Peds Exam 3 Combined
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
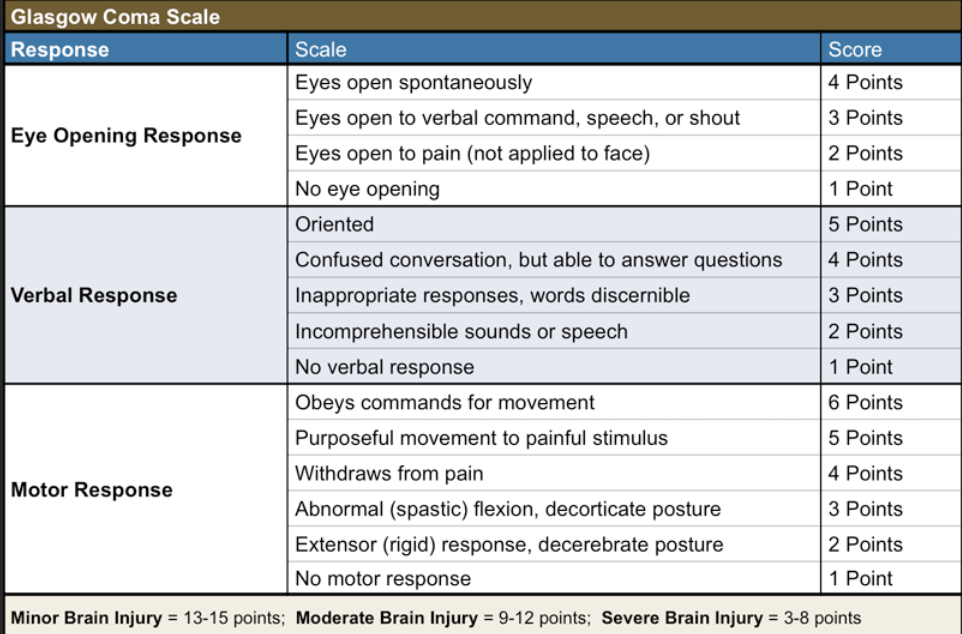
What does GCS measure:
3 levels
LOC:
eye opening
verbal response
motor response
13+: normal or mild brain injury
9-12: moderate injury
< 8: severe brain injury/ coma
LOC and their meanings: (5)
Alert: use normal voice
awake, answers appropriately
Lethargic: use loud voice
Drowsy, but responds to voice and falls asleep easily
Obtunded: shake gently
confused, decreased awareness in surroundings
Stupor: painful stimuli
only responds to pain
minimal verbal response
Coma: repeated painful stimuli
doesn’t respond to any stimuli
What info needs to be assessed with headaches- basic? (6)
basically OLDCARTS
onset/pattern
frequency/severity over time
location
associated s/s
migraines accompanied by GI changes
triggers
stress level
school, fam, homework
HA red flags: (10)
