Oral Pathology LO 6
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
59 Terms
Developmental disorder
A failure during the process of cell division and differentiation into various tissues and structures. Some may be identified clinically, by radiographic examination, biopsy, or histologic examination.
Inherited disorder
This is a developmental disorder caused by an abnormality in genetic makeup.
Congenital disorder
This is a developmental disorder that is present at birth. May be inherited or developmental. The cause of most ——————— abnormalities is unknown.
Ankyloglossia
An extensive adhesion of the tongue to the FOM. Can effect feeding and speech. Treatment: frenectomy

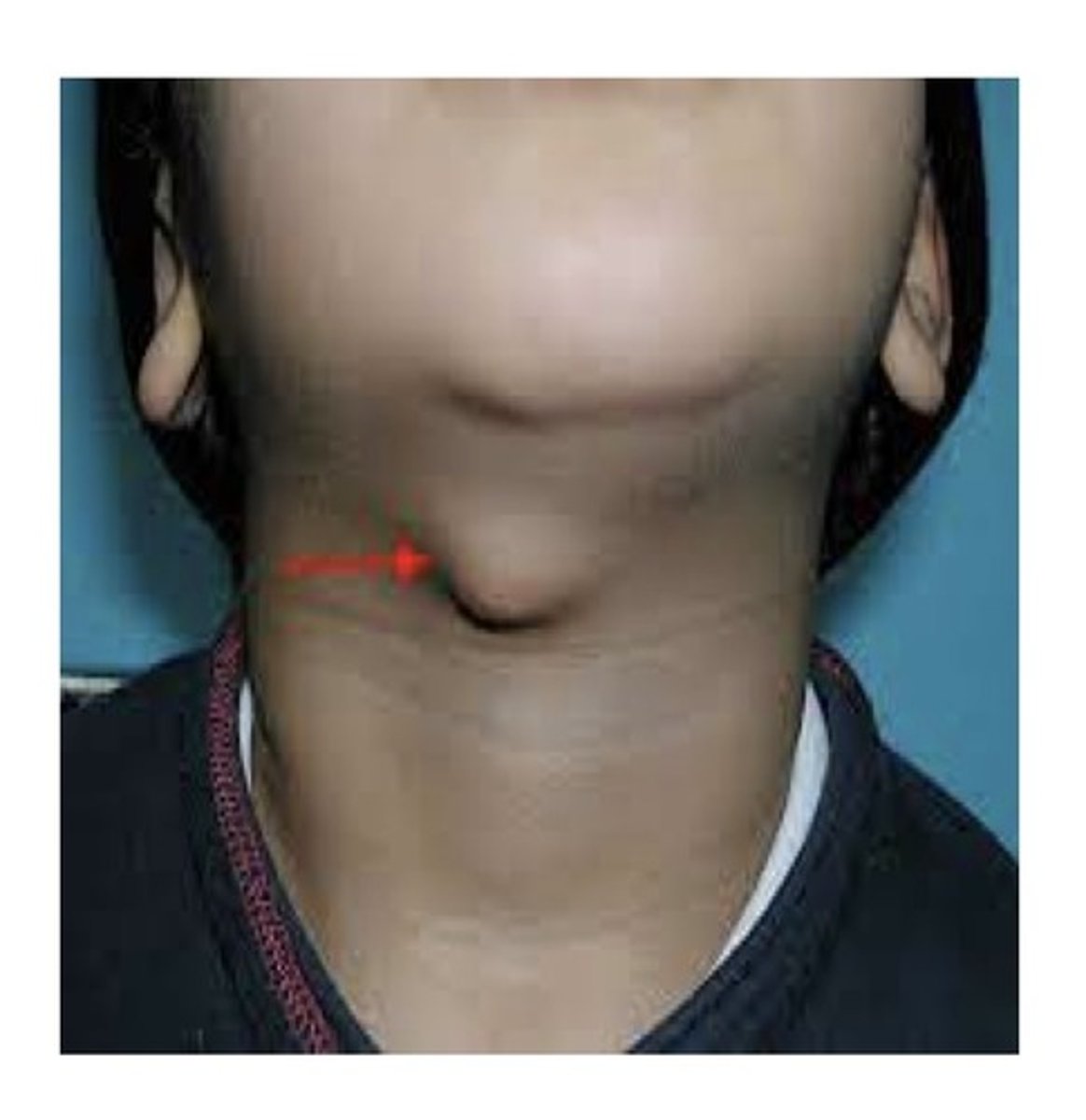
Lingual thyroid
This is a small mass of thyroid tissue located on the tongue. Results from the failure of the primitive thyroid tissue to migrate from its developmental location in the area of the foramen cecum on the posterior portion of the tongue to its normal position in the neck. Tx: it may be removed if it is obstructive, provided the patient has other functioning thyroid tissue.
Developmental cysts
An abnormal fluid-filled epithelium-lined sac or cavity.
Radicular cysts (periapical cyst) and residual cyst
What are the 2 most common oral cysts?
