Looks like no one added any tags here yet for you.
What neurotransmitters are in play in the adrenergic nervous system
epinephrine or norepinephrine
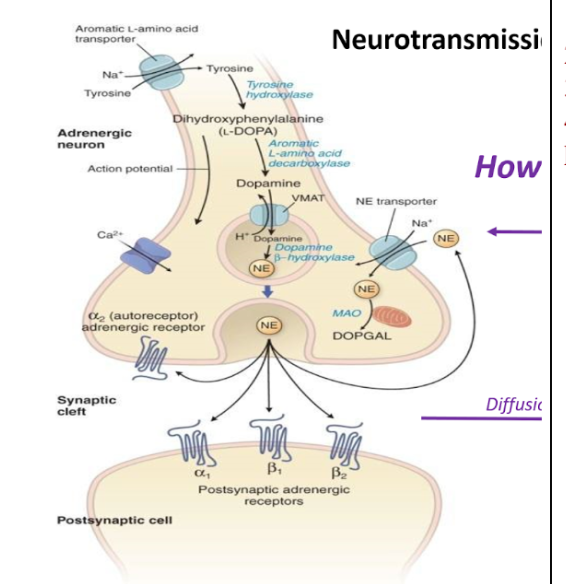
Neurotransmission events at adrenergic receptor
1)Tyrosine is actively transported in to the neuron
2)Tyrosine is converted into L Dopa via tyrosine hydroxylase
3)L Dopa is converted into Dopamine via Aromatic L amino acid decarboxylase
4)Dopamine turns into NE via dopamine B hydroxylase in the storage vesicle
Calcium influx triggers release of NE from storage vesicles
What receptors are present in the synapase?
alpha1, alpha2, beta1, beta2
Where are alpha1, alpha2, beta1, beta2 receptors located in the synapse?
Alpha 2- Adrenergic neuron (autoreceptor)
Alpha1, B1, B2- Postsynaptic cell
what mechanisms are important to removing norepinephrine/epinephrine from the synapse?
Ne can get reuptaken into the neuron via a NE transporter then it will a)get recycled into the vesicle and b) get degraded by MAO
2)NE can diffuse out of the synpase and get degraded by COMT and MAO
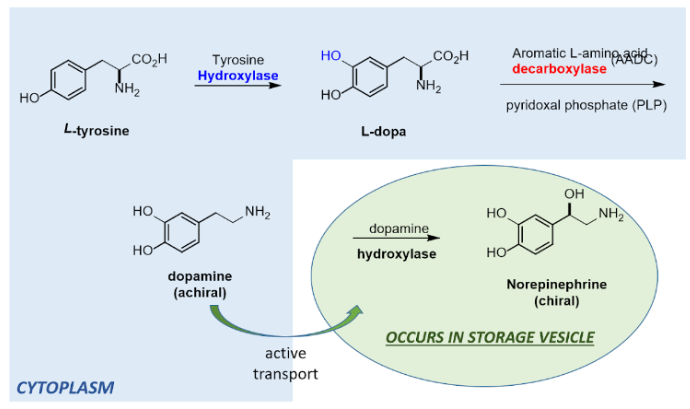
Norepinephrine Biosynthesis
•L tyrosine is hydroxylated by tyrosine hydroxylase into L-Dopa
•L Dopa is decarboxylated by Aromatic L amino acid with cofactor PLP decarboxylase turning it into dopamine
•Dopamine is actively transported into a storage vesicle
•Dopamine is turned into norepinephrine by dopamine hydoxylase
protonated state of epinephrine/norepinephrine at physiological pH
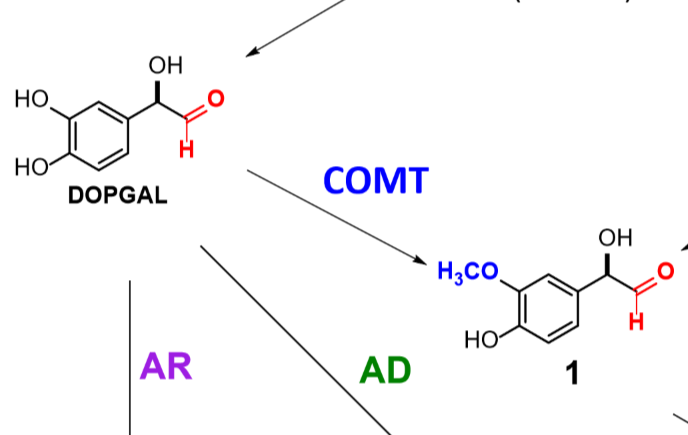
what enzymes are involved in the metabolic breakdown of norepinephrine/epinephrine.
