Forensic Psych Midterm Chapters 7, 8, 12, and 13
1/128
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
129 Terms
Violence
physical force for inflicting pain, discomfort, or abuse.
Aggression
behavior with intent of harming another individual physically or psychologically
Violence vs. aggression
• All violence behavior is aggressive, but not all aggressive behavior is violent
• Forensic psychologists frequently work with individuals who are violent
- Conducting a psych eval of an individual who has threatened to harm others
- Conducting a risk or threat assessment
- Providing therapy or rehabilitative services
Instrumental violence
: occurs when injury is secondary to acquisition of external goal
Reactive (expressive) violence
physical violence precipitated by a hostile and angry reaction to a perceived threat or dangerous situation.
Theoretical Perspectives on Violence
Violent actions often fall within the middle range on this continuum

Four Causes of Violence
Neurobiological
Socialization
Cognitive
Situational
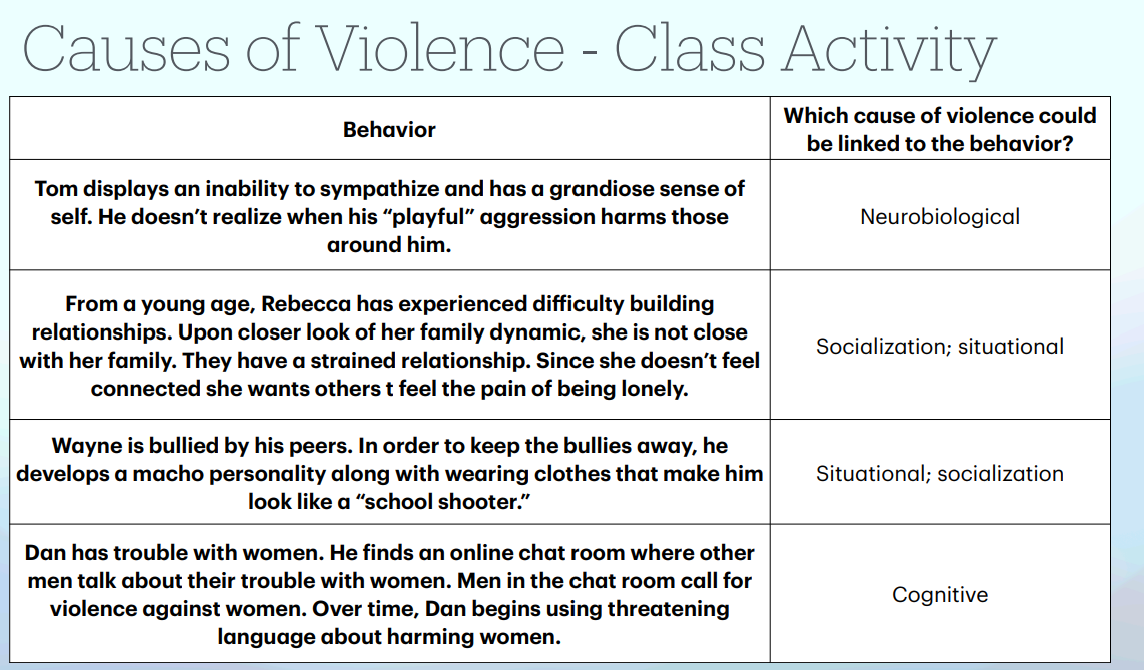
Neurobiological Factors
a wide array of neurological and neurochemical influences on the brain during the life course that may result in high levels of aggressive and violent behavior (e.g., TBI, malnutrition, lead exposure, drugs used during fetal development, executive functions, mental illness)
Socialization Factors
: processes through which a person learns patterns of thinking, behavior, and feeling from his or her early life experiences learned from significant others (including TV, movies, fictional characters, etc.)
