Assessing Resonance CC12 Voice/Resonance
1/71
Earn XP
Description and Tags
Dr. Estes
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
Cleft overview
Each year in the United States approximately 3% of all infants are born with a birth difference (Centers for Disease Control and Prevention, 2023).
One of the most common birth differences is cleft lip with or without palate involvement (National Institute of Dental and Craniofacial Research, 2021).
Children born with cleft lip and/or palate often require multiple surgeries to reconstruct oral and facial structures to establish improved speech, hearing, and swallowing abilities.
Cleft lip and cleft palate are among the most common birth differences (Mayo Foundation for Medical Education and Research, 2024).
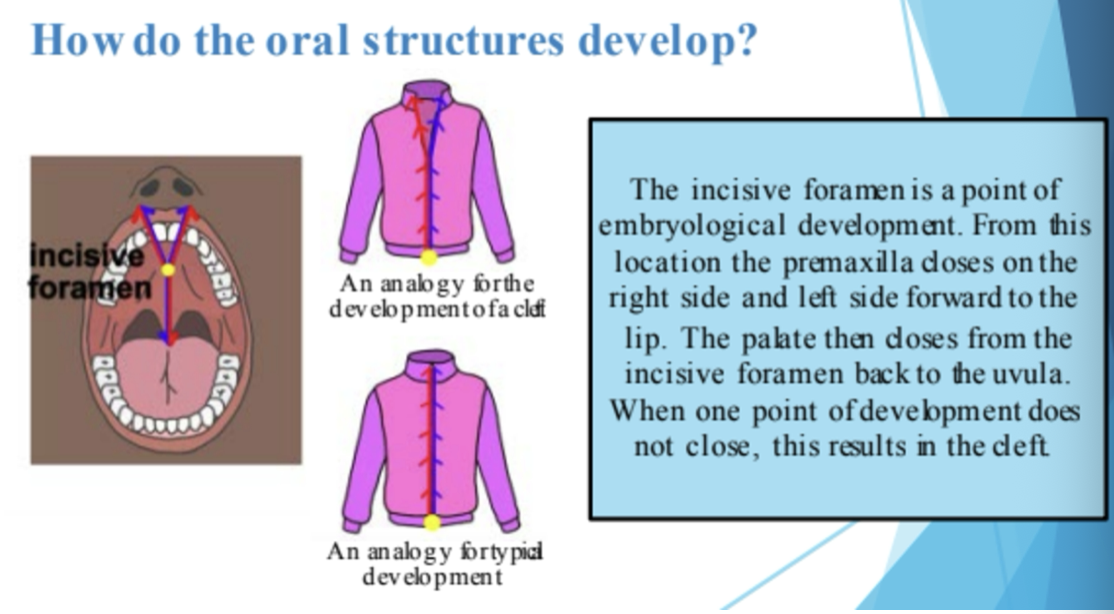
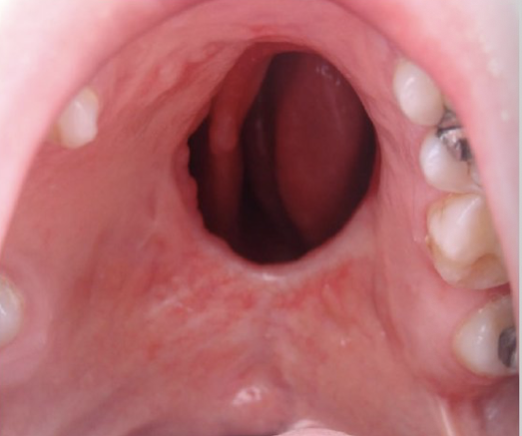
How do the oral structures develop?
