Psychopathology: AQA A-Level Psychology
1/108
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
109 Terms
1) Definitions of abnormality, including deviation from social norms, failure to function adequately, statistical infrequency and deviation from ideal mental health.
What are the four criteria for abnormality?
- Deviation from social norms
- Failure to function adequately
- Deviation from ideal mental health
- Statistical infrequency
What is meant by 'deviation from social norms'?
When someone behaves in a way that violates social norms.
There is a distinction between desirable and undesirable behaviours.
What is an example of deviation from social norms?
ASPD (Anti-social personality disorder):
- Absence of prosocial internal standards.
These are associated with a failure to conform to lawful and culturally normative ethical behaviour.
What are some limitations or weaknesses of 'deviation from social norms'?
1. Ignores the role of context.
- For example, washing hands 50 times a day is considered abnormal as it deviates from social norms.
- However, if this person was a surgeon, this behaviour would be completely normal as it is a job requirement.
Does not take contextual factors into account; questions validity, as we may falsely claim that a person is abnormal when they are actually normal.
Could lead to misdiagnosis / people receiving unneeded treatments.
2. Ignores that social norms change over time.
- E.g. Homosexuality was not removed from the DSM until 1990
Questions temporal validity; we cannot classify / guarantee someone as abnormal in today's society because attitudes constantly change.
3. Culturally relative.
- Social norms vary within and across cultures.
- E.g. being naked in public in Britain = abnormal
- In some cultures e.g. native tribal communities is natural = not abnormal.
Questions population validity, cannot be generalised
What is meant by 'failure to function adequately'?
When a person's behaviour suggests that they cannot cope with everyday life.
Focuses on the everyday behaviour of the individual.
What is an example of 'failure to function adequately'?
Depression:
Someone may be unable to get out of bed in the morning, and be unable to maintain a normal pattern of behaviour.
What criteria did Rosenhan and Seligman (1989) propose for failure to function adequately?
1. Suffering; may suffer themselves, or inflict suffering on others
2. Maladaptiveness; behaviour prevents person from reaching goals/maintaining routine
3. Irrational, hard to understand
4. Observer discomfort; makes others watching feel uncomfortable
5. Vividness; others find the behaviour odd
6. Violation of moral codes; not behaving in accordance with society's norms
6. Unpredictable
What are some limitations of failure to function adequately?
1. Abnormality = not always accompanied by dysfunction.
- Those with psychopathy can commit murders and still appear normal.
- E.g. Harold Shipman; murdered 215 patients over 23 year period, maintained his ability to appear 'normal' (Outward appearance of being in a respected profession)
Questions the validity; may define abnormal people as normal because they can act normal. Leads to misdiagnosis, or leave them untreated/not convicted.
2. Ignores the role of context.
- People sometimes suffer from distress, which leads them to fail to function adequately.
- Losing a loved one; struggle to go to work or college
- Grieving = psychologically healthy and normal
Questions validity; can falsely label those going through stress as abnormal when they are actually normal.
3. Culturally relative.
- E.g. going home in the afternoon from work to sleep may be abnormal in Britain; in Spain, a siesta is normal.
Questions population validity; cannot be generalised, leads to false labelling of people as abnormal.
What is meant by 'deviation from ideal mental health'?
An absence of well-being, proposed by Marie Jahoda in 1958.
What is the criteria of 'deviation from ideal mental health'?
1. Self-actualization; ability to fulfill your potential
2. Ability to resist stress
3. Positive self-esteem, strong sense of identity
4. Ability to function as an independent person, take responsibility (autonomy)
5. Accurate perception of reality (e.g. not seeing things that aren't there)
6. Mastery of environment; competency in all areas of life
What are some limitations of deviation from ideal mental health?
1. Over-demanding criteria.
- Most people do not meet all the ideals.
- According to this, most people would be considered abnormal.
- E.g. we cannot always cope with stress effectively.
Questions the validity; can label people who are actually healthy as abnormal. + A high percentage of the population would be falsely considered abnormal.
2. Ignores that ideal mental health changes over time.
- E.g. in thirteenth century Europe, visions were a positive sign of religious commitment; nowadays it would be a sign of schizophrenia.
Questions the temporal validity; doesn't account for changes in perceptions of ideal mental health.
3. Culture-bound
- Some types of abnormality only exist in certain cultures.
- e.g. 'Koro'; a syndrome where a man believes his penis is fatally retracting into his body (SEA, China, Africa).
- Some of Jahoda's criteria for ideal mental health are firmly located in the context of the US and Europe.
- The concept of self-actualisation might be considered self-indulgent and dismissed in many other parts of the world.
