paediatric optometry - lecture 6 paediatric development
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
What ocular conditions might be attributed to complications in paediatric development?
- retinopathy
- myopia
- tropia
- amblyopia
What are the 3 phases of growth and development?
- psychomotor: including physical and sensory perceptual
- Cognitive: including language
- Affective: including emotional, social, personality and moral
What are the goals of child health supervision?
•Growth
•Language
•Assessment tools
•Nutrition
•Dentition
•Feet and walking
•Hearing screening
•lowered child mortality
•reduced disability and morbidity
•promotion of optimum growth and development
•help for children to achieve longer, fuller, more productive lives, i.e., maximise their potential
How are the goals of child health supervision achieved by?
•measurement and recording of physical growth
•monitoring of developmental progress
•administration of screening tests
•offering and arranging intervention when required
•prevention of disease by immunisation
•information and support to parents
•health education
Define 'growth' and 'development'?
growth - the increase in the number and size of cells
Development - the maturation of the organs and systems of the body and acquisition of skills
ways to determine growth
standard growth charts - compare a child with
• other children, note rate of growth; failure to
thrive;
• short stature; tall stature
What is normal/abnormal in a child in regards to feet and walking?
•Flat feet - normal in a toddler
•Toeing in - normal in young children (decreases with age)
•Toe walking - may be part of normal progression
•Bow-legged - normal in first 3 years (concern if excessive or family history)
•'Knock kneed' - normal ages 3-6 years, straight - ages 7-8 years and beyond
•Limps - foot, knee or hip: concern if accompanied by fever
When can majority of hearing impaired children be recognised?
- ages of 3 to 7 years.
Delay or failure to identify can lead to problems in speech, language, academic, intellectual and social development of children
hearing impairment stats
• new-borns: 1 in 1000 have a serious hearing impairment
• children 5-19: 3 in 4000 totally deaf, 1 in 200 hearing
impaired
• age 65+: 25-40% are hearing impaired
• age 90+ : 90% are hearing impaired
Hearing screenin
What is meant by receptive and expressive?
Receptive: listening. can they understand?
1 year old should follow 1 step command
expressive: verbalising.
2 years 2 word sentences
• 3 years 3 word sentences
Language
When does a baby get their first teeth?
5 to 9 months
first dental visit at age 3
- children lose baby teeth at around 5 - 6 years
- important for fluoride use
What does the denver developmental screening test assess?
•Gross motor
•Language
•Fine motor-adaptive
•Personal-social
Describe the information for a newborn to birth baby?
•Sleeps for much of the 24 hours
•Baby yawns, coughs, hiccoughs, sneezes, stretches and salivates.
•Baby can suck, swallow, smell, taste, hear and see.
•Shows a variety of primitive reflexes, e.g.
•Moro reflex, Grasp reflex, Walking reflex
•Cardinal points: a variety of mouth and lip reflexes
•"rooting reflex" - searching for mother's milk
•Blink reflexes - various stimuli provoke blinking
What is the moro reflex?
•Moro reflex: seen when the baby is suddenly moved. It consists of rapid abduction and extension of the arms with opening of the hands. The arms then come together as in an embrace.
- gives an indication of muscle tone
- usually disappears within 2 to 3 months
What is the grasp reflex?
•Grasp reflex when baby's palm is stimulated, the hand closes.
•Baby's grasp at this stage is strong and could support its weight.
•However, the strength disappears overnight, although the reflex itself persists for up to 2-3 months.
What is the walking reflex?
Walking reflex: when the sole of the foot is pressed on the floor the baby walks.
Disappears after 3-4 weeks
What are the different aspects in child skill aquisition?
•Gross motor
•Fine motor
•Adaptive
•Language
Personal-social (affective)
What is the skill acquisition of a 4 week old?
Gross motor: head flops forwards when sat up
Fine motor: hands clench on contact
Adaptive: looks at object in line of sight
What is the skill acquisition of a 16 week old?