Cognitive factors
the ideas, beliefs, and patterns of thinking that emerge as a result of interactions with the world during a person’s lifetime. (e.g., processing & interpreting information, aggressive children have more antisocial, violent beliefs than their nonaggressive peers
Situational factors
The characteristics of the environment, such as stress or aggression in others, that encourage or engender violent behavior. (e.g., supportive or hostile family)
The Effects of Violent Media
• Viewing of violent media can be ONE of many factors contributing to the development of aggression and violence
• It is NOT CASUAL relationship
• Negative effects of viewing violence
- Can increase a viewers fear of becoming a victim
- Desensitize the viewer to violence, more accepting of pain and suffering of others
Observational learning
strong tendency to imitate admired person or role model, especially in children
School Attackers (examples)
Columbine High School, 1999
Sandy Hook Elementary, 2012
Majory Stoneman Douglas, 2018
Forensic School Psychology
• Relates to the intersection of psychology, the educational system, and the legal system
• 1998 - recognized by APA as a specialty
• Role of forensic psychologists:
- Work with schools on suspensions/expulsions, placement of youth into a residential school program
- Perform a variety of assessment and preventative efforts
- Provide psychological services to survivors, witnesses and their families
- Recognize psychological impact on school community
- Educate school community on prevention options
• One of the greatest areas of interest and growth in forensic psychology
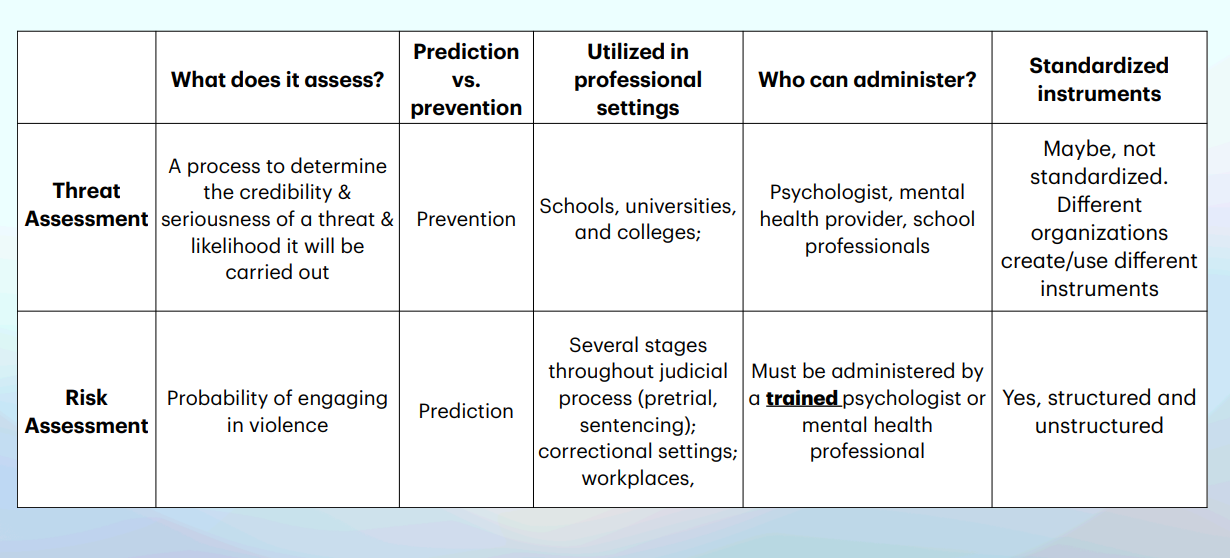
• Threat: expression of intent to do harm.
• Threat assessment: a process to determine the credibility and seriousness of a threat and the likelihood that it will be carried out - forensic psychologists more concerned with prevention than on predicting violence
• Psychological risk assessment: likelihood of dangerous behavior
• December 2013: APA recommends early prevention and implementation of threat assessment teams
Threat assessment vs. Risk assessment
Workplace Violence
• Encompasses assortment of complex behaviors of threatening and injurious behaviors that occur within a place of employment
three based on behaviors:
Workplace homicides
Nonfatal workplace violence
Psychological workplace violence
Four based on assailants relationship
Workplace Homicides
could be perpetrated by a current/former employee or someone outside the workplace
Nonfatal workplace violence
violence that occurs in the workplace, but doesn’t result in death (e.g., robbery, aggravated assault)
Psychological workplace violence
: non-physically aggressive, intimidating, or offensive interpersonal behavior that is psychological in nature, likely to have negative psychological impacts (e.g., bullying, harassment, spreading rumors).
