The process of labor and birth
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
The Five P’s
All forces must work together for a successful birth!
Powers (contractions)
Passenger (fetus)
Passageway (birth canal)
Position (position of birthing person)
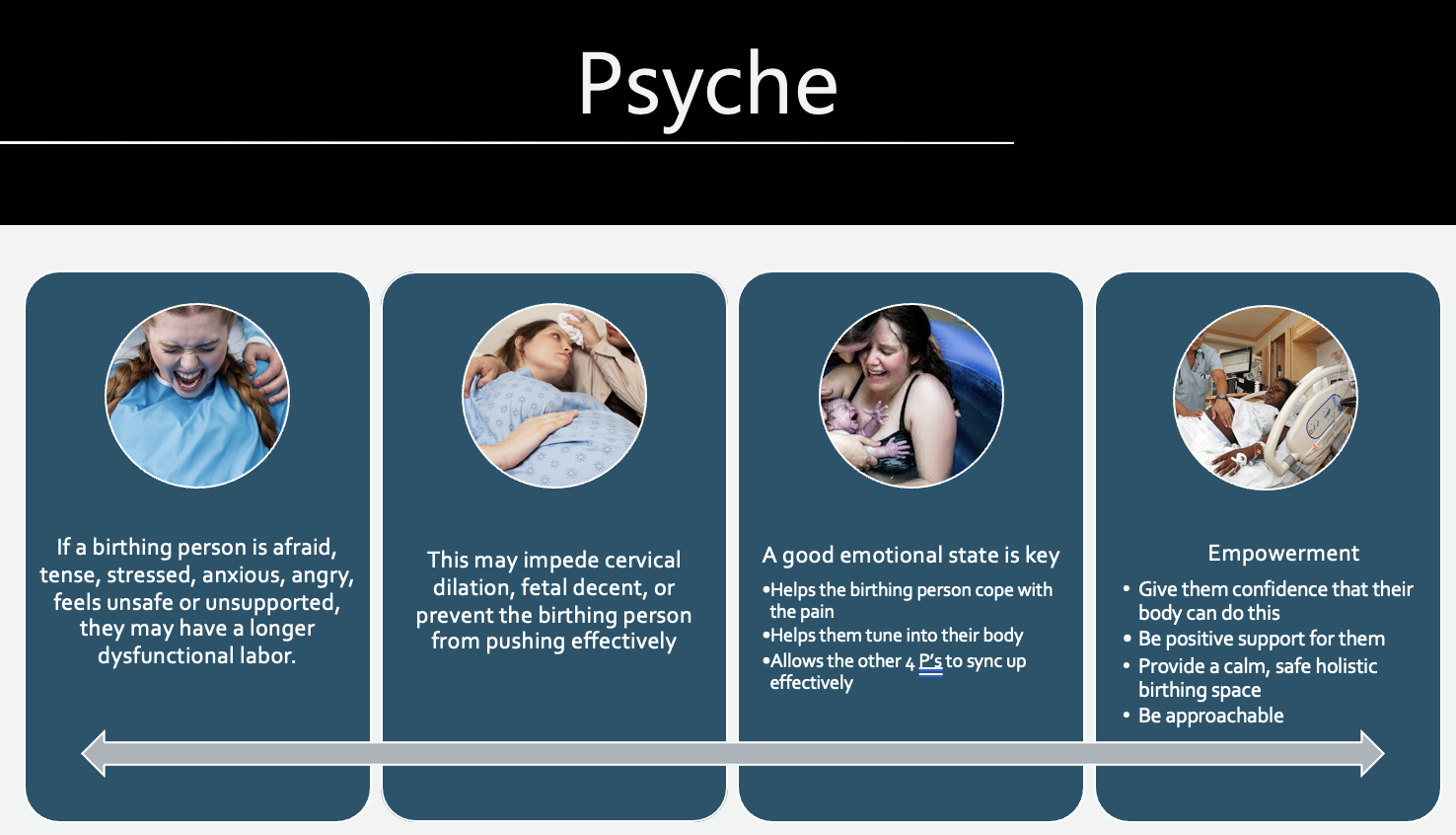
Psyche (psychological response)
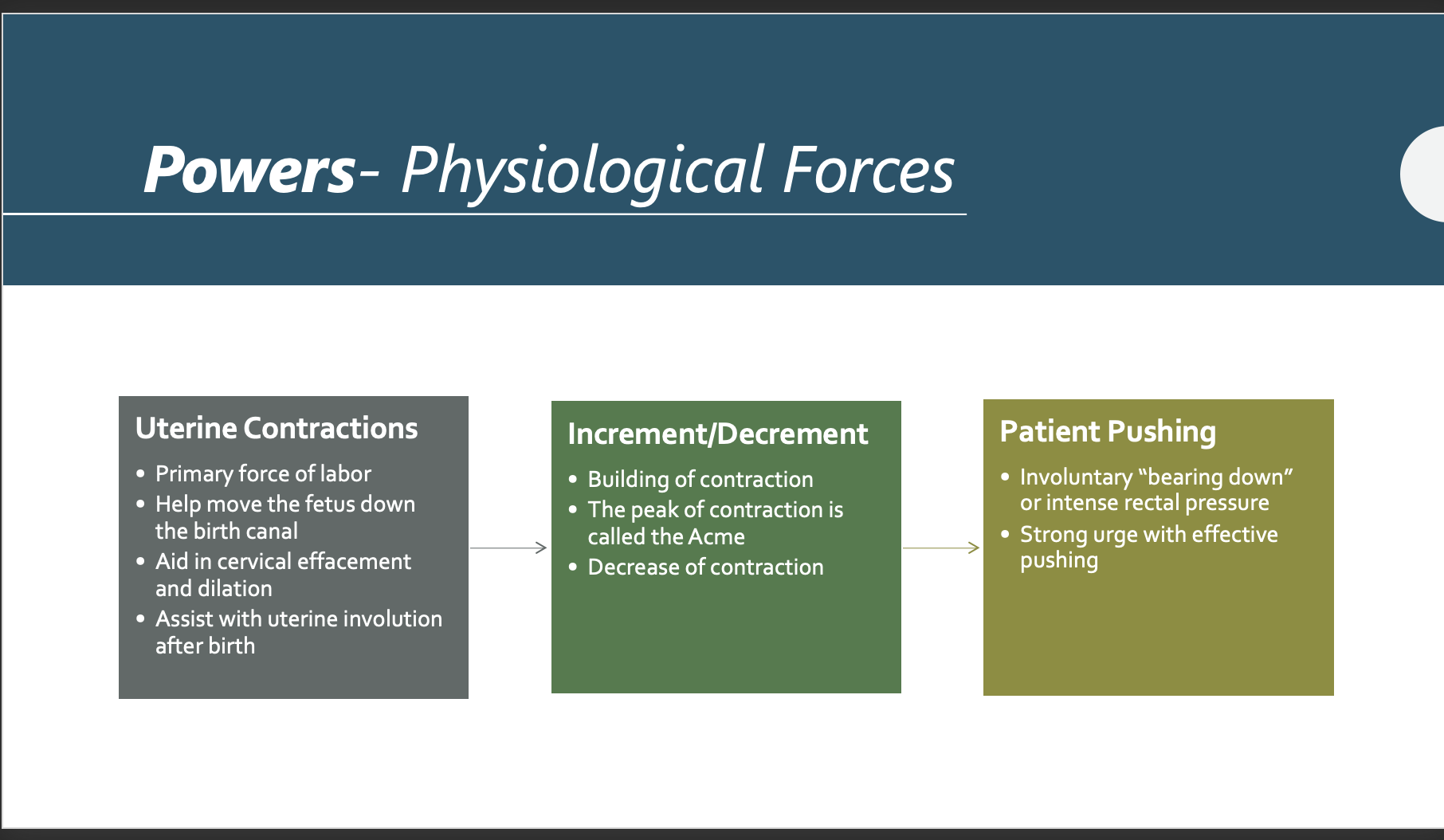
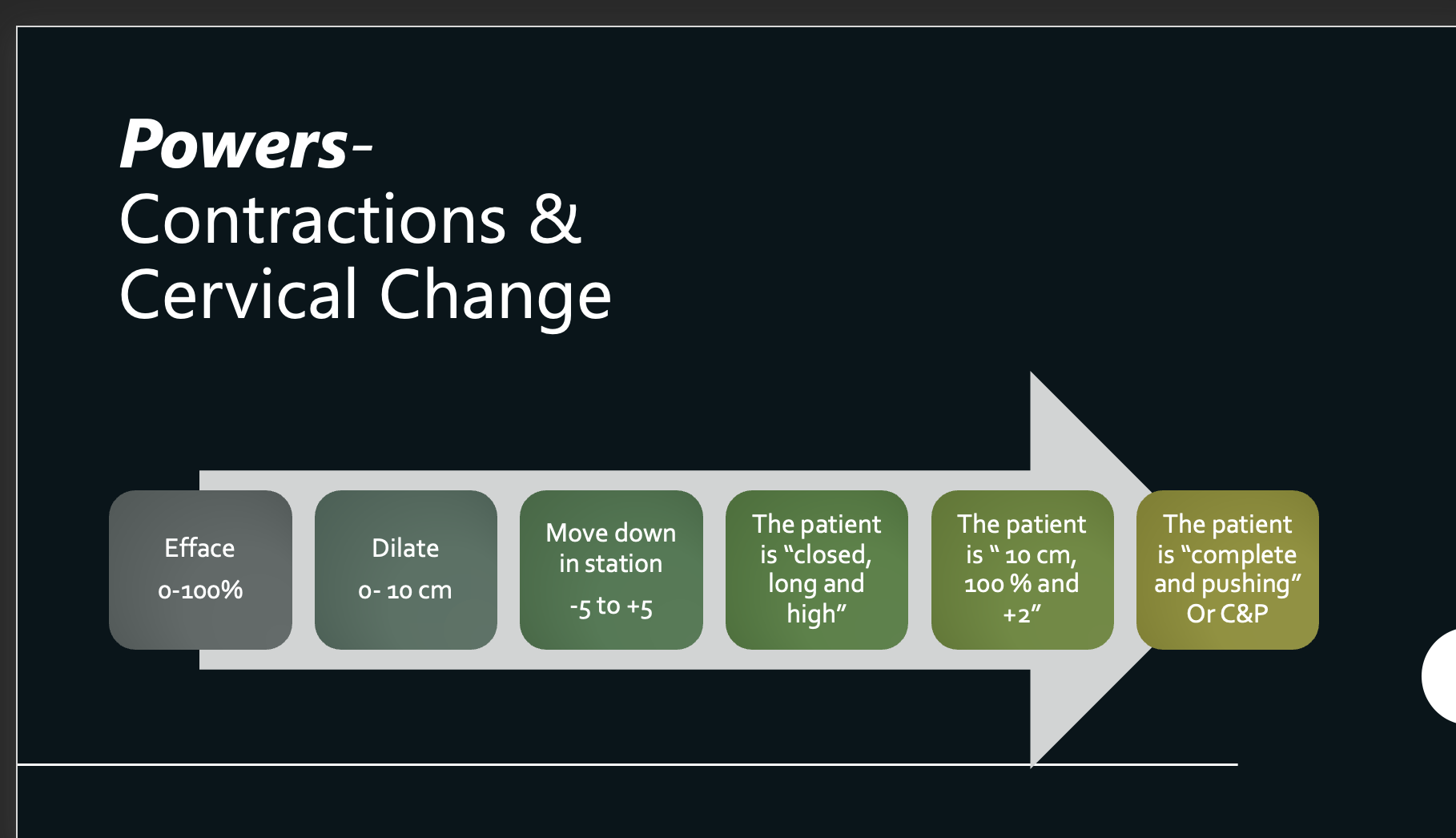