Gross motor: head steady on sitting. Lifts head when prone on forearms
Fine motor: hands clutch, scratches
Adaptive: slow pursuits, hypometric saccades, holds and looks, oral
Language: laughs, excited noises
Personal/social: social smiles, recognises food
What is the skill acquisition of a 28 week old?
Gross motor: sits briefly, with help from hands
Fine motor: radial palmar grasp
Adaptuve: one handed approach and grasp. Bangs and shakes
Language: vocalises when crying. Baby babble
Personal/ social: feet in mouth, reaches for mirror image
What is the skill acquisition of a 40 week old?
Gross motor: sits steady, pulls to feet
Fine motor: thumb and index grip
Language: mama, dada and possibly one or two other words
Personal/ social: wave bye bye, simple self feeding, games
What is the skill acquisition of a 12 month old?
Gross motor: crawls, stands alone momentarily
Fine motor: Neat pincer grasp
Adaptive: serial play; 2 block tower
Language: gives on request, 1 or 2 more words
Personal/social: cooperates in care
What is the skill acquisition of a 15 month old?
gross motor: toddles independently, stands alone for short periods
Fine motor: puts small object in bottle
Adaptive: looks at objects in line of sight
Language: few more words. Pats picture
Personal/social: thanks, shows wants
What is the skill acquisition of an 18 month old?
gross motor: walks, seats self in chair, throws when standing
Fine motor: turns pages
Adaptive: 4 tower block, scribbling
Language: 10 words. identifies picture, 2 direction commands
Personal/social: pulls toy, carries doll, helps feed
What is the skill acquisition of a 2 year old?
Gross motor: runs, climbs stairs, kicks large ball
Adaptive: 7 blocks, copies hand movements
Language: pronouns, 3 word sentences, 4 direction commands
Personal/Social: toilet trained
What is the skill acquisition of a 3 year old?
Gross motor: jumps off step, pedals trike
Fine motor: holds crayon in fingers
Adaptive: 10 blocks, simple bridge, copies simple drawings
Language: uses plurals, verbs, understands prepositions
Personal/social: feeds well, dresses, sings
What is the skill acquisition of a 4 year old?
Gross motor: alternating foot descent
Fine motor: Draws 2 part people, copies cross
Adaptive: counts 3 objects with correct pointing
Language: names colours
Personal/ social: self hygiene, runs errands
What is the skill acquisition of a 5 year old?
Gross motor: skips, stands on one leg for more than 3 seconds
Adaptive: counts 10 objects, copies triangle, unmistakable people
Language: Knows red/ green/ bluee; describes pictures
Personal/ social: asks meaning of words, starts to write letters
What is the skill acquisition of a 6 year old?
Gross motor: Stands on either foot with eyes closed
Fine motor: 3 step structures with blocks
Adaptive: copies diamond
Personal: ties shoelaces, knows L and R. am and pm. counts the 30
Why examine children?
•Visual sensory deprivation in the early years of life can lead to irreversible loss of visual function
•The early detection, diagnosis and treatment of vision problems is critical to success
who to examine paediatric
All children?
- May need specialised expertise?
- May need specialised equipment for full diagnosis?
- May require more specialised techniques for proper evaluation of visual
function in infants (e.g., VEP, preferential looking techniques, ERG)
• Preschool children ( 3 to 5 years of age)
• School aged children and beyond
what factors affect ability to conduct eye test on child
- developmental status
- cognitive ability
- attention span
- effect of the consulting room environment
- rapport with you
What are the different problems a child can have which may affect the examination?
•Developmental problems
•Strabismus and amblyopia
•Motor development
•Learning problems
Paediatric diseases
children vs adults
• Children are not just small adults
• Children can have different problems
• Children present differently
• Age is an important factor in the paediatric
examination
child presenting with issues in practice
Frequently presented by parents or other relatives
• Difficulty in child knowing if they have a problem
• Children's vocabulary and experiences are different
• Child's views may not coincide with parents
• Child may not want to be there
how to adjust the paediatric practice to adress concerns well
Provide a child-orientated environment
• Spend time building rapport with child
- but don't neglect the parents
• Structure the exam to suit the child?
