Exam 3: Functional Mobility
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
what is mobility?
mvmts that results in a change of body position or location
what is bed mobility?
moving from one bed position to another
-rolling to sidelying
-supine to sit
-sit to stand
what is a transfer
mvmt from one surface to another
influencing factors for functional mobility include
-age
-stage in life cycle (infancy → adulthood)
-social and cultural variations (walking, wheelchair)
-physical environment (ramps, stairs)
-acceptable degree of independence
-individual environmental factors
-societal environmental
functional mobility outcome measures
-patient's build (body weight, height, etc.)
-pre-morbid performance patterns (if sedentary before, then won't be active now)
-habits, roles, routines
-psychological state
-pain (pre-existing, secondary impairment)
activities in supine position include
1) bridging
2) rolling (toward affected - easier; toward unaffected - hard)
3) side-lying to sit
bridging
-back and hip extensors support the body
-UE's assist in providing proximal stability
what muscles support the body when bridging
back and hip extensors
when bridging, the _____ assists in providing proximal stability
a) UEs
b) LEs
a) UEs
what are the functional purposes of bridging
-use of a bedpan
-LB dressing in supine
-reduce pressure on butt
-bed scooting
what are the causes of ineffective mvmt when bridging
-absent or decreased back and hip extensors
-decreased recruitment of abdominals
-reduced proximal stability
easier?
a) rolling toward affected side
b) rolling toward unaffected side
a) rolling toward affected side
more difficult?
a) rolling toward affected side
b) rolling toward unaffected side
b) rolling toward unaffected side
rolling toward affected side
1) preposition affected arm (shldr F 90, elbow F/E, scap pro)
2) flex unaffected knee
3) unaffected arm reaches across midline
4) unaffected leg crosses midline
*instruct pt NOT to push against surface w/ unaffected LE
*practice rolling to affected side and back to supine
*once improvement occurs, have pt lift head slightly and rotate toward direction of mvmt
rolling toward unaffected side
-frequently initiated by extensor pattern of head, neck, and back
-affected arm is "left behind"
-instruct pt to use unaffected UE to 1) flex affected knee and bring it across midline and 2) bring affected UE up and over chest
*can use bedrail as assist but discouraged bc not readily available at home
*provide manual A to hip and trunk during rolling (decrease A as ability improves)
what are the goals of rolling toward UNaffected side
1) to decrease maladaptive compensatory strategies
2) promote more effective and efficient mvmt patterns
what ineffective movement strategies are seen with rolling toward unaffected side
-extensor pattern of head, neck, and back
-affected arm is "left behind"
supine to sit
adults typically use momentum strategy in which force is generated within the trunk and transferred to the LEs
*instead use a force control strategy
what ineffective movement strategies are seen with supine to sit
momentum strategy in which force is generated within the trunk and transferred to the LEs
what is a force control strategy for supine to sit?
