Looks like no one added any tags here yet for you.
What is a solid organ tumor?
§ Cancer in solid organs.
What is the clinical presentation of breast cancer?
§ Painless lump on exam
What is the clinical presentation of prostate cancer?
§ Ureteral dysfunction
§ Urinary frequency
§ Urinary hesitation
What happens if a solid organ tumor that is cancerous spreads to the brain?
§ It can cause confusion and motor impairment.
What happens if a solid organ tumor that is cancerous spreads to the liver?
§ It can cause abdominal distention and jaundice ( yellow of the eyes and skin).
What happens if a solid organ tumor that is cancerous spreads to the bone?
§ It can lead to bone fractures.
What are some risk factors that can increase the risk of getting breast cancer?
· Increase in age.
· Female
· Increased estrogen/progesterone exposure:
o Starting period early
o Late onset menopause
o Nulliparity or having 1st pregnancy after the age of 30.
o Postmenopausal hormone replacement therapy ( > 5 years carries highest risk
· Hereditary : 5-10% of cases:
o Tumor suppressor genes are responsible for repair of double stranded DNA breaks.
o Mutations confer high lifetime risk of developing breast cancer.
· Lifestyle:
o Increased alcohol consumption.
o Decreased physical activity/obesity.
o Radiation exposure to the chest wall.
What are some local signs/symptoms of breast cancer?
o Most seen is painless/ palpable lumps.
o Less commonly seen is pain, nipple discharge, retraction, skin edema, redness, warmth, dimpling, peau d’ orange ( breast looks like an orange)
o Palpable local-regional lymph node may also be present.
What are some systemic metastases signs/symptoms of breast cancer?
o This can vary depending on the site.
o It can include bone pain, difficulty breathing, abdominal pain or enlargement , jaundice, or mental status changes.
What laboratory test are done on breast cancer patients?
o Tumor markers such as cancer antigen ( CA 15-3) or carcinoembryonic antigen (CEA) may be elevated.
How do you diagnose breast cancer?
o Tumor markers such as cancer antigen ( CA 15-3) or carcinoembryonic antigen (CEA) may be elevated.
How do you diagnose breast cancer?
o Take a careful patient history.
o Do a physical exam on patient.
o Do a 3-D mammography of the breast tissue.
o May do other imaging of the breast.
o Take a breast biopsy.
What is non-invasive carcinomas of the breast?
o The abnormal cells are confined to the ducts or lobes.
What is invasive carcinomas of the breast?
o Abnormal cells infiltrate surrounding breast tissue.
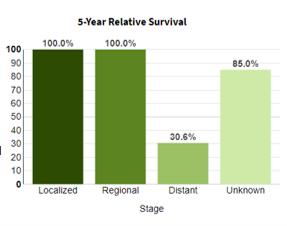
What is the prognosis of breast cancer?
5-year relative survival by subtype and stage | ||||
Subtype | All stages | Localized | Regional | Distant |
Luminal A: HR+/HER2- | 94% | 100% | 90% | 30% |
Luminal B: HR+/HER2+ | 90% | 99% | 90% | 43% |
HER2 enriched: HR-/HER2+ | 83% | 96% | 81% | 37% |
Triple Negative: HR-/HER2- | 77% | 91% | 65% | 12% |
What is the most aggressive subtype of breast cancer?
o HER2-/HR- ( aka: triple negative (TNBC))
What is the most common, but least aggressive subtype of breast cancer?
o HR+/HER2- ( aka: luminal A)
Which subtype of breast cancer is considered dual positive breast cancer?
o HR+/HER2+
What percent of breast cancers express estrogen and/or progesterone receptors?
§ 70% of breast cancers express estrogen and/or progesterone receptors.
How should HR testing be performed?
§ It should be performed on all tumors via immunohistochemistry.
What percent of tumor nuclei are HR positive?
§ Greater than or equal to 1%
What is HER-2?
§ A proto-oncogene that encodes for a transmembrane tyrosine kinase growth receptor.
§ It is involved in several regulatory pathways in the breast tissue.
What happens when the HER-2 gene is amplified?
§ When the gene is amplified, this can lead to overexpression of HER-2 receptor.
§ This results in uncontrolled cell growth.
What is the percent of breast cancers that express HER-2?
§ 15-20%
What does the IHC detects?