sudden, severe HA
increasing severity
HA in ONE location only
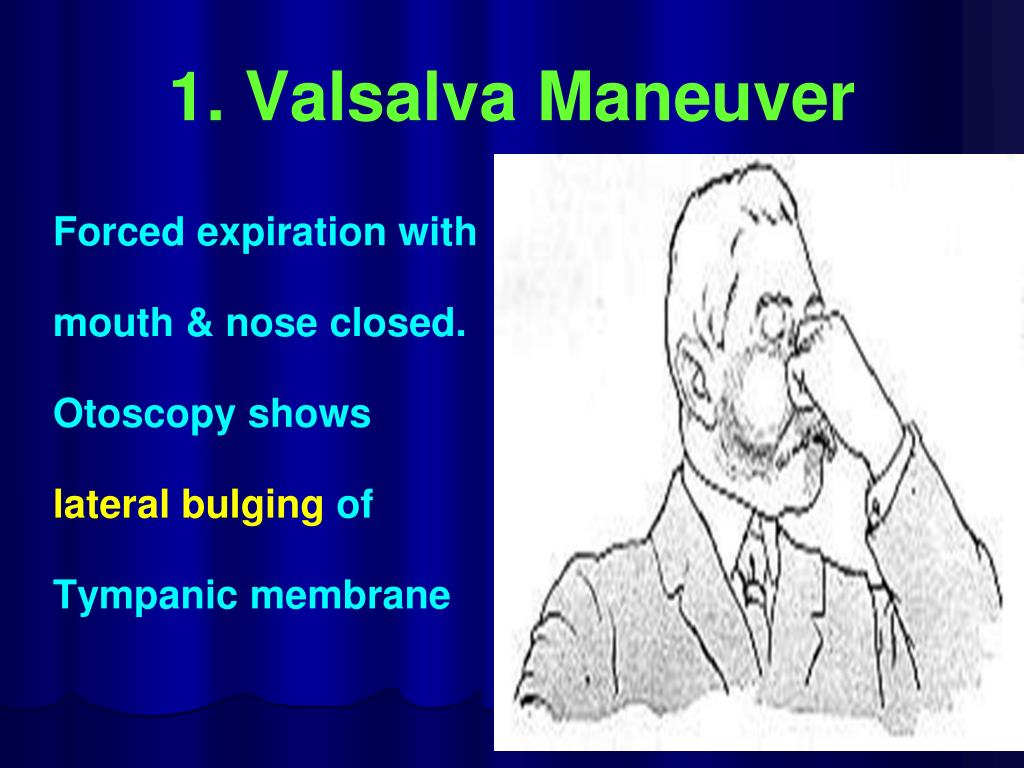
HA wakes child from sleep
worse when coughing/sneezing or Valsalva maneuver
papilledema
unilateral weakness
diplopia
imbalance
seizures
Whats meningitis?
caused by (2)
inflamed meninges surrounding brain + spinal cord
caused by viral or bacterial infx
What can cause meningitis? (3)
skull fractures
crowded spaces (dorms)
penetrating head wounds
Difference b/w viral and bacterial meningitis:
CSF:
WBC:
Protein:
Glucose:
Gram stain:
Viral: (milder)
CSF: clear
WBC: slightly high
Protein: normal
Glucose: normal
Gram stain: negative
Bacterial: (can be fatal)
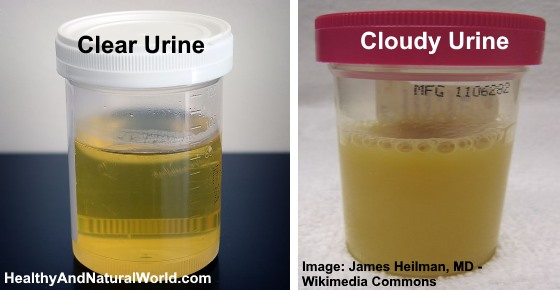
CSF: cloudy!
WBC: high!
Protein: high!
Glucose: LOW
Gram stain: positive
Meningitis s/s newborns (7)
NO nuchal rigidity!! (neck is supple/flexible)
weak cry
bulging fontanel (LATE sign)