graduated changes in position
1) roll to side lying
2) push up with UEs
3) bring LEs over side of bed (counterweight)
*provides increased stability
-concentric and eccentric forces used in these movements
treatment strategies for supine activities
-roll toward affected side first (decreased effort and reduces maladaptive mvmt strategies)
-rise from both sides of bed early in tx (reduces associated rxns)
-start sitting upright and learn to lie down first
activities in sitting
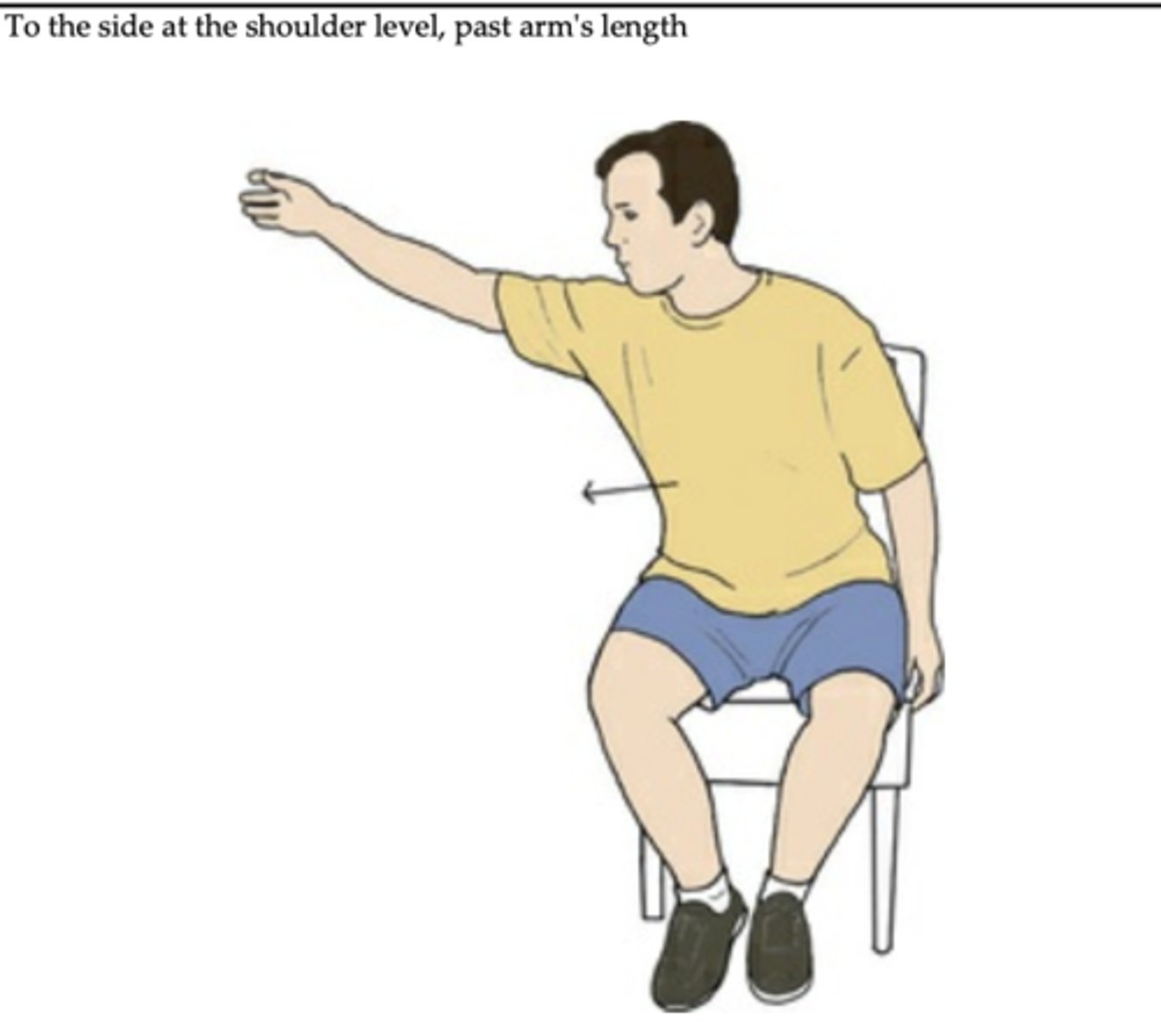
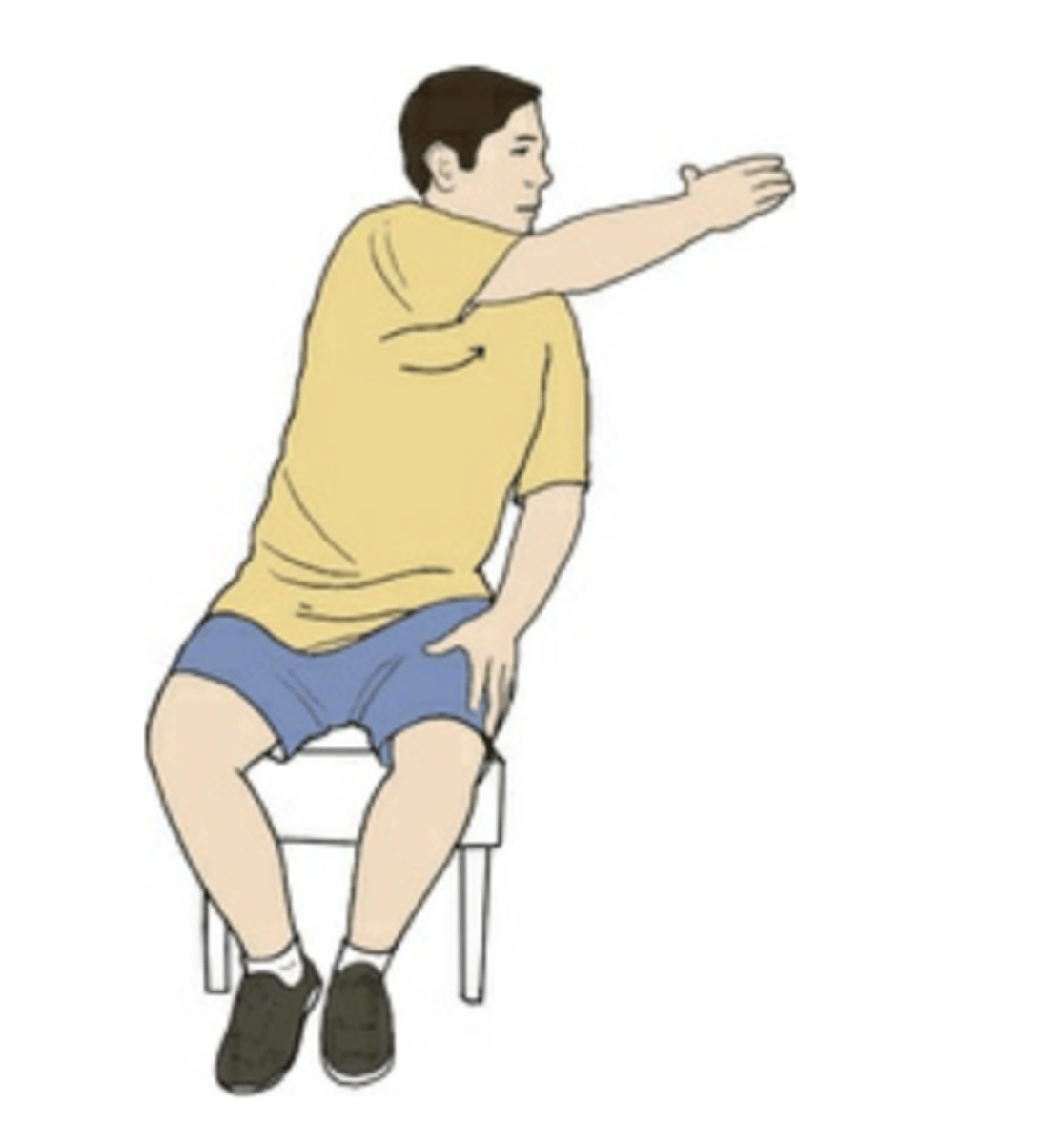
sitting and reaching
-anteriorly
-posteriorly
-laterally
-in rotational pattern
why are activities in sitting important?
