Autonomic Nervous System (ANS) Clinical Correlations
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
Clinical Correlations
horner’s syndrome (sympathetic nervous system)
peripheral nerve lesions
spinal cord lesions
autonomic dysreflexia
This is just a partial list of ANS deficits
Horner’s Syndrome
if a lesion affects the sympathetic pathway to the head, sympathetic activity on one side of the head (ipsilateral side) is defective
can occur with lesions of the:
descending sympathetic fibers from the hypothalamus (central lesion: CNS)
upper thoracic spinal cord (T1-T4) (preganglionic lesion: spinal cord)
superior cervical ganglion (from cervical sympathetic chain) (postganglionic neuron cell body)
can also be the result from another injury, disorder (head injury, lung tumor, etc)
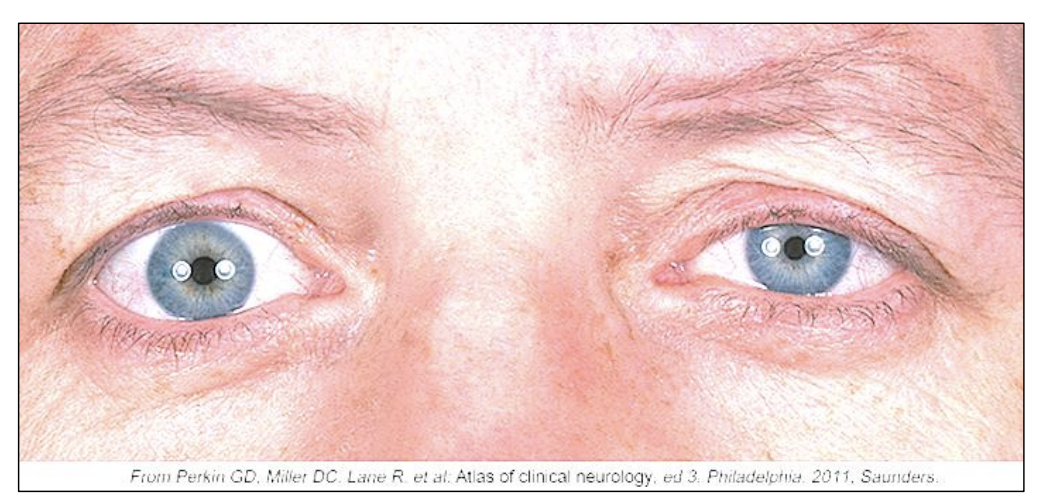