- The value placed on independence varies greatly even in Europe; in Germany it is highly encouraged while in Italy, not so much.
- Also, what defines success in different parts of our lives is very different across cultures.
Questions the population validity; cannot be generalised
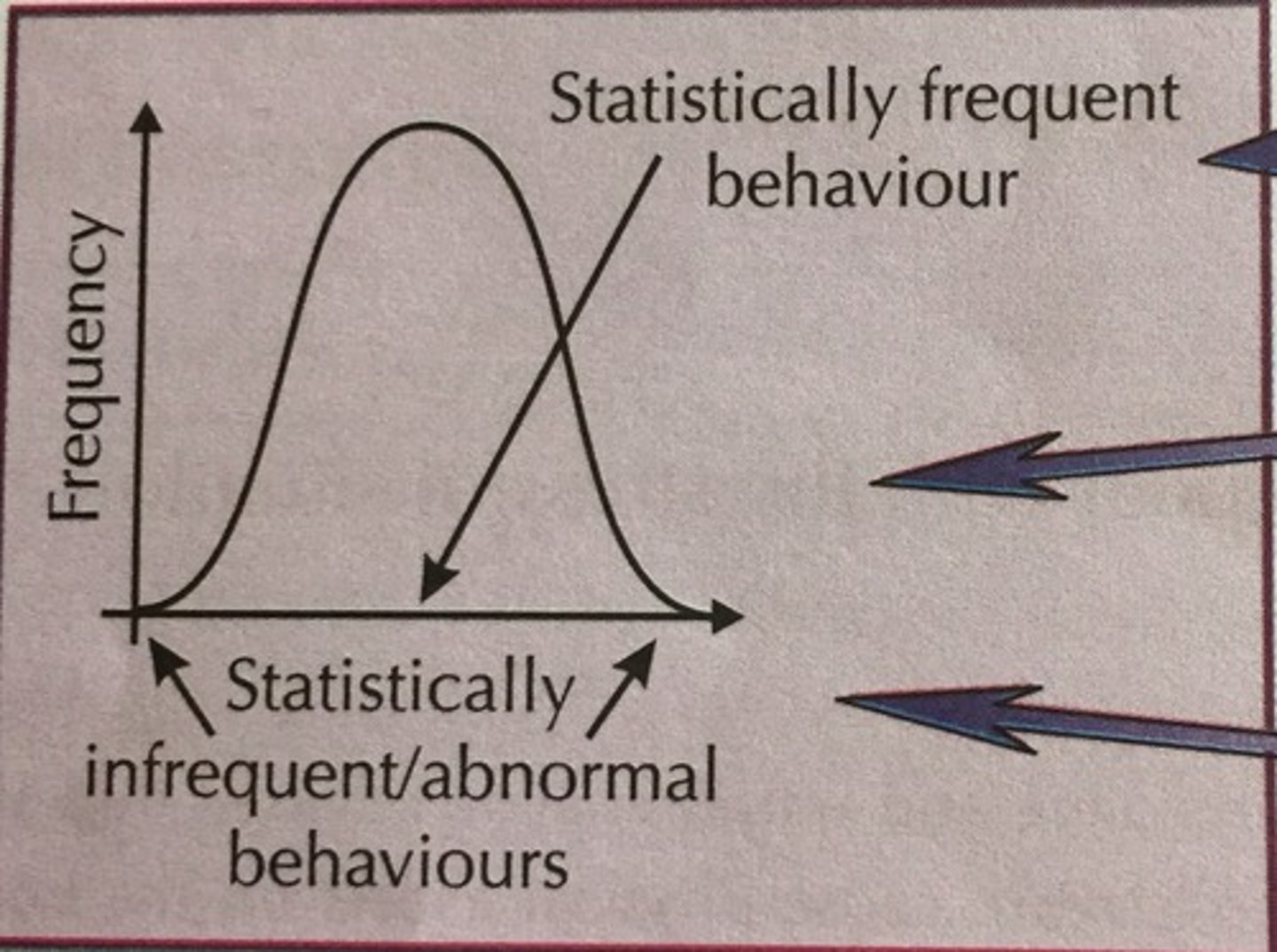
What is meant by 'statistical infrequency', or 'statistical deviation'?
Statistically unusual; when people fall outside of the middle of the normal distribution curve.
These people are defined as abnormal.
Human behaviour is abnormal if it falls outside of the range that is typical for most people.
What is a strength of statistical deviation?
1. Real life application
- Doctors can identify the severity of disorders e.g. depression for patients by seeing how statistically infrequent their symptoms are.