Four types of workplace violence based on assailants relationship
1. No relationship to workplace or victim
2. Recipient of service provided by workplace or victim
3. Connected to workplace through an employment-related involvement (e.g., current or former employee)
4. Indirect relationship with an employee who works at a workplace
Criminal Homicide
• Causing death without legal justification or excuse (at times, killing can be justifiable)
• Two Major Levels of Criminal Homicide:
1. Murder: unlawful killing with malice, usually “degrees” based upon level of planning
2. Manslaughter: unintended killing from unjustifiable conduct
• Is a heterogeneous phenomenon associated with different contexts, motivations, and types of offenders
• Typical murder
• Homicide-suicide
• Atypical murder - forensic psychologist most likely to consult
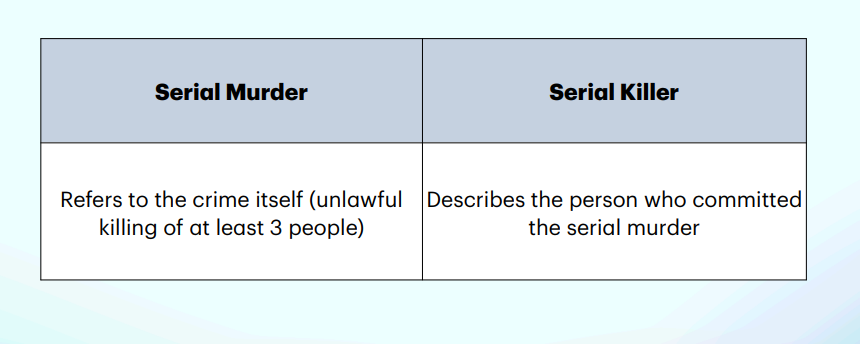
Serial Murder
• Individual (s) separately kills a number of people (minimum of 3) over time.
•There is a “cooling-off period,” which refers to time between the killings; may be days or weeks, but more likely months or years.
Spree Murder
• Individual (or individuals) kills three or more individuals without a cooling off period, usually at two or three different locations.
Mass Murder
• Killing of three of more individuals at a single location without a cooling off period between killings
• Two types: Classic and Family (aka Familicide or Family Annihilation)
• Misinformation on mass murders
Serial Killers
• Little empirical research
• No single killer type
• Excellent interpersonal skill.
• Descriptive information on killers:
- Can be placed on a continuum
- Majority do not present symptoms in line with mental diagnoses
Visionary type serial killer typology
driven by hallucinations or delusions to kill a particular group of individuals
Mission oriented serial killer typology
believes a particular group of people are undesirable, must be eliminated or destroyed
Hedonistic type serial killer typology
strives for pleasure and thrill-seeking, lust and induce pain are primary motives
Power/control type serial killer typology
obtains satisfaction in having control over life-or-death
Serial Murder vs. Serial Killer
Stalking
• Course of conduct directed at a specific person that involves repeated physical or visual proximity, nonconsensual communication, or verbal, written, or implied threats sufficient to cause fear in a reasonable person
• Motives: control, intimidate, or frighten their victims
• Stalking is a crime of POWER and CONTROL
• Three categories based on behavioral clusters (erotomanic, love obsessional, simple obsessional)
• Four categories based on relationship to victim (intimate (most common), acquaintance, public figure, private stranger)
• Four categories based on motive (simple obsession, love obsession, erotomania, vengeance)
When does Stalking usually stop?
1. Stalkers find new love interest.
2. Law enforcement interventions
3. Formal interventions not effective.
4. Persistent Stalking: relocate.
• Stalkers with mental illness less violent
• Juvenile Stalkers more violent
Summary of chapter 8
• All violence behavior is aggressive, but not all aggressive behavior is violent
• Forensic psychologists need to understand the research on causes of violence to apply to operational tasks
• The main difference between serial murder, spree murder, and mass murder is TIMING and LOCATION(s)
What is crime?
• Crime: an intentional behavior that violates criminal code, it did NOT occur accidentally
• Crime encompasses an extremely wide behavior spectrum.
• Persistent antisocial behavior begins early in life, not in adulthood
• Criminal behavior is not one dimensional, it’s the result of a complicated interaction of many different influences
Juvenile Delinquency
• Broad definition: behavior against criminal code committed by non adults.