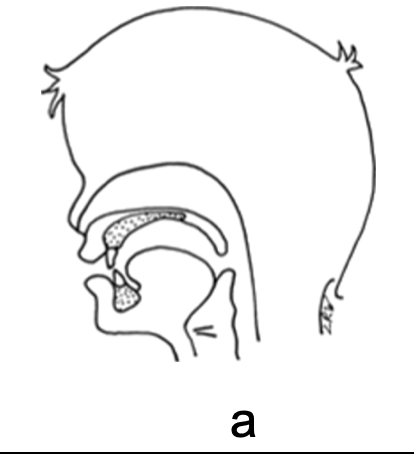
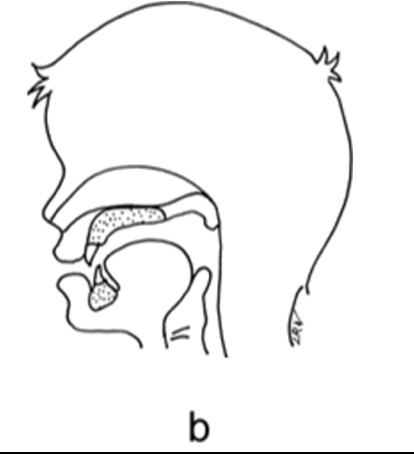
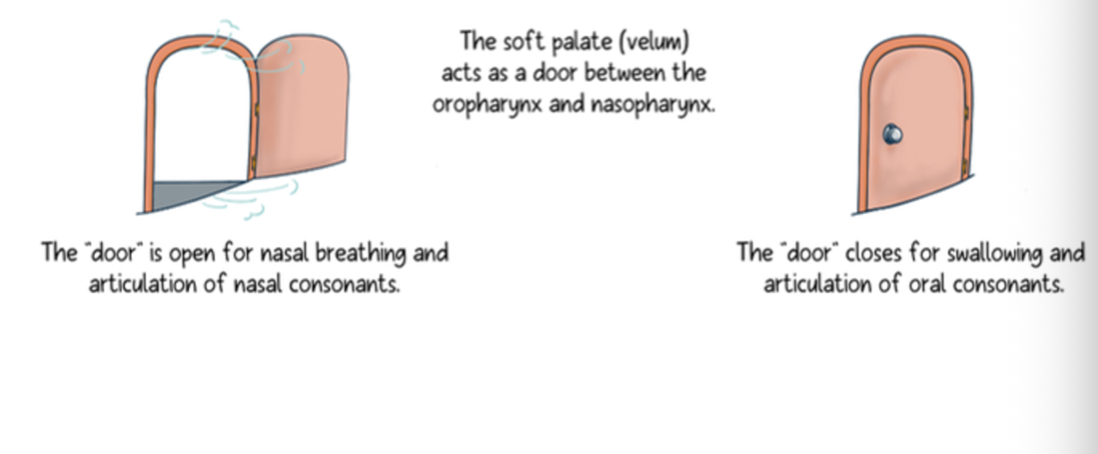
Velopharynx at rest
Competent velopharyngeal function
Incompetent velopharyngeal function
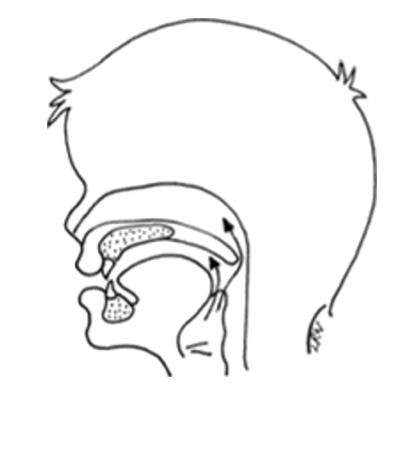
Normal Velopharyngeal Function
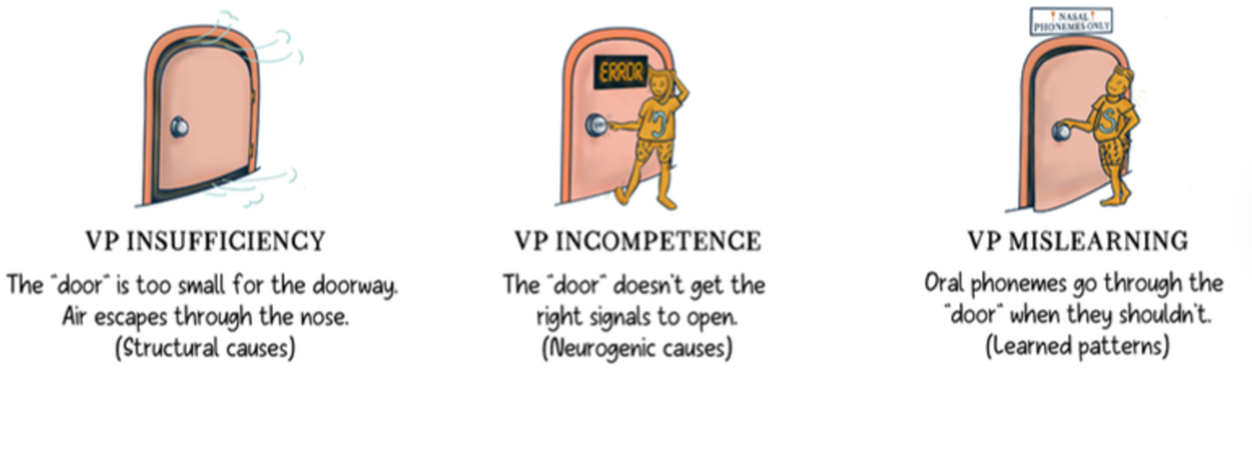
Velopharyngeal dysfunction
Comprehensive Assessment of Clefts
Detailed case history
Hearing screening
Oral mech exam
Resonance - Hypo/hypernasaltiy, cul-de-sac or mixed
Articulation - usually related to VPD (compensatory articulation)
Feeding/swallowing - usually related to VPD (nasal regurgitation)
Language - may be related to syndrome
Diagnostic Interview
Caregiver or patient fills out questionnaire
Form needs to include questions about
Resonance
Phonation
Articulation
Feeding/swallowing
Language
Clinician asks probing questions to fill in gaps from the questionnaire
Feeding/Swallowing Screening
Many patients with resonance issues related to VPD also report issues with swallowing
Nasal regurgitation is commonly reported by patients
Gagging or globus (feeling of food stuck in the pharynx) is sometimes reported
In adults with degenerative disorders, VP function and swallow function may be first signs of the disorder
SLP may be first professional to identify the neurodegenerative disease and will need to make further referrals to the neurologist and other professionals
Language Screening
Children with cleft lip/palate are at increased risk for language delay
Best practice is to conduct a language screening annually
Formal language screener or language sampling procedures
Comprehensive language evaluation should be done for children with
Syndromes
Hearing loss
Neurological issues
Other risk factors
Adults with degenerative diseases often have language and cognitive deficits as well, so it’s always good to screen for these areas
Articulation, Phonation, and Resonance Diagnosis
Begins with a perceptual assessment
Perceptual assessment is far more important than instrumental
This will determine if instrumental assessments need to be performed - can save time and money
Survey of 126 SLPs found 99.2% of SLPs on cleft teams use perceptual assessment of VPI (Kummer, 2012)
Listen for articulation of speech sounds, phonation, and resonance
Perceptual (Non-instrumental Assessment)
Perceptual assessment: SLP uses clinical judgment to determine if hypernasality or NAE is present, and makes inferences about VP function