Horner’s Syndrome: Clinical Signs
Signs are on the same side (ipsilateral) as the lesion
ptosis: partial drooping of the eye lid (superior tarsal muscle)
miosis: pupillary constriction
anhidrosis (Hypohidrosis): lack (or decrease) of sweating
enophthalmos: eye appears to sink into the orbit
Peripheral Nerve Lesions
if peripheral nerve is severed, interruption of sympathetic efferents can cause loss or decrease of sympathetic functions in the areas supplied by that nerve or nerves
vascular control (sympathetic efferents control diameter of blood vessels)
temperature regulation
sweating
Spinal Cord Lesions
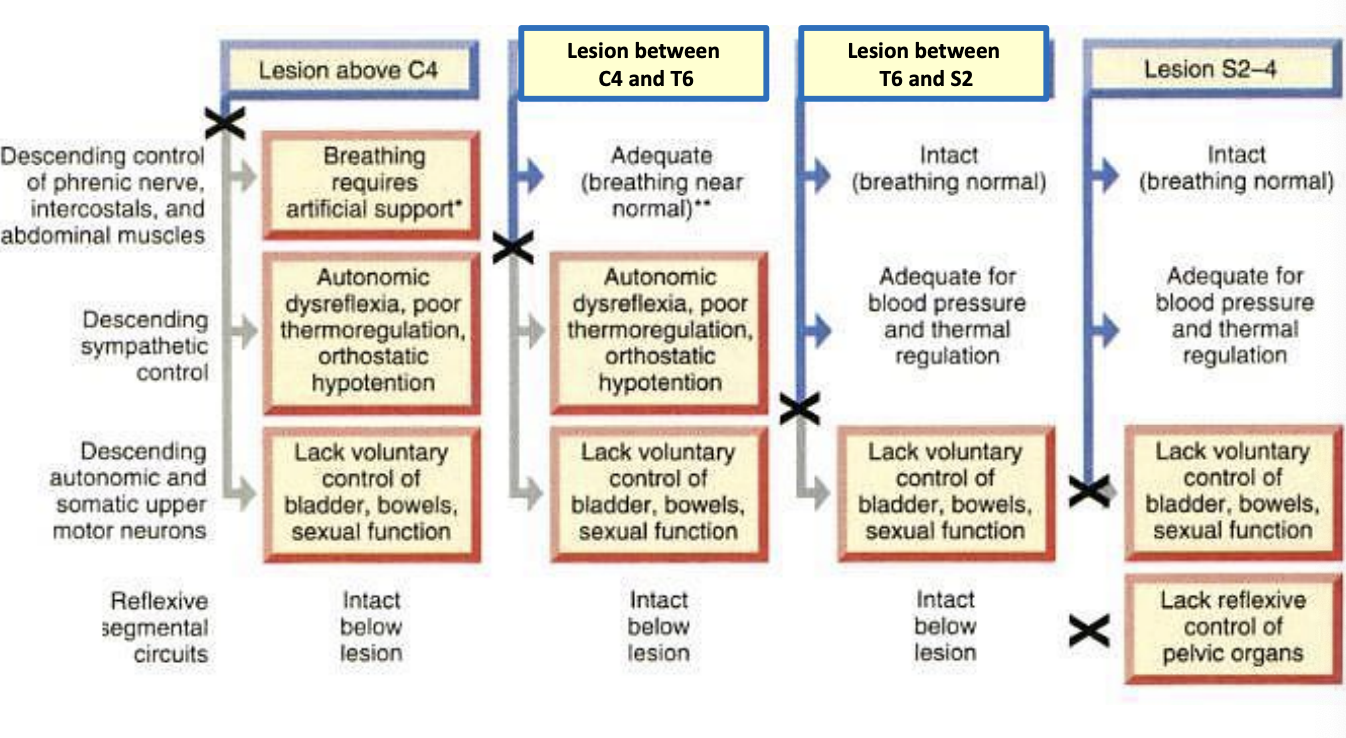
complete spinal cord lesion interrupts all communication between the brain and the spinal cord region located below the lesion
effects of spinal cord lesions on bladder, bowel, ad sexual functions depend on the location of the lesion along the levels (C, T, L, S) of the spinal cord