Odontogenic or non odontogenic
Developmental cysts are classified as either ———————— or ——————————.
Intraosseous (occur within the bone) or extraosseous (occur in soft tissue)
Developmental cysts can cause expansion of bone. They are either ———————— or ————————.
Intraosseous (within bone)
This type of developmental cyst generally appears as a well-circumscribed radiolucency. (Intraosseous or extraosseous)
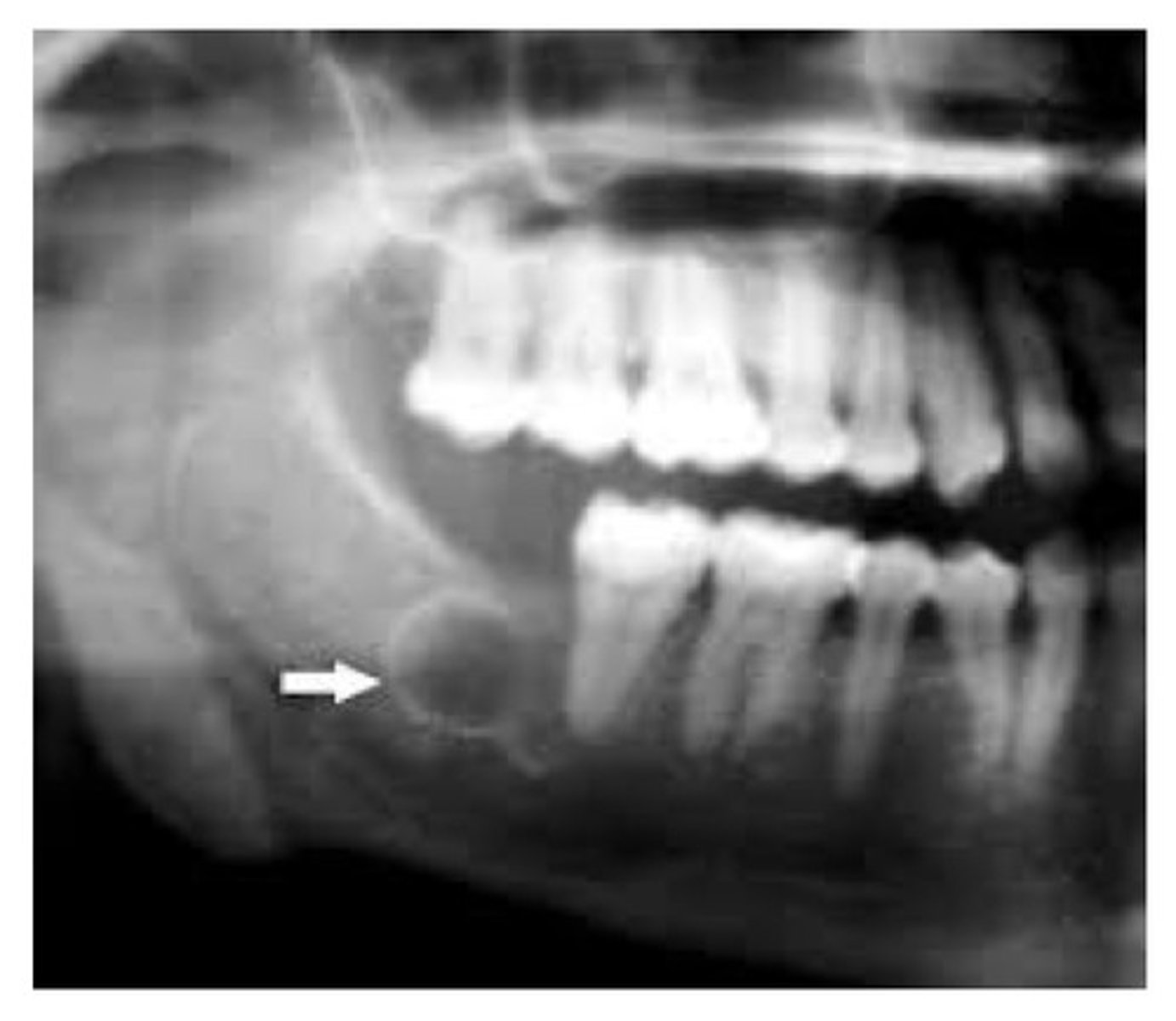
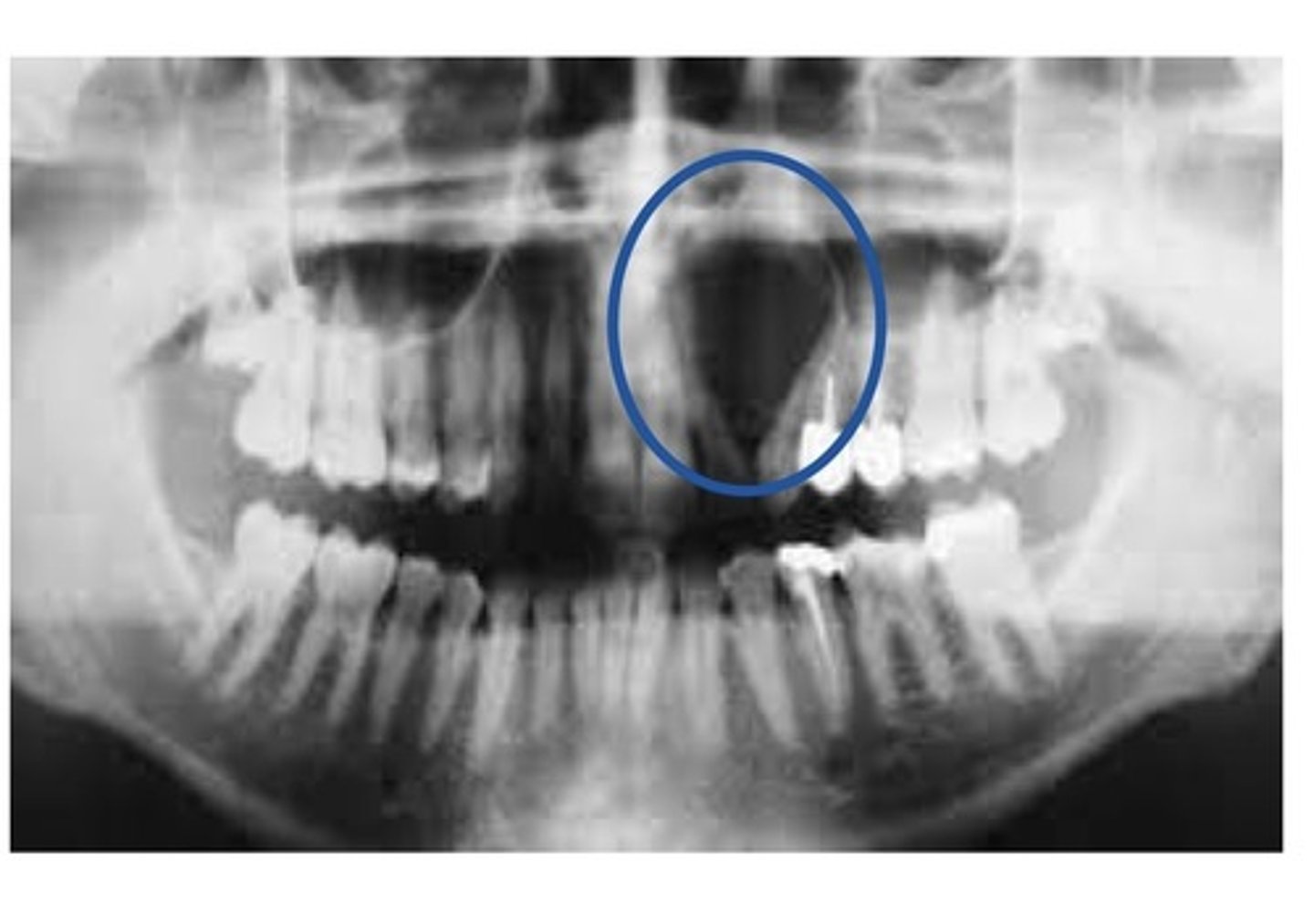
Odontogenic: Dentigerous cyst (follicular cyst)
This is a common type of cyst that forms around the crown of an unerputed or developing tooth. The epithelial lining originates from the reduced enamel epithelium (REE) after the crown has formed and calcified. Most commonly occurs around the crown of an unerupted or impacted third molar.
Radiographically: a well-defined, unilocular radiolucency around the crown of an unerupted or impacted tooth.
Treatment: removal of the cyst as there is some risk of cystic transformation into a neoplasm.
Odontogenic: Eruption cyst
Similar to a dentigerous cyst. Found in the soft tissue around the crown of an erupting tooth. Occurs only on primary teeth, fairly common. Pain associated with inflammation only, very small risk of infection. No tx.