• Juvenile status offenses: prohibited behavior only for juveniles
• Running away, truancy, violating curfew
• Legal definition: behavior committed against criminal code and adjudicated delinquent by an appropriate court
Five Categories of Juvenile Unlawful Acts
• Unlawful acts against persons
• Unlawful acts against property
• Drug offenses
• Offenses against public order
• Status offenses
• Small percentage of offenders are responsible for a large portion of total crimes committed
• Conduct disorder (CD)
Diagnostic designation used to represent a group of behaviors characterized by habitual misbehavior
• Antisocial behavior
• Serious, habitual misbehavior, in which actions are directly harmful to the well-being of others
• Antisocial personality disorder (ASP, APD)
• Psychiatric diagnosis for adults who displayed CD as children or adolescents and continued into adulthood, at least 18 years old
• Forensic psychologists avoid using diagnosis in evaluations in court
The Developmental Perspective
Delinquency patterns begin in early childhood
• Emphasizes neurological, biological, mental, emotional, and social influence role
• People follow different developmental pathways in their offending or non-offending history
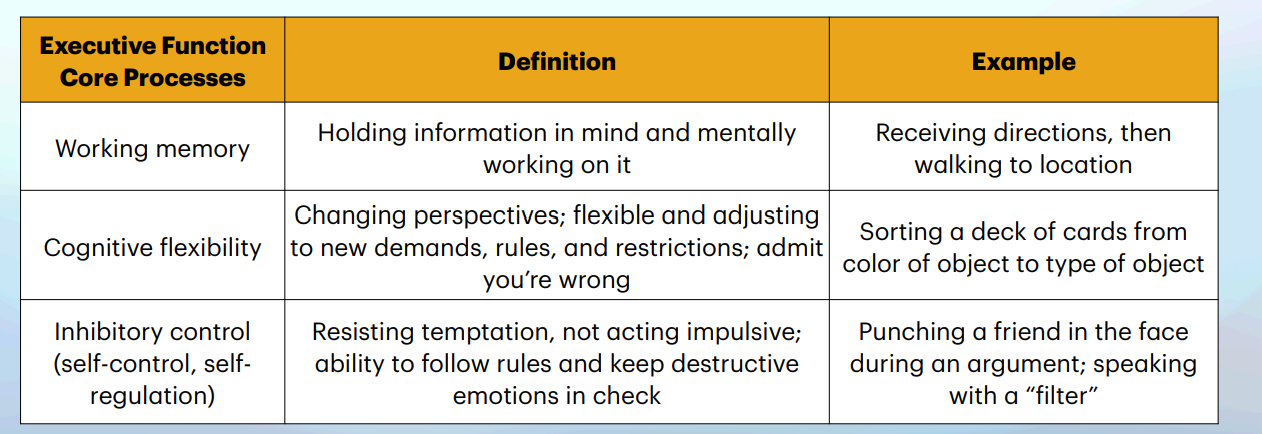
Executive Functions (EF)
• Forensic perspective: EF plays a crucial role
• Cognitive system in the brain that helps successfully navigate our daily activities
• Helps regulate emotions, and to think flexibility and creatively
• EF is not fully mature as a group until late adolescent or young adulthood
• Factors that can affect EF development:
• Quality of parenting
• Stress
• ADHD
• Disadvantageous environments
• Age
• EF impairments associated with many forms of psychopathology (e.g., CD) and antisocial behavior
• Predictor of academic success (EF)
• Well-functioning EF —> achievement and academic success
• EF impairment —> poor academic performance, poor inhibitory control plays a role
• Predictor of antisocial behavior (EF)
• Poor EF is one of the hallmarks of antisocial personality disorder
• EF impairment less likely to override maladaptive responses to maintain appropriate behavior
• Engaging in risk taking (EF)
• Acting without thinking linked to deficits in EF
Moffitt Developmental Theory
• Two developmental paths:
1. Life course persistent offenders (LCPs): delinquency begins in early childhood, continues into a lifetime career of offending
2. Adolescent limited offenders (ALs): delinquency occurring only in adolescents, stop offending around age 18
• Neurological differences in LCPs and ALs
• LCP have thinner cortex in brain regions associated with EF, emotional regulation, & motivation compared to AL
• EF deficits can result from nature or nurture
Steinberg’s Dual-Systems Model
