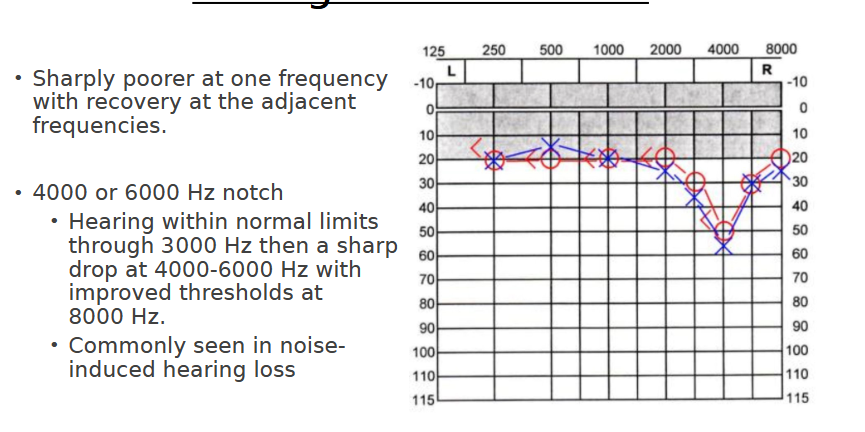
Notch
Corner audiogram
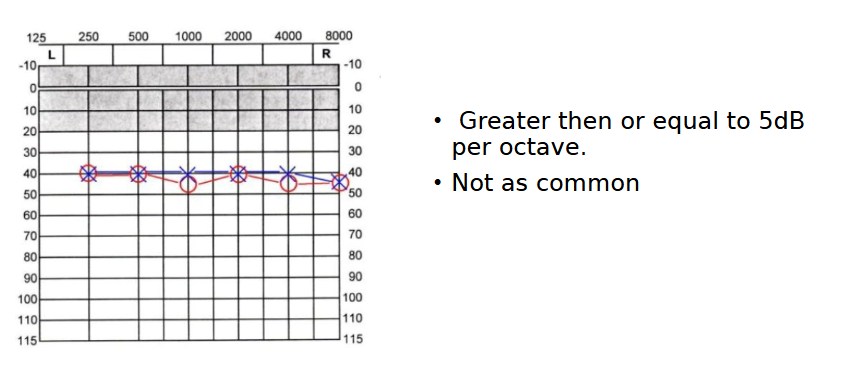
Flat configuration
“Mild flat hearing loss”
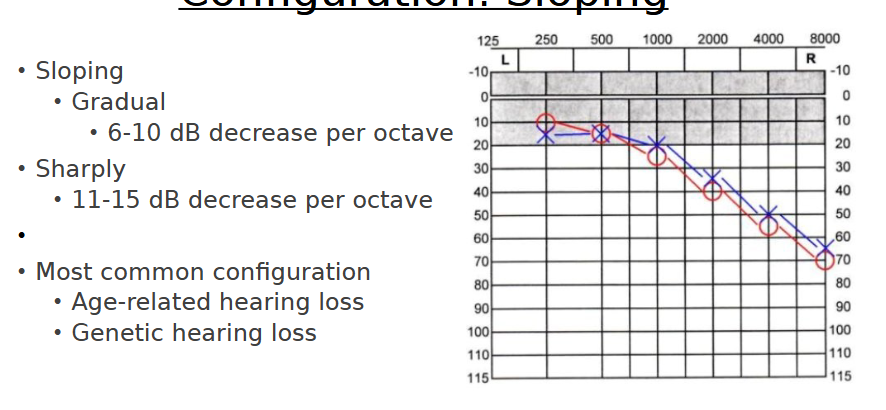
Sloping configuration
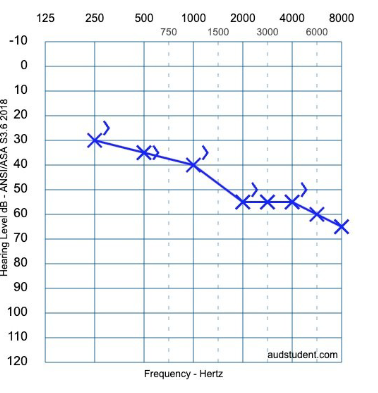
“Normal sloping to moderately severe hearing loss bilaterally
Normal hearing sensitivity through 500 Hz sloping to severe in the right ear
Normal hearing sensitivity through 1000 Hz sloping to severe in the left ear”
Precipitous configuration
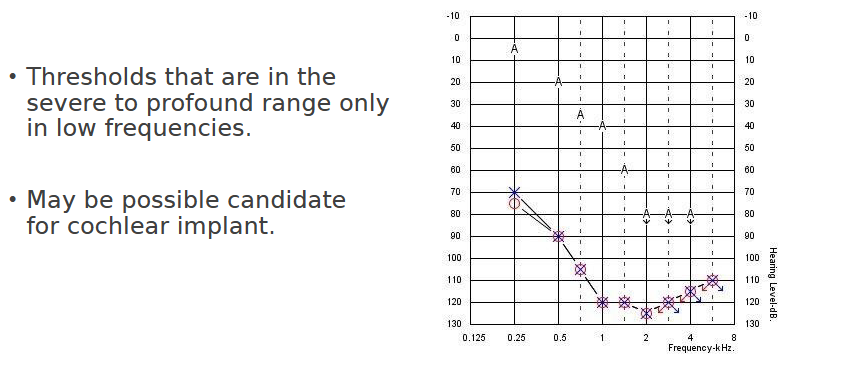
“Normal through 1500 Hz precipitously sloping to profound hearing loss bilaterally”
Rising/reverse slope configuration
“Severe through 500 Hz rising to normal at 1500 Hz hearing loss”
Cookie-bite/trough configuration
“Moderate cookie-bite hearing loss between 1000 Hz - 5000 Hz”
Notch configuration
“Normal-mild hearing with a notch”
Corner audiogram configuration
Formula to describe an audiogram in a sentence
Degree + configuration + type + lateralization
Use air conduction results to determine configuration, lateralization, and degree
Use both air and bone conduction to determine the type
How would you describe this audiogram?