poor feeding/vomit
poor muscle tone
poor suck
fever or hypothermia
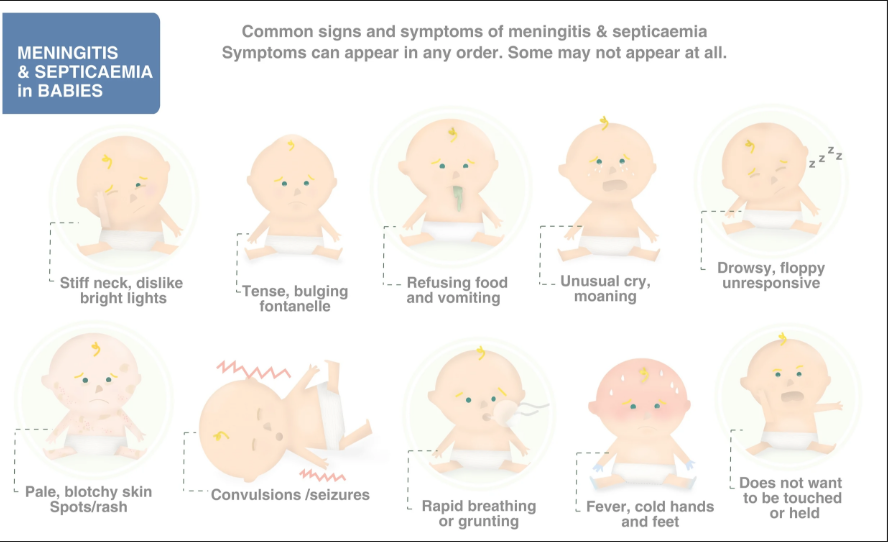
Meningitis s/s infants (3 mon-2yrs): (7)
high pitched cry
bulging fontanels
HAS nuchal rigidity!!
photophobia
fever/irritable
poor feeding/ vomit
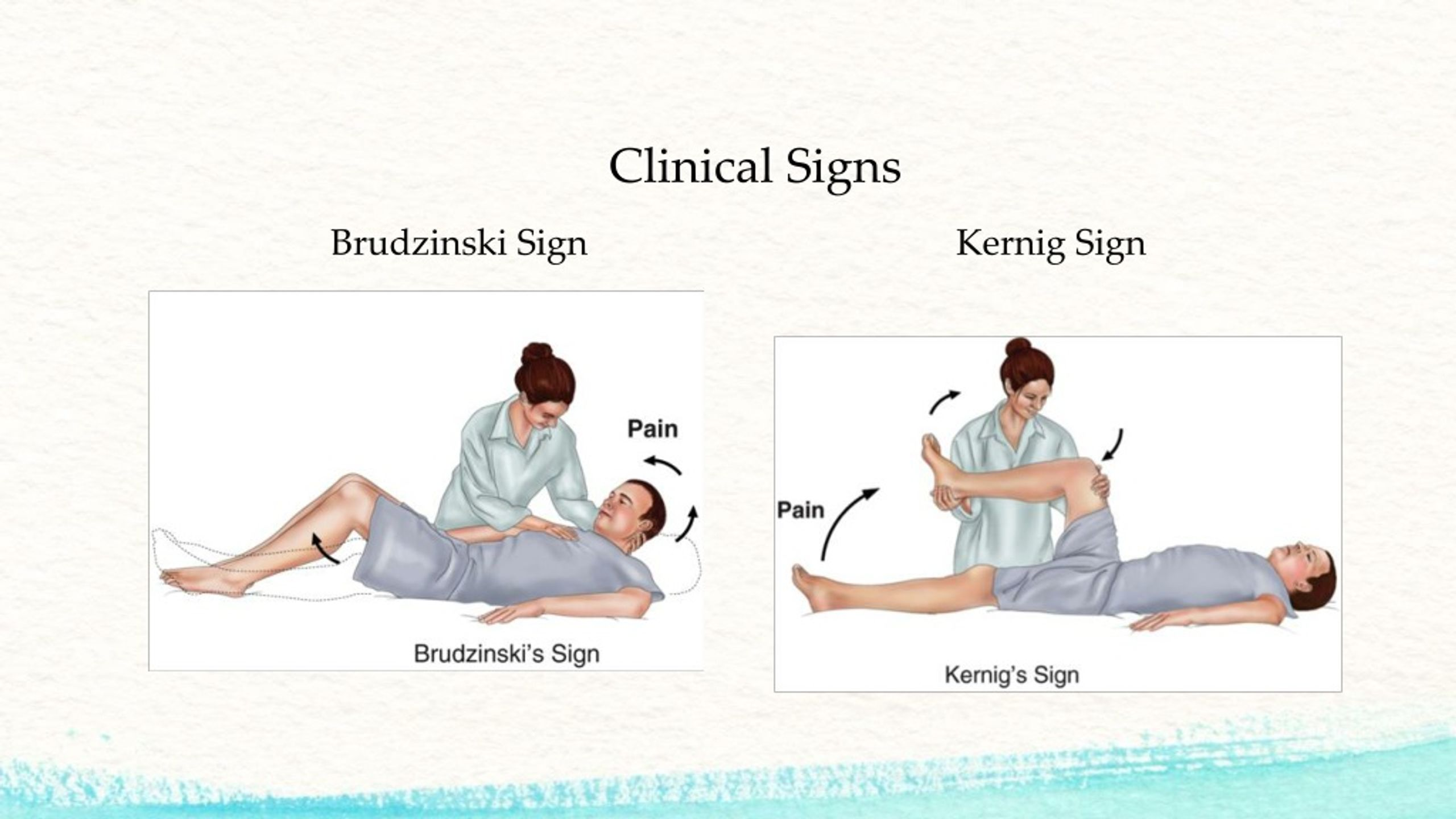
Brudzinski’s and Kernig’s signs NOT reliable!!!
Brudzinski’s and Kernig’s signs
Brudzinski’s
A sign of meningitis where the hips and knees automatically bend when neck is bent forward.
Kernig’s
the leg cant fully straighten b/c of pain and resistance.
Meningitis s/s children-adolescents (2-18 y/o):
specific (5)
common (7)
+ Brudzinski’s sign
+ Kernigs sign
petechiae or purpuric rash (meningococcal infx)
joints are involved (Hib and meningococcal infx)
chronic ear draining (pneumococcal infx)
common s/s: (7)
seizures
nuchal rigidity
fever/chills
HA
confused
vomit
irritable/restless