Powers- Physiological Forces
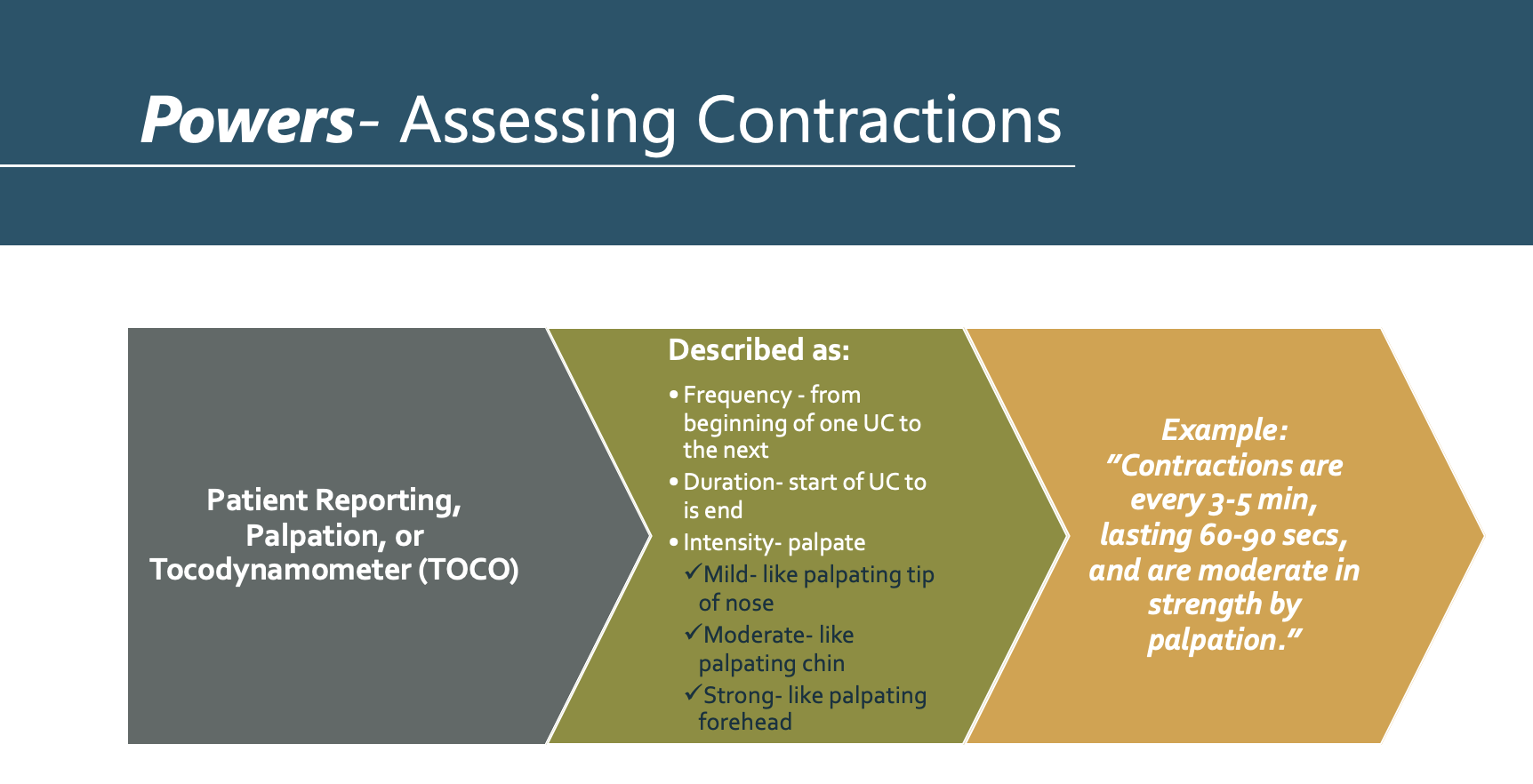
Powers- Assessing Contractions
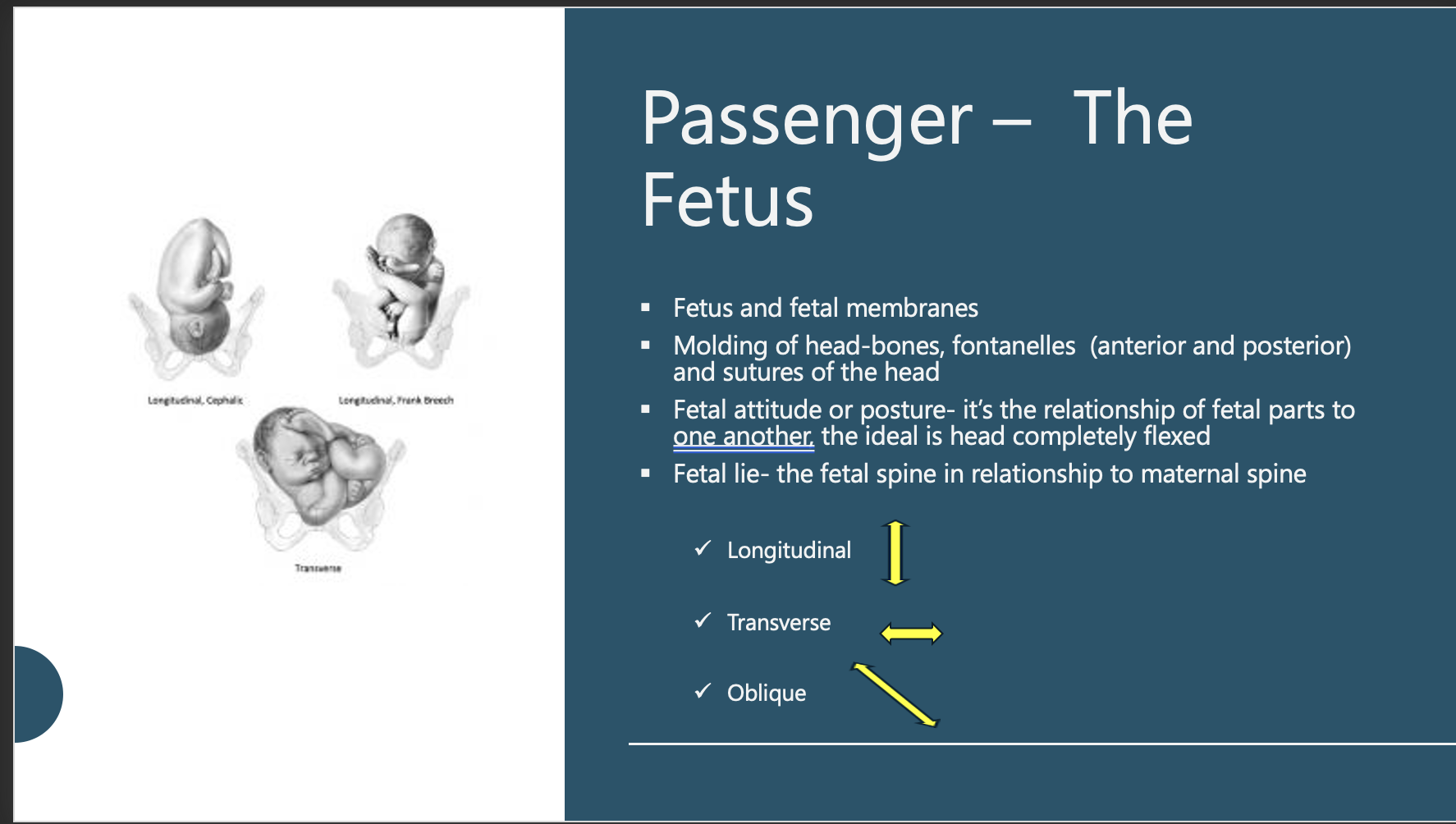
Passenger – The Fetus
Fetal attitude refers to the position or posture of a baby in the womb. It describes how the baby is flexing or extending its body parts, such as the head, arms, and legs. The most common and ideal fetal attitude is when the baby is curled up with the chin tucked down towards the chest, arms, and legs pulled in close to the body. This helps the baby fit better through the birth canal during delivery.