Adds to validity; it is able to have a positive impact on patients' lives and society.
What are some limitations of statistical deviation?
1. Unusual characteristics can be positive
- High IQ = may deviate from statistical norm; but is not undesirable.
- Their intelligence can positively contribute to society.
Questions the validity; can label those with desirable characteristics as abnormal because it is infrequent.
2. Not everyone benefits from a label.
- Dwarfism; height is not the same as the statistical average, but can still function well within society.
Questions validity; ignores that unusual/infrequent characteristics don't define functioning in society.
2) The behavioural, emotional and cognitive characteristics of phobias, depression and obsessive-compulsive disorder (OCD).
What is meant by a 'phobia'?
A phobia is an irrational and extreme fear of an object, situation, or activity.
It is disproportionate to the actual danger/risk it poses.
It interferes with normal living.
What are the three types of phobias?
1. Specific phobia
2. Social phobia
3. Agoraphobia
What is a specific phobia?
Any kind of anxiety disorder that amounts to an unreasonable or irrational fear related to exposure to specific objects or situations.
May be triggered by both the presence and anticipation of the object/situation.
What is a social phobia?
A long-lasting and overwhelming fear of social situations.
What is agoraphobia?
A fear of being in situations where escape might be difficult.
Criteria for specific phobias
1. Marked/persistent fear that is excessive or unreasonable.
2. Exposure almost always provokes immediate anxiety response.
3. Person knows the fear is excessive/unreasonable.
4. Phobic situation is avoided or endured with intense anxiety
5. Anxiety interferes significantly with person's normal routine
Behavioural characteristics of phobias
(How they act)
1. Panic
- Screaming, crying, heavy breathing
- Children might freeze, act clingy, or have a tantrum
2. Avoidance; avoiding situations that involve coming into contact with the phobic object.
3. Endurance; choosing to remain in the presence of the phobic stimulus.
E.g. someone with arachnophobia choosing to remain in a room with a spider to keep an eye on it rather than leaving.
Emotional characteristics of phobias
(How they feel)
1. High state of arousal around phobic object:
- Fear: intense but short term unpleasant state of high arousal from phobic stimulus
- Anxiety: unpleasant long term state of high arousal from phobic stimulus
2. Unreasonable emotional response
- Having a greater fear than what the phobic object should
Cognitive characteristics of phobias
(The way people think)
1. Irrational beliefs about phobic object
- E.g. arm exploding through blood pressure
2. Cognitive distortions (misinterpretations)
- What they think about the phobic object is different from the majority view.
E.g. butterflies are scary.
3. Selective attention to phobic stimulus
- Placing overt focus on the phobic stimulus to give the best chance of reacting quickly to a threat
What is the behavioural explanation for phobias?
Phobias are learned.
This takes place through the two-process model as suggested by Mowrer.
Study to support acquisition of phobias through classical conditioning
Watson and Rayner (1920)
Watson and Rayner (1920), Little Albert
Created a phobia in a 9 month old baby, Little Albert.
- Initially showed no unusual anxiety at the start; tried to play with the white rat.
- Each time the rat was present, the researchers made a loud frightening noise by banging metal close to Albert's ear.
The noise = unconditioned stimulus (UCS). Creates an unconditioned response (UCR) of fear.
When the rat (neutral stimulus, NS) and UCS were encountered together, the rat became a conditioned stimulus (CS) that produces a conditioned response (CR) of fear.
The conditioning was generalised to similar objects; fur coats and rabbits induced distress from Little Albert as well.
How is a phobia acquired according to the two-process model?
1. Classical conditioning; learning phobia through association. E.g. Watson and Rayner's study, Little Albert.
2. Operant conditioning; phobia is then maintained through negative reinforcement of avoidant behaviour.
A phobia is acquired through classical conditioning, then maintained by operant conditioning.
What are some strengths of the behavioural explanation?
1. Led to development of effective treatment - systematic desensitization
- Helps people unlearn their phobias
- Found to be effective at treating phobias
Adds to validity; positive impact on society
2. Scientific
- Focuses on behaviour that we can observe and measure, such as symptoms of a disorder.
- Observed through lab experiments
Adds to validity; establish a cause and effect relationship as the environment controls extraneous variables.
What are some weaknesses of the behavioural explanation for phobias?
1. Contradictory evidence
- Menzies and Clarke; only 2% of children who have a phobia of water have had a frightening experience with water in the past.
Questions the validity; we may not acquire and learn phobias through classical conditioning + association.
2. Reductionist
- Ignores other factors, e.g. hormones + imbalances of neurotransmitters
- Also doesn't completely explain symptoms of phobias because it focuses on outwards behaviour; Ignores cognitive symptoms.
