Cardiac Catheterization
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
4 types of info rendered from cardiac catheterization:
Cardiovascular pressure readings
Blood flow determination
Angiography
visualization of cardiac / vascular structures
Electrophysiological studies
Cardiac Cath Personnel
There will be many people in the Cath lab during a procedure
some will be sterile while others will not
when you are in the lab, be prepared to wear a lead shield / apron
must work as a team!
Cardiac Cath Physician
Well trained Cardiologist
Cardiac Cath Nurses
Prepare and monitor the pt
give med’s
prepare instruments / catheters
Cardiac Cath X-ray tech
special procedures
fluoroscopy
Hemodynamic assessment:
Rt heart Cath
access vein (Femoral, Brachial, Subclavian)
pass cath through IVC into the RA and RV
When doing a rt heart cath, (1) do pressure measurements of:
RA
RVSP
RVEDP
mean PA
SPAP
PAEDP
Pulmonary-Capillary Wedge
What precent of the left heart pressure is the right heart?
The rt heart pressure is 20% of the lt heart
When doing a rt heart cath, you take blood samples to check the oxygen saturation of:
SVC
IVC
RA
RV
MPA
Left Heart Cath
more difficult b/c assessing A instead of V
pass catheter through Aorta into the LV
When doing a lt heart cath, you take pressure measurements of:
LVSP
LVEDP
mean Ao
systolic Ao
diastolic Ao
NO LA pressure taken
With a lt heart cath, the ventriculography / LV angiography will evaluate:
assess LV function
severity of MR
shunt flow
aka: VSD / ASK
hole or communication between right and left heart
During a lt heart cath, a Coronary Arteriography / Angiography is placed:
pass catheter through Aorta into the ostium of the CA’s
at the sinus of valsalva
During a lt heart cath, an aortic root angiography is the assessment of:
Aortic aneurysms / dissection
AI
AS
Electrophysiological studies
testing of Cardiac Pacing
Tx of arrhythmias
Interventional / Special Techniques
PTCA
myocardial biopsy
balloon balvuloplasty
catheter ablation
irritable foci and accessory pathways are terminated
Electrophysical studies
testing of Cardiac Pacing
Tx of arrhythmias
Examples of Interventional / Special Techniques:
PTCA
percutaneous transluminal coronary angioplasty
myocardial biopsy
balloon valvuloplasty
catheter ablation
irritable foci and accessory pathways are terminated
Indications for a cardiac catheter:
CAD
MI
Valvular heart disease
Congenital heart disease
Ao disease / dissection
Pulmonary angiography
Cardiomyopathy
Pericardial constriction / fluid
Pre- and s/p Cardiac transplant
Coronary Artery Disease (CAD)
atherosclerotic plaque blockage of the CA’s leading to insufficient blood flow to the myocardium
Symptoms of CAD:
angina (chest pain)
silent ischemia
CHF
positive stress test (EKG or Echo)
Contra-indications for a cardiac catheter:
fever / infection
anemia
hemorrhage
hypercoaguable state
shock
hypoxia
uncooperative pt
dementia
Contra-indications for a cardiac catheter:
pregnancy
no X-ray
renal failure
can’t rid of contrast
technical reasons
failed vascular access
calcified vessel
Cardiac Cath Pt Prep:
explain procedure
should be MD’s responsibility
Pre-Admission Testing
12 lead EKG
Labs:
creatinine
BUN
prothrombin time
Cardiac Cath Pt Prep:
Obtain informed consent
pt understands the risks and benefits of the procedure
AKA to medications
Pt fasting from midnight prior
before pt comes to lab:
IV access
remove dentures / eyeglasses
shave groin area
Cardiac Cath Pt Prep:
Pre-Cath sedation
valium or demoral
if very anxious about the procedure
Lab set up
check crash cart supplies
run cinefilm
check current pt ID
sterile trays / equipment