COMT
MAO
Aldehyde reductase
Aldehyde dehydrogenase
What does COMT do
Recognizes catechols & converts one of the OHs to an ester
What does MAO do
Monoamine oxidase - oxidative enzyme that focuses on the amine functional group of norepinephrine and drugs like it.
Turns amine into aldehyde
What kind of receptors are Adrenoreceptors
G protein coupled receptors
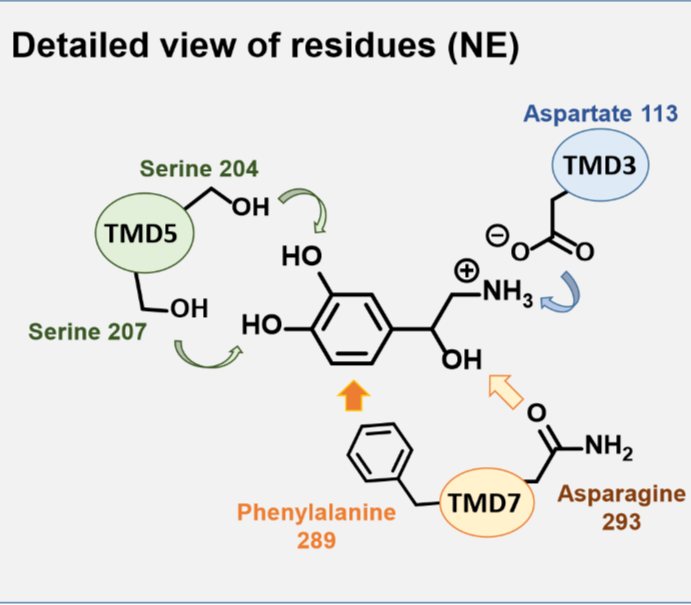
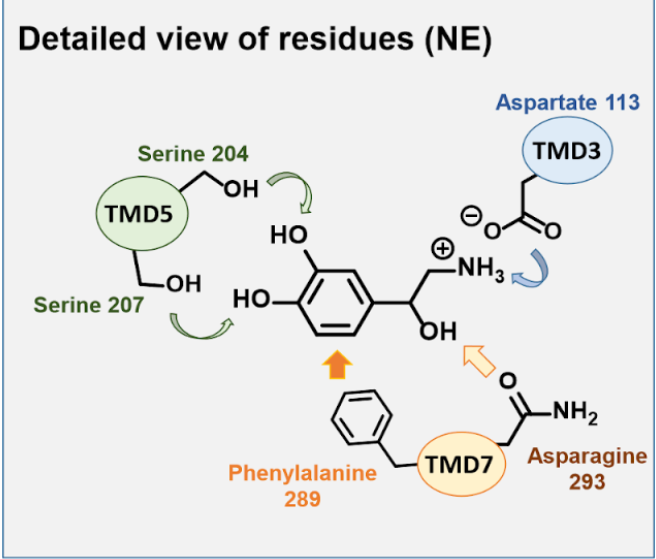
binding features of NE with its receptor-What residues are important and with what functional groups of NE do they interact?
Serine interacts with the catechol
Aspartate interacts with the amine via charges
Asparagine interacts with OH
Phenylalanine interactions with the aromatic ring
Where are adrenergic alpha receptors found ?
alpha 1 & 2 on vascular smooth muscle
alpha 2 on presynaptic neuron
What is the role of alpha 2 receptors on the presynaptic neuron?
regulating NE release
What three second messengers are relevant in the stimulation of alpha-1 adrenergic receptors?
Stimulation results in increase in:
Inositol 3 phosphate (IP3)
1,2 diacylglycerol (DAG)
Calcium
what physiological effects result from stimulation of alpha-1 adrenergic receptors?
Vascular smooth muscle contraction
Vascular constriction
(antagonists used to treat hypertension)
Where are beta adrenergic receptors found
•Beta 1 reside mostly on cardiac tissue
•Beta 2 reside in lung tissue, liver, skeletal muscle blood vessels, intestine, uterus
what physiological effects result from stimulation of beta adrenergic receptors?
→Increased heart rate (B1)
→Dilation of bronchioles and skeletal muscle blood vessels (B2)
→Breakdown of glycogen to glucose (B2)
B1 antagonists used to treat hypertension
B2 agonists treat asthma or COPD
What are the relevant effector protein and second messengers in adrenergic beta receptor signaling?