- When they are alert?
• Can be especially important with babies
- Often see children after school (when they are tired)
What are some common complaints from parents about their child?
-eye turns when tired
-sits too close to the TV
-blinks a lot
-rubs eyes a lot
school difficulties
Which other relevant infomation would you need besides main concern ?
•Explore complaint
•Child's neonatal history
•Development
- milestones and abilities
•Family history
What neonatal history do you need to gather?
•Neonatal: Normal birth? Caesarean? Trauma?
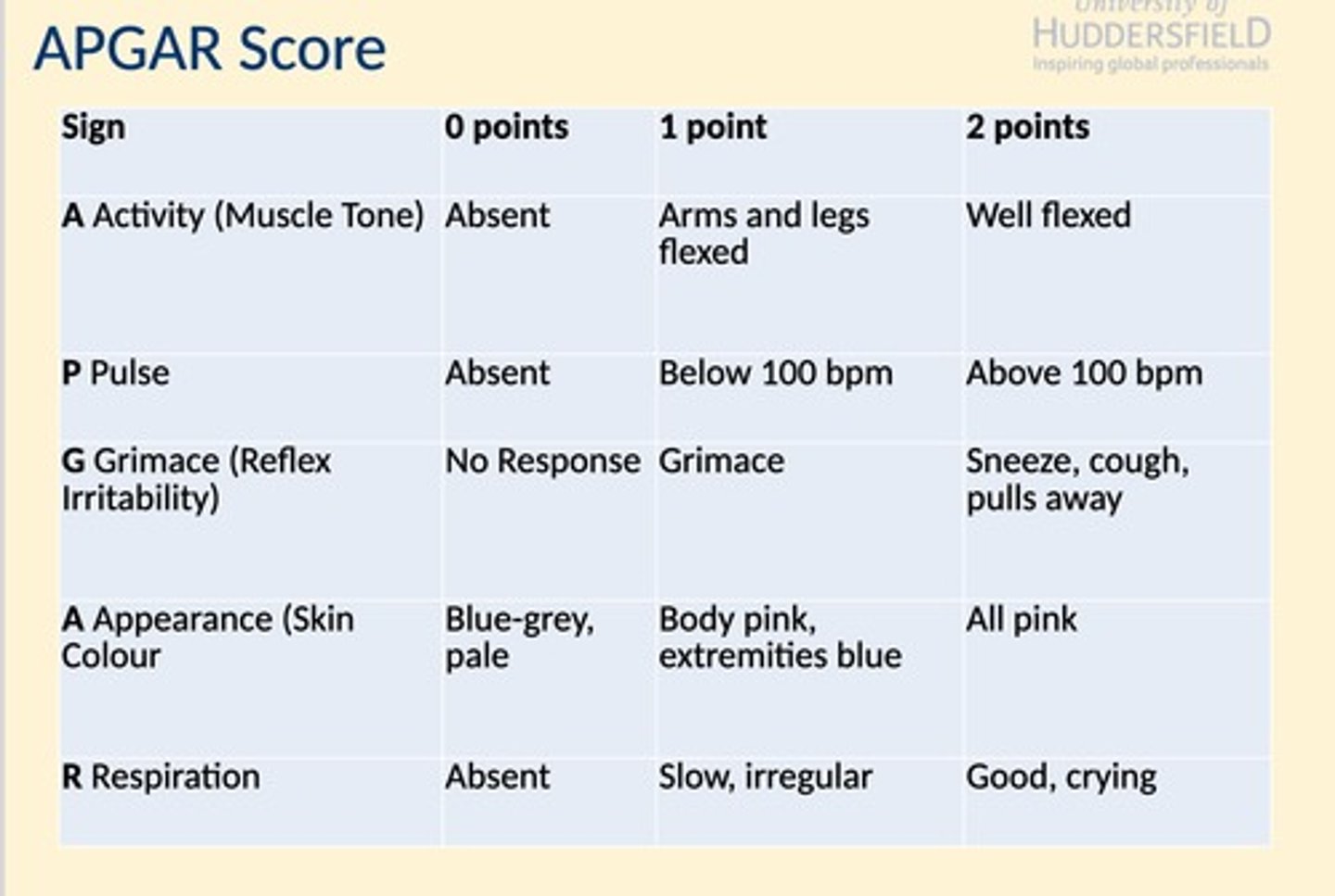
•APGAR Score: Assessed 1 minute after birth, better later
-Score 8 or over is good
-Score of 4 signals a weak baby with possible problems later
What are the risk factors for development of refractive erroe?