needle
guide wire
catheter
med’s
Cardiac Cath Pt Prep:
Attach EKG electrodes
Explain procedures such as:
Clean and drape entrance site
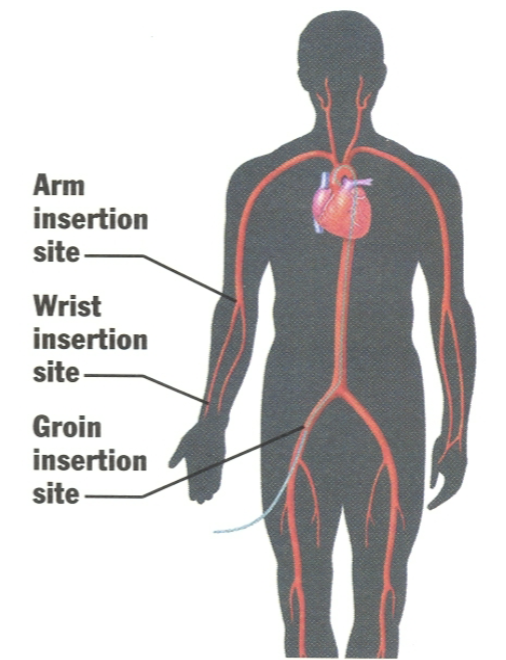
Entrance sites of cardiac catheter insertions:
Femoral
Subclavian
Brachial (more vasc complications associated)
Radial → becoming more and more popular
Arm, Wrist, and/or Groin
Procedure and Protocol:
monitor pt
check pt’s vital signs
maintain records
puncture sites
types and gauge of catheter
pressure recordings
time/dosage of med’s
Procedure and Protocol:
Pt supine
radiolucent, padded operating tavle
X-ray equipment
sterile technique
surgical scrub
scrub suits, gloves, mask, booties
radiation precautions
lead apron
do not go in if pregnant
radiation badges
Insertion steps:
clean and drape access site
inject local anesthetic
needle inserted to puncture site
guide wire fed through needle
used to avoid vessel damage
done w/ fluoroscopy to observe progress
real time x-ray
little sensation to pt
remove needle and apply pressure
vessel dilator inserted and removed
insert catheter over guide wire
remove guide wire
Following the cath procedure:
monitor pt’s clinical S&S’s
pt placed in holding area for a few hours
apply pressure to entrance site
10-15 minutes
pt should not bend affected extremity
4-6 hrs
enter all procedure notes on pt chart
Cardiac Cath Complications:
there are risks involved
morality rate: 3-4 / 1000 pts
always be performed by well trained physician / staff
up-to-date equipment
risks need to be weighed against possible procedure benefits
Possible complications:
Death
MI
Arrhythmia
Vascular injury
pseudoaneurysm, AV fistula
Cardiac perforation
may cause Cardiac Tamponade
severe pericardial effusiion
Septal defects
ASK or VSD
Allergic reaction to contrast media
Hemodynamic Data
By using a fluid filled catheter, it is possible to determine pressures at almost any circulation site
remember: fluid flows from a high to low pressure area
RA pressure AKA:
Central Venous pressure
RA pressure
represents the filling pressure of the RV
2-7 (0-5) mmHg
What is RA pressure normally equal to?
RVEDP
What causes elevated Central Venous pressure?
increased RVEDP
TS (Tricuspid Stenosis)
causes outflow obsruction from RA to RV
RV End Diastolic pressure (RVEDP)
2-6 mmHg
increased RVEDP causes:
increased RA pressure
RV Systolic pressure (RVSP)
25 mmHg
RVSP increases w/ pressure overload
RVSP pressure overload is caused by:
Increased right-sided outflow resistance d/t:
Pulmonary stenosis (PS)
PHTN
SPAP
25 mmHg
DPAP
10-12 mmHg
Mean PAP
16 mmHg
There is an increase in Pulmonary Artery pressure (PAP) with:
Pulmonary vascular obstruction
COPD
pulmonary embolism
increased Pulmonary Capillary pressure
PHTN
Lt heart disease
Pulmonary Capillary pressure (PCP) AKA:
Pulmonary Capillary “wedge pressure” (PCWP) → b/c cath is wedged (via balloon on cath tip) into PA
Pulmonary Capillary pressure (PCP)
mean pressure - 10-12 mmHg
in pt’s with normal pulmonary symptoms:
PCP will approximate LA pressure
we cannot get a direct measure of the LA
Elevated pulmonary capillary pressure is a result of:
Mitral Stenosis
LA pressure
represents the filling pressure of the LV
mean - 10-12 mmHg
Elevated LA pressure is due to:
MS
Increased LVEDP
As LA pressure increases:
So does PCP
PAP next
then RVSP
then RA pressure
LV end-diastolic pressure (LVEDP)
10-12 mmHg
What causes LVEDP to increase?
dyastolic dysfunction
“relaxation” problems due to:
CAD & ischemia w/ resultant scarring
CHF
toxic (alcohol) damage (DCM)
constrictive pericarditis
MV and AoV insufficiency
What results from increased LVEDP?