-it detects the amount of HER2 protein present in the cells ( this a quantitative test)
-it is reported as negative: 0 or 1+ , equivocal: 2+ ( requires the FISH test), positive: 3+
What is the FISH test?
-detects HER2 gene amplification ( this is a qualitative test)
-results are reported as negative or positive
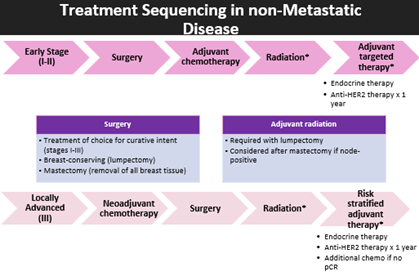
What are the treatment pathway for patients with non-metastatic breast cancer?
When is endocrine therapy given in breast cancer patients?
o It is not given until after chemotherapy treatment is completed.
Endocrine Therapy for Breast Cancer Patients:
Menopause status at diagnosis | |||
Premenopausal | Postmenopausal | ||
Tamoxifen | Aromatase inhibitor + ovarian suppression ( high-risk) | Aromatase inhibitor ( preferred | Tamoxifen |
Fulvestrant for 3rd line or metastatic , in postmenopausal status: continue until disease progression or unacceptable toxicity | |||
What is the optimal duration of therapy for endocrine therapy for a breast cancer patient?
o Therapy is for at least 5 years .
o Can be 10 years in select patients.
What are the sites where tamoxifen acts as an antagonist?
§ Breast: it helps to stop breast cancer growth.
§ Vaginal mucosa: vaginal dryness and bleeding.
What are the sites where tamoxifen acts as a partial agonist?
§ Endometrium: hyperplasia may lead to cancer.
§ Bone: increased bone strengthening in postmenopausal women.
§ Coagulation system: can increase the risk of VTE.
§ Liver: can decrease lipids.
What is the effectiveness of Tamoxifen?
§ It is a very effective medication no matter if the female patient is postmenopausal or premenopausal.
What is the metabolism of tamoxifen?
§ It is a prodrug that gets converted to endoxifen ( this medication is 100 times more potent than tamoxifen) via CYP2D6.
§ CYP2C9 inhibitor.
What are some drug-to-drug interactions that can happen when taking tamoxifen?
§ A patient should avoid strong CYP2D6 inhibitors like paroxetine and fluoxetine.
§ Warfarin ( metabolized by CYP2C9).
Aromatase Inhibitors Vs. Tamoxifen
Aromatase Inhibitors | Tamoxifen |
Increased cholesterol | Improved cholesterol and bone strength |
Decreased bone density | Vaginal dryness and bleeding |
Tendonopathies | Risk of GU cancer |
Ischemic cardiovascular events | thromboembolism |
What is the dose for fulvestrant?
§ 500 mg IM split into 2 doses ( one in each buttock) on Days 1, 15, and 29, then once monthly thereafter.
§ If a person has hepatitic impairment than you give them ½ the dose.
What is required in premenopausal women if they are taking fulvestrant?
§ It requires ovarian ablation/suppression in premenopausal women with LHRH/GnRH agonist.
What are the side effects of Fulvestrant?
§ Risk of bleeding
§ Injection site reactions
§ Hot flashes
§ Bone pain
§ Arthralgias
§ Musculoskeletal pain
§ Asthenia
§ Fatigue
§ Headache
What are the treatment for HR+ metastatic breast cancers?
-CDK4/6 inhibitors
What is the MOA of CDK4/6 inhibitors?
-inhibition of CDK4 and 6 reduces proliferation of breast cancer cells by halting progression from G1 to S phase.
CDK4/6 Inhibitor:
| Pabociclib | Ribociclib | Abemaciclib |
Starting dose | 125 mg daily 3 weeks on, 1 week off | 600 mg daily 3 weeks on, 1 week off | 150 mg bid , Monotherapy: 200 bid |
CDK4/6 affinities | CDK6>4 | CDK6>4 | CDK4>6 |
Metabolism | Primarily Via CYP3A4 | Primarily via CYP3A4 | Primarily via CYP3A4 |
Hepatic dosing | Child-Pugh Class C: reduce to 75 mg daily | Child-Pugh class B/C: reduced to 400 mg daily | Child-Pugh C: reduce to daily dosing |
Drug interactions | Strong CYP3A4 inhibitors: reduce to 75 mg daily | Strong CYP3A4 inhibitor: reduce to 400 mg daily | Strong CYP3A4 inhibitor: reduce to 100 mg bid daily. |
Dose limiting toxicity | Neutropenia | Neutropenia QTC prolongation | Diarrhea |
Dose reduce | Dose reduce for hepatic dysfunction and certain rug interactions; hold /dose reduce for neutropenia | ||
What CDK4/6 inhibitor has good blood brain barrier ( BBB) penetration?