Odontogenic: Primordial cyst.
This cyst develops in place of a tooth. Most commonly in place of a 3rd molar. Most often seen in young adults and discovered on radiographic exam. Tx: surgical removal.
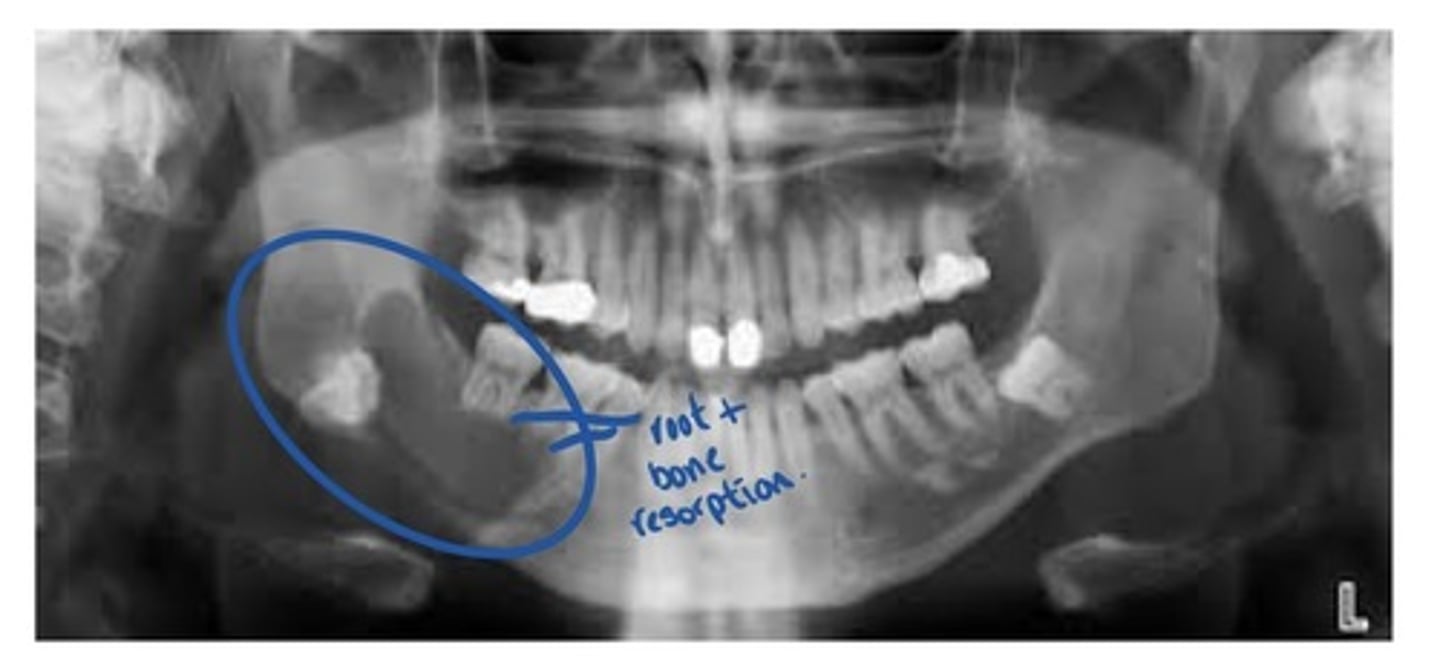
Odontogenic: keratocyst (OKC)
This type of cyst is most often seen in the mand 3rd molar region. Can move teeth and cause resorption. Tx: high recurrence rate so, surgical removal with osseous curettage is recommended. Radiographic: frequently appears as a well defined, multilocular, radiolucent lesion.

