There's a surprise in this one <3
dilated
Which cardiomyopathies lead to systolic dysfunction?
hypertrophic, restrictive
Which cardiomyopathies lead to diastolic dysfunction?
Dilated cardiomyopathy (DCM, congestive cardiomyopathy, idiopathic cardiomyopathy)
Which cardiomyopathy is most common and characterized by the dilation and impaired contraction of one/both of the ventricles NOT caused by HTN, coronary atherosclerosis, valvular dysfunction, or structural heart disease?
Genetics (~40%), Coxsackie B, HIV, influenza, alcoholism, peripartum, endocrine disorders, chemo, substance abuse, lead, cobalt, autoimmune conditions, nutritional deficiencies (reversible)
What is the etiology behind DCM?
African American males
Who is at risk for DCM
increased end-diastolic pressures, pulmonary/systemic congestion, mitral/tricuspid regurg, progressive remodeling
Ventricular dilation in DCM leads to
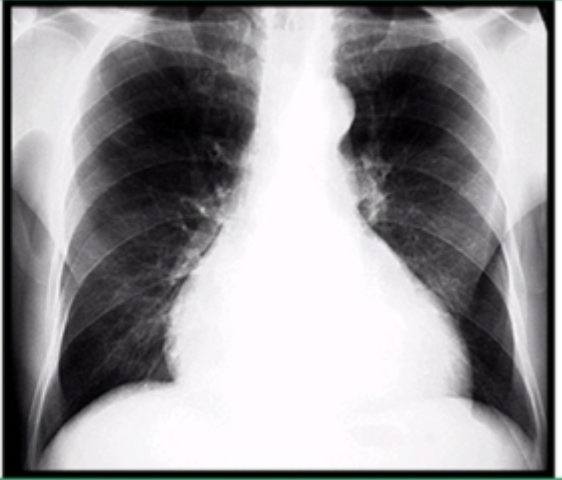
BNP, trop, TSH, iron, ANA, ESR, CRP, CXR, ECHO, EKG
Patient presents to the ER with SOB and fatigue. He states the the SOB is worse when he lays down, especially at night. On a physical exam you note a high pitched holosystolic at the LLSB that radiates to the back and increases with isometric hand grips. You also note an S3, JVD, pulmonary rales, hepatomegaly, and peripheral edema. No hx of travel. What studies do you want to order?
Maybe LBBB, arrhythmias, sinus tach
What is an EKG going to show for DCM?
evaluates myocardial fibrosis, differentiates ischemic vs. nonischemic
What is the purpose of a cardiac MRI in a DCM workup
Cardiac cath (rule out ischemic), biopsy (rule out infiltrative)
Which advanced diagnostics are used for DCM?
Treat underlying, Restrict sodium, stop smoking and drinking, exercise (cardiac rehab), daily weight monitoring, avoid NSAIDs
Non-pharm therapy for DCM
4-prong (ACE/ARB, Beta blockers, aldosterone antagonist, SGLT-2 inhibitors), diuretics, ARNI, Ivabradine (if intolerant to betas), hydralazine-nitrate (if ACE/ARB intolerant), ICD, cardiac resynchronization therapy, transplant (if end-stage and unresponsive to meds)
Meds for DCM
NYHA class III/IV symptoms, severe LV dilated, reduced EF, persistent arrhythmias, elevated BNP, low sodium, frequent hospitalizations
Poor prognosis for DCM
Multidisciplinary team (cardio, primary, rehab), regular imaging, labs, and symptoms monitoring
Follow up care for DCM
Hypertrophic cardiomyopathy (HCM, idiopathic hypertrophic subaortic stenosis, Asymmetric septal hypertrophy, hypertrophic obstructive cardiomyopathy, familial hypertrophic cardiomyopathy)
Which cardiomyopathy is an autosomal dominant disorder with marked LV hypertrophy WITHOUT dilation that commonly affects the interventricular septum resulting in outflow tract obstruction and diastolic dysfunction?
commotio cordis
Trivia Question (For 500 points) What is the name of the thing that happened to Bills safety Damar Hamlin during the game with the Bengals in 2023?