Beta receptor stimulation:
Activates adenylate cyclase which converts ATP to cAMP → increased concen of cAMP → alters Ca2+ flux
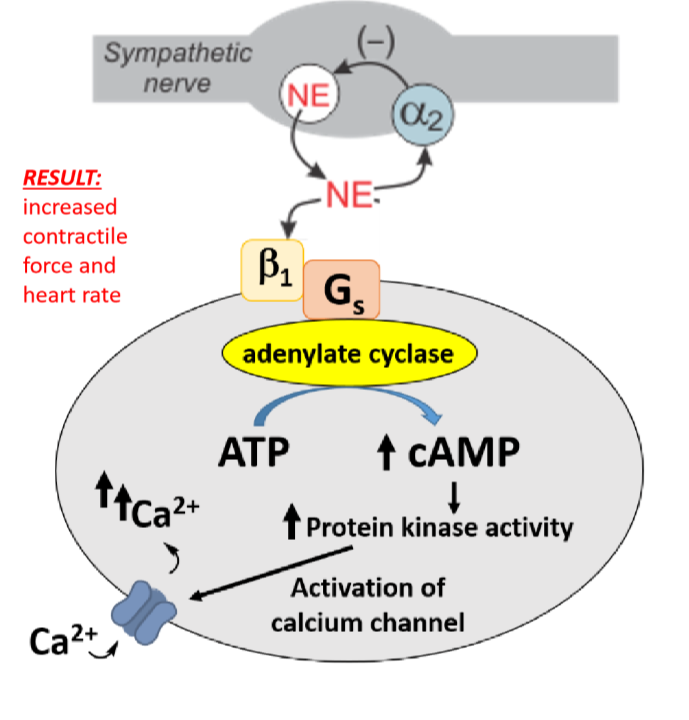
B1 receptor stimulation
Resides mostly on cardiac tissue
Activates adenylate cyclase → increased concen of cAMP → increased protein kinase activity → phosphorylation of calcium channels →increased influx of calcium → increases association between actin and myosin→ increases contractive force and heart rate
Result: increased heart rate and contractile force
B1 antagonists treat
hypertension
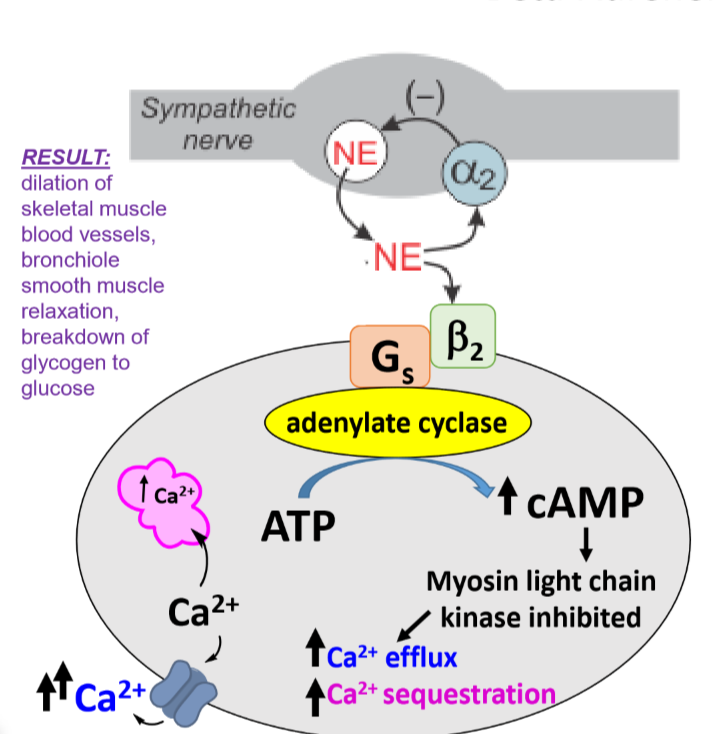
B2 receptor stimulation
Reside in lung tissue, liver, skeletal muscle in blood vessels, intestine, uterus
Increased adenylate cyclase activity → increased cAMP production → myosin light chain kinase inhibition → increased calcium flux in opposite direction compared to B1 receptors→ reduced actin myosin interactions → smooth muscle relaxation in bronchioles
B2 agonists treat
Asthma or COPD
SAR for phenylethanolamines
Amine is separated by 2 carbons from a benzene ring
2)C1 is hydroxylated
3)Nature of substitution elsewhere affects selectivity and duration of action by augmenting lipophilicity or oral bioavailability
Why does NE have limited clinical use?
Nonselective agonist
Is NE an oral drug?
IV only- No oral bioavailability
What is NE used for? What adrenergic receptors are relevant to its clinical use?
Hypotensive crisis (sudden drop in BP)
alpha activity raises BP
B activity stimulates heart
What uses does epinephrine have clinically? What adrenergic receptors are relevant to those uses?