Calcifying odontogenic cyst (COC)
A non aggressive, cystic lesion lined by odontogenic epithelium
Closely resembles an ameloblastoma
Characteristic feature called ghost cells

lateral periodontal cyst
Cyst most often seen in the mandibular cuspid and premolar area. An asymptomatic, unilocular or multilocular radiolucent lesion on the lateral surface of a tooth root. If its Intraosseous, it's called a ————— ——————— ————. If it's extraosseous, it's called a gingival cyst.

Botryoid odontogenic cyst.
multilocular variant of lateral periodontal cyst.
Glandular odontogenic cyst (GOC)
Enlargement of bone-posterior mand and anterior max.
Male and female. 50-59 yrs (menopause). Appears similar to ameloblastoma or odontogenic keratocyst (OKC) high recurrence rate.
Microscopic appearance: multi cystic lesions. Eosinophilic cuboidal cells on the surface of the epithelial, columnar cells with cilia, intraepithelial microcysts, epithelial thickenings show whorls of cells similar to lateral periodontal cyst and botryid cyst.
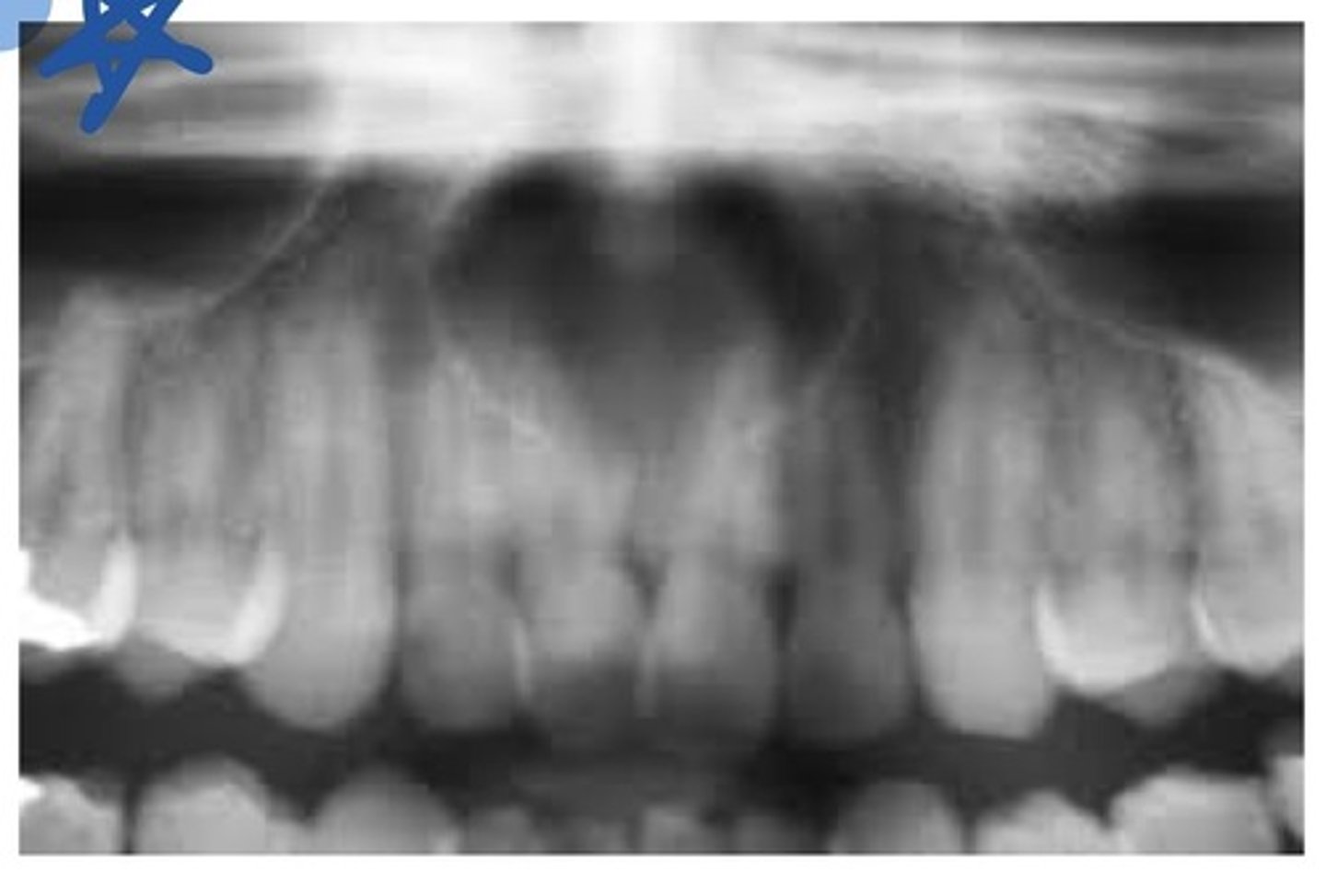
Non-odontogenic: nasopalatine canal cyst (incisive canal cyst)
This is a cyst located within the nasopalatine canal or the incisive papilla. More common in men, 40-60 yrs. Usually asymptomatic. May see a small, pink bulge near the apices and between the roots of the maxillary central incisors on the lingual surface. Client may have a salty taste (nasal fluid salty).
Non-odontogenic: Median palatine cyst
A well-defined, unilocular radiolucency. Located in the midline of the hard palate. Lined with SSE surrounded by dense fibrous connective tissue. Tx: surgical removal.