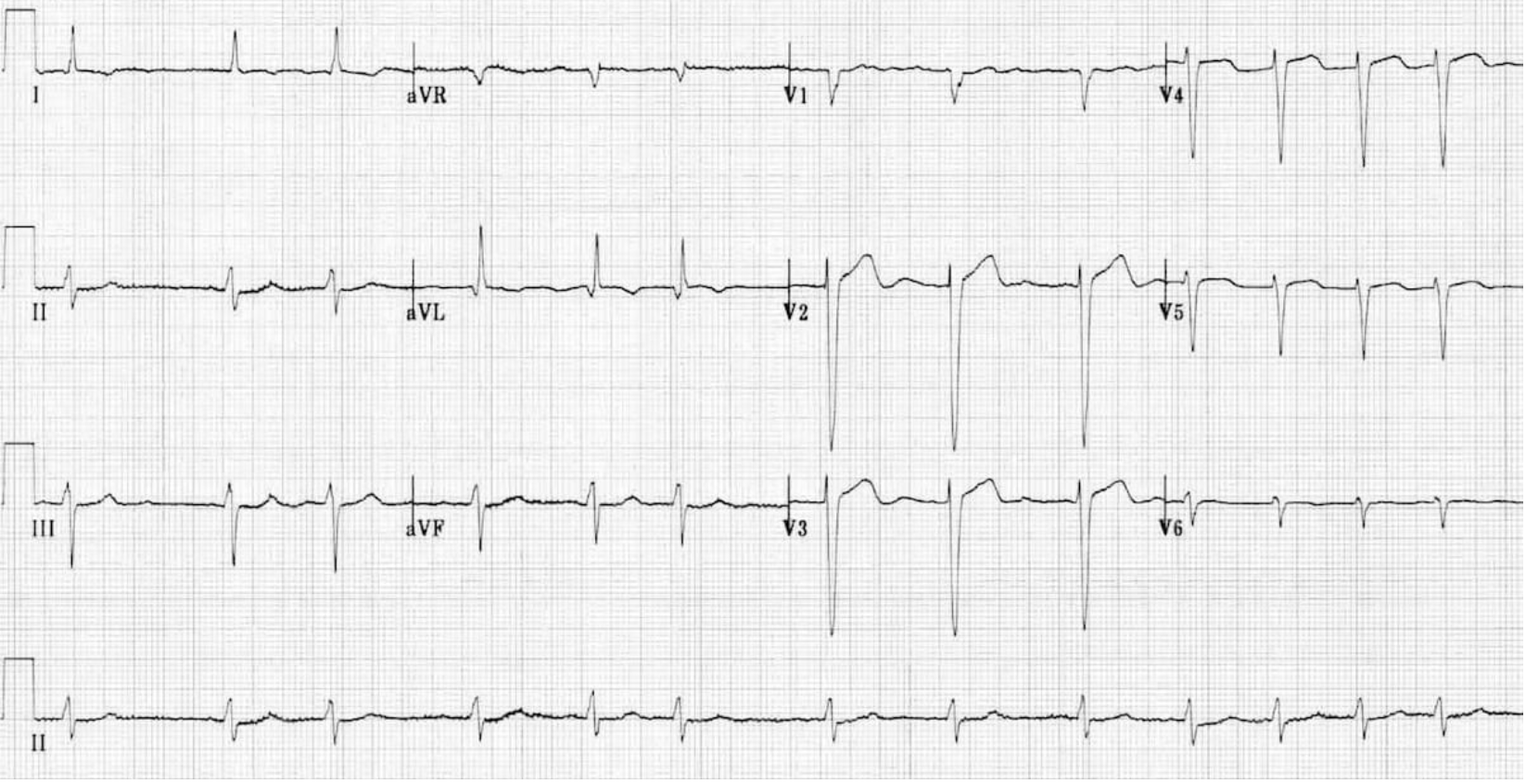
ECHO
14 y/o Patient presents to the clinic for a sports physical, he states that he needs to be cleared because he passed out during football practice. On a physical exam you note a systolic murmur at the LLSB that radiates to the sternal border and a paradoxical split of S2. EKG shows LVH with ST-T wave changes and deep Q waves in leads II, III, AVF, V5, V6. Mother reports that she has a family history of early cardiac death. What is the gold standard for diagnosis?