If the perceptual assessment shows no speech abnormality, then it does not matter what the instrumental assessments show
No treatment is warranted
If there is a speech abnormality - perceptual assessment should determine if it is structural or functional
Judgment of phonation - determine if full voice evaluation is needed
Perceptual Assessment
Perceptual assessment is sufficient to diagnose type of resonance disorder (hypernasality, hyponasality, etc.)
Strategically using different speech samples, such as comparing an all oral passage vs a nasal-loaded passage, can facilitate differential diagnosis for type of nasality
Perceptual Assessments Reveal
Formal Articulation Tests
Typically only assess word level, some have sentences also
Usually neglect other levels of the articulation hierarchy, but SLP can probe
Does not take into account co-articulatory or context effects
Often too time-consuming in a medical setting
GFTA-3
Arizona-4
Iowa Pressure Articulation Test
Templin-Darley Tests of Articulation
Bzoch Error Pattern Diagnostic Articulation Test
Assessment of Speech Sounds and Intelligibility
Document phonetic inventory
Note any phonological or developmental errors (GFTA or DEAP)
Rate overall intelligibility
Parent rating scale like the Intelligibility in Context Scale (ICS) and a quality of life measure like the CLEFT-Q
Speech Samples Use
Use of speech samples is highly recommended in this population (adults and children)
Speech Sample Assess
Assess speech production, resonance, and phonation simultaneously
Speech Samples Do not Focus
Do not focus just on word level, but includes isolation, syllables, sentences, and connected speech
Speech Samples Consider
Consider developmental guidelines for speech sound production and syntax in children
Must determine if it is a developmental error, obligatory error, or a compensatory error caused by the structural/functional deficit
Speech Sample: Phoneme/Syllable Repetition Critical in children with
Limited repertoires
Little connected speech
Minimal English
Poor compliance with standardized tests
Speech Sample: Phoneme/Syllable Repetition Critical in adults with neurogenic disorders
May be able to produce sounds in isolation/syllables, but not in longer utterances
May fatigue over time, so beginning of speech sample and end of speech sample may sound different.