it could affect both sympathetic and parasympathetic innervation
it could just involve the sympathetic or parasympathetic innervation
sexual function is a significant issue for many following SCI
with SCI, the effects of spinal cord lesions on bowel control and sexual organ functions are similar to bladder function
so, as an example we will discuss bladder dysfunctions following a SCI
Types of bladder dysfunctions after spinal cord injury
lower motor neuron (LMN) bladder, aka:
flaccid bladder
atonic or hypotonic bladder
underactive bladder
Upper Motor Neuron (UMN) bladder, aka:
spastic neurogenic bladder
hyper-reflexive bladder
Levels of SCI for bladder dysfunctions
LMN bladder (flaccid bladder) due to complete lesion of:
Cauda Equina
spinal cord levels S2-S4 (located in the conus medullaris)
UMN Bladder (spastic bladder) due to complete lesion of:
spinal cord above S2 (above the conus medullaris)
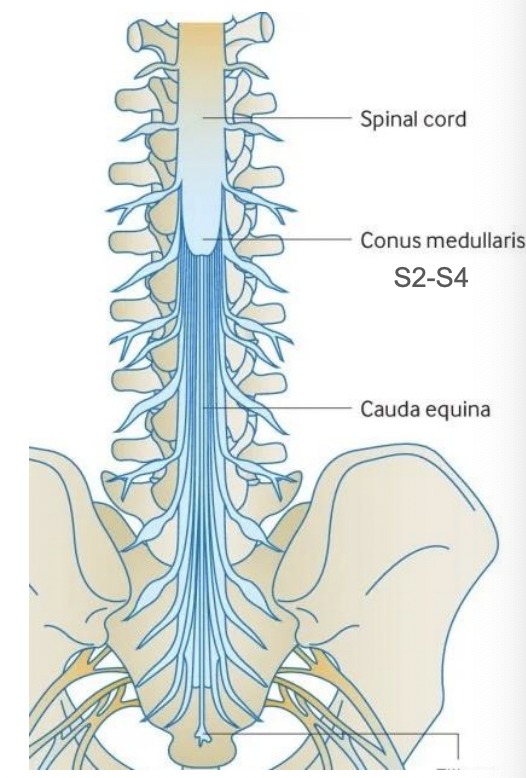
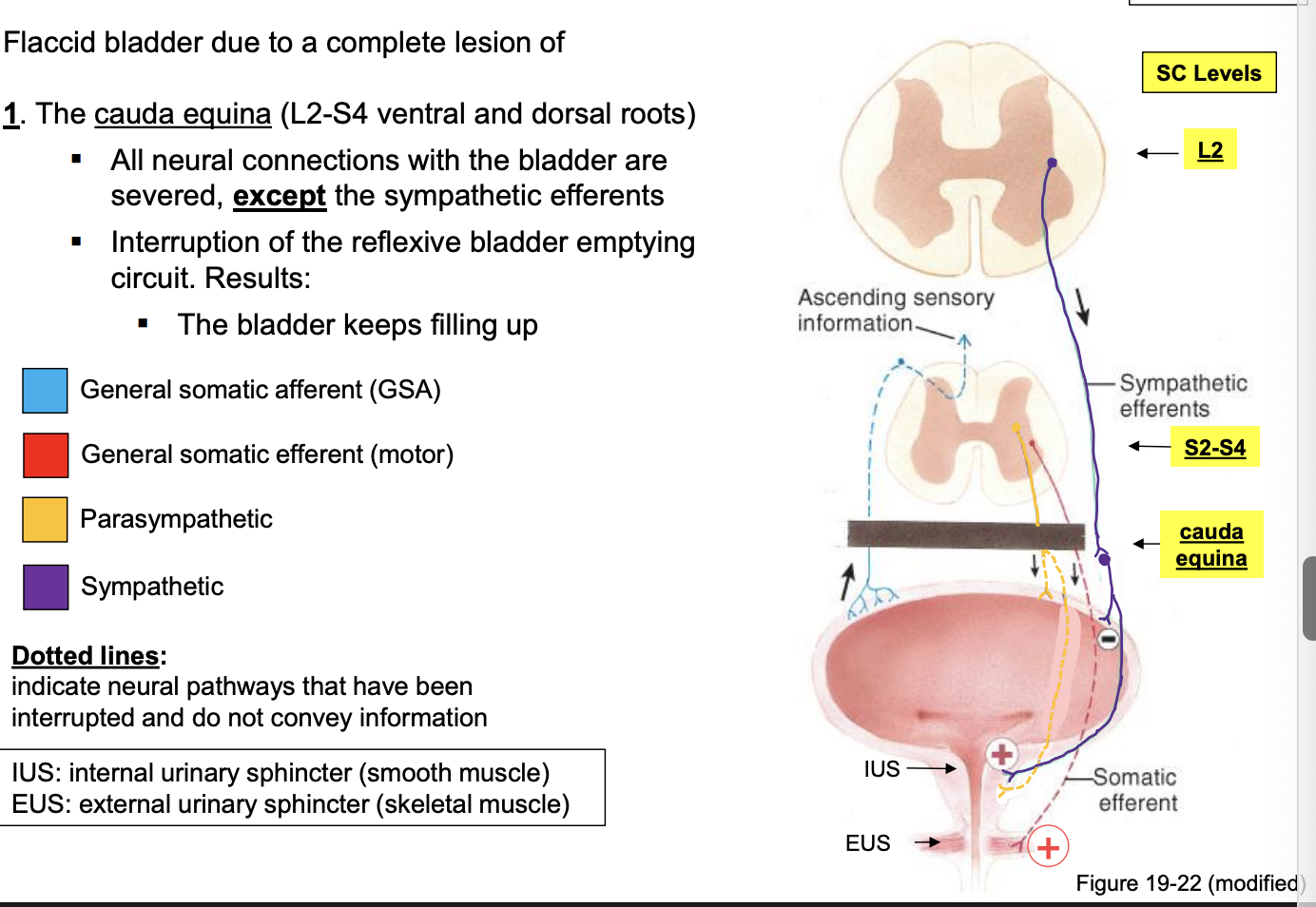
LMN bladder: cauda equina lesion
flaccid bladder due to a complete lesion of:
the cauda equina (L2-S4 ventral and dorsal roots)
all neural connections with the bladder are severed, except the sympathetic efferents
interruption of the reflexive bladder emptying circuit. Results:
the bladder keeps filling up
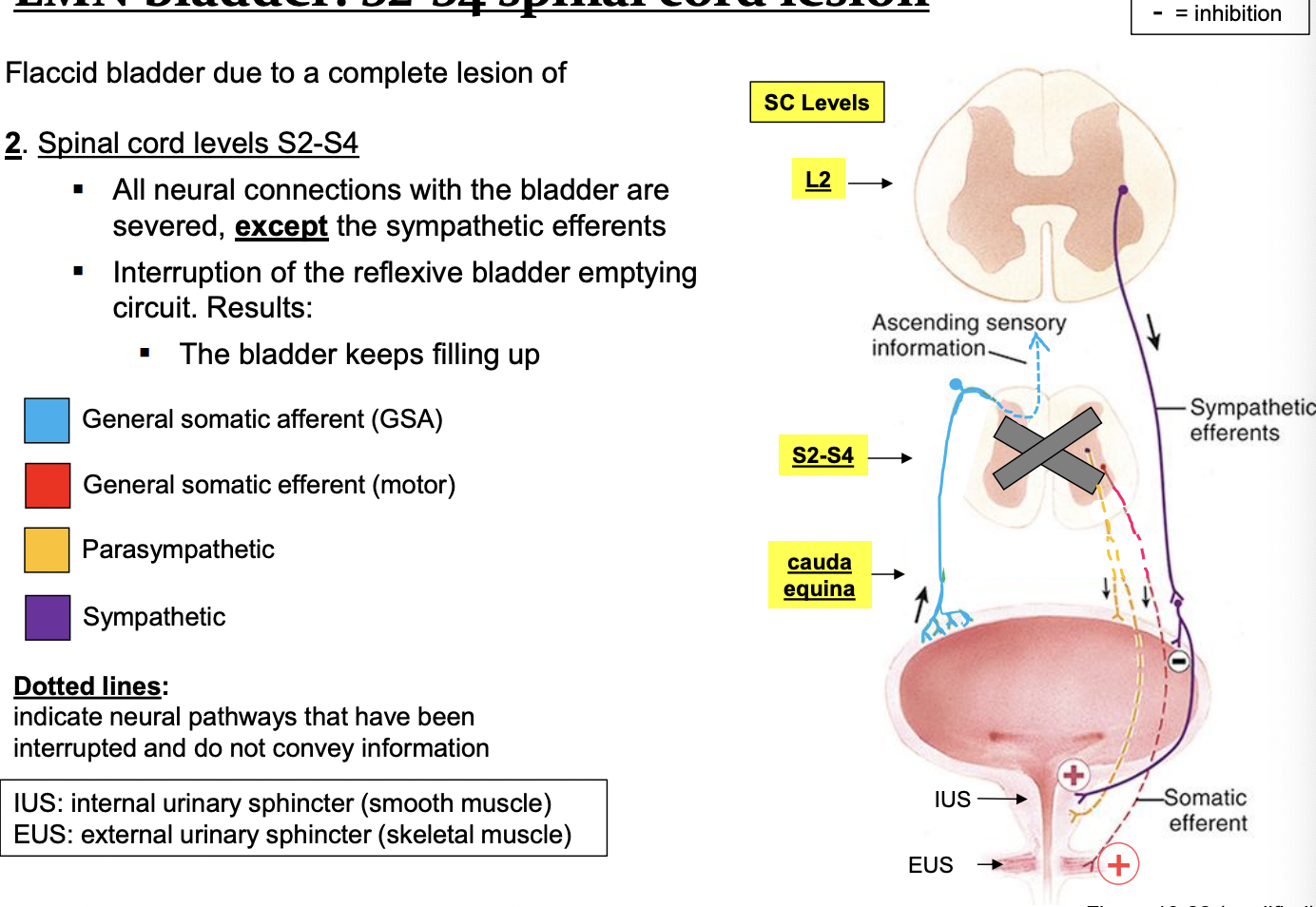
LMN bladder: S2-S4 spinal cord lesion
flaccid bladder due to a complete lesion of:
spinal cord levels S2-S4
all neural connections with the bladder are severed, except the sympathetic efferents
interruption of the reflexive bladder emptying circuit. Results:
the bladder keeps filling up