• Focus on the maturation of two different realms:
1. socioemotional network: influence of peers and emotional arousal, remodeled by hormonal changes in puberty
2. cognitive network: reasoning ability, represents the 3 EF
• Brain develops rapidly during adolescence, but these 2 realms develop of different timetables
• Socioemotional networks hampers the cognitive network leading to risk taking and criminal behavior during adolescents
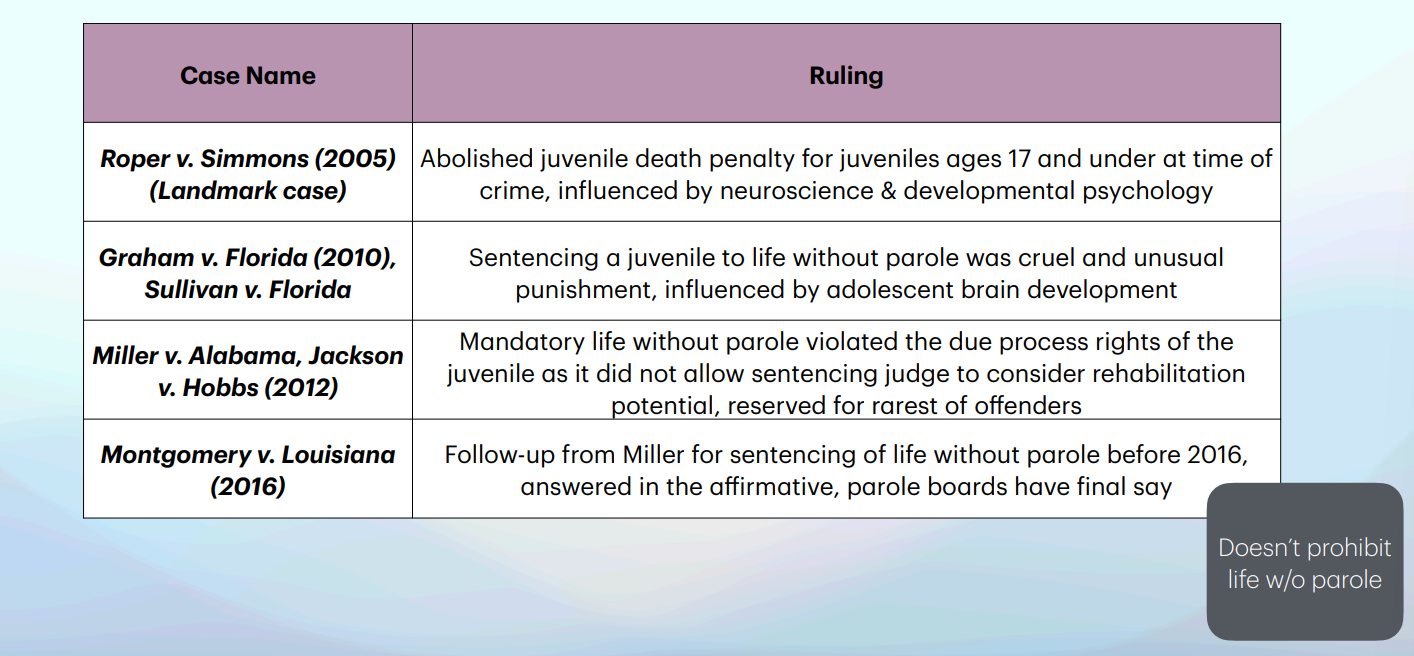
U.S. Supreme Court Cases - Adolescent Offending
Development Factors - formation of Persistent Criminal Behavior
Disruptive behaviors
Externalizing disorders
Internalizing disorders
Disruptive behavior
applied to a variety of actions that create problems for some children and their caretakers
• Examples: hyperactivity, impulsivity, defiance, aggression, disregarding rights of others
• Account for more than 50% of juvenile referrals to mental health clinics
Externalizing disorders
maladaptive behaviors directed at the environment
• Examples: acting out, hostility, antisocial behavior, aggression
Internalizing disorders
maladaptive behaviors directed at the self
• Examples: anxiety, suicidal thoughts, low self-confidence
Four Prominent Disruptive Behaviors
1. Hyperactive-impulsive attention problems (ADHD)
2. Conduct problems (externalizing problems)
3. Deficient cognitive ability
4. Poor interpersonal or social skills
1. ADHD and Delinquency
• Chronic neurological condition characterized by developmentally poor attention, impulsivity, and hyperactivity, now viewed as deficiency in interpersonal skills
• Three central behaviors:
1. Excessive motor activity: cannot sit still, fidgets, runs about, is talkative and noisy
2. Impulsivity: shifts quickly from one activity to another, interrupts others, does not consider consequences of behavior
3. Inattention: Does not seem to listen, easily distracted, loses things necessary for tasks or activities
• Oppositional Defiance Disorder (ODD): angry & defiant behavior towards authority
• Features of children with ADHD
• Generally lack friendship and intimacy
• Difficulty sustaining academic achievement
• Low frustration tolerance, irritability, rapid mood changes
• Causes of ADHD
• Inhibitory problems due to neuropsychological deficits
• Born with biological predisposition toward inattention and excessive movement
• Delinquency, substance abuse common, high risk for developing lengthy and criminal careers
2. Conduct Disorder (CD)
• Cluster of maladaptive behaviors characterized by a variety of antisocial behaviors
• Examples: stealing, skipping school, running away from home, cruelty towards animals and people
• ADHD frequently co-occurs with CD
• Two subtypes: childhood onset (before 10yo) and adolescent onset (after 10yo)