Non-odontogenic: nasolabial cyst
A soft tissue cyst. Thought to originate from the lower anterior portion of the nasolacrimal duct. Observed in adults 40-50 years of age. 4:1 in favour of females (menopause). Salty taste.

Non-odontogenic: lymphoepithelial cyst
Most commonly found in major salivary glands. Epithelial lining surrounded by a well circumscribed component of lymphoid tissue. Appears to arise from epithelium trapped in a lymph node during development. Most commonly found intraorally on the FOM and lateral boarders of the tongue. Appears as a pinkish-yellow raised nodule. Tx: surgical excision.

Pseudocysts
These are not true cysts because they are not lined by epithelium.
Nonodontogenic: dermoid cyst
A developmental cyst often present at birth or noted in young children. Usually found on the floor of the mouth when it is located in the oral cavity. May cause tongue displacement. May have a doughy consistency when palpated.
Nonodontogenic: thyroglossal tract (duct) cyst.
Cyst that forms along the tract the thyroid gland follows in development. Found in young individuals (<20 yrs of age). No sex predilection. Tx: excision of the cyst and tract.
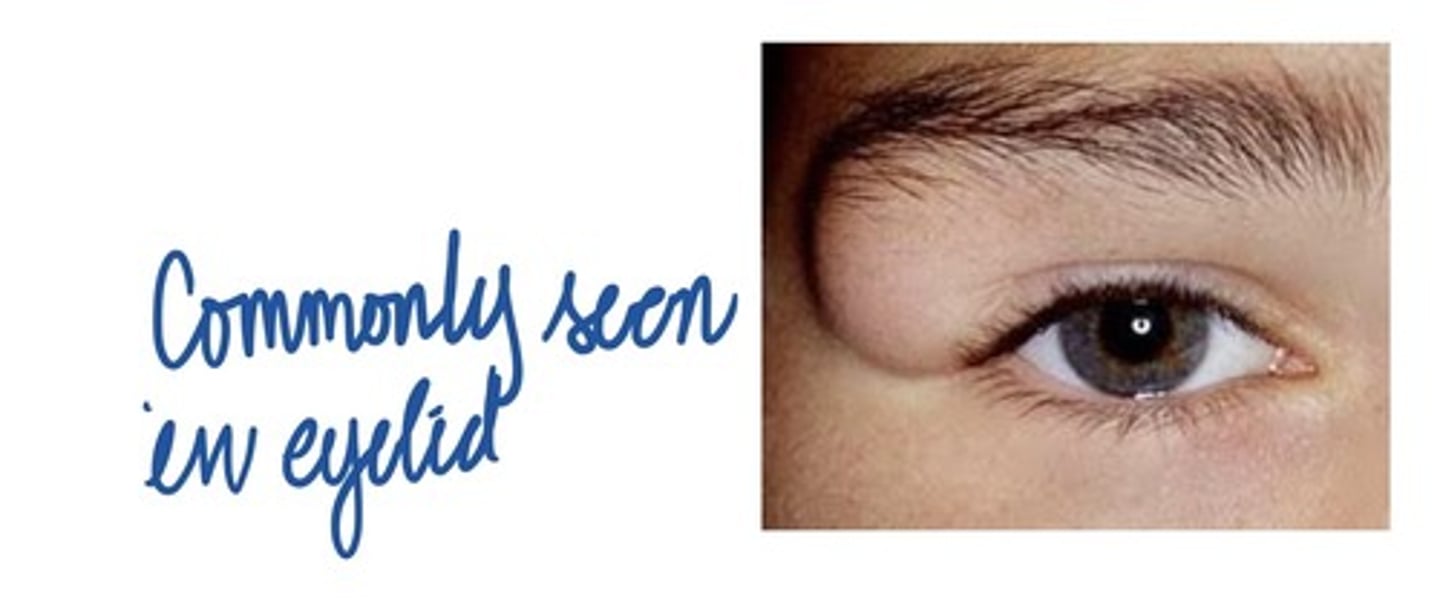
Nonodontogenic: Epidermal cyst
A raised nodule on the skin of the face or neck. May be noted intraorally on occasion. Lined by keratinized epithelium that resembles the epithelium of the skin. Lumen is filled with keratin scales. Tx: surgical excision.