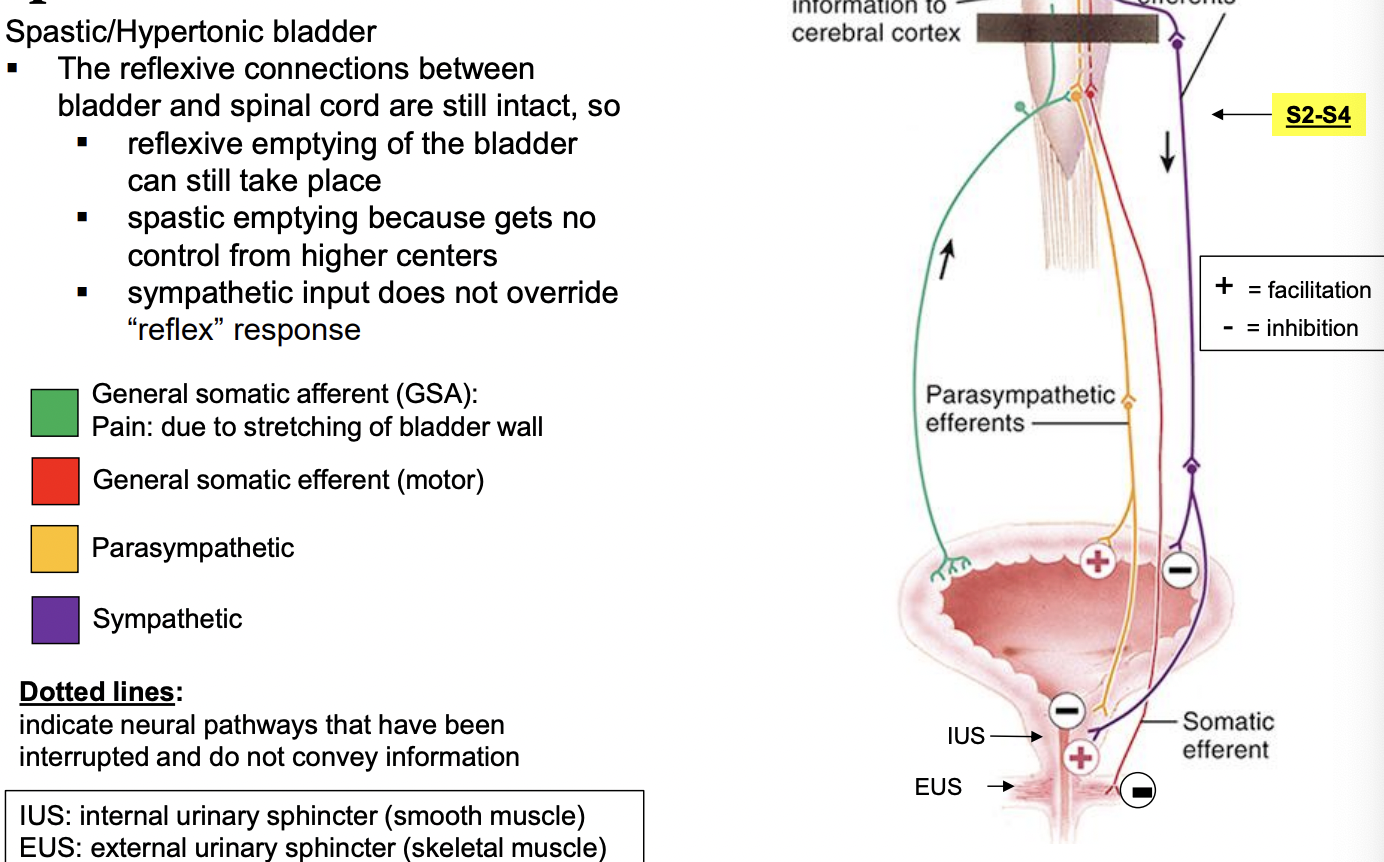
UMN bladder: Lesion above S2 spinal cord level
Spastic/Hypertonic bladder
the reflexive connective between bladder and spinal cord are sill intact, so
reflexive emptying of the bladder can still take place
spastic emptying because gets no control from higher centers
sympathetic input does not override “reflex” response
Autonomic Dysreflexia (hyperreflexia)
sudden over-active autonomic nervous system
potentially life threatening (medical emergency)
can result in stroke, heart attack, seizures, death
who is at risk for autonomic dysreflexia?
people with SC injury at T6 or above is most common cause
other factors:
brain injury, stroke, multiple sclerosis, Guillain-Barre syndrome, side effects of medication
triggers: irritation, noxious stimuli (painful or not)
bladder — over-distention, kink in a catheter, bladder spasms, infection