Counterpoint: allows us to examine the area in great detail, likely to be scientific + empirically testable. Cause and effect relationship able to be established
However; questions validity, other important factors are not taken into account; model is too simplistic.
3. Diathesis stress model
- A better explanation of phobias takes into account both biological and environmental factors.
- Biology may predispose someone to phobias; environmental factors need to be present.
Questions the validity; behaviourist explanation = doesn't take biological factors into account.
What are the two types of treatment for phobias? How do they work?
1. Systematic desensitization; gradually introduces patient to the phobic content, replacing fear and anxiety with relaxation.
2. Flooding; exposing the patient to the phobic object without a gradual buildup.
What are the stages of systematic desensitization?
Stage 1:
- Patient and therapist work together to construct an anxiety hierarchy (list of things that produce fear for the client)
- At the bottom = most comfortable.
- At the top = most anxiety and fear
Stage 2:
- Relaxation training; client learns deep muscle relaxation, which is achieved through deee breathing.
Stage 3:
- Gradual exposure to the phobic object / situation
- Work from the bottom of the anxiety hierarchy upwards.
- Cannot move up the fear hierarchy until they are completely relaxed and no longer feel fear at the stimulus on the fear hierarchy.
What are some strengths of systematic desensitization?
1. Evidence to support
- Barlow et al. (2002) examined those with injections and spider phobias.
- Found that SD had a 60-90% success rate for these clients.
Adds to the effectiveness of SD. Shows that it does reduce the symptoms of anxiety.
2. Requires little effort
- Three simple steps, including just an anxiety hierarchy + learning relaxation techniques.
- Easy and not cognitively demanding; many people can complete including those w/ learning difficulties + young children.
Adds to appropriateness; more accessible, suitable for anyone.
3. Not as unethical as other treatments e.g. flooding
- Aim is to treat phobia through replacing anxiety with relaxation; less chance of psychological harm through stress caused by the treatment.
- Flooding causes psychological harm; involves full, immediate exposure to the phobic object.
What is a weakness of systematic desensitization?
1. Treats the symptoms, not the disorder
- Focuses on behaviour displayed in response to the phobic object
- Replaces anxiety w/ relaxation to reduce symptoms (e.g. panic, avoidance), but not the reasons behind the behaviour.
- Phobia may return later
Questions the effectiveness of SD; causes of phobia are not dealt with, and the phobia isn't treated in the long term.
What is flooding?
Exposing the patient to the phobic object without a gradual buildup. It involves immediate exposure to the phobia.
Sessions last longer than the ones in systematic desensitization; however only one session is involved in flooding.
What does it do for the patient?
- Shows the patient that the phobic object is harmless; their fear was wrong in the first place (shows the fear is irrational)
- Gets the patient calm and relaxed around the phobic object (they are no longer scared)
Classical conditioning term for when the client learns the phobic stimulus is harmless
Extinction
What is a strength of flooding as a treatment for phobias?
1. Cost-effective treatment
- Requires less time; only one session of immediate exposure
- Cheaper for the client; they only need to pay for one session
Adds to the appropriateness; phobias can be treated in less time; treatment is more accessible to more people
What are some weaknesses of flooding as a treatment for phobias?
1. Not effective for all phobias
- Works well for some phobias, e.g. arachnophobia.
- However may be more difficult to treat other phobias, e.g. social phobia because people have irrational thoughts, which flooding fails to treat.
Questions the effectiveness of flooding; cannot successfully treat all phobias
2. Traumatic
- It's not necessarily unethical, but needs fully informed consent. Even then, it can be very troubling for the client.
- Involves immediate full exposure to the phobic object; causes psychological harm.
- Some people may pass out or have anxiety due to them being exposed so quickly to their phobia.
- The traumatic nature of flooding also means that attrition rates are higher than for SD
Questions the appropriateness of flooding; though not unethical, it doesn't protect patients from psychological harm, therefore may be deemed inappropriate.
What is obsessive-compulsive disorder?
OCD: an anxiety disorder which involves obsessions and/or compulsive behaviour.
Other subtypes of OCD
Trichotillomania; compulsive hair pulling
Hoarding disorder; compulsive gathering of possessions and the inability to relinquish them regardless of value
Dermatillomania; compulsive skin picking
What is an 'obsession'?
Obsessions are cognitive internal intrusive thoughts.
For example, germs are everywhere and they could harm you.
What is a 'compulsion'?
Compulsions are behavioural external repetitive behaviours.
For example, you need to wash your hands every time you touch something to avoid germs / getting sick.