What is considered a medical emergency and the most severe form of meningitis?
Petechiae!!!!
means infection reached bloodstream

Nurse care for meningitis: (9)
look for petechiae!!! Emergent
droplet isolation! ASAP
assess bulging fontanel if < 18 mon.!!
seizure precautions (suction, padding, turn)
correct fluid volume deficit, the restrict fluids till ICP resolved
NPO (bc ⬇LOC)
quiet, low stim environment
no pillow (neck flexion), semi fowlers
side-lying
Signs of increased ICP in infants: (4)
bulging fontanel
⬆head circumference!
high pitched cry
distended scalp veins

Interventions to reduce ICP: (5)
elevate HOB
neutral head alignment
no coughing/straining
quiet dark room
limit suctioning
what are:
tonic clonic seizures
myoclonic
absence seizures
atonic
tonic clonic seizures:
body stiffens w/ jerking movements
loss of LOC and control of bladder, tongue biting
myoclonic
quick muscle jerks; person conscious
absence seizures
brief loss of awareness where they stare into space
atonic
muscle suddenly lose strength (collapse or drop)
What are Febrile seizures
d/t infx causing high fever >101 F in children 5 mon.-6 yrs
lasts for 15-20 secs
Causes for seizures in neonates: (6)
hypoxia
intracranial hemorrhage
birth injury
metabolic disorders
hypoglycemia
kernicterus
Whats kernicterus and how to prevent it?
→ severe neonatal jaundice where bilirubin accumulates and enters brain= damaged brain cells
phototherapy!!

3 stages of seizure:
aura: warning sensation
ictus: actual seizure
postictal: after seizure (recovery)
Nursing care during seizure: (4)
airway patency (no loose tooth)
O2 >95%; pink skin
IVP meds slowly (prevent resp or circulatory failure)
raise and pad side rails/floor
Whats Reye Syndrome?
who does it affect? (2)
rare condition causing encephalopathy and fatty liver
affects children/teens recovering from viral infx (chicken pox)
children taking too much aspirin

Labs seen in Reye syndrome: (4)
Elevated AST/ALT
Increased ammonia
prolonged PT d/t liver not making correct amt of blood clotting proteins
abnormal electrolytes d/t cerebral edema
What causes CP? (7)
drugs
kernicterus (severe jaundice)
maternal infx (TORCH)
premature birth
poor O2 to baby
traumatic birth
meningitis
4 types of CP
spastic
dyskinetic
ataxic
mixed
Spastic CP: (4)
hypertonic muscles (⬆DTR)
abnormal clonus
positive Babinski reflex
exaggerated reflexes
Dyskinetic CP: (5)
involuntary mvmts
poor tongue/swallowing mvmts
drools
speech difficult to understand
jerking
**think of parkinson’s tardive dyskinesia
Ataxic CP: (3)
poor balance
awkward, wide gait
cant do fine motor motions
finger to nose test
rapid repetitive mvmts
CP physical assessment: (7)
anoxia @ birth (lack O2 when born)
strabismus (cross eyed)
refractive disorders (needs glasses)
abnormal speech rhythm/ articulation
recurrent seizures
ADHD
autism

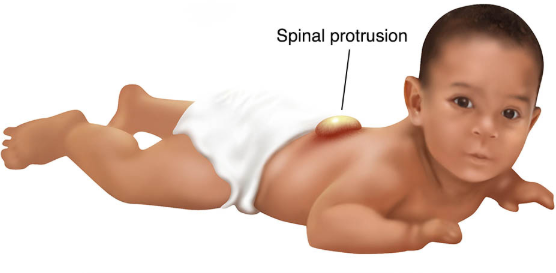
Spina Bifida care: (5)
cover defect w/ moist, sterile, non-adhesive dressing (prevent drying)
dressing changed q2-4 hrs
newborn in PRONE!!
dont place diaper over defect (prevent pressure on sac/rupture/infx)
LATEX FREE environment
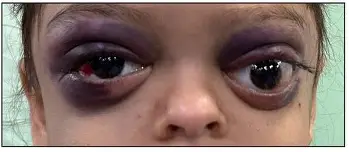
Head Injury assessment: (5)
s/s increased ICP
laceration/hematoma @ site
skull fracture
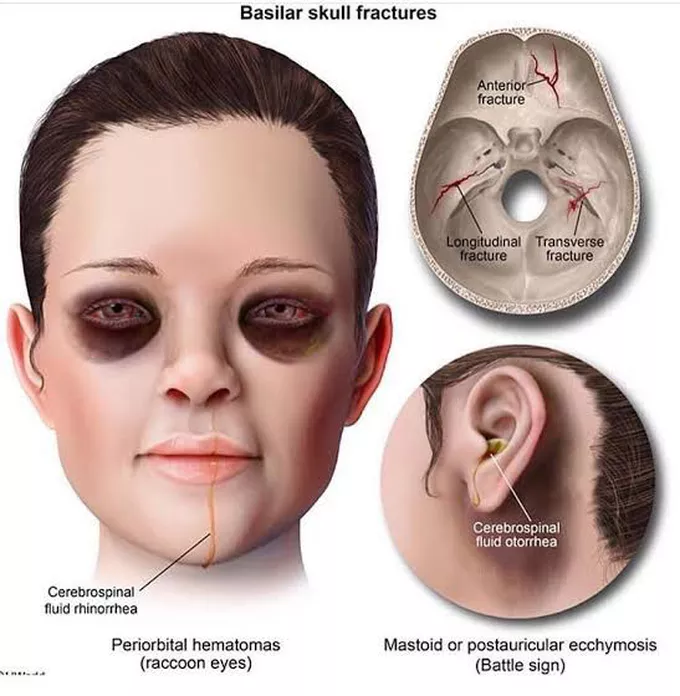
hemotympanum
blood behind ear drum (use otoscope)
periorbital ecchymosis (raccoon eyes)
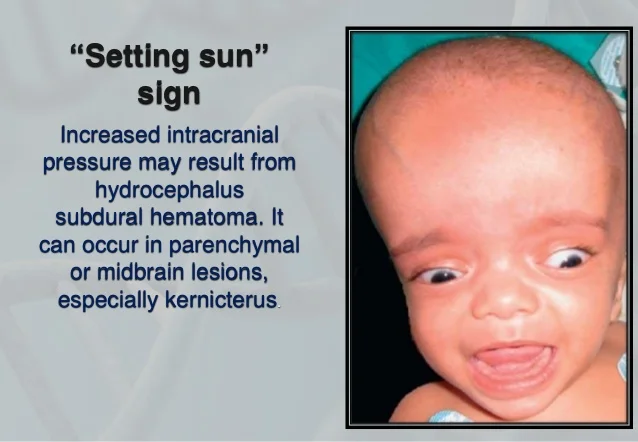
Early signs of head trauma in infants: (5)
bulging fontanel (⬆ICP)
sun setting eyes (driven downward bilaterally—usually in hydrocephalus)
separation of cranial sutures
increased sleep
poor feeding
Late signs of head trauma: (4)
pupillary changes
posturing (Decorticate/Decerebrate)
Cheyne-stokes respirations
CUSHINGS triad