• Considered a serious childhood and adolescent disorder - often precursor to chronic criminal behavior during adulthood
• Marked by a repetitive and persistent pattern of behavior that violates the basic rights of others
3. Deficit Cognitive Ability & Crime
• Importance of cognitive and mental processes in undertaking development of antisocial behavior and violence
• Language acquisition, self-regulation, executive functions, and emotional intelligence
• Strong interactions between neurodevelopment, the environment, and culture in developing antisocial behavior
• Hostile attribution bias: perception of hostile intent in others, but not actually present
• Lack the ability to “put themselves in someone else’s shoes”
4. Social Development Influences
• Peer rejection is one of the strongest predictors of engaging in persistent, serious offending, like violence
• Peer rejection observed through ADHD, CD, hostile attribution bias
• Children who are liked and accepted by peer group from a young age = less likely to engage in antisocial behaviors
• Other developmental factors that can influence adolescents delinquency trajectory
• Physical abuse, exposure to aggressive peers (modeling behavior)
• Poverty
Psychopath
demonstrates a cluster of features that distinguish them from the general population (e.g., psychologically, interpersonally, neuropsychological); reduced capacity for emotional experience, NOT a formal clinical diagnosis
Sociopath
someone who commits repeated crime, different than psychopaths! NOT a formal clinical diagnosis
Criminal psychopath
reserved for psychopaths who engage in persistent antisocial behavior, not ALL psychopaths engage in criminal behavior though
Psychopath v. Sociopath

Psychopaths: General Behavioral Characteristics
Selfishness (egocentricity), express genuine affection, lack of remorse, frequent deceitfulness, callousness, poor judgement, superficial charm, stimulation seeking (excessive need for thrills), low in emotional intelligence
Antisocial Personality Disorder (ASPD)
pervasive pattern of disregard for and violation of the rights of others, starting around 15 years old (not diagnosed until 18)
• ASPD and Psychopathy are NOT the same!
- BOTH focus on specific behavioral patterns, but:
- Psychopathy also focuses on measurable differences in cognition, emotions, and neurological;
- ASPD is a formal diagnosis, while Psychopathy is a set of traits. Not all people diagnosed with ASPD are psychopathic.
Offending Patterns and Measuring Psychopathy
• Persistent, serious offending and engage in violent behavior (e.g., verbal abuse, threats, aggression), mainly directed towards women who are strangers
• May engage in these behaviors as a form of revenge or retribution, or after drinking
• Very few psychopaths are serial killers
• High recidivism in Psychopaths.
