Optimising medicines management in women's health
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
What is the role of oestrogen in the body?
Physical changes associated with puberty in women
Regulating the menstrual cycle
Various roles in a healthy pregnancy
In women and men oestrogen helps control
Sexual desire
Erectile function
Lipid metabolism
Brain function
Bone health
Skin health
What is the role of testosterone in women?
Essential for development and maintenance of female sexual anatomy and physiology, and modulation of sexual behaviour
Best known for influencing libdo, but…
Also plays a substantial role in a number of physiological processes in the brain
Helps with muscle mass and bone strength, cardiovascular health, and overall energy levels and quality of sleep
It strengthens nerves in the brain, and contributes to mental sharpness and clarity. It strengthens arteries that supply blood flow to the brain, which protects against loss of memory. It regulates serotonin levels and plays a role in its uptake in your brain, which helps improve overall mood. Testosterone also stimulates the release of dopamine, another neurotransmitter responsible for your feelings of pleasure.
WHAT IS MENOPAUSE?
Definition: Menopause is defined as the permanent cessation of menstruation resulting from the loss of ovarian follicular activity. This is typically diagnosed after 12 consecutive months without a menstrual period. Usually occurs between the ages of 45 and 55
Average Age: The average age of menopause in the UK is around 51 years
WHAT IS PERI-MENOPAUSE?
Definition: The peri-menopause is the transitional phase leading up to menopause, characterised by irregular menstrual cycles and symptoms due to fluctuating hormone levels.
Duration: Peri-menopause can begin several years before menopause and last until one year after the final menstrual period. The average number of years a woman is in peri-menopause varies but on average is 4 years
Not all women will experience menopausal symptoms when they go through the menopause, up to 80-90% will have some symptoms, with 25% describing them as severe and debilitating
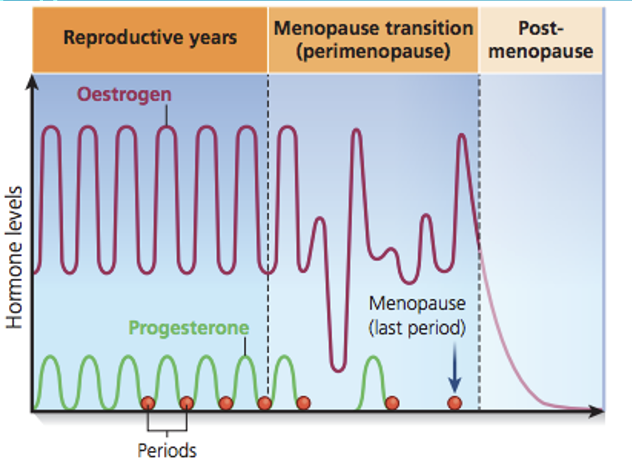
Describe the pathophysiology of the hormonal changes in perimenopause and menopause.
Oestrogen: Most produced by ovaries pre-menopause. Levels fluctuate and eventually decline
Progesterone: Levels decrease with the reduction of ovulation
Testosterone: 25% produced in ovaries. Levels decline through menopause and stay low thereafter
FSH: Levels increase due to loss of feedback mechanisms to the pituitary gland
What are the Vasomotor Symptoms (70-80% women) of menopause?
Hot Flushes: Sudden feeling of heat, often accompanied by sweating and palpitations
Night Sweats: Excessive sweating during the night
What are the Menstrual Irregularities of menopause?
Irregular Periods: Variations in cycle length, flow, and duration
Amenorrhoea: Complete cessation of periods
What are the Psychological Symptoms of menopause?
Mood Changes: Depression, anxiety, irritability
Cognitive Changes: Memory lapses, difficulty concentrating
What are the Urogenital Symptoms of menopause?
Vaginal Dryness: Due to oestrogen deficiency
Dyspareunia: Painful intercourse
Urinary Symptoms: Increased frequency, urgency, and risk of UTIs
What are the other symptoms of menopause?
Sleep Disturbances: Insomnia or disrupted sleep
Joint and Muscle Pain: Generalised aches
Weight Gain: Particularly around the abdomen
Skin Changes: Thinning, dryness, loss of elasticity
What is the diagnostic criteria for menopause?
Menopause in women who have:
Not had a period (amenorrhoea) for at least 12 months and are not using hormonal contraception. Often diagnosed retrospectively
Or, symptoms in women without a uterus
Can be made without laboratory tests in otherwise healthy women aged over 45 years with appropriate symptoms
Perimenopause based on vasomotor symptoms and irregular periods; lab tests are not always necessary but can be used to rule out other conditions
What are the differential diagnosis to menopause?