Emotional characteristics of OCD
(How you feel)
1. Anxiety/distress
- Unpleasant and frightening
2. Depression
- Often accompanies OCD; compulsions may reduce anxiety, but they're only short term fixes.
3. Guilt/disgust
- Either about the self, or external.
- Guilt is often irrational
Behavioural characteristics of OCD?
(What you do)
1. Repeated compulsions
- Repetitive and habitual
e.g. washing, counting
2. Anxiety-reducing compulsions.
- Done in response to e.g. obsessive fears
3. Avoidance
- May attempt to avoid anxiety by avoiding situations.
e.g. to avoid germs, they avoid bins.
Cognitive characteristics of OCD
(What you think)
1. Obsessive thoughts
- Recurring, unpleasant thoughts
2. Cognitive coping strategies
- Devise ways to cope with obsessive thoughts e.g. praying
- Frequency can interfere with everyday life
3. Awareness of excessive anxiety.
- Aware that their thoughts/behaviour are not rational.
- Hyper-vigilant, alert of potential hazards.
What is the biological approach to explaining OCD?
OCD is caused by a physical/bodily problem.
What are the two main biological explanations for OCD?
1. Genetic explanation
2. Neural explanation (neurotransmitters + brain structure)
What is the genetic explanation for OCD?
People may be genetically at risk of developing OCD. It may be inherited.
Monozygotic twins come from _____ zygote and share _____% of their genetics, making them identical twins.
Monozygotic twins come from one zygote (same egg) and share 100% of their genetics, making them identical twins.
Dizygotic twins come from ________ zygotes, and share _____% of their genes, making them non-identical twins.
Dizygotic twins come from two different zygotes, and share 50% of their genes, making them non-identical twins.
What did Carey and Gottesman (1981) find about the concordance rate between MZ twins and DZ twins for OCD?
MZ twins = concordance rate of 87%
DZ twins = concordance rate of 47%
What is meant by 'concordance rate'?
The probability that two individuals will have shared characteristics.
What do the findings of Carey and Gottesman (1981) tell us about OCD?
Genetics must play a role in OCD.
Those who are more genetically similar (MZ twins, share 100% of their genes) are more likely to share the same disorder than those who are less genetically similar (DZ twins, share 50% of their genetics).
This shows that the cause of OCD has a biological basis.
What are candidate genes?
Specific genes that create susceptibility or vulnerability to OCD.
What are the two candidate genes for OCD? What do they do?
1. SERT gene, responsible for serotonin transport:
- Mutation of the SERT gene creates lower levels of serotonin in the person, which is linked to causing OCD.
2. COMT gene, responsible for reducing/regulating the action of dopamine:
- Variation in the COMT gene decreases the amount of COMT.
- Therefore dopamine is not controlled; causes too much dopamine, associated with OCD.
SERT (low serotonin), COMT (high dopamine) = linked to OCD.
OCD is 'polygenic'. What does this mean?
OCD is not caused by one singular gene, but by a combination of genetic variations that together significantly increase vulnerability.
OCD is aetiologically heterogenous, meaning...
OCD can be caused by different combinations of genes
What are some strengths of the genetic explanation for OCD?
1. Evidence to support
- Billett (1998); MZ twins where one twin had OCD/genes for OCD were more than twice as likely to develop OCD than DZ twins.
Adds validity to the bio. approach to OCD; supports the idea that genetics play a role in OCD.
2. Animal studies
- Particular genes are associated with repetitive behaviours in other species e.g. mice.
Counterpoint: though mice and humans share most DNA, the human mind is more complex. Repetitive animal behaviour may not be able to be generalized to human OCD.
What is a weakness of the genetic explanation for OCD?
1. Relies heavily on nature side of nature v. nurture debate. No such thing as 100% concordance rate.
- OCD cannot completely be caused by genetics
- If it were, we would find concordance rates of 100%.
Questions the validity; there may be other factors e.g. environmental factors
What are the two neural explanations for OCD?
1. Neurotransmitters (serotonin)
2. Brain structure
What are neurotransmitters?
Chemicals that transmit electrical messages from one nerve cell in the brain to another, across the synaptic gap.
How does it explain OCD?
There are imbalances in these neurotransmitters.
In particular, OCD is linked to low levels of serotonin.
Outline the neural explanation for OCD (neurotransmitters)
Neurotransmitters are responsible for relaying information from one neuron to the other.
In OCD, there is a link to a reduction in the functioning of the serotonin system in the brain.
^ If someone has low levels of serotonin, they may be more susceptible to OCD.
Outline the neural explanation of OCD (brain structure).