Define Cushing’s Triad and how does it present: (3)
LATE sign ⬆ICP
HTN (⬆systolic BP + wide pulse pressure)
bradycardia
Irregular resp
Nurse management for Head Injuries-basic: (9)
Cervical collar (DONT flex head)
Assess fluid drainage from ears/nose (CSF)
Seizure precautions
pad rails
nothing in mouth
Keep body aligned
Minimize suction/cough/blow nose (⬆ICP)
Stool softener
LOC
PERRLA
GCS

Basilar skull fracture signs: (2)
Basilar
base of skull
raccoon eyes
CSF leak
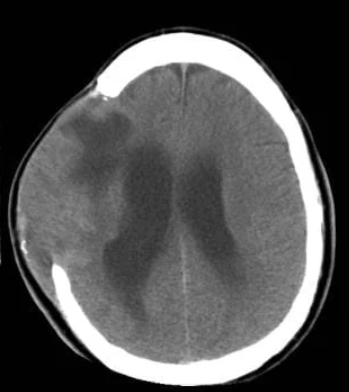
4 complications of skull fractures
epidural hematoma
causes rapid neuro decline
subdural hematoma
bleed after head injury
causes ⬆ICP→ HA, slurred speech
cerebral edema
⬇blood flow to brain
⬆ICP
brain herniation
brain tissue shifts d/t high ICP (life threatening!!)
Cushings
loss of blinking & gag reflex
pupils dont react to light
Infant GI system compared to older kids: (5)
smaller stomach capacity→ need frequent feeds
low esophageal sphincter tone → increased reflux
slower gastric emptying
immature liver function→ limited drug metabolism
higher fluid needs d/t faster peristalsis
Feeding and digestions in infants: (4)
suck/swallow/breathe develops @ 34-36 weeks
breastmilk easier to digest then formula
immature enzymes (amylase and lipase)
introduce solids @ >6 mon.
look @ changes in stool
C/D

What physical assessments important in pediatric GI evals?
hx (2)
inspection (2)
auscultation (1)
palpation (3)
history:
subjective:
amt of stool/characteristics
diet/feeding patterns
if they were sick
pain
objective: growth (h/w)
hydration status
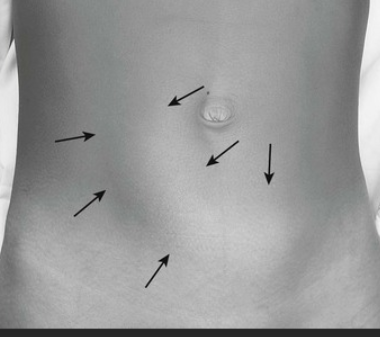
inspection
distention
visible peristalsis
auscultation
hyper/hypo-active bowels
palpation
tenderness
mass
rigid