• Psychopathy Checklist- Revised (PCL-R): “gold standard”
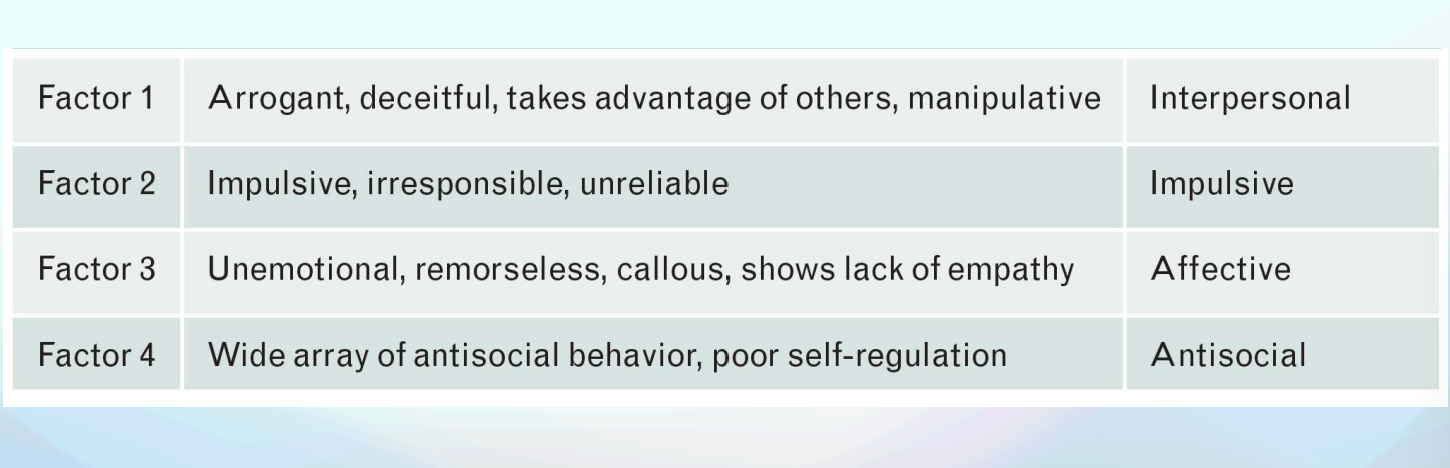
Four Core Factors of Psychopathy
Treatment of Psychopaths
• Limited research focusing in prevalence of psychopathy in females and juveniles
• No known treatment for psychopathy, newer research shows some hope
• Treatment needs to be uniquely tailored to individuals diagnosed with psychopathy
Correctional supervision
broad term to include individuals in prisons, jails, and in the community (probation or parole)
Community corrections
broad team for the variety of options that allows a person convicted of a crime to be supervised in the community (e.g., house arrest, electronic monitoring, halfway houses, etc.)
Probation
sentence to serve time in the community, subject to supervision (courts, probation officer)
Parole
conditional release after completing a portion of sentence
Detention center
facilities where pretrial detainees are held (jails)
Pretrial detainees
persons held in jail before trial, unable to afford bail, denied bail due to dangerousness, awaiting transfer to mental institution, or to another facility
• Functions of jails
Temporary detention facility for individuals awaiting trial or resolution of their case
Facilities for convicted offenders serving a less than 1 year sentence
Prisons
Correctional facilities hold persons convicted of felonies, sentences to more than 1 year
Classified by levels of security (minimum, medium, maximum, supermax)
Overview of Correctional Facilities
• Prisons and jails in rehabilitation.
• Assessment and crisis intervention.
• Issues faced by correctional facilities.
Institutional Corrections: Limitations faced by psychologists
1. Inmates get transferred to other prisons,
2. Correctional officers may not support the psychologist’s role,
3. Administrators may cut their budgets,
4. There is no time to conduct research,
5. Confidentiality is limited, and
6. They are seen as representatives of the prison administration rather than advocates for prisoner’s interests.
• Estelle v. Gamble (right to treatment)
• Inmate argued his rights against cruel and unusual punishment has been violated by prison officials to attend to his medical needs
• Widely interpreted to include psychological or psychiatric assistance for serious mental disorders
Right to Treatment • Violation of Eighth Amendment protection
- To deprive the inmate of adequate medical care violates the Eighth Amendment ban on cruel and unusual punishment.
- Inmates do not have a right to “state-of-the art” treatment or therapy, but the right to adequate treatment.
- A constitutional right to receive treatment for mental illness that is less serious or for substance abuse is not a certainty.
- However, the professional correctional standards advocate meeting all mental health and substance abuse needs of inmates.
Right to refuse treatment
McKune v. Lile
Washington v. Harper
McKune v. Lile
2002: rules loss of privileges for refusal to participate in treatment program
• Forcing and persuasion to treatment
Washington v. Harper
1990: psychoactive medication may be administered against will, administrative hearing within the prison is sufficient
• Challenging the treatment: 3-person panel comprising a psychologist, psychiatrist and a member of the prison administration
Right to Rehabilitation
Rehabilitation: any attempt to bring about changes in behavioral or thought patterns
• Rejection of rights to rehabilitation:
- Inmates have no constitutional rights to rehabilitation in correctional settings
• Prisoners ability to participate in particular programs is at the discretion of the corrections officials.