Increased LA pressure
therefore PCP, PAP, etc.
LV Systolic pressure (LVSP)
120 mmHg
without AoV abnormalities:
LVSP will equal systolic BP
found w/ brachial BP cuff
Elevated LVSP is due to:
systemic HTN
most common cause
Atrial Stenosis (AS)
Systolic Aortic pressure (SAP)
120 mmHg
Diastolic Aortic Pressure (DAP)
80 mmHg
Mean Aortic Pressure (AP)
92 mmHg
Pressure Gradient
difference in pressure between two chambers
necessary for blood flow
What is the most accurate means of evaluating valvular function?
Pressure gradients across a valve
3 ways Cath measures pressure gradients:
Peak to Peak PG
always slightly lower than peak instantaneous
Peak instantaneous PG
always slightly higher than peak to peak
Mean PG
Peak to Peak PG
represents difference between peak systolic pressures at two different locations, regardless of where they occur in the cardiac cycle
example: compare LVSP to Ao systolic pressure ( or RVSP to SPAP) to determine severity of semilunar valve stenosis
reported from the Cath Lab only
Peak instantaneous PG (Max PG)
represents pressures at two different locations at the same time during the cardiac cycle
can be reported from the Echo Lab too
trace the spectral waveform obtained across a valve
True or False. Measurements reported in both Cath and Echo should be closely correlated.
True
Cardiac Output (CO)
the volume of blood ejected by the heart per minute
gives information about the amount of blood in circulation
Normal resting CO:
4-8 L/min
CO=
SV x HR
Stroke Volume (SV)
the difference between end diastole and end systole volume per beat
volume of blood ejected from the heart w/ each contraction
Heart Rate
Number of ventricular contractions per minute
Cardiac Index
CO is used to find the CI
CO expressed in relation to the pt’s body surface area (BSA)
CO / square meters of BSA
Normal cardiac index:
2.76 - 3.6 L/min/m2
3 methods to determine CO in the Cath Lab:
All are based on the Fick Principle
Fick Method
Indicator Dilution Technique
Thermodilution Technique
Fick Principle
In a closed steady-state system (heart and vessels), the amount of Indicator flowing into the system equals the amount of Indicator flowing out of the system
Fick Method
Oxygen is used as the Indicator
requires 3 pieces of data:
oxygen consumption
amt of O2 taken up by the body
determined by having the pt breath into a mask to collect the expired air
oxygen content of arterial blood
oxygen content of venous blood
O2 consumption / A-V content
Indicator Dilution Technique
Indocyanine Green dye
dye is injected into the right heart and the concentration of the dye is them measured on the arterial side w/ a Densitometer
Rarely used
What was the Indicator Dilution Technique replaced with?
Thermodilution Technique
Thermodilution Technique
utilizes a decrease in blood temp as the thermal Indicator
chilled saline is injected into the right heart and the difference is measured on the arterial side w/ a thermistor
O2 Sats
Amount of oxygen contained in blood
Right Heart O2 Sats:
= 75%
IVC
RA
RV
MPA
Left Heart O2 Sats:
= 95%
LA
LV
Ao
Oxygen Step-up
Cath Lab will check for this
a “step-up” in the right heart will indicate a shunt from the left heart increased the amount of O2 present
Angiography
Contrast media is injected into the blood
causes the blood to appear as a radiopaque area under fluorosopy
a silhouette of the chamber or vessel containing the media will be seen
will aid in the assessment of:
chamber / vessel size
stenosis
contraction
Selective Angiography
dye injection is done only near the area from which the info is desired
not circulated through the entire system
used generally for 4 areas
will help identify or R/o pathology in the specific area
Types of angiography:
Coronary angiography
stenosis / occlusion of CA’s and branches
Left Ventriculography
wall motion, EF, MR, VSD
Pulmonary Angiography
pulm embolism
Aortography
dissection, aneurysm, rupture, etc
Balloon Angioplasty
may be utilized in:
PAD
CAD
alternative to CABG
the heart is like the extremities in the presence of stenosis
blood flow will not be able to increase enough w/ stress (exercise) to supply the muscle (myocardium)
results in constructive pericardium (CP)
What is the re-stenosis rate balloon angioplasty?