Phoneme/Syllable Repetition:
Test for hypernasality with vowel prolongation (low vs high vowels)
Test NAE with high-pressure voiceless consonants (fricatives, affricates, stops)- easier to hear
Prolong /s/ to assess ability to maintain palate closure
Connected speech:
Places the highest demand on the VP for closing, maintaining closure, and timing for re-opening
Counting:
Have the patient count from 60 to 70
Small-medium size VP gap- NAE will be audible
Large VP gap: there will be no pressure build up for /s/ or the /kst/ blend
Speech Sample: Sentence Repetition
Assess articulation placement and resonance at sentence level
See Table 11-3 for recommended sentences for each phoneme
This will reveal if there is breakdown with:
Length of utterance
Speed of production
Specific phonemic contexts
Fatigue factor
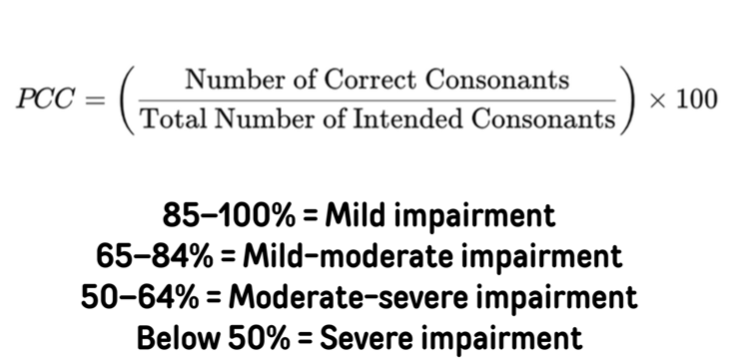
Calculating Precent Consonants Correct (PCC) can give you an easy baseline measure for progress monitoring
Speech Sample: Counting
If old enough, have patient count from 60 to 70
Numbers contain repeated combinations of high vowel /i/ with /s/ and triple blend /kst/
There is a constant build-up and controlled release of air pressure in the oral cavity
The VP port should maintain closure from 60 to 67, then VP closure alternates from 67-68-69-70
Small-medium sized VP gap - NAE will be audible on this counting task
Large VP gap: there will be no pressure build up for /s/ or the /kst/ blend
Speech Sample: Connected Speech
If the patient is willing to be conversational, this is an important last piece of speech sample
Connected speech has the highest demands on VP mechanism for closing, maintaining closure, and timing the re-opening
Both hypernasality and NAE are more apparent in connected speech
Articulation errors often increase during connected speech
VPD related to fatigue generally worsens during connected speech
What should an SLP look for in speech sample
Speech sound production
Stimulability
NAE
Weak consonants
Short utterance length
Oral-motor dysfunction
Type of resonance disorder
Voice disorder - is there concomitant voice problem?
Speech Sound Production & Stimulability
All articulation errors in speech sample should be classified as:
Developmental Errors: in children only, not adults
Do not correct in ST until it is developmentally appropriate
Obligatory Distortions: articulation placement and manner is correct, but abnormal anatomy causes distortions in speech
These are not ST issues - they are surgical or dental issues
Speech Sound Production & Stimulability
Compensatory Errors: patient attempts to produce the sound, making errors in placement or manner due to working around incorrect anatomy and physiology (hence compensatory)
To treat compensatory errors, SLP should correct placement and manner
May still be obligatory errors until the VP mechanism is surgically corrected
Manner is maintained but placement is moved backwards behind the point of cleft or fistula (/?/ for /d/ or /k/ for /t/)
Placement is similar but manner of production is changed, e.g. /n/ for /s/
Also look for co-articulations (i.e., placement for /t/ along with a glottal stop)
SLP should eliminate glottal stop
Use diacritics or write words (pharyngeal stop) when completing articulation tests with odd compensatory productions
Do stimulability testing for each error
Note any weak consonants: often accompanies hypernasality or NAE
NAE Describe type of nasal emission sound
Low intensity (large VP gap)
Turbulent, rustle sound (small VP gap)
NAE
Nasal grimace (scrunched face) may be present
NAE Observe and Note
which sounds have NAE
consistency of NAE across phonemes
consistency of NAE on short versus long utterances
NAE Utterance Length: have patient count 1-20
Patient should make it to 15 before taking a breath
Why would a patient with VPD have shorter utterance length?