Suggests that OCD is caused by issues with the structure of the brain.
Several areas of the frontal lobes = abnormal in people with OCD.
What two part of the brain in particular are linked to OCD?
1. OFC - Orbital Frontal Cortex.
2. Thalamus
There is overactivity in the OFC and thalamus in those with OCD.
What is the orbital frontal cortex's role?
It is linked to carrying out a compulsion due to an obsession; e.g. washing hands after touching meat.
What is the thalamus responsible for in OCD?
Carrying out safety behaviours e.g. cleaning and checking.
In OCD, what are the issues with the thalamus?
Thalamus = overactive.
If the thalamus is overactive, the OFC is also overactive.
Overactive thalamus = increased motivation to clean or check for safety.
In OCD, what are the issues with the orbital frontal cortex?
- The caudate nucleus is thought to be damaged, so it cannot suppress anxiety signals.
- Anxiety signals = become more frequent, increasing compulsive behaviour + anxiety
Overactive OFC = increased anxiety
What are some strengths of the neural explanation of OCD?
1. Evidence to support
- Research found mutations to the SERT gene, which causes low levels of serotonin, in people with OCD
Adds validity; evidence to support, adds accuracy to explanation
2. Scientific
- Empirical and scientific methods used to study biology of OCD patients.
- E.g. PET scans (positron emission tomography) + twin studies
- Effects of differences in brain structure + genetics can be identified
- Methods are rigorous, have control over extraneous variables.
Adds to internal validity; researched in a scientific manner = adds to accuracy, able to establish relationship between OCD and biology.
What are some weaknesses of the neural explanation for OCD?
1. Difficult to establish C+E relationship.
- Unclear whether OCD is caused by a physical difference; or if the difference occurs as a result of getting the disorder.
- E.g. those who have a difference in the structure of their brain may not have had these differences before developing OCD.
- OCD may have caused the difference itself because it causes high activity in the OFC.
Questions the validity; it may be that OCD causes these differences rather than the differences causing OCD.
2. Questionable compatibility with serotonin-increasing drugs.
- Neural explanation suggests low levels of serotonin = OCD.
- However, when patients with OCD take serotonin-increasing drugs, it does not work for everyone.
Questions the validity; evidence from patients suggests that low serotonin is not always the cause of OCD. Accuracy is lowered.
(If OCD arises from neural dysfunction like low levels of serotonin, we'd be able to treat it with drugs. But if it doesn't work for everyone, there must be different factors).
How is OCD treated biologically?
Drug therapy; altering the amount of neurotransmitters in the brain.
Outline drug therapy in relation to the neural explanation.
The neural explanation for OCD is that it is caused by low levels of serotonin.