§ Abemaciclib
What are the medications treatments from HER2+ Breast Cancer?
o Pertuzumab and Trastuzumab
Why do you give pertuzumab and trastuzumab together in HER2+ Breast Cancer?
§ It allows for more complete blockade of HER2 in curative intent.
What are the treatment of HER2+ metastatic breast cancer?
o Fam-trastuzumab deruxtecan :
§ Tumor antigen: HER2
§ Topoisomerase I inhibitor ( deruxtecan).
What are the side effects of fam-trastuzumab deruxtecan?
· Diarrhea
· Myelosuppression ( comes from the topoisomerase inhibitor)
· Cardiotoxicity ( comes from HER2)
· Hypersensitivity reactions ( comes from monoclonal antibodies).
What is the dosing for fam-trastuzumab deruxtecan?
· 5.4 mg/kg IV Q21D.
Sacituzumab govitecan:
§ Tumor antigen: Trop-2
§ Topoisomerase I inhibitor
What is the adverse effects of Sacituzumab govitecan?
· Diarrhea
· Myelosuppression ( from topoisomerase inhibitor)
· Hypersensitivity reactions ( monoclonal antibodies.
How do you manage adverse effects of antiandrogens in breast cancer?
· Hot flashes/Night Sweats:
o Non-pharmacologic management
o Do not treat with estrogen containing products.
o Watch for DDI with fluoxetine/paroxetine with tamoxifen which are often prescribed for hot flashes/night sweats:
§ Use venlafaxine instead.
· Vaginal discharge/dryness:
o Do not treat with estrogen containing products if possible.
o Dryness: OTC products
o Baseline GYN exam
· Decreased bone density:
o Baseline DEXA scan and annually thereafter
o Co-prescribe calcium 1,200 mg daily and vitamin D 1,000 IU daily.
· Teratogenic:
o Use contraception in premenopausal women.
· VTE:
o Counsel on signs and symptoms and when to report to ED.
What are the risk factors for a patient that can increase their risk of getting prostate cancer?
· Age:
o Rare in those < 40 yrs. old.
o Increases with age.
· Race/Ethnicity:
o Scandinavian countries and the US have the highest reported incidence.
o African Americans have the highest rate of prostate cancer:
§ Testosterone is 15% higher in African Americans than compared to Caucasians.
· Family history of prostate cancer:
o Men with a brother or father with prostate cancer have 2 times the risk.
What is the pathophysiology of Prostate Cancer?
o The size of the prostate can increase with age.
o Prostate cancer begins when the cells in the prostate start to grow uncontrollably.
o More than 95% of primary prostate cancers are adenocarcinomas.
What symptoms are seen at the onset of prostate cancer?
§ Urinary hesitation
§ Urinary retention
§ Painful urination
§ Hematuria
§ Erectile dysfunction
When are most prostate cancers identified?
§ Most are identified prior to the development of symptoms.
What are the symptoms seen in localized prostate cancer?
§ No symptoms
What are the signs and symptoms of locally invasive prostate cancer?
§ Ureteral dysfunction
§ Frequency
§ Hesitancy
§ Dribbling
§ Impotence
What are the signs and symptoms of advance prostate cancer?
§ Back pain
§ Cord compression
§ Lower extremity edema
§ Pathologic fractures
§ Anemia
§ Weight loss
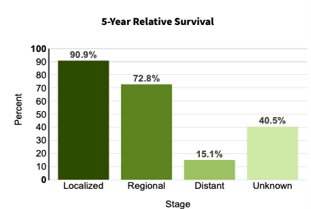
What is the prognosis for patients diagnosed with prostate cancer?