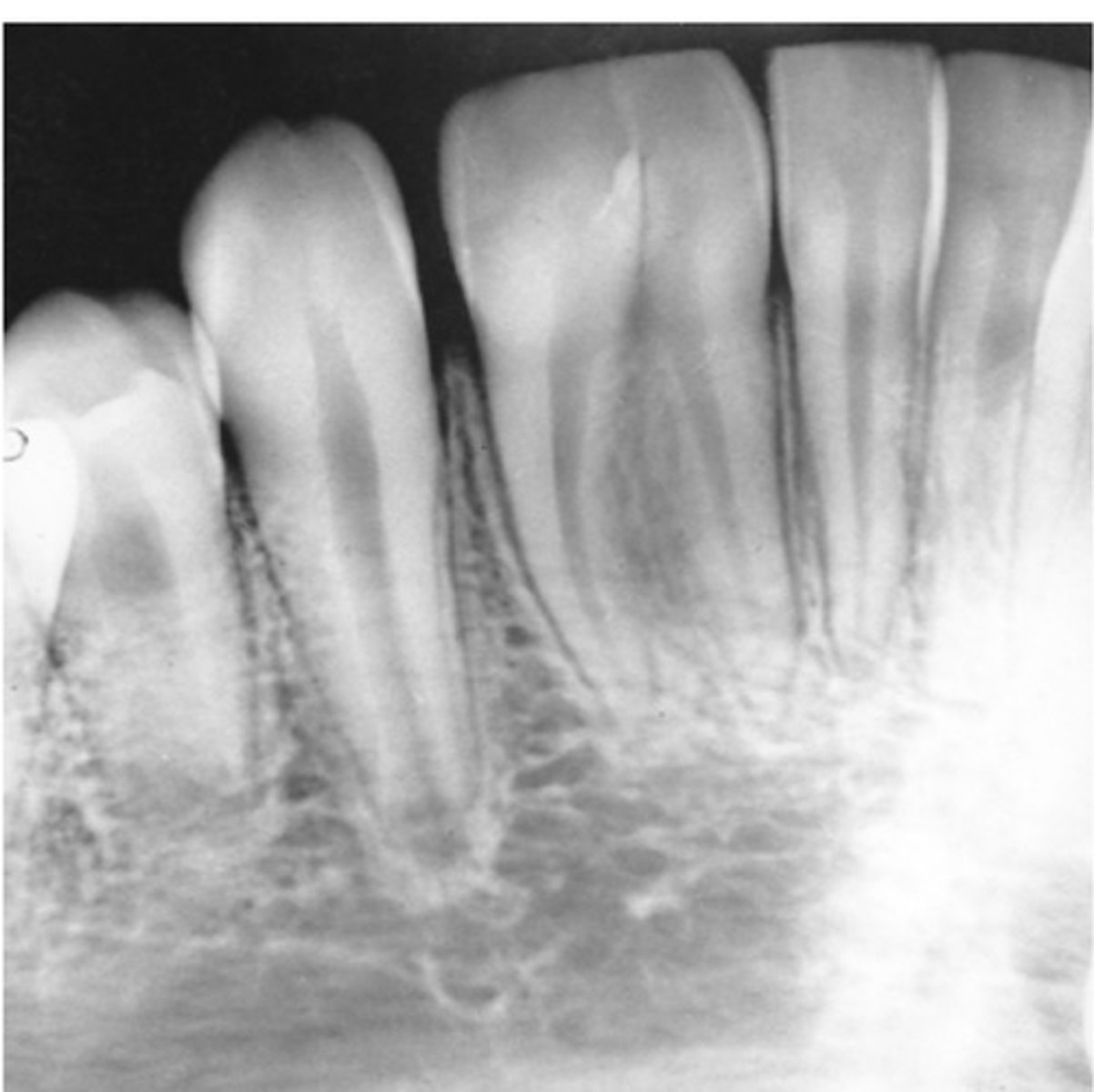
Simple bone cyst
A pseudocyst, pathologic cavity not lined with epithelium. May be associated with trauma. Radiographic: a well defined unilocular or multilocular radiolucency. Characteristically shows scalloping around the roots of teeth. Tx: curettage on the wall lining in the void.
Aneurismal bone cyst
A pseudocyst that consists of blood filled spaces surrounded by multinucleated giant cells and fibrous connective tissue. Radiographic: multilocular appearance! Usually seen in persons less than 30 years/o, slight predilection for females. Tx: surgical excision.
Nonodontogenic: Globulomaxillary cyst.
A well defined, pear-shaped radiolucency located between the roots of the maxillary lateral incisor and cuspid. Tx: surgical removal. Pokes into sinuses and may cause a salty taste or infection.
Ectodermal dysplasia
Anodontia is the congenital lack of teeth. Total anodontia is lack of all teeth. May be associated with this condition:
Stafne defect
-A pseudocyst
-Not a pathologic cavity
Clinically: An anatomic depression on the posterior lingual area of the mandible
Treatment: None
Lined with thickened bone which makes it look radiopaque