GI Red flags in peds that needs immediate evals: (7)
bilious vomiting
means intestinal blockage
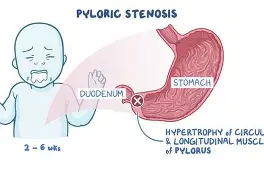
projectile vomit
d/t pyloric stenosis
failure to thrive
d/t poverty, SDOH
multiple kids, fixed income→ dilute formula
chronic illness (CF)
severe dehydration
sunken fontanels/eyes
lethargic
bloody stools
intestinal injury
absent bowels sounds
obstruction (mass/poop) → perforation → peritonitis
persistent abd pain
appendicitis
infx
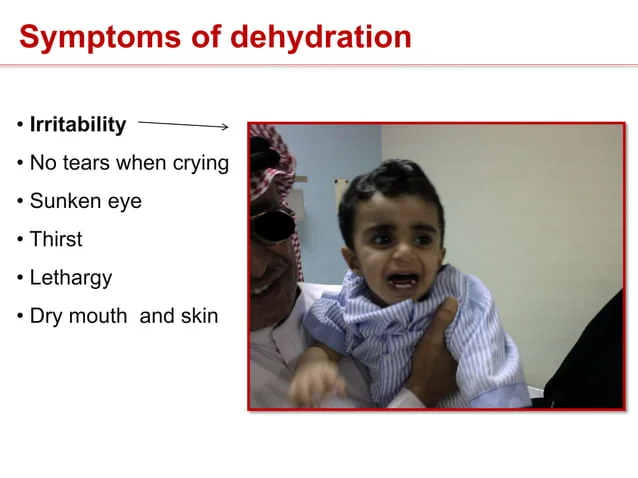
Common cause/risk factors for dehydration: (5)
V/D
dont drink fluids
viral/bacterial infx
rotavirus
salmonella
e.coli
c.diff
crowded environments (sick→ dehydrated)
contaminated water

s/s severe dehydration: (9)
sunken fontanels
lethargic
oliguric + concentrated urine
dry mucous membranes
< 6-8 wet diapers/day
no tears when crying
skin turgor > 3 sec
pale
hypotensive
Nurse care for dehydrated child: (3)
oral rehydration: mild 40-50 mL/kg over 4 hrs
moderate 100mL/kg over 4 hrs
no juice/caffeine/soda/jello/broths (salty)
draw labs
CBC
BUN/Cr
Urine specific gravity
stool test (tape test for pinworms)
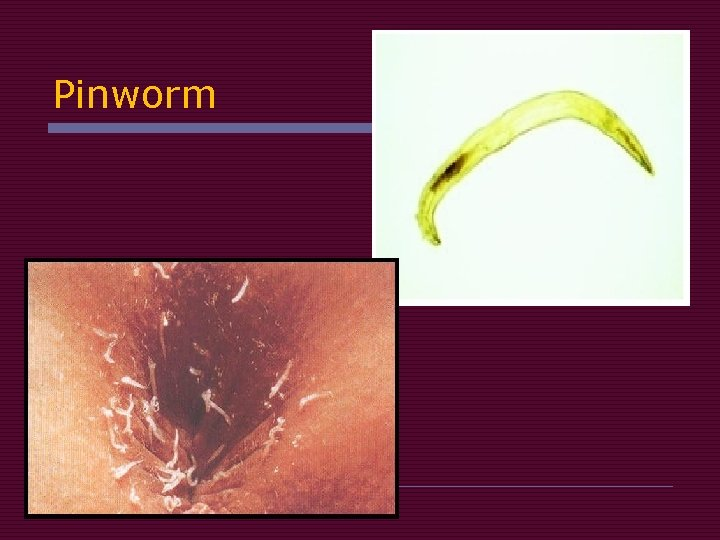
Pinworm infx (enterobiasis)
how it spreads (3)
symptoms (2)
diagnosis (1)
→ spreads through
1) contaminated hands (scratching butt then touching mouth)
2) Dirty toys/ surfaces
3) Close contact with infected children
→ s/s:
itchy butthole
restless sleep
→ dx:
tape test
Clear tape pressed against the butthole in the morning before bathing
worm eggs stick to tape
What parent education helps prevent GI infx? (6)
rotavirus vax
shower/ skin care daily
babies are exception bc they dont get as dirty
changes undies daily
clip nails (pinworms)
no sharing cup/utensils
no undercooked/raw meats
GERD s/s in children (5)
excessive spitting up
projectile vomiting
back arching
heartburn/ abd pain
poor weight gain

Interventions for GERD: (4)
upright feeding
burping
smaller, frequent feeds
no caffeine, citrus, spicy, peppermint for older children

Pyloric stenosis s/s: (4)
projectile, non-bilious vomit
olive shaped mass in RUQ
visible peristalsis
metabolic alkalosis (vomiting)
Common causes of pediatric constipation: (5)
holding stool in
transition from cows milk
toilet training stress
fear of public/school bathrooms
painful and doesnt want to go