Prison Transfers
• Moving from one facility to another is not a constitutional right to select the facility
• Implications in inmates with mental disorders
- Prison transfer has constitutional implications if the transfer is to a civil mental institution
- Inmates who are being transferred to a mental health facility outside the prison system are entitled to a hearing beforehand
- These transfers are rarely challenged
Privacy and Confidentiality
No right to privacy in prison or jail settings.
• Hudson v. Palmer, 1984
• Ethical obligation of psychologists: preserve inmate confidentiality to the maximum extent possible, release forms need to be completed by inmates if sharing of records is needed
• Importance of adequacy of the records.
Hudson v. Palmer
limits on privacy within one’s cell
Ford v. Wainwright
1986: disallows execution of severely mentally ill person, violates the Constitution
Right to Competency for Execution
Ford v. Wainwright
• Competency to be executed: at the time of the execution, must be emotionally stable or intellectually capable to understand the meaning of being put to death, psychologists role here in competency assessment
• Resistance of psychologists to participate in evaluations: mainly in reference to medication
Rights to Pre-Trial Detainees
• Innocent unless and until proven guilty.
• Bell v. Wolfish
• Inmate rights under state constitutions
- Confidentiality of records, rights to participate in rehabilitation programs, and visitation rights.
- The psychologist must be aware of the rights guaranteed under the U.S. Constitution, but also of the laws specific to the state
Bell v. Wolfish
1979: limits on rights of pretrial detainees
Inmates with Mental Disorders
Right to adequate mental health care.
• Brown v. Plata
• Inadequate psychological intervention: wide-spread issues
• Impact on female inmates: pre-incarceration history of mental health utilized services more frequently than women who has onset once incarcerated
Brown v. Plata
California ordered to reduce crowded prison population due to the state of mental health care deteriorated to the point of violating prisons Eighth Amendment right
Roles of the Correctional Psychologist
• Correctional psychologist have areas of specific training
• The correctional psychologist, defined as a Psychologist working in corrections, limited time to conduct research
• Managing potential stressors at work
Psychological Assessment in Corrections
• Psychological assessment to measure and evaluate an individual’s past, present, or future psychological status (e.g., interviews, observations, various measuring procedures).
• A variety of psychological measures
• Screening instruments, interviews, review case records
• Need for assessments (entry level, reentry into community, psychological crisis, & ongoing)
• Assessment: key to providing treatment - weighing the balance of security and rehabilitation, evaluating risk/needs assessment
Initial Inmate Screening and Classification
• Psychological processing of inmates: screening to psychologically process inmates & assign to a specific facility
• Screening of pretrial detainees in jails: focus on suicide risk, indicators of substance abuse, history of hospitalizations & medications, indicators of violence
• The reception unit in prisons
• Includes psychologists, psychiatrists, social workers and other professionals
• Administer tests, interview the offender, review records, and recommend programs/ treatment
Competency to be Executed
• Conditions which prohibit death penalty: severe mentally ill, intellectual disability, dementia
• Challenging execution: forensic psychologist requested to perform a competency for execution assessment
• Role of correctional psychologists: rarely requested to conduct competency for execution, small percentage have contact with inmates on death row, challenges usually related to other aspects of their case
• Techniques for competency assessment.
Treatment and Rehabilitation in Correctional Facilities
• Role of psychologist in correctional systems is providing psychological treatment encompassing a wide spectrum of strategies, techniques, and goals
• Goals of treatment:
1) mental health stabilization and
2) rehabilitation
• Common treatments used:
1) therapy,
2) motivational interviewing,
3) dialectical behavior therapy
• Reducing criminogenic needs
- Psychological treatment often follows the risk/needs/responsivity (RNR) principles by reducing an offender’s criminogenic needs .Treatment that adheres to principles of RNR is effective in reducing recidivism and cost-effective
Principles of Risk, Needs, and Responsively (RNR)
• Associated with effective treatment.
• Criminogenic needs: focuses on dynamic risk factors (substance abuse, misogynistic attitudes)
• Non-criminogenic needs: needs that are subject to change, but have little influence on an offender’s criminal behavior
• Level of Service Inventory–Revised (LSI-R): assesses dynamic and static risk factors to determine offenders needs for services as well as risk of reconnection, including violence offenses