Hypodontia
Lack of one or more teeth. Tends to be familial, or a component of a syndrome.
Mandibular incisor
what is the most common missing deciduous tooth?
Supernumerary teeth
Extra teeth. May result from formation of extra tooth buds in the dental lamina or from the cleavage of already existing tooth buds. May occur in either deciduous or permanent dentition. Most often seen in the maxilla.
Dentigerous
What is the most common type of cyst around unerupted teeth?
Mesiodens
The most common supernumerary tooth. Located between the max incisors, may be inverted when seen on rads.
Distomolar
This is the 2nd most common supernumerary tooth. Located distal to the 2rd molar.
Cleidocranial dysplasia or Gardner syndrome
Multiple supernumerary teeth may be associated with these 2 conditions:
Max lateral and max 3rd molar
The 2 teeth that are most commonly effected by microdontia are:
True generalized microdontia
This is seen in a pituitary dwarf; all teeth are smaller than normal.
Generalized relative microdontia
This is when normal sized teeth appear small in a large jaw.
Microdontia
1 or more teeth are larger than normal. True ——————— is seen in cases of pituitary gigantism. Relative generalized ——————— is when teeth appear large in a small jaw.
Hemihypertrophy
Macrodontia affecting a single tooth may be seen in cases of faclial:
Enamel hypoplasia
This means that there is not enough cells of enamel or the cells are defective.
Turners tooth
Enamel hypoplasia on one tooth is called:
Enamel hypo calcification
A developmental anomaly resulting ion a disturbance in the maturation of the enamel matrix. Usually appears as a chalky, white spot on the middle 3rd of smooth crowns. The underlying enamel may be soft and susceptible to caries.
Gemination
A single tooth germ attempts to divide in 2. Appears as 2 crowns joined together by a notched Incisal area. Radiographically: usually one single root and one common pulp canal. Pt has full complement of teeth.

Fusion
The union of 2 normally separate adjacent tooth germs. Appears as a single large crown that occurs in place of 2 normal teeth. Radiographically, either separate or fused roots and root canals are seen. Patient is usually short one tooth.
Dilaceration
An abnormal curve or bend in the root of a tooth. Usually discovered on a radiograph. May cause a problem if the tooth must be removed or a root canal performed.

Hypercementosis
Excessive cementum on the roots of the teeth. occurs in adults; incidence and amount increase with age. Feature associated with several local and systemic factors. No treatment necessary.
Talon cusp
An accessory cusp located in the cingulum area of a max or mand permanent incisor. Contains a pulp horn. May interfere with occlusion.

Concrescence
Usually adjacent teeth are united by cementum. Usually discovered on a radiograph.

Erythroblastosis fetalis.
This condition may cause endogenous staining of teeth. This condition is due to Rh incompatibility- fetus and pregnant person have different blood types. Mom's body "attacks" fetus bc it's seen as an intruder. This causes stain.
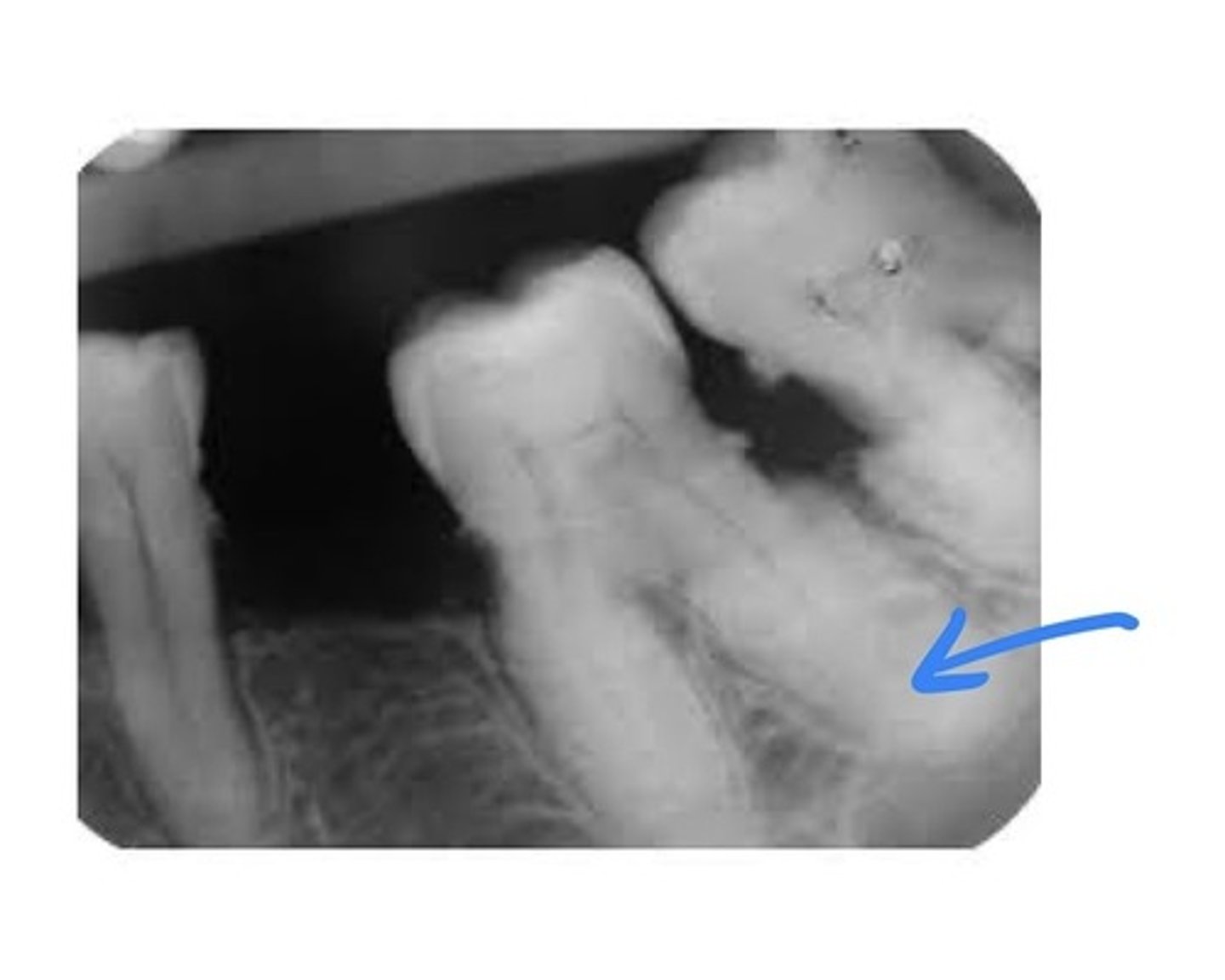
Enamel pearl
A small, spherical enamel projection on a root surface. Usually found on maxillary molars. Sadiographically, it appears as a small, spherical radiopacity. Removal may be necessary if periodontal problems occur in the furcation.