What is encopresis and s/s: (4)
repeated involuntary stool leakage bc of chronic constipation
s/s basically same as constipation:
low fiber
not enough fluids
fear of toilet during training
fear of public restrooms
tx for encopresis: (3)
empty colon w/ laxatives/enemas
schedule toilet time after meals (30 mins)
gradually reduce bowel meds
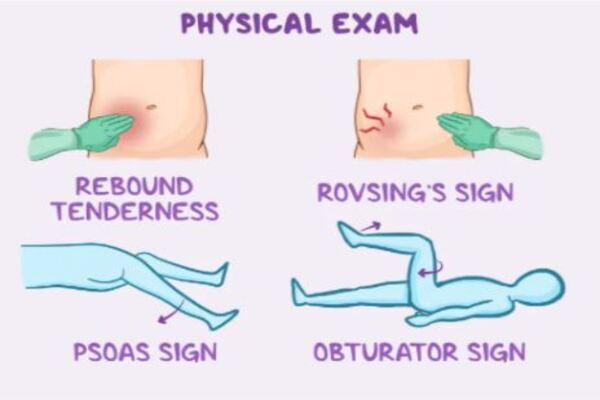
s/s of appendicitis: (6)
periumbilical pain→ RLQ pain
anorexia
guarding
rebound tenderness
pain w/ mvmt (jumping/ coughing)
N/V/D/C

signs of perforation: (4)
sudden relief of pain, then extreme pain
rigid abd
high fever
toxic appearance
appendicitis physical exams: (4)
McBurneys point tenderness: RLQ pain when pressing down
rovsings sign: pain in RLQ when left side is pressed
psoas sign: pain in right abdomen when right leg lifted
obturator sign: pain when hip and knee are bent and the leg is rotated inward
Nursing care for appendicitis: (4)
no heat to abdomen
no enema or laxatives
IVF
NPO
Define intussusception:
include age
bowel blockage in 3 mon.-6 yrs where part of intestine telescopes into another
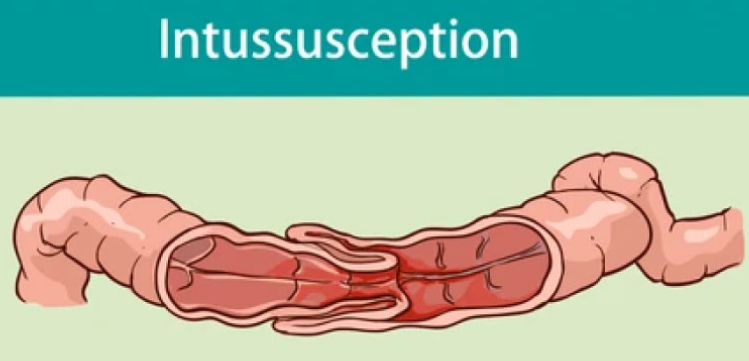
s/s of intussusception: (4)
knees drawn to chest
sausage shaped abdominal mass in RUQ
“Dance sign”: bowel shifts out of the RLQ, leaving that area empty due to telescope
stools mixed w blood, mucus “jelly stool”
What causes Hirschsprung Disease?
no ganglion cells in colon → NO peristalsis
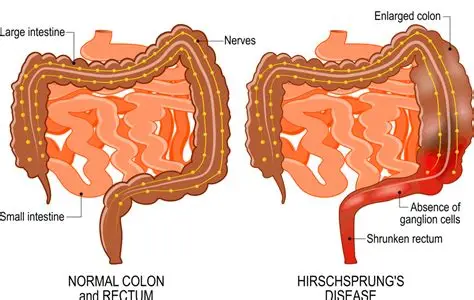
Cardinal sign of Hirschsprung disease in newborn?
FAILURE to pass meconium w/in 24-48 hrs after birth
Symptoms of Hirschsprung disease in infant/children? (5)
foul smelling stool
ribbon-like or pellet-like poop
distention
undernourished, anemic appearance
palpable fecal mass

Whats the most common cause of UTIs in children?
Escherichia Coli (E.Coli)
UTI risk factors: (11)
Vesicoureteral Reflux: pee flows backwards from bladder → ureters/kidneys
urinary stasis (holding pee)
catheters
uncircumcised male (not cleaned well)
female (urethra close to rectum)
tight/synthetic undies
wet bathing suits
bubble baths
pinworm infx
sexual activity (pee after)
toilet training stage