Hypotensive crisis (IV) - alpha activity raises BP, B activity stimulates heart
Asthma (inhaler)- relieves bronchoconstriction (B2)
Allergic emergency (Anaphylaxis
Is epinephrine an oral drug?
No- no oral bioavailability due to rapid metabolism
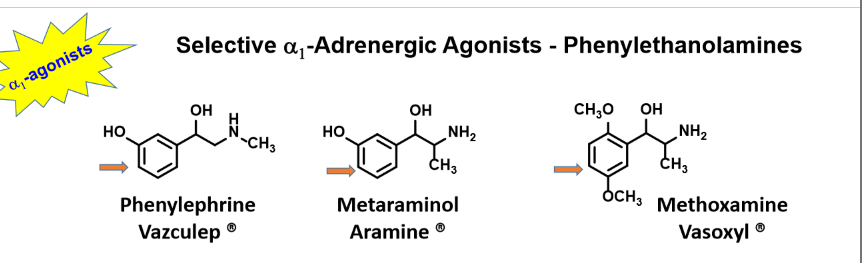
Selective alpha 1 adrenergic agonists- phenylethanolamines
Phenylephrine
Metaraminol
Methoxamine
why phenylethanolamines phenylephrine, metaraminol and methoxamine have longer duration of action compared to NE?
No COMT liability leads to longer duration of action
why phenylethanolamines phenylephrine, metaraminol and methoxamine have limited cardiac stimulatory effects compared to NE?
No beta 1 activity
physiological effects of using phenylephrine, metaraminol and methoxamine and why/how they are used clinically?
Strong vasoconstrictors
Use: Hypotension during surgery or accompanying shock
Phenylephrine use: nasal decongestant
Selective alpha 1 agonists- 2 arylimidazolines
Xylometazoline
Oxymetazoline
Tetrahydrozoline
Naphazoline
how the 2-arylimidazolines xylometazoline, oxymetazoline, tetrahydrozoline, and naphazoline are used clinically and with what receptor(s) they interact preferentially.
Alpha 1 agonists
Use: eye drops to treat red eye and topical nasal decongestants
Alpha 2 agonist
Brimonidine
Brimonidine
Use: Glaucoma
Side effects: fatigue/drowsiness
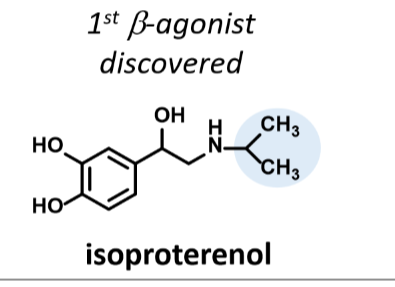
Isoproterenol
1st B agonist discovered
Non selective
Not orally active bc catechol is metabolized by COMT
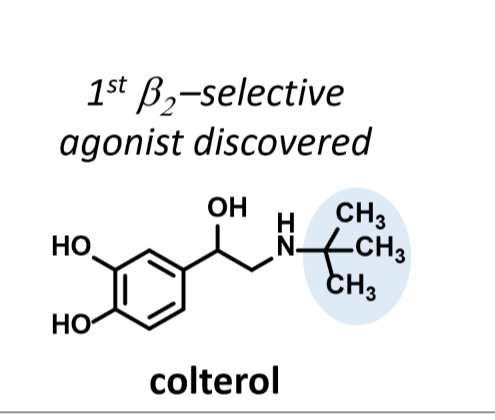
Colterol
(One more methyl group than isoproterenol)
selective B2 agonist
Not orally active bc caetchol is metabolized by COMT
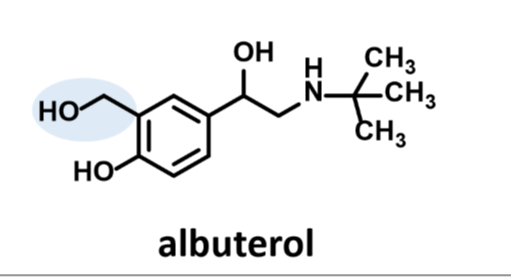
Albuterol
Selective B2 agonist
Orally active
Altered catechol is not a substrate for COMT
Short acting B2 agonists
Albuterol
Pirbuterol
Airsupra
what albuterol and pirbuterol are used for clinically.
Bronchodilator
the structural difference between albuterol and pirbuterol?
Pirbuterol has an N in the aromatic ring
What side effect profile albuterol that might make pirbuterol a better patient choice?