cardiac MRI (looks for fibrosis), genetic testing for sarcomere mutations, holter monitor to watch for NSVT, stress test
What are some other diagnostic tools for HCM?
Avoid volume depletion, alcohol, and strenuous exercise; beta blockers (1st line for symptoms), CCB, dysopyramide/mavacamten (refractory), ICD, septal myectomy, alcohol septal ablation
Treatment plan for HCM
unexplained syncope, NSVT, severe hypertrophy
Risk factors for unexplained cardiac death with HCM
Restrictive cardiomyopathy (RCM, idiopathic restrictive cardiomyopathy, infiltrative cardiomyopathy, storage disease cardiomyopathy)
Which cardiomyopathy is a rare myocardial disorder causing restrictive filling and diastolic dysfunction but has pretty normal systolic function and is caused by secondary diseases or can be idiopathic?
Amyloidosis, sarcoidosis, storage diseases
What are the most common causes of RCM?
infiltrative, storage (hemochromatosis, Gaucher, Fabry), noninfiltrative (idiopathic, scleroderma), endomyocardial (fibrosis, hypereosinophillic syndrome)
RCM etiology
Echo, cardiac MRI, endomyocardial biopsy
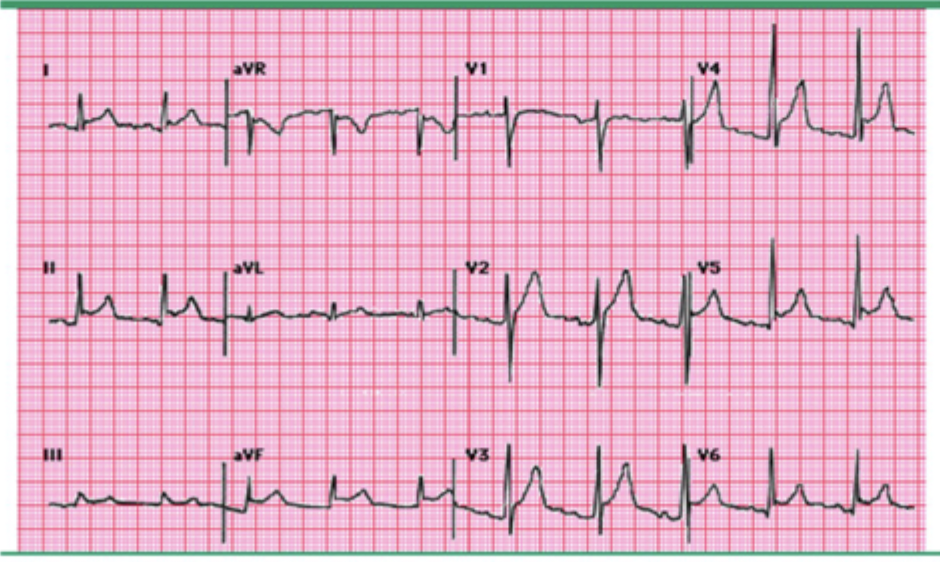
Patient presents to the ED with SOB and fatigue. On a physical exam you note JVD with a positive Kussmaul sign and edema. An EKG is provided by your amazing ED tech. What are some of the key diagnostic tools you want to use?
pericardial thickening, ventricular discordance with inspiration
What does constrictive pericarditis look like?
elevated filling pressures, ventricular discordance
What does RCM look like?