Mild sloping to moderately severe sensorineural hearing loss in the left ear
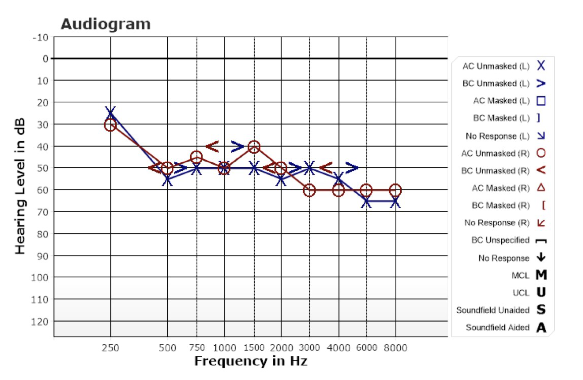
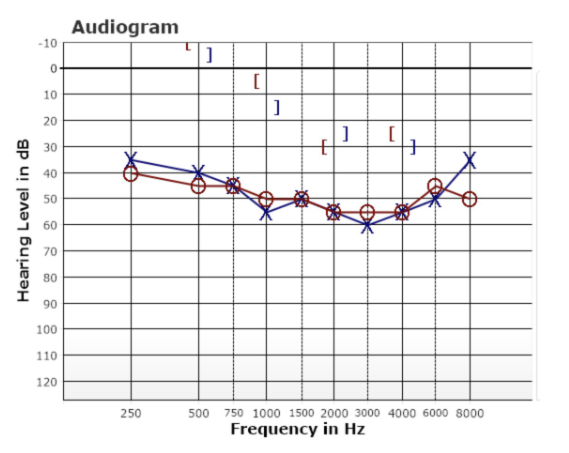
How would you describe this audiogram?
Mild to moderately severe sensorineural hearing loss bilaterally
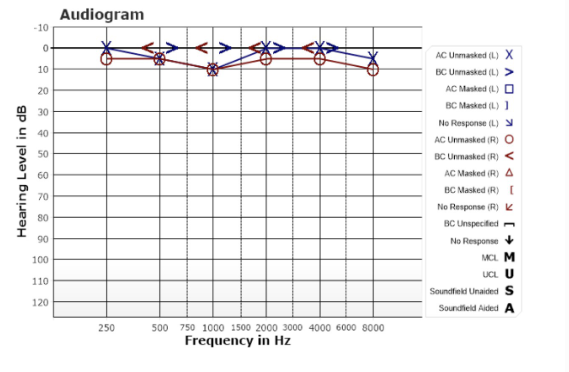
How would you describe this audiogram?
Normal hearing sensitivity bilaterally
How would you describe this audiogram?
Mild to moderately severe mixed hearing loss bilaterally
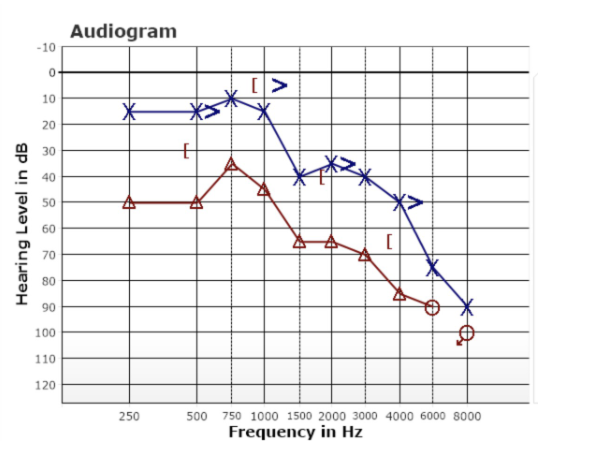
How would you describe this audiogram?
Moderate precipitously sloping to profound mixed hearing loss in right ear
Normal hearing sensitivity through 1000 Hz precipitously sloping to profound hearing loss in the left ear
Outer ear primary function
Collects sound waves and channels them into the ear canal (external auditory meatus) where the sound is amplified
Outer ear structures
Pinna/auricle
External auditory canal (EAC)
Tympanic membrane
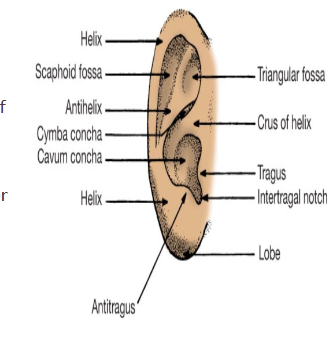
Pinna/auricle
Helps localize the sources of sounds that come from in front of, behind, below, and above the head
Helps funnel sounds directed to it from the surrounding air into the opening of the ear canal
Delivers high-frequency sounds better
Made entirely of cartilage
Ear lob = lobule
Helix
Antitragus
Antihelix
Tragus
Concha