Exclude other causes of symptoms such as thyroid disorders, depression, or pregnancy
Premature Ovarian Insufficiency (POI) (if aged <40) and early menopause (if aged <45) need to be considered
Women with POI and early menopause are at an increased risk of both osteoporosis and CV disease – benefits of HRT may be greater in this cohort
Consider using an FSH test to diagnose menopause only for…
In women aged 40 to 45 years with possible menopausal symptoms, including a change in their menstrual cycle
In women aged under 40 years in whom menopause is suspected
If on contraception and period history is not reliable then can use FSH to see if contraception needed
What are the laboratory investigations that can help to diagnose menopause?
FSH Levels: Elevated Follicle Stimulating Hormone (FSH) levels (>30 mIU/mL) may indicate menopause, but these levels can fluctuate during peri-menopause
If FSH high, then need contraception for a further 2 years (over 12 months if aged >50)
Oestrogen Levels: Low levels may be observed but are not routinely measured for diagnosis
What are the treatment options for menopause?
Consideration should be given to the patient’s full medical history, including personal, family and drug history and basic parameters e.g.height, weight, BMI and BP
Ask women to track and record their symptoms over a period of time
Provide advice on lifestyle modifications to reduce menopausal symptoms
Only after the above should HRT be considered in the context of a supportive consultation
SSRIs, SNRIs or clonidine should not routinely be offered as first-line treatment for vasomotor symptoms alone
Treatment should be adapted as needed, based on changing symptoms
What are the NON-PHARMACOLOGICAL treatment options for menopause?
Healthy diet, including a diet that is low in saturated fat and salt and rich in calcium and vitamin D to strengthen bones
Regular exercise, as this helps to relieve stress and lowers the risk of heart disease
Stopping smoking, as smoking has been shown to increase the risk of an earlier menopause and trigger hot flushes. If women smoke they also run a higher risk of developing osteoporosis and heart disease
Drinking moderately, as alcohol increases hot flushes and is associated with an increased risk of breast cancer. Women should try not to drink more than 2 to 3 units of alcohol per day, and keep at least 1-3 days a week alcohol-free
Relaxation techniques such as meditation and yoga
Cognitive Behavioural Therapy (CBT) is also an effective option in improving hot flushes, nights sweats and other menopausal symptoms and can be considered in women who do not wish to take HRT or are unable to take HRT
What are the PHARMACOLOGICAL treatment options for menopause?
Hormone Replacement Therapy (HRT)
Oestrogen-only Therapy: Effective for vasomotor symptoms and urogenital atrophy (only ever used as monotherapy in patients without a uterus)
Combined HRT: Oestrogen + Progestogen for women with an intact uterus to prevent endometrial hyperplasia
Routes of Administration: Oral, transdermal, vaginal
Risk put into perspective for transdermal V oral
How should HRT be taken?
Oestrogen available as patches, gels, sprays and oral tablets
Progesterone available through the ‘Mirena’ IUD (synthetic progesterone but low dose), oral tablets and combined patches (although combined patches include synthetic progesterone)
Non-oral route for oestrogen prefered, especially if >60 years old and/or VTE risk factors e.g. FHx VTE or BMI >30
Different formulations will suit different people – always consider changing formulation before increasing dose
→ Separate Rxing of oestrogen and progesterone sensible as you can then alter the dose of oestrogen independently
→ Generally start at lower doses, review at 3M and alter doses accordingly. Younger women may require a higher dose than older women
→ Mirena changed every 5 years for HRT
Compare SEQUENTIAL and CONTINUOUS HRT.
Use Sequential HRT for Pre-menopausal Women still having periods
In Sequential, oestrogen taken everyday a month and progesterone for half a month only – this is to avoid bleeding → Micronised progesterone 200 milligrams daily for 2 weeks
Sequential HRT causes a monthly bleed
Use Sequential for 6-12 months, then consider Continuous – no further periods
In Continuous, use micronised progesterone 100mg at night
Can give progesterone vaginally (off-licence) – half oral doses
If period-free for >12 months can go straight onto Continuous regimens
When and why might a patient need progesterone alongside oestrogen for HRT?
If a woman has an intact womb then they MUST have progesterone alongside their oestrogen HRT
Dose needed depends on dose of oestrogen. As oestrogendose increases, progesterone dose must also increase alongside
Significantly reduces risk of endometrial cancer by protecting womb from affects of oestrogen
Synthetic or body identical progesterone available
Body identical (micronised) – neutral affect on VTE risk and slightly lower breast cancer risk
Compare the TRANSDERMAL VERSUS ORAL ROUTE for progesterone therapy.
Gels, patches and sprays do not affect the risk of blood clotting or stroke at standard doses
Safer option if patient at higher risk of blood clots or stroke (e.g. smoker, obese BMI, or a migraine sufferer)
Note progesterone in a patch is usually synthetic, not body identical
Micronised progesterone (Utrogestran – a capsule) is body identical and likely to have a lower risk of breast cancer compared with alternatives. Unlike synthetic progestogens, it should not affect the risk of heart disease or blood clotting
What are the potential rise effects of HRT?