25-35%
Balloon Valvuloplasty
same principle as balloon angioplasty
used to open up stenotic valves
balloon tipped cath is inserted across the affected valve
balloon inflated to stretch the valve orifice
Coronary Stents
a metalic coil is mounted on the balloon tipped catheter
when the balloon is inflated, the coil expands
the balloon catheter is then withdrawn
the coil stays in place to maintain vessel patency
Coronary Laser Angiography
uses a fiber-optic catheter to destroy plaque formations
difficult to only vaporize plaque and not vessel wall
Rotoblater (roto-rooter)
Uses rotating drill type catheter to break plaque into microscopic pieces
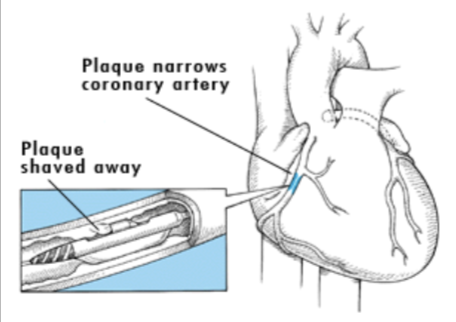
Atherectomy Catheter
the catheter tip contains a tube-like structure w/ a window in it
the tube rotates to cut or shave off the plaque
the plaque is collected in the tube
Endomyocardial Biopsy
removal of heart tissue for diagnostic purposes
will be performed to:
assess possible rejection following transplant
diagnose myocardial disorders
Hypertrophic cardiomyopathy (HCM)
myocarditis
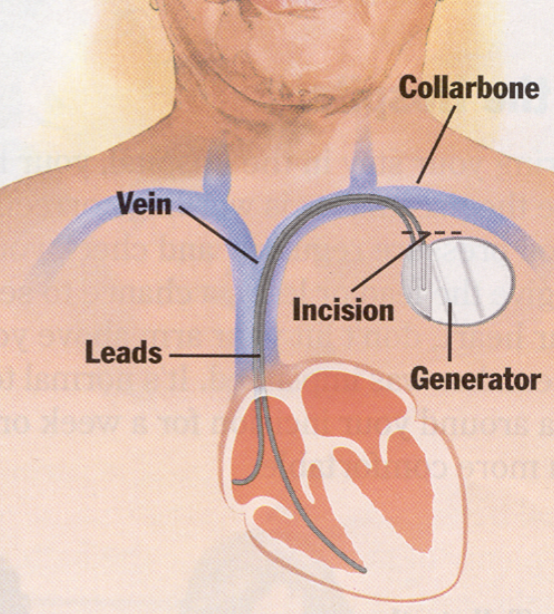
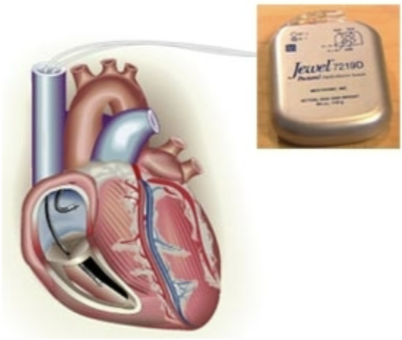
Implantable Cardioverter-Defibrillator (ICD)
act as a pacemaker, defibrillator, and cardioverter
detect and prevent sudden cardiac arrest
device works by detecting a dangerous rapid heart beat and then delivering a shock to help restore a normal rhythm
no more discomfort than being kicked in the chest
Where is the generator of the ICD placed in the chest?
Below the collarbone and the leads are placed in