What are UTI symptoms in infants? (8)
hematuria
crying w/ urination
jaundice
cyanosis
V/D
irritable/lethargic
poor feeding
fever/hypothermia

manifestation of pee in UTIs: (4)
thick and cloudy w/ mucous
pyuria (WBC in urine)
bacteria in urine
foul odor
UTI symptoms in older children? (5)
fever w/ severe flank/abd pain (leukocytosis→ pyelonephritis)
hematuria
dysuria (malodourous)
incontinence in toilet trained child
boys dribble when peeing
Nursing actions for UTIs: (3)
drink water!
frequent peeing + total emptying of bladder
push on bladder
high fiber!! (prevent constipation)
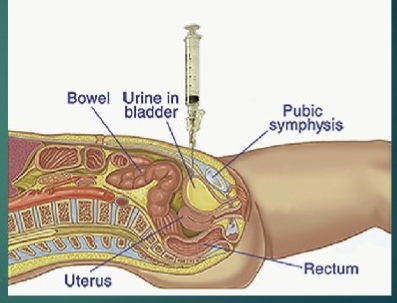
How to collect urine: (3)
clean catch method/ or take from catheter
collect midstream urine
collect first morning urine
help w/ suprapubic aspiration if needed
UTI parent education: (8)
wipe front to back
“double voiding”
wear cotton/loose undies
dont stay in wet clothes
NO bubble baths/hot tubs/whirlpools
clean foreskin
void after sex
no caffeine

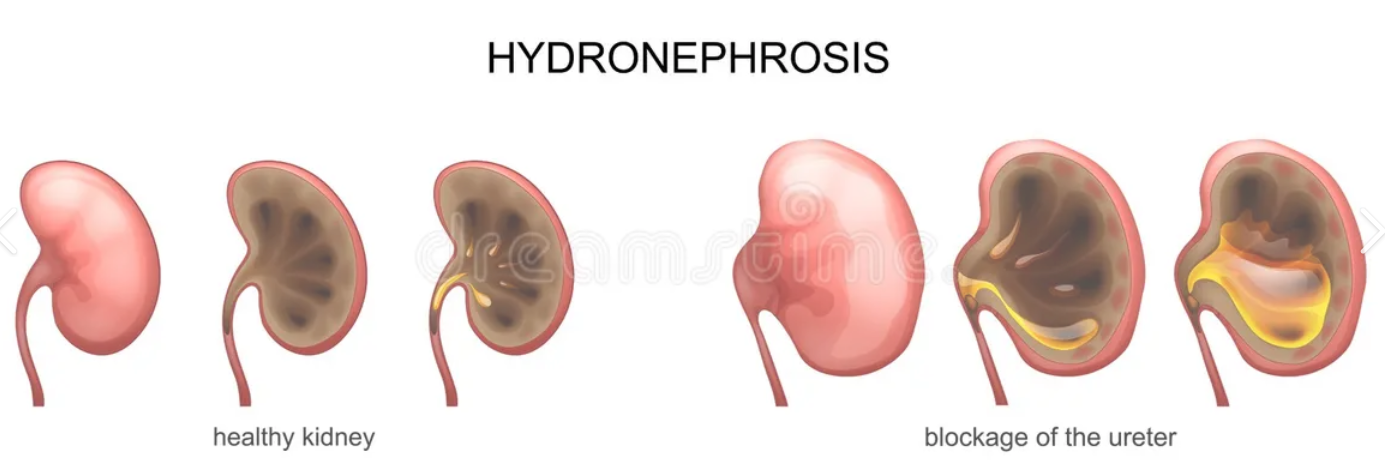
whats hydronephrosis?
causes? (2)
swelling of kidney due to buildup of pee when obstructed
Vesicoureteral Reflux
kidney stones
whats Nephrotic Syndrome?
kidneys leak protein into urine (preschoolers 2-3 years old)
proteinuria
signs of nephrotic syndrome: (7)
edema
periorbital (face)
generalized anasarca (abdomen, genitals, legs)
weight gain
ascites
frothy dark urine
pallor white lines in nails (Muehrcke)
anorexia
lethargic/irritable/fatigue

Nursing interventions Nephrotic syndrome: (5)
monitor daily weights and urine protein
strict I/O
skin care
LOW Na diet
elevate edematous parts (legs)
complications: clots/circulatory insufficiency

Parent education Nephrotic syndrome: (3)
Check loss of protein in urine
Low Na diet
monitor clotting risk/PE
anticoagulants lost in urine = ⬆platelets (500,000-1,000,000)
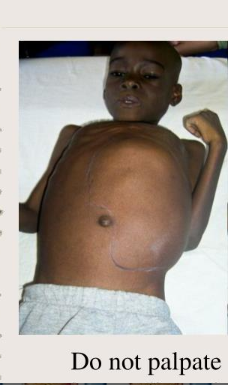
Whats Wilms Tumor?
most common kidney cancer in children (2-3 y/o)
key nursing precaution for Wilms Tumor: (3)
DONT palpate abdomen!! (can rupture it(
prep for nephrectomy
NO contact sports!!!!