Prematurity and low birth weight infants
Increased prevalence of myopia and astigmatism
Maternal disease
Diabetes
Fetal alcohol syndrome
Rubella
Genetic predisposition
40% chance of myopia when both parents myopic
apgar chart point system
step 2 - forming hypothesis
What are the most likely causes of the complaint?
• Are any of these the province of the optometrist?
• If yes, what tests will tend to confirm or deny the
hypotheses?
• If no, counsel and refer.
epidemiology of ocular disorders
Refractive error
• Amblyopia
• Strabismus
• Ocular disease
• Other conditions
- Colour vision problems
- Visual perceptual problems
- Reading difficulties associated with vision
refractive error in children
Significant refractive error is the most common cause of decreased
vision in children (and adults)
• Infants are generally born hypermetropic (+2.00D ± 2.7). The
refractive error reduces (emmetropisation) over the first 18 months
of life to emmetropia. The variance in the refractive error
distribution also reduces
mechanism of emmetropiasiton in children
is currently unknown.
There is some suggestion that the eye senses the sign and
magnitude of the refractive error and then adjusts its rate of growth
through an active feedback process to reduce the refractive error
refractive error distribution in children
The distribution of
refractive errors in infants
is relatively broad and
achieves the more typical
leptokurtic appearance
over the first 18 months
to 2 years
refractive error stats in children
• Over 80% of children 1-7 years are between +0.50 and +3.00 D
• Less than 5% of all 5-7-year-olds are over +5.00D
• Less than 3% are myopic
myopia prevelence in children
The prevalence of myopia increases with age after about 8 years
and may be as high as 15-30% (early onset myopia) at 15 (while
hypermetropia remains at around 6%)
astigmatism in infants
Reports vary but anywhere between 17-63% of infants have
astigmatism > 1.00DC (most report against the rule)
– Astigmatism appears to be transient, and the prevalence
decreases in the first year or two of life
amblyopia in children
Single most prevalent cause of vision
loss in children (and adults up to
about 45 years of age!)
• Prevalence of amblyopia estimated
at 2-3% in the general population
risk factors of amblyopia in children
Strabismus
• Anisometropia
• High refractive error
• Form deprivation - rare (e.g.
cataract)
strabismus prevalence in children
Prevalence less well
established but estimated
to be around 3-5%
(horizontal deviations)
• Prevalence for vertical
deviations not well known
but probably much less
ouclar disease in children
- However - MUST always be aware of the possibility of the
presence of underlying ocular pathology
- Especially important in the assessment of strabismus in
children
• Note that the cause of vision loss in children with some
ocular conditions may be amblyopia e.g., congenital
cataracts
other conditions of children that may affect vision
Non-strabismic binocular vision anomalies
– Convergence insufficiency
– Accommodative insufficiency
• Learning difficulties
– Association with vision?
• Colour vision defects
– Congenital defects - may have an impact on learning
• Developmental defects
– e.g., Down Syndrome, Cerebral Palsy
– Usually associated with significant visual defects
3 main causes of vision changes in children
- Refractive error
- Amblyopia
- Strabismus
What is sometimes not agreed is how/when to
treat the above
• however Ocular disease in children, when it occurs,
should be treated