Oral-Motor Dysfunction
Hypernasality can be due to neuromotor disorder
VP structure may be normal, but neuromotor control may lead to VPI
Levator veli palatini: pharyngeal branch of vagus
Tensor veli palatini: mandibular branch of trigeminal nerve
Pharyngeal constrictors: vagus nerve
Formal apraxia test
Kaufman Speech Praxis Test
Dynamic Evaluation of Motor Speech Skill
Diadochokinesis
Phonation (Voice Diagnostic Screening/Assessment)
Dysphonia is common in patients with resonance disorders
CAPE-V (Consensus Auditory-Perceptual Evaluation of Voice)
Phonation (Voice Diagnostic Screening/Assessment) Listen for and rate on severity scale:
Hoarseness
Breathiness
Glottal fry
Glottal attacks
Inappropriate pitch level
Restricted pitch range
Inappropriate intensity level
Visual Detection
Mirror Test: hold a small mirror under the nose
See how much mirror fogs up during oral speech sounds (no nasal sounds)
Air Paddle: hold a slip of paper under the nose
See it move during production of high-pressure oral speech sounds (no nasal sounds)
See-scape: a small flexible tube runs from the nostril to a vertical rigid tube
As high-pressure oral consonants are produced, NAE will cause the Styrofoam ball in tube to move up and down
Tactile Detection
Feeling sides of the nose = by palpating the sides of the nose, SLP can sometimes feel the vibrations in the nasal cavity
Auditory Detection
Nose Pinch Test: patient says an all oral utterance with nose pinched closed, then repeats with nostrils open
If resonance sounds same both times, VP port functions normally
If there is a difference in resonance, VP port is not closing on its own
Stethoscope: place drum of stethoscope beside nose, or remove drum and place the tube in end of nostril
Can clearly hear hypernasality or NAE
Listening tube/straw: place one end in nostril and other end near ear to clearly hear hypernasality or NAE
Differential Diagnosis of Cause: VPI vs Fistula vs Artic Diagnosis
Consistency of hypernasality/NAE
Phoneme-specific hypernasality/NAE = mislearning (Only /s/ or high vowels but not low vowels)
Consistent NAE on all pressure sensitive consonants = VPI
Intermittent hypernasality = apraxia
Consistent hypernasality = VP
2. Stimulability testing
Hypernasality/NAE do not improve with articulation correction = VPI
Hypernasality/NAE do improve with articulation correction = mislearning
Fistula contributions to resonance/NAE
Plug fistula with chewing gum or a cotton ball covered in Vasoline
Compare speech with fistula plugged and unplugged
Small fistula (less than 5 mm) = no effect b/c airstream is lateral to opening
Large fistula will likely produce hypernasality
Medium ones are difficult (oral side opening may look larger than actual opening in nasal cavity)
Pharyngeal fricative vs lateral /s/ versus NAE with /s/ production (Pharyngeal fricatives can sometimes sound like NAE because of rustly sound in back of pharynx)
First, place a straw in the nostril to listen for NAE on /s/ attempt
Then, place straw at midline of the dental arch and listen for airflow on /s/
Move the straw laterally (at small increments) until SLP hears airflow on /s/ attempt
Will determine if the airflow is coming medially or laterally through oral cavity, or through nasal cavity
Small Fistula

Large Fistula
Referrals
Radiology, ENT, neurology, sleep study, etc.
Reccomendations
ST?
Frequency?