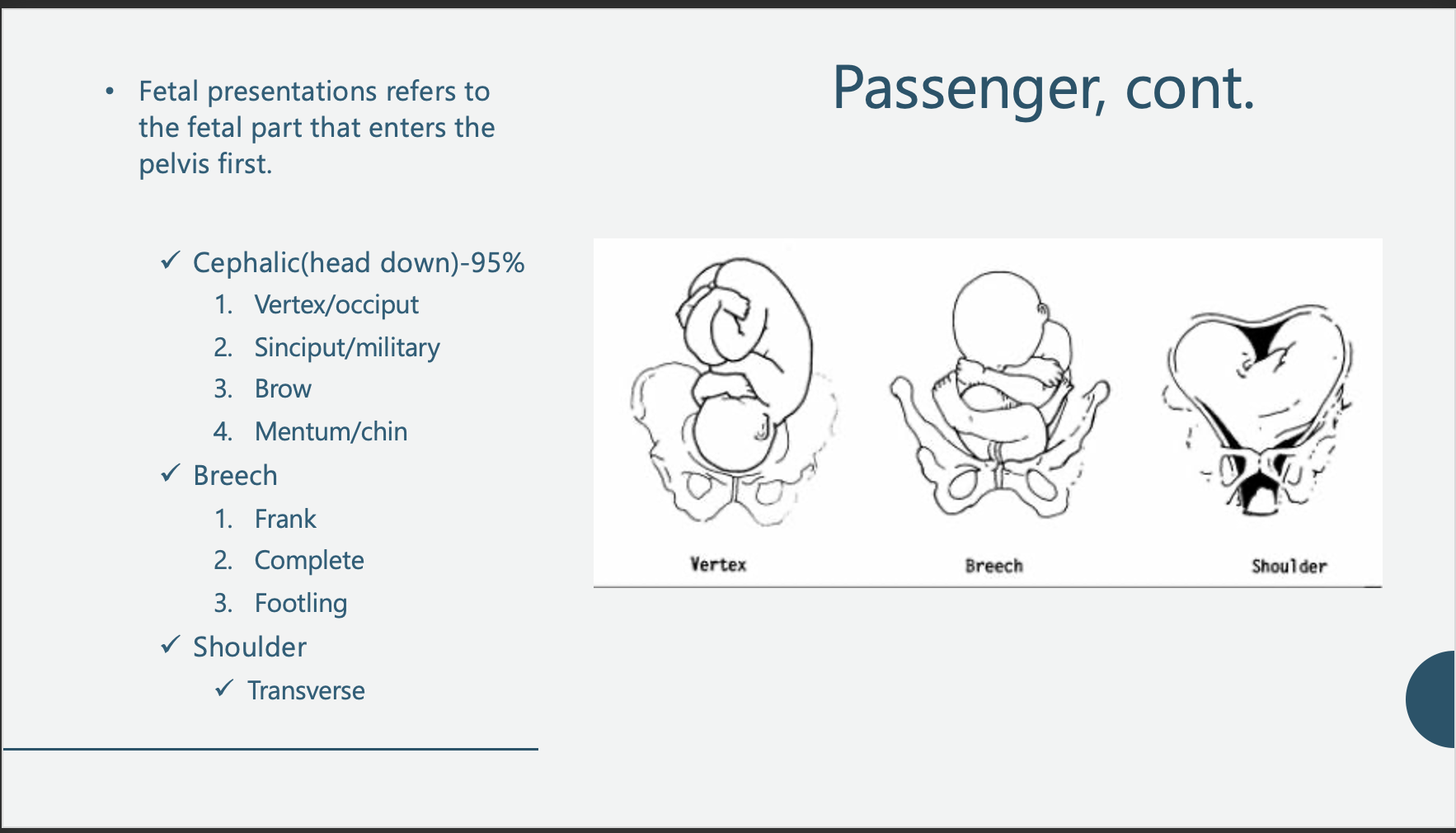