bc they help to promote controlled mvmt and bear and shift weight
reaching anteriorly
concentric contraction of low back muscles
eccentric contraction of abdominals
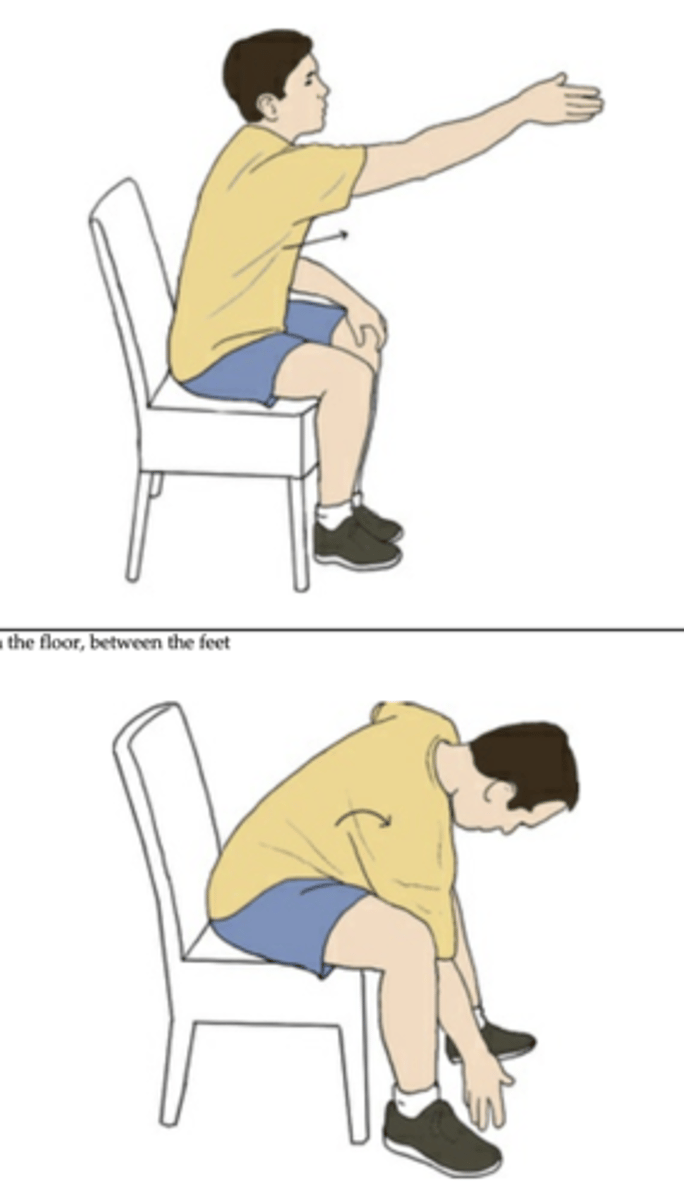
reaching posteriorly
concentric contraction of trunk flexors
eccentric contraction of trunk extensors
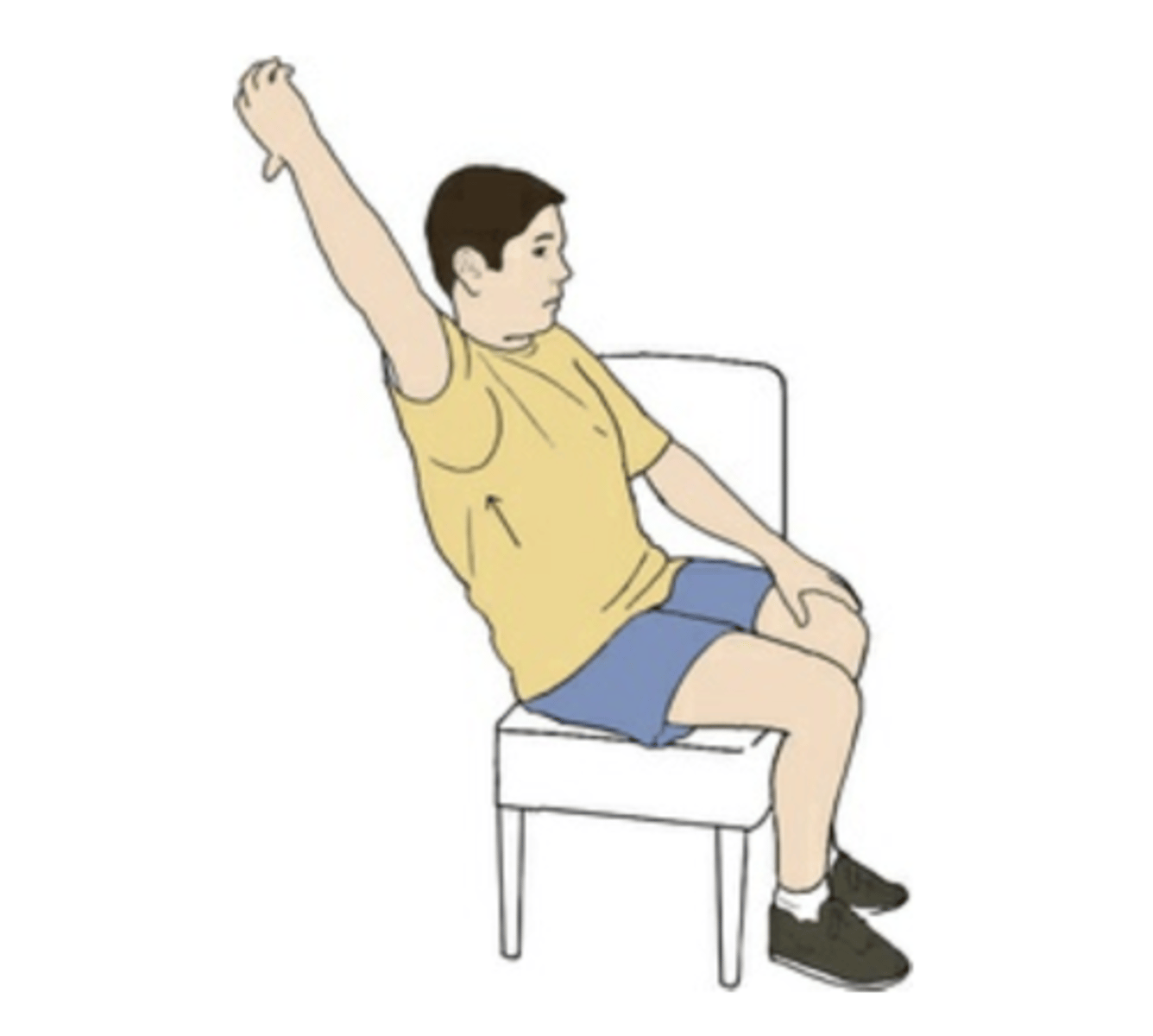
reaching laterally
concentric contraction of trunk flexors and extensors on non-WB side
eccentric contraction of ^^ on WB side
reaching in rotational pattern
primary muscles are abdominal obliques
implicit skill learning
set up the activity and environment to elicit desired movement
gradations
-modify force of manual assist
-modify amount of contact area (i.e. NDT)
-alter the reach distance (sagittal, frontal, transverse planes)
sit to stand
-knees flexed
-anterior weight shift
-elbow extension
-trunk extension
sitting treatment strategies
-begin training in "high seats" (gradually lower to standard heights)
-train to scoot toward edge to follow for hip extension and knee flexion
-promote anterior weight shifts (use verbal +/or tactile cues; manual A if needed)
-lots of forward reaching activities
-WC push-ups as HW
why are forward reaching activities important?
-increases confidence
-decreases fear of anterior weight-shifting
-important step in sit-to-stand
-increases ability of affected LE to bear weight
standing activities
1) static standing
2) dynamic standing
3) free standing balance
static standing
can use a standing table
blocking method
-pts hips against a raised mat
-OT sits on stool on pt's affected side
-OT blocks pt's knees with their own
-OT's BUE free to stabilize
dynamic standing
-gradually incorporate weight shifts (ant., post., rot.)
-introduce knee bending during weight shifts
-introduce reaching activities
free standing balance
-begin with CGA
-progressively increase distance from pt
-scanning environment while standing
-holding conversation while standing to engage cognition (make balance subconscious)