Counseling
Family counseling
Genetic counseling
Evaluation Report
No standardized method
Should contain all components of a typical evaluation (like the ones in our clinic)
Indirect Instrumental Procedures
Nasometry
Speech aerodynamics
Provide objective data regarding the physical correlates of VP function
Acoustic output
Airflow
Air pressure
Provide scores that can be compared to standardized norms
Pre- and post-treatment scores can be compared
Do not directly visualize VP port and other structures
Provide data to infer velopharyngeal function
Cannot directly observe velopharyngeal functions
Nasometry
Assesses hyper/hyponasality, NAE, and VP function
Survey of 126 SLPs found 28.9% use nasometry (Kummer, 2012)
Only 19% of SLPs who work on cranio teams use nasometry
Far fewer SLPs who work in other settings use nasometry
Almost no SLPs in public schools or private clinics use nasometry
Some universities use it, but usually only if needed for research
Nasometry
Separator Plate divides nasal airflow from oral airflow
Standardized passages are repeated or read aloud
Measures nasal airflow (N) and oral airflow (O)
Calculate nasalance score by dividing N/(N+O) and convert to a percentage
Nasalance = % of nasality in speech
Nasalance distance: range between maximum and minimum nasalance
Nasalance ratio: minimum nasalance divided by maximum nasalance
Standardized Speech Samples Good for adults, but requires reading, attention span, cognitive ability for complex vocab and syntax (Appendix 14-1 in Kummer)
Zoo passage: no nasal phonemes
Can VP closure be achieved and maintained throughout connected speech? Does not test timing of closure
Rainbow passage: has 11.5% nasal phonemes (same as normal SAE)
Nasal Sentences passage: 35% of phonemes are nasal
Good for testing hyponasality and nasal obstruction
Standardized Speech Samples For children, recommend using SNAP Test-R (App 14-2 in Kummer)
Subtest 1: syllable repetition
Subtest 2: connected speech, using carrier phrases
Subtest 3: reading child-friendly passages
Nasometry in Treatment
Provides real-time visual feedback about nasality
Treatment is only useful if the patient is anatomically and physiologically capable of closing VP mechanism during connected speech
Indicated for phoneme-specific learned hypernasality
Helpful for post-surgical treatment when patient is learning to use newly corrected anatomy
SLP sets goal by creating a reference line, and patient works to keep their nasalance line below reference line
As patient makes progress, reference line can be moved little by little until the patient matches normative score
Speech Aerodynamics
Measures the airflow and air pressure in the oral and nasal cavity during speech to:
Estimate airway obstruction by measuring nasal airway resistance
Calculate the size of the VP opening
Survey of 126 SLPs found 4.3% use aerodynamics (Kummer, 2012).
Used more in research than actual clinical practice
“Orifice Equation”
Cross-sectional area across the opening of any orifice (including the VP port) can be calculated if you know:
Air pressure before the orifice (Point A)
Air pressure after the orifice (Point B)
Air flow through the orifice
“Orifice Equation” Applied to VP Port Pressure-Flow Technique
Insert one pressure transducer into oral cavity (Point A)
Insert second pressure transducer into nasal cavity (Point B)
Insert flowmeter into other nostril to measure air flow through VP port
“Orifice Equation” Applied to VP Port Placement of oral transducer must be behind place of artic
If there is a moving airstream, the open end of the catheter must be perpendicular to flow
Bilabial stops are usually the easiest placement for the transducer
“Orifice Equation” Applied to VP Port Reported measures can be compared to norms