Non Metastatic vs. Metastatic Prostate Cancer Treatment Plan
| Castrate-sensitive ( decrease in PSA) | Castrate -resistant ( increase in PSA) |
Non-metastatic | Monitoring (preferred) or ADT
| Continue ADT; Start category 1 preferred: • Apalutamide • Enzalutamide • Darolutamide
|
Metastatic | ADT + one of the following Category 1 Preferred regimens: • Apalutamide • Enzalutamide • Abiraterone +/- docetaxel 75 mg/m2 x 6 • Darolutamide + docetaxel 75 mg/m2 x 6 **Docetaxel is used if symptomatic
| • Continue ADT • ADD denosumab (category 1, preferred) if bone metastasis • Palliative XRT for painful bone metastasis • Systemic anticancer therapy
|
What is the goal of androgen deprivation therapy?
§ Induce castrate levels of testosterone.
§ Serum testosterone < 50 ng/dL after 1 month of therapy
What are some options for androgen deprivation therapy?
· Surgical castration (remove testes)
· Medical castration: Luteinizing hormone releasing hormone agonist/antagonist.
True/False: Never stop giving ADT even in the setting of progression
-True
What medications used for ADT therapy are GnRH antagonist?
§ Degarelix
§ Relugolix
What medications used for ADT therapy are LHRH agonist?
§ Goserelin
§ Leuprolide
§ Triptorelin
§ Histrein
How long does it take GnRh antagonist to reach castrate levels?
-7 days
How long does it take LHRH agonist to reach castrate levels?
-28 days
This medication combination contains a CYP17 inhibitor and a steroid and is considered a biosynthesis inhibitor:
-abiraterone + prednisone
What are some side effects of abiraterone + prednisone?
hypertension, adrenal insufficiency , electrolytes ( prednisone/hydrocortisone).
What is the most common 1st generation non-steroidal antiandrogen?
· Bicalutamide : glucose intolerance
What are the common 2nd generation non-steroidal antiandrogens?
· Enzalutamide: seizures
· Apalutamide: seizures
· Darolutamide:
What are the side effects of non-steroidal antiandrogens and how do you manage those side effects?
· Edema/fluid retention: check electrolytes, wear compression stockings, check adrenal function.
· Hepatotoxicity: monitor LFTs
· Fatigue: exercise, diet, CBT, stimulants
· Nonsteroidal: HTN
· Steroidal: VTE/thrombosis
After how many years do most patients with advance cancer stop responding to ADT?
o Within 2-4 years.
How do you monitor adverse effects associated with prostate cancer?
· Bone mineral density baseline and every 6 mo.
· Serum testosterone and PSA at each clinic visit
· HgbA1C every 3 mo.
· Baseline lipids and biometrics for risk assessment; reevaluate periodically; self-monitor BP, PCP checkups.
What are some acute events associated with prostate cancer?
· Tumor flare with agonists, combine with an antiandrogen.
· Gynecomastia
· Hot flashes: increase dietary intake of soy.
· Erectile dysfunction: consider tadalafil, sildenafil.
· Injection site reaction
What are some long term effects that can happen in prostate cancer?
· Osteoporosis fracture: baseline and periodic DEXA scan; calcium+D and denosumab indicated for prevention.
· Depression: CBT, figure out cause if organic/reversible, psych consult
· Increased CVD risk and hyperlipidemia: monitor and treat according to guidelines.
· Hyperglycemia, insulin resistance, DM: monitor and treat according to guidelines.
What is the tumor flare seen with LHRH agonists used in prostate cancer?
-surge in testosterone that can flare the symptoms of the metastatic deposit
-seen in the first 1-2 weeks.
What cause a tumor flare?
-it is caused by initial induction of LH and FSH
What are some signs/symptoms of a tumor flare?
-increased bone pain
-spinal cord compression
-obstructive bladder
How do you prevent tumor flare?
-begin antiandrogen therapy 7 days prior to starting LHRH agonist to help prevent tumor flare.
How can you detect the progression of prostate cancer?
o Increased PSA/ the rate of PSA increasing.
o Evidence of more disease on imaging scans.
o New or more severe symptoms.
In addition to checking for increasing PSA what else, should be checked to indicate progression of the prostate cancer?
o Scans and clinical symptoms should be checked as well.
Why should LHRH agonist or antagonist be maintained throughout therapy?
o Patient must maintain castrate levels of testosterone even after recurrence.