Enamel hypoplasia
This is an umbrella term. An incomplete or defective formation of enamel. May be due to many factors, including: amelogenesis imperfecta (most severe), febrile illness, vitamin deficiency, infection of a deciduous tooth, ingestion of fluoride, congenital syphilis, birth injury, premature birth, idiopathic factors.

Taurodontism
The teeth have elongated pulp chambers and short roots. May occur in both deciduous and permanent dentition. Identified on radiographs. Resemble teeth of bulls.

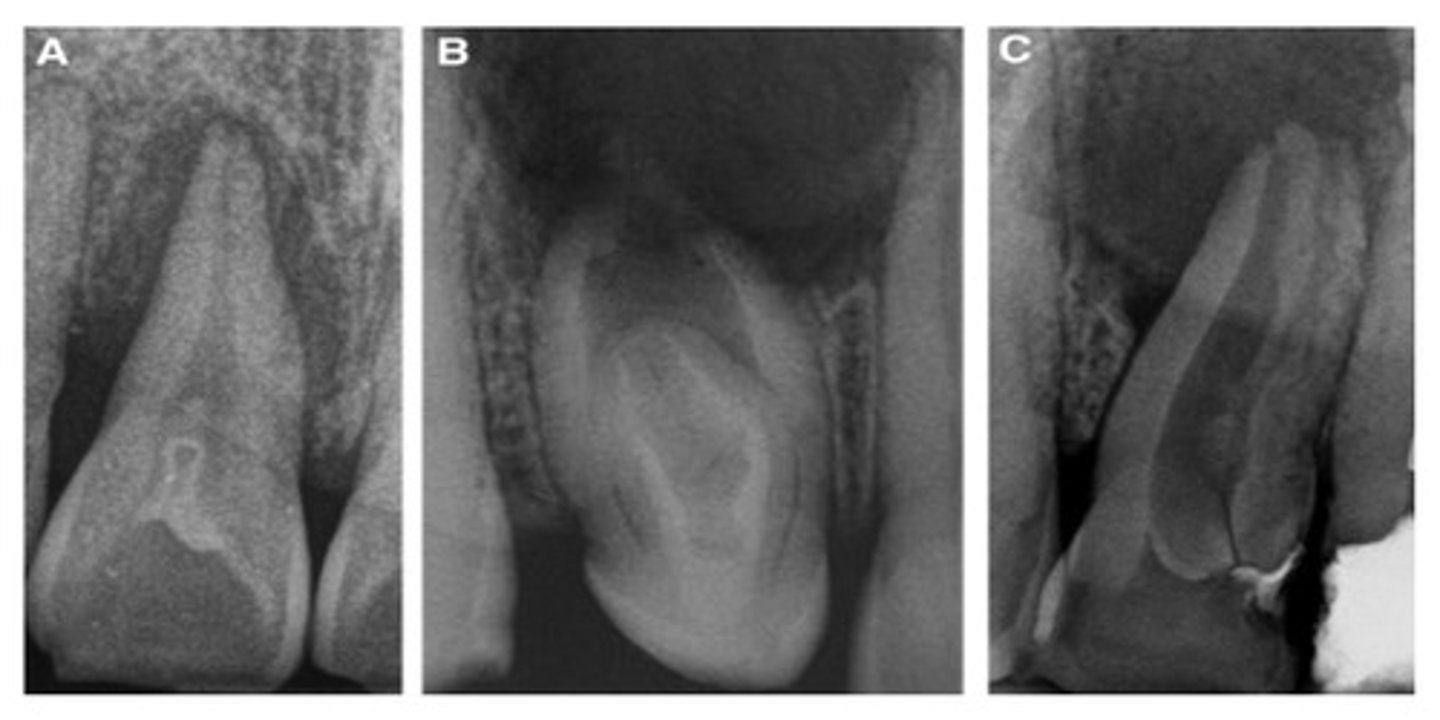
Dens invaginatus a.k.a. Dens en dente
Occurs when the enamel organ invaginates into the crown of a tooth before mineralization. Radiographically, it appears as a toothlike structure within a tooth. Vulnerable to caries, pulpal infection, and necrosis.
Dens evaginatus
An accessory enamel cusp found on the occlusal tooth surface. Most often seen on mand premolars. May cause occlusal problems.

Regional odontodysplasia (ghost teeth)
Exhibit a marked reduction in radio density and a characteristic ghostlike appearance. Very thin enamel and dentin are present. Usually treated by extraction.