Diuretics, Anticoags, treat the underlying, pacemaker (if there’s a block), LVAD/transplant (refractory heart failure)
Treatment plan for RCM
beta blockers, CCBs
What meds do we need to be cautious with for RCM due to risk of low CO?
infective endocarditis
What is an infection of the endocardial surface of the heart or mural endocardium?
S. aureus, Streptococcus pneumoniae
Acute endocarditis has a rapid onset and is caused by
viridans streptococci
Subacute endocarditis has an insidious onset and is caused by
Injection drug users, prosthetic valves, intracardiac devices, poor dental hygiene
Who do we need to worry about with infective endocarditis?
Endothelial injury allows bacteremia vegetations on the valves
How does endocarditis occur?
strept viridans, S. Aureus
What bacteria do we need to worry about with endocarditis on native valves
Staph epidermis, S. aureus
What bacteria do we need to worry about with endocarditis on prosthetic valves
Pseudomonas
What bacteria do we need to worry about with endocarditis in IV drug users?
platelets, fibrin, microorganisms, inflammatory cells
What are vegetations in endocarditis made from
Septic emboli (stroke, abscess, organ infarction), immune mediated damage (glomerulonephritis, vasculitis)
What are some systemic effects that you may see in infective endocarditis?
blood cultures, echo (TTE, TEE), CBC, ESR, CRP, Rheumatoid factor, UA
45 y/o patient presents to the ER with chills, malaise, weakness, and HA. Patient also reports SOB and a cough as well as muscle pain. Vitals are stable with the exception of a fever. You note splenomegaly, petechiae, janeway lesions and Osler nodes. Hx is positive for a mitral valve replacement and IV drug use. What diagnostics do you want queen?
positive blood culture with typical orgs, Echo shows vegetations/abcesses
What are the Major criteria for the Modified Duke criteria for infective endocarditis?
predisposing criteria, Fever above 100.4, vascular/immunologic phenomena, positive cultures with atypical orgs
What are the Minor criteria for the Modified Duke criteria for infective endocarditis?
2 major, 1 major + 3 minor, 5 mino
Definite infective endocarditis Duke criteria
1 major + 1 minor, 3 minor
Possible infective endocarditis Duke criteria
Pencillin, ceftriaxone, Vanc (6 weeks)
Treatment plan for native valve infective endocarditis
rifampin + gentamicin (6+ weeks)
Treatment plan for prosthetic valve infective endocarditis
HF, abscess, large vegetations
When is surgery indicated for infective endocarditis?
prosthetic valves, prior cases, congenital heart defects, cardiac transplant recipients with valve disease
Which peeps can get prophylactic antibiotics such as amoxicillin, clindamycin, Keflex, ampicillin, or cefazolin before dental procedures to prevent infective endocarditis?
embolic events, HF, abscess, conduction abnormalities, septicemia, metastatic infections
Complications of infective endocarditis
Staph aureus
Which bacteria has the worst outcomes with infective endocarditis?
Pericarditis
What is define as inflammation/infiltration of the pericardium?