Oestrogenic side effects: Breast tenderness, breast enlargement, bloating, nausea, headache/migraine and leg cramps
Progestogenic side effects: Sedation (take at night), fluid retention, headaches, breast tenderness, lower abdomen pain, backache, depression, mood swings, acne/greasy skin and headache
When can unscheduled bleeding occur for HRT patients? Why does it occur and how can the risk be reduced?
Occurs in up to 40% of women on HRT
Very common in first 6 months of any HRT use or 3 months post change in HRT
Often needs further investigation outside these parameters
Increase in HRT use has led to an increase in consultations with women experiencing unscheduled bleeding → urgent gynecological referrals for suspected endometrial cancer increased by 43% between 2021 and 2024 (but no increase in endometrial cancer diagnoses)
HRT optimisation can reduce risk of unscheduled bleeding e.g.considering an IUS-Mirena, reduce oestrogen dose, switch to a different progesterone, switch to a different formulation (oral associated with increased bleeding risk) and consider vaginal oestrogen for GUS
Discuss the benefits and risks of HRT for Endometrial cancer.
Major risk factors: BMI >40, genetic risk, unopposed oestrogen for >6/12, >5 years sequential HRT use in women >45 years, inadequate progesterone dose alongside oestrogen HRT for >12 M
Minor risk factors: BMI 30-39, diabetes, unopposed oestrogen for 3-6M, inadequate progesterone dose alongside oestrogen HRT for >12M
Baseline age-related incidence in newly menopausal women 0.7% if aged 50-54; 1.2% if aged 55-59
Sequential regimens associated with an increased risk if used for >5 years
Continuous combined regimens have a reduced risk compared with baseline
Discuss the benefits and risks of HRT for Breast cancer.
NICE states that:
Any increase in the risk of breast cancer is related to treatment duration and reduces after stopping HRT
HRT with oestrogen alone is associated with little or no change in the risk of breast cancer
HRT with oestrogen and progestogen can be associated with an increase in the risk of breast cancer
Most women die in the UK from dementia and CV disease, not breast cancer
HRT can be protective from CV disease, diabetes, OP (and fragility fractures – 1/3 of women will die within 12 months of FF) and possibly dementia
Does HRT have any cardiovascular risks?
If less than 10 years since LMP, then benefits are likely to outweigh risks
Stopping and restarting HRT is less safe than staying on it
If arterial or venous risk factors including hypertension use non orals, if no problems in the past and no risk factors oral may be reasonable (HRT does not raise BP)
NICE (NG23) states that HRT:
does not increase cardiovascular risk when started in women aged under 60 years
does not affect the risk of dying from cardiovascular disease
HRT with progestogen is associated with little or no increase in the risk of coronary heart disease
HRT does not increase cardiovascular disease risk when started in women aged under 60 years
HRT does not affect the risk of dying from cardiovascular disease
HRT with oestrogen alone is associated with no, or reduced, risk of coronary heart disease
HRT with oestrogen and progestogen is associated with little or no increase in the risk of coronary heart disease
HRT generally very safe for women <60 and within 10 years of their menopause
Does HRT increase the risk of Venous Thromboembolim (VTE)?
If BMI > 30kg/m2 consider swapping to oestradiolpatch/gel, ensure not on high dose norethisterone, this is because: NICE (NG23) states that:
The risk of VTE associated with the use of HRT is greater for oral than transdermal preparations
The risk of VTE associated with transdermal HRT given at a standard therapeutic dose is no greater than baseline population risk
The risk of stroke is slightly higher for women taking oral (but not transdermal) HRT
What are the CONTRAINDICATIONS TO HRT?
Known or suspected oestrogen-dependent cancer
Undiagnosed vaginal bleeding
Untreated endometrial hyperplasia
VTE or history of recurrent VTE, unless the woman is already on anticoagulant treatment
Active or recent arterial thromboembolic disease
Thrombophillic disorder or thrombophlebitis
Untreated or unstable hypertension
Active liver disease with abnormal liver function tests
Acute Porphyria
Pregnancy
Dubin-Johnson and Rotor syndromes (monitor closely)
Previous Hx of Breast Ca not necessarily a complete CI – would get specialist advice
Hypertension not a CI
What are the benefits to HRT?
Reduction in risk of heart disease and CV mortality*
Reduced risk of Fragility Fractures
Maintaining muscle strength
Relief of perimenopause and menopause symptoms
Improved QOL
* If started before the age of 60 years or within 10 years of the menopause
What are the IMPORTANT COUNSELLING POINTS for HRT?