bowel — constipation, hemorrhoids, gas, diarrhea
skin — constrictive clothing (jeans, socks, shoes), bed sores, ingrown toenails, cuts, bruises
results in uncoordinated autonomic responses
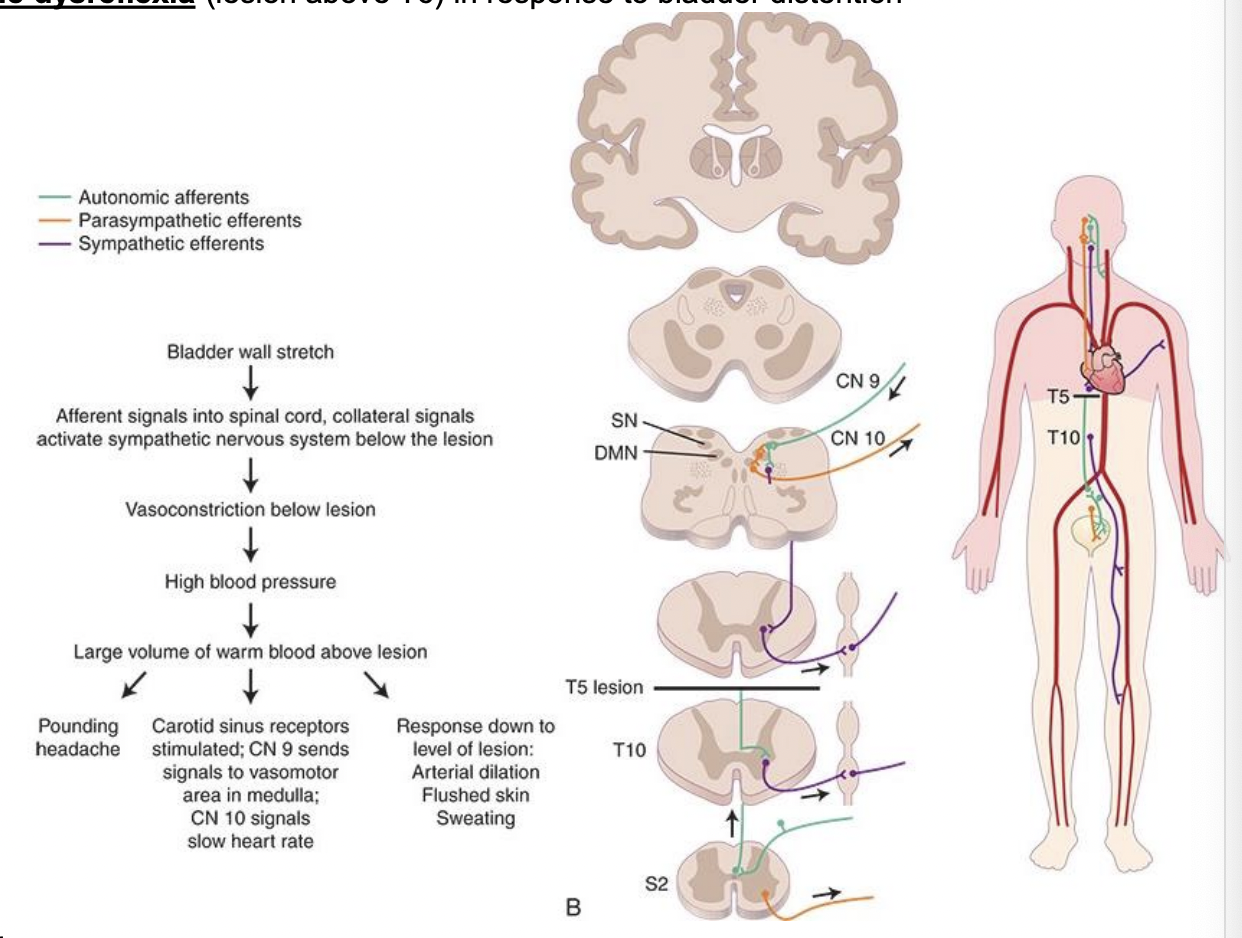
Autonomic Dysreflexia (hyperreflexia) cont’d
a noxious afferent stimulus (distended bladder, bed sore, etc) below SC lesion triggers excessive peripheral sympathetic response below lesion
results in: vasoconstriction to viscera and muscles below the level of the lesion
causes: abrupt increase in blood pressure
baroreceptors in blood vessels detect this hypertensive crisis and signal the brain via cranial nerves IX and X
descending inhibitory singals respond to counteract the rise in blood pressure with slowed heart rate and vasodilation
however, vasodilation is blocked at the level of the spinal cord injury and below
results:
uncoordinated autonomic control responses (high BP)
above lesion: flushed/warm skin (vasodilation), profuse sweating and pounding headache, reduced heart rate
below the lesion: vasoconstriction, cold/pale extremities, goose bumps
Autonomic Dysreflexia (hyperreflexia): Treatment
stroke can be an immediate life-threatening concern associated with this
treatment/management
first step:
sit the patient upright with their legs dangling
remove source of noxious stimulus (tight clothing, constrictive devices, ask about bladder or bowel issues)
this will help lower their blood pressure by inducing the pooling of blood in the abdominal and lower extremity vessels
if the source of noxious stimuli cannot be found, emergency medical services should be contacted
ANS dysfunctions at various levels of spinal cord injury