Therefore, the treatment for OCD is drugs, which increase the level of serotonin.
Which drug is used in therapy for OCD?
SSRIs = Selective Serotonin Reuptake Inhibitor
- An antidepressant drug.
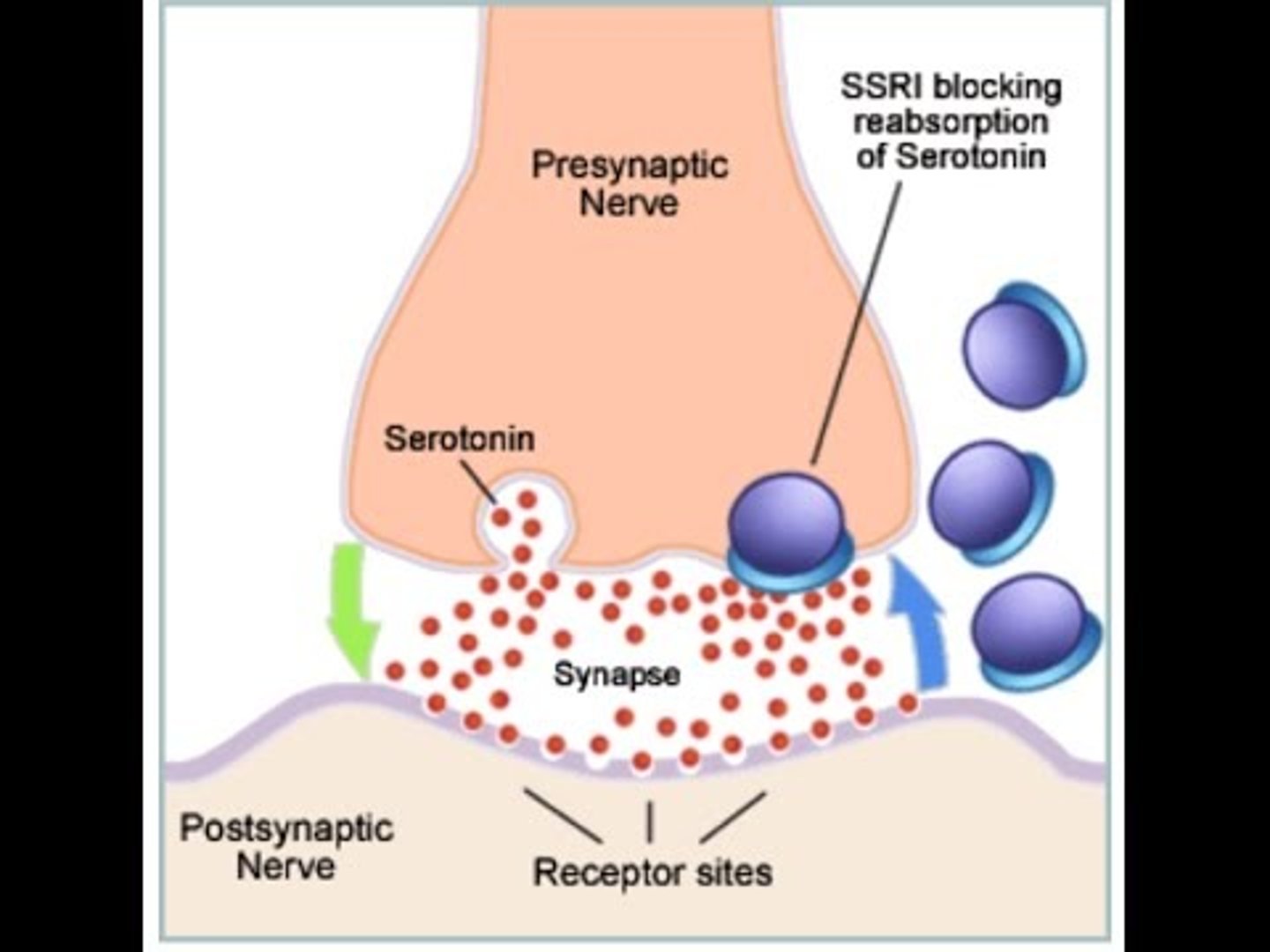
How do SSRIs treat OCD?
Increase the amount of serotonin by blocking the reuptake pump in the presynaptic neuron.
This allows more serotonin to attach to the receptors.
Example of SSRI
Prozac (fluoxetine)
SSRIs can be combined with...
Cognitive behaviour therapy
Alternatives to SSRIs for those who don't respond to them
Tricyclics
SNRIs -- increase both serotonin and noradrenaline
Evaluation of drug therapy for treating OCD
1. Quick + easy
- Swallowing a pill
- Not as difficult as other treatments e.g. CBT; requires you to reconstruct thoughts
Adds to the appropriateness of DT; not cognitively/physically demanding, more accessible. Increases likelihood of people engaging with DT = higher success rates.
2. Evidence to support effectiveness
- Soomro (2009); compared patients treated with SSRIs vs. a placebo for OCD
- Found the SSRI was more effective in treating OCD
Adds to the effectiveness; suggests there must be biological components to OCD.
3. Treats symptoms, not the disorder
- Drugs only increase levels of serotonin
- Without the drugs, symptoms (cognitive) would persist, causing more symptoms (emotional + behavioural).
Questions the effectiveness; doesn't treat OCD fully. When someone stops taking the medication, disorder returns, increasing relapse rates.
4. Not long-lasting
- Doesn't guarantee that a patient won't relapse.
- Patient can simply stop taking their drugs at any time; OCD resurfaces
Questions effectiveness/appropriateness; cannot be used as a sustainable treatment.
5. Side effects
- Though SSRIs help most people, some get no benefit and experience side effects e.g. indigestion and blurred vision.
- For those taking tricyclics, side effects are more common and can be very serious.
Means that some people have a reduced quality of life as a result of taking the drugs, dealing with OCD but posing a new problem (or even adding to the failure of not treating OCD).
What is depression?
A mood disorder
- Involves a disturbance of mood; mainly having a low mood
What are the two types of depression?
Major Depressive Disorder (MDD); unipolar, one single disorder of either mania or depression
Bipolar; both mania and depression - extreme highs and lows
Emotional characteristics of depression
- Lowered mood
- Anger
- Lowered self esteem
Behavioural characteristics of depression
- Lowered activity levels (reduced energy). Can also lead to the opposite effect, heightened activity levels (psychomotor agitation)
- Disruption to sleep/eating patterns (insomnia or hypersomnia)
- Aggression and self-harm (cutting, suicide attempts)
Cognitive characteristics of depression
- Poor concentration
- Dwelling on the negative
- Absolutist or black/white thinking; everything is good or everything is bad
What are the key assumptions of the cognitive approach to explaining depression?