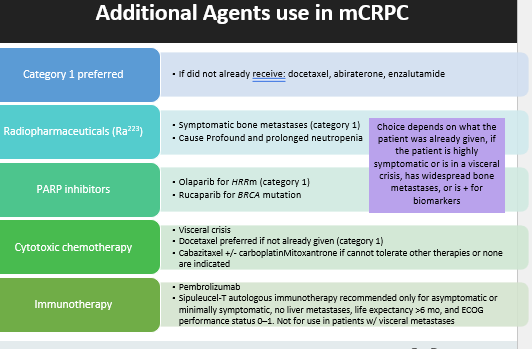
What are some additional medications that are used in metastatic prostatic cancer?
What are the risk factors of colon cancer?
· Hereditary factors:
o Hereditary colorectal cancer syndromes
o positive family history.
· Modifiable risk factors:
o Smoking
o Moderate/heavy alcohol consumption
o Poor diet
o Obesity/low physical activity
· Age
What are some symptoms seen with colon cancer?
o Change in bowel habits or rectal bleeding
o Constipation (depending on location of tumor)
o N/V and abdominal discomfort
o Fatigue (if severe anemia)
What can be signs of colon cancer?
o Positive guaiac stool test and anemia from blood loss
o Elevated CEA (more likely with high stages)
o Altered LFTs with metastatic disease (high T-bili, low albumin, high AST/ALT)
What is the prognosis for patients with Colon Cancer?
What is the pathophysiology of colon and rectum?
· Involves the colon and rectum
· Typically arises from a polyp
· Adenocarcinoma accounts for 92% of tumors
True/False: Right sided colon cancer has a worst prognosis, higher likelihood of MSI-H, BRAF, and RAS mutations
-True
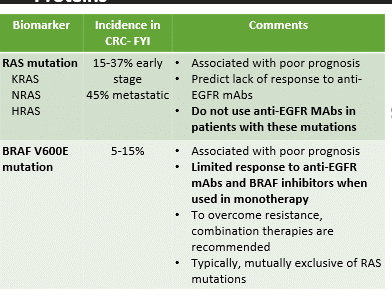
What are some biomarkers in Colon Cancer?
What is the treatment plan for early stage colon cancer?
Stage | Treatment | Goal of Treatment |
Stage I | Surgical resection followed by surveillance | Curative |
Stage II | *Surgical resection +/- 5-FU-based chemotherapy depending on presence of high-risk features | Curative |
Stage III | *Surgical resection followed by adjuvant 5-FU based therapy | Curative |
What are some common drug regimens used to treat colon cancer?
· Fluorouracil (5-FU):
o Administered as a Bolus
o Can be administered as a continuous infusion due to short half-life of drug.
· Leucovorin
· Capecitabine:
o 150 mg and 500 mg tablets.
o Administered orally in two divided doses.
o Swallow whole with water within 30 minutes of a meal.
o Round to nearest pill size to ensure total daily dose is within 10% of target.
· CapOX
· FOLFOX
· FOLFIRI
· FOLFIRINOX
· Panitumumab
· Cetuximab
What patients cannot take 5- fluorouracil?
§ If a patient has a known dihydropyridine dehydrogenase ( DPD) deficiency: it is not routinely tested.
What is the use of Uridine Triacetate (Vistogard)?
o It is used for the emergency treatment for 5-FU or capecitabine:
§ Overdose
§ Patient who exhibit:
· Early onset, sever, or life-threatening toxicity affecting CNS or early onset unusually severe adverse reactions within 96 hours following 5-FU/capecitabine overexposure.
§ 10 grams po q6h x20 doses without regards to meals.
§ Can only obtain from one pharmacy.
If a patient has CrCl 30-50 mL/min, how do you reduce the dose of capecitabine?
-reduce the dose by 75% of usual dose.
If a patient has a CrCl <30 mL/min , how do you reduce the dose of oxaliplatin?
o Reduce initial dose by 25%
How do you manage HFS in Colon Cancer Patients?
· Prevention:
o Avoid friction/heat exposure.
o OTC moisturizer BID
· Call doctor:
o At first sign of burning or tenderness.
· Treatment:
o Urea 40% cream apply to hands/feet twice daily
o May need to hold and/or dose reduce offending agent:
§ Dependent on grade
o