Racing heart beat
Airsupra
Albuterol + Budesonide
Rescue inhaler
Use: Asthma and associated exacerbations in adults over 18
MOA: Bronchodilator (albuterol) + anti inflammatory (budesonide)
Side effects: headache, oral candidiasis, cough, hoarseness
Long acting B2 agonists
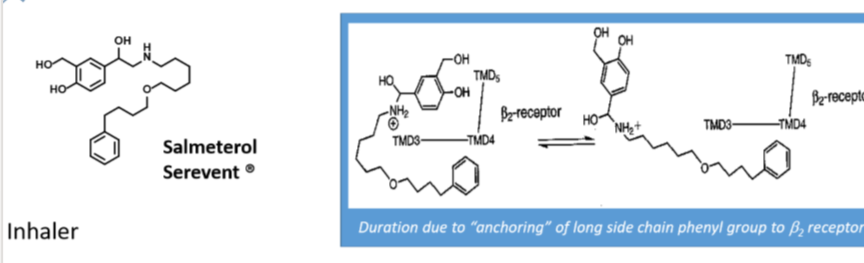
Salmeterol
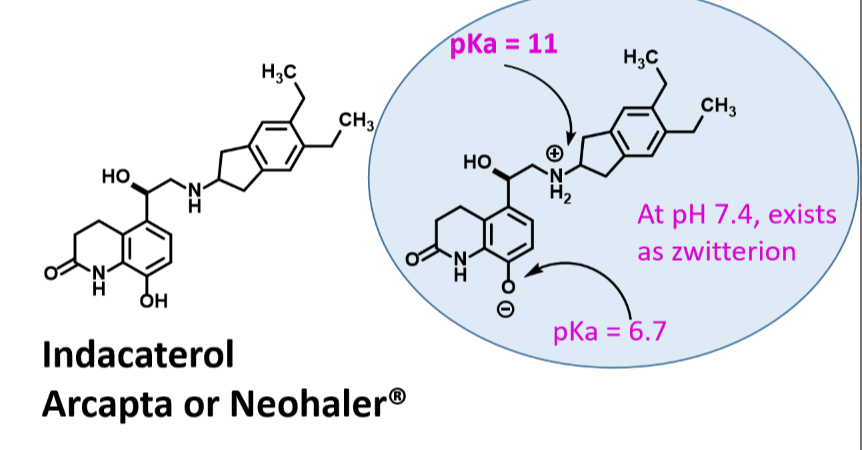
Indacaterol
Symbicort
Advair
Trelegy
Breztri
Salmeterol
Inhaler
Long acting Beta2 agonist
Use: Severe persistent asthma following treatment with short acting B agonist
Duration: 12 hours
Longer duration due to anchoring of long side chain phenyl group to B2 receptor
Indacaterol
Long acting Selective B2 agonist
Zwitterionic character promotes membrane interactions → longer duration
Duration: 24 hour
Use: Bronchodilator for COPD
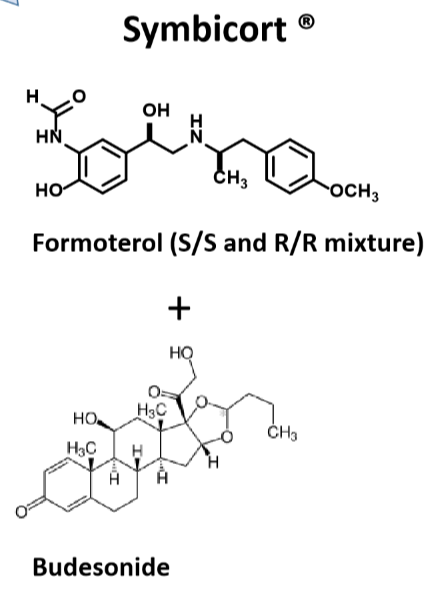
Symbicort
Long-acting B2 agonist
Formoterol + Budesonide
Inhaler
Use: reduce exacerbations of asthma, COPD
Wash mouth after use to avoid thrush (budesonide steroid)
Advair
LABA
Fluticasone (corticosteroid) + Salmeterol
use: severe persistent asthma following treatment with short acting B agonist, COPD
Wash out moth after to avoid oral flush
Trelegy
LABA
Fluticasone (Corticosteroid) + Vilanterol (Ulta LABA) +Umeclidinium Bromide(long acting muscarinic antagonist
1)Open airways
2)Keep airways open
3)Reduce inflammation
Use: Asthma and COPD
Does not replace rescue inhaler
Breztri
Budesonide (corticosteroid), Formoterol (LABA), Glycopyrrolate (long acting muscarinic antagonist)
1)Open airways
2)Keep airways open
3)Reduce inflammation
Use: COPD ONLY
Does not replace rescue inhaler