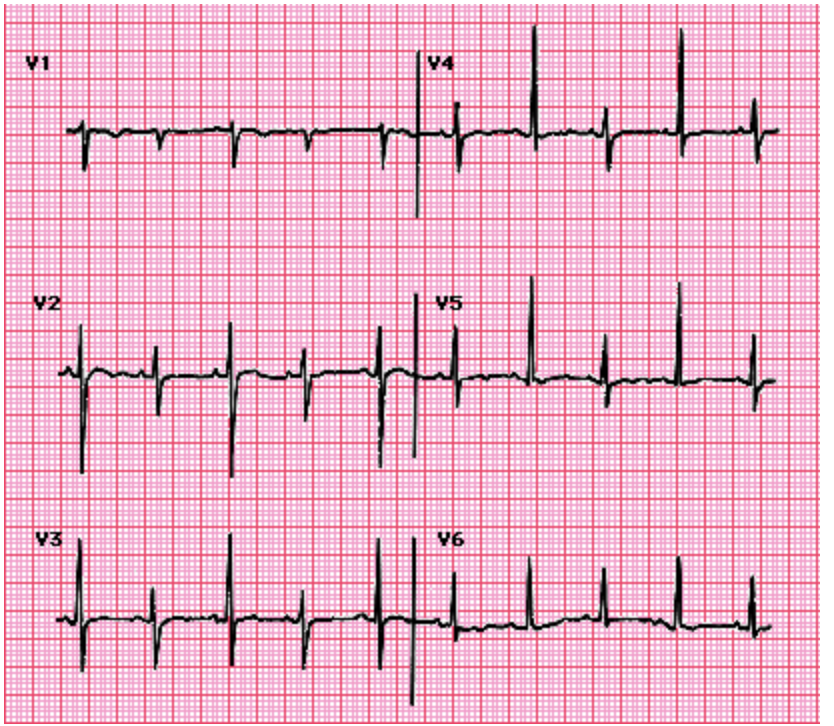
Sharp, pleuritic, positional chest pain, pericardial friction rub, Diffuse ST elevation with PR depression, pericardial effusions
To Diagnose pericarditis, you need 2 of 4
Coxsackie virus, HIV, influenza, TB (most common globally), staph A, all strept species, lupus, TA, sjorgrens, MI (Dresslers), uremia, hypothyroidism, lung/breast/hematologic cancers, hydralazine, isoniazid, immune checkpoint inhibitors
Common causes of pericarditis
ESR, CRP, Trop, CBC, CMP, Echo, CSR, MRI/CT
Patient presents to the ER for chest pain which he describes as “Holy shit I feel like I am being stabbed in the chest!” When the head of the bed is elevated he stops screaming. Patient reports he recently got over a cold. On a physical exam you auscultate a scratchy sound at the left sternal border as well as muffled heart sounds. You also note an elevated JVP. Vitals are stable with the exception of tachycardia, hypotension, and fever. Your amazing ED tech hands you the following EKG, what do you want to order?
hypotension, muffled heart sounds, elevated JVP
What is Beck’s triad - sign of pericardial effusion?
NSAIDs/ASA (1st line, ASA for MI), colchicine (reduces recurrence), corticosteroids (refractory), antibiotics if bacterial, antitubercular for TB, dialysis (uremia), NO ANTICOAGs, pericardoectomy (last resort)
Treatment plan for pericarditis
cardiac tamponade, chronic constrictive pericarditis, recurrence, myopericarditis
Complications of pericarditis
Cardiac tamponade
What is a life threatening condition due to increased pericardial pressure that limits diastolic filling and reduces CO?
Trauma, cancers, infections, post MI, uremia
Causes of cardiac tamponade
CXR, Echo (SPECIFC), cardiac cath
Patients is brought to the ER for chest pain and SOB. On a physical exam you note that the patient is clammy to the touch and has cool extremities. You also see elevated JVP and muffled heart sounds. Vitals are stable with the exception of tachypnea, tachycardia, and severe hypotension. After you throw an A line in, you see a 10 mmHg drop of the SBP during inspiration. You are handed this EKG, what test do you want?
aggressive volume resuscitation, avoid nitrates and diuretics (reduce preload)
Initial measures for Cardiac tamponade
Pericardiocentesis (1st line), surgery (pericardial window, pericardectomy)
Definitive treatment for cardiac tamponade
hemodynamic supports with inotropes, serial echos
How are we monitoring tamponade patients?
hypotension, cardiogenic shock, PEA, organ failure, recurrent pericardial effusion/tamponade, constrictive pericarditis
Complications of Cardiac tamponade?