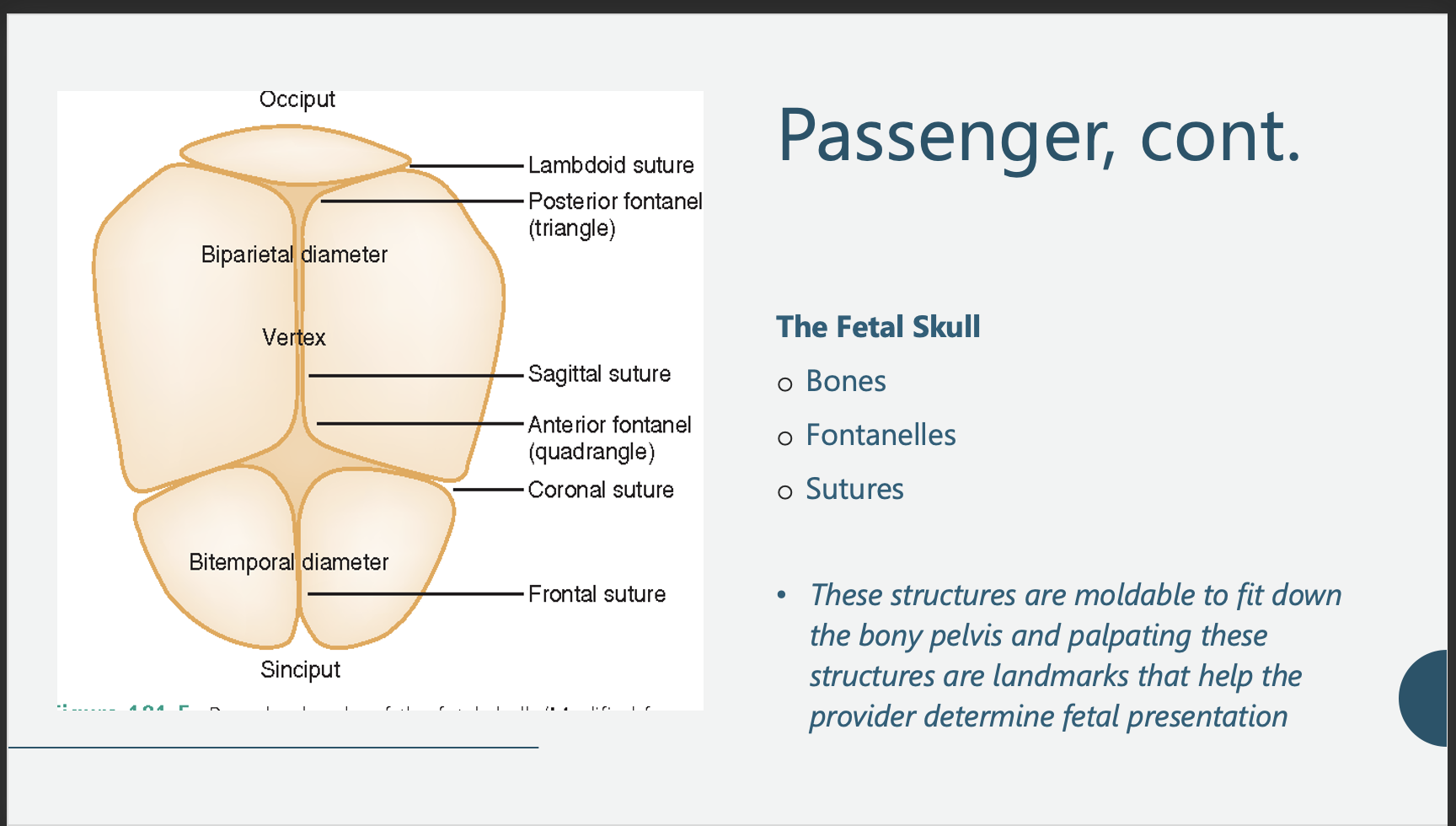
Passenger, cont.