Air pressures will be reported as cm H2O
Air flow will be reported as mL/sec
VP area will be reported as mm2
“Orifice Equation” Applied to the Nasal Cavity Anterior
Rhinomanometry: nasal resistance and nasal area are measured for both nostrils during quiet breathing
Uses tubing placed in each nostril one at a time
“Orifice Equation” Applied to the Nasal Cavity Posterior
Rhinomanometry: nasal resistance and nasal area are measured for each nostril during quiet breathing
Uses a mask placed over the whole nose
“Orifice Equation” Applied to the Nasal Cavity
Patient scores must be compared to aged norms, as the face grows dramatically throughout childhood changing the average cross-sectional area of the nasal cavity
Direct Instrumental Procedures
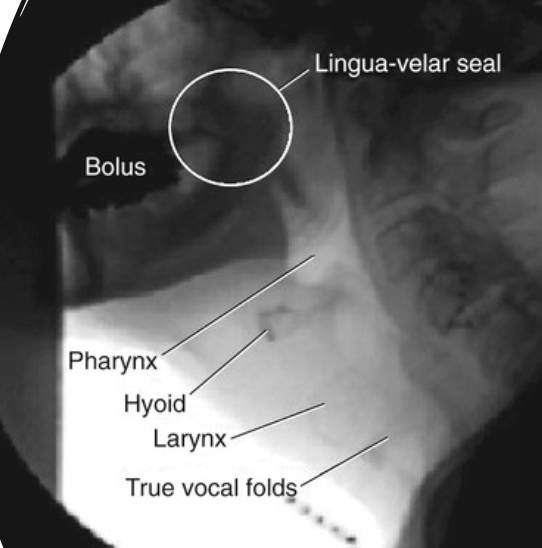
Videofluoroscopic Speech Study (VFSS)
Video Nasendoscopy Evaluation of Speech (VNES)
Allow direct visualization of anatomy and physiology during speech and swallowing, but actual assessment is subjective
See cause of VPD
Determine location of VP gap
Determine pattern of VP closure
Assess placement of prosthetic
Pre- and post-operative assessments
VFSS was gold standard until 1980s
59.3% of SLPs use VNES and 19.2% use VFSS (Kummer, 2012)
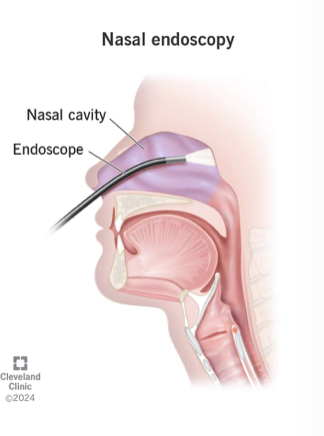
Nasal Endoscopy
Direct Instrumental Procedures
MRI can also be used
Disadvantages = too loud for some children, claustrophobic, too expensive
MRI may eventually replace videofluoroscopy as technology becomes cheaper
VFSS and VNES Speech Sample
Must tax the velopharyngeal mechanism to induce VPD in mild cases
Repetition of sounds, syllables, words, and sentences
Use high-pressure phonemes with high vs low vowels
/pa/ /pa/ /pa/ vs /pi/ /pi/ /pi/
Use front and back consonants
/pa/ /pa/ /pa/ vs /ka/ /ka/ /ka/
Prolong /s/ sound
Reading of passages, age permitting
Counting 60-70
Videofluoroscopy
With patient supine, use a syringe to inject barium into both nostrils and instruct patient to “sniff it up”
Rotate head to evenly distribute
Will coat nasal cavity, nasopharynx, and oropharynx
Use multiple positions while patient repeats the speech samples (VFSS is 2-D, so multiple views needed to reconstruct 3-D port)
Lateral (sagittal) view: visualize velar lift, adenoids, posterior pharyngeal wall, lingual movement
Frontal (a-p) view: visualize lateral pharyngeal wall movement and septum
Base (bottom-up) view: visualize the circular port from below
Towne’s (top-down) view: visualize the circular port from above
Oblique view: visualize the port at a 45 angle on the right and the left = used with large adenoids or patients with asymmetrical lateral pharyngeal wall movement
Have patient swallow first to check VP port function during swallow
Patient completes the speech sample in each position
Barium will bubble up on small VP gaps, allowing better visualization for gaps that may not be visible to the eye on screen
Videofluoroscopy
Video Nasendoscopy
Minimally invasive direct visualization of nasal, pharyngeal, and laryngeal cavities by inserting a flexible camera scope thru nose
Used during speech sound production or swallowing to observe function
Full color, high resolution cameras provide maximum visibility
No barium or radiation required
Can be performed by an SLP independently
Much more cost effective that fluoroscopy
Patient completes speech sample
Documenting instrumental assessment
Some SLPs use narrative/descriptive format
Other SLPs use check lists or rating scales
No standardized format
Must include cause of resonance disorder, size of VP gap, location of the gap, location of any fistulae, pattern of closure, phoneme-specific differences in VP function or gap size, severity ratings for hypo/hypernasality and NAE