Explain to women with a uterus that unscheduled vaginal bleeding is a common adverse effect of HRT within the first 3-6 months of treatment; women should report this promptly
Advise women of the usual bleeding pattern to expect with their HRT; After 6 months, patients on sequential HRT should expect a light bleed at the end of the progesterone phase and if on continuous HRT patients should expect to be amenorrhoeic
Reinforce the importance of adherence with therapy – allow 3-6 months after initiation or change to review efficacy
Remind women in the peri-menopause or with premenstrual ovarian insufficiency that that HRT is not a contraceptive and contraceptive precautions are still necessary
Discuss with women the importance of keeping up to date with nationally recommended health screening
What are important things to consider and check with HRT regularly?
Symptoms not controlled: Increase dose (within licensed dose range) or change formulation (after persistence with treatment for at least 3 months)
Poor patch adhesion or irritation at patch site: Try alternative brand or route
Drug interactions: Enzyme inducers lower the circulating levels of hormone e.g. barbiturates, phenytoin, carbamazepine. Change to non-oral route. Intra-Uterine Systems are not affected
Reiterate lifestyle advice at every review opportunity
What are some of the NON-HORMONAL TREATMENTS for menopause?
SSRIs/SNRIs: For mood symptoms and hot flushes (e.g., venlafaxine, fluoxetine).
Clonidine: An alpha-agonist that can reduce hot flushes.
Gabapentin: Can be effective for vasomotor symptoms.
Vaginal Moisturizers and Lubricants: For urogenital symptoms.
Should TESTOSTERONE be used for the treatment of menopause?
NICE Menopause Guideline (NG23) and the BMS recommend that a trial of conventional HRT is given before testosterone supplementation is considered
Should only be considered in post-menopausal women who complain of low sexual desire (Hypoactive Sexual Desire Disorder; HSDD) after a biopsychosocial approach has excluded other causes
Randomised clinical trials of testosterone to date have not demonstrated the beneficial effects of testosterone therapy for cognition, mood, energy and musculoskeletal health therefore primary indication should be for HSDD
Likely that testosterone does have benefit on improving mood and energy levels
No evidence in pre-menopausal women
Potential SE’s : Excess hair growth, acne and weight gain which are usually reversible with reduction in dosage or discontinuation. Alopecia, deepening of voice and clitoral enlargement are rare with physiological testosterone replacement
Currently, no licensed product available in the UK
How can you treat GENITOURINARY SYNDROME OF MENOPAUSE (GSM)?
Topical oestrogens - NOT HRT
Local application to the vagina via vaginal ring, pessary or cream
Little to no systemic absorption
No need for endometrial protection with progesterone
Vaginal oestrogen reduces UTI by 50-60%
Can give local oestrogen to older women, even if you don’t want to give HRT – far less risk and work very well. Cheap and safe
Regular use (over 12 months) of Vagifem 10 micrograms is less than taking just one ‘1mg’ oestrogen tablet.
How can you provide contraception alongside HRT?
Women < 50 years of age – considered potentially fertile up to 2 years after her last menstrual period
Women >50 years of age - considered potentially fertile up to 1 years after her last menstrual period
In general, all women can cease contraception at age 55 as spontaneous conception after this age is exceptionally rare (FSRH)
If Mirena not an option, then combined pill (which contains oestrogen may work well for younger women – up to age 50 in absence of other risk factors)
If higher risk associated with CHC use, then consider Depo-Provera (stop at 50), implant, POP, Cu-coil – all can be used alongside HRT
The Mirena® IUD has now been licensed for 8 years for contraception if you are under 45
If using the Mirena as part of HRT only then it can now be used for up to 5 years before it needs removing or replacing.
Contraceptive method will depend on individual patient factors including age, co-morbidities, BMI etc. A discussion on this is beyond the scope of this lecture
When should you follow-up and review HRT?
At initiation of HRT or change in therapy - three months follow-up
Established on HRT – at least annual review
Review/ follow-up should:
Assess effectiveness and side effects of therapy; discuss any bleeding patterns; review type and dose of HRT; assess on-going risk/benefit balance; ensure patient attending National cervical and breast screening when invited, advise self-checking breasts and encourage healthy lifestyle
When should progesterone be taken?
progesterone take at night as help with sleep matches sequential cycle
main side effect makes you sleepy
also hair greasy mood disturbances
When should HRT be stopped?
Risks slightly higher, although no increased mortality >60
Natural risk of breast cancer and CV disease does increase with age
Does not need to have an abrupt end to treatment
Always consider their QoL
Shared decision making with each patient
Document decision made with patient
synthetic hormone give slightly increased risk of
clotting and breast cancer
When do you use continuous or sequential HRT?
continuous haven’t had period in 12 months
sequential if still period then after 6-9 months swicthc to continous
What is the general idea of HRT?
HRT idea ids replacing oestrogen being lost to manage symptoms of menopause
can only give oestrogen only therapy to women without uterus as women with uterus oestrogen only therapy the womb with thicken and putting women at risk of endometrial cancer