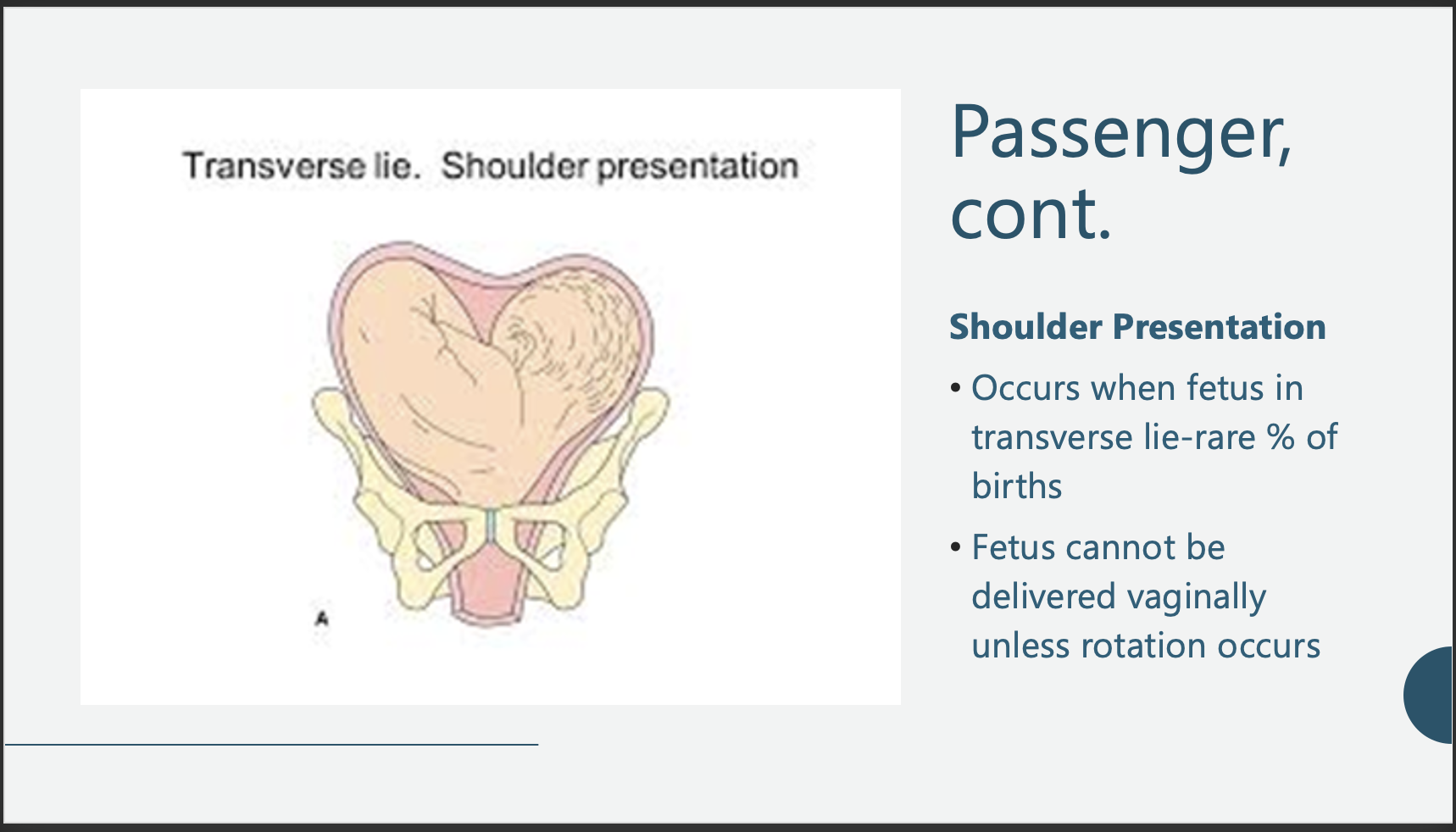