The way they think about the problem causes the mental disorder rather than the problem itself.
- If people can think positively, they can be helped to feel better.
(Negative thoughts + irrational beliefs, + misinterpretation of events = cause of depression)
What are the two cognitive explanations for depression?
1. Beck's Negative Triad 1967
2. Ellis's ABC Model 1962
What did Beck believe was the cause of depression?
Negative thoughts:
- Faulty information processing
- Negative self-schema
- The negative triad.
childhood experiences eg continual parental criticism or rejection by other, leads to negative cognitive schemas developing
What is meant by 'faulty information processing'?
When people pay more attention to the negative aspects of a situation than the positive ones; black/white thinking.
What is meant by a 'negative self-schema'?
A mental framework of ideas about the self that is negative.
People with negative self-schemas interpret all information about themselves in a negative way.
What is the negative triad?
A dysfunctional view of themselves, the world, and the future.
- Negative view of the self; e.g. 'I am incompetent & undeserving'
- Negative view of the world; e.g. 'it is a hostile place'
- Negative view of the future; e.g. 'problems will not disappear, there will always be emotional pain'
What are some strengths of Beck's negative triad?
1. Evidence
- Research supports the proposal that depression = associated with faulty information processing, negative self-schemas, and the negative triad.
Adds validity; there is research to support
2. Practical application
- Beck's cognitive explanation forms basis of CBT.
- Therefore, all cognitive aspects of depression can be challenged in CBT.
Adds validity + real life application; able to be used in treatment for depression, betters society
What is a weakness of Beck's negative triad?
1. Does not explain all aspects of depression.
- Explains basic symptoms of depression
- However, it is a complex disorder with a range of symptoms, not all of which can be explained.
E.g. hallucinations and delusions, which likely require a different explanation.
Therefore, cognitive vulnerability (as Beck claims) is not a comprehensive explanation for depressive phenomena.
What did Ellis believe was the cause of depression?
Irrational thoughts.
He believed that good mental health is the result of rational thinking; thinking in ways that allow people to be happy and free from pain.
Outline how Ellis represented the way irrational thoughts caused depression.
The ABC model:
A = Activating event; e.g. failing an important test
B = Beliefs; e.g. belief that failing is a disaster. The idea that we must always succeed is 'musturbation'.
C = Consequences; emotional + behavioural consequences, e.g. depression
What is a strength of Ellis' ABC model?
1. Practical application
- CBT; irrational, negative beliefs are challenged.
- One form of CBT, rational emotive behaviour therapy (REBT) helps alter irrational beliefs of the client
- Helps to reduce depressive symptoms
Adds validity as it suggests that irrational beliefs had some role in depression + benefit to society; can better people's lives
What are some weaknesses of Ellis' ABC model?
1. Partial explanation
- Some depression does occur as a result of an activating event (reactive depression)
- However, not all depression arises as a result of an obvious cause (endogenous depression)
Lowers validity/applicability; we cannot identify a C+E relationship, concept of 'activating event' doesn't apply because it assumes there must be a cause.
2. Does not explain all aspects of depression
- E.g. does not explain why people experience anger associated with depression + why some patients suffer hallucinations & delusions.
However, the 'consequence' part of the ABC model may be open-ended enough to suggest that any symptom may arise from the activating event and belief.
What are some weaknesses of the cognitive explanation for depression?
1. Difficult to determine a cause
- Unclear whether depression = caused by irrational thoughts, or whether thoughts = caused by depression.
Questions validity; hard to establish C+E relationship between irrational + negative thoughts and depression.
2) also be explained biologically, in terms of neurotransmitters and genetic factors. studies found low levels of serotonin in depressed people and show that drug therapies which raise serotonin levels are successful in the treatment of depression
means neurotransmitters also play a role in causing depression
What is a strength of the cognitive explanation of depression?
1. Led to development of effective therapy
- CBT = second highest success rate among 10 different therapies for depression
Adds to validity; has a real life practical application, leads to positive impact on society.
if depression is alleviated by challenging irrational thinking then this suggests such thoughts had a role in depression in the first place
What is cognitive behavioural therapy?
A method for treating mental disorders. which works by changing irrational + negative thoughts to more rational + positive ones.
What is meant by the 'cognitive element'?
An assessment in which the client and therapist work together to clarify the client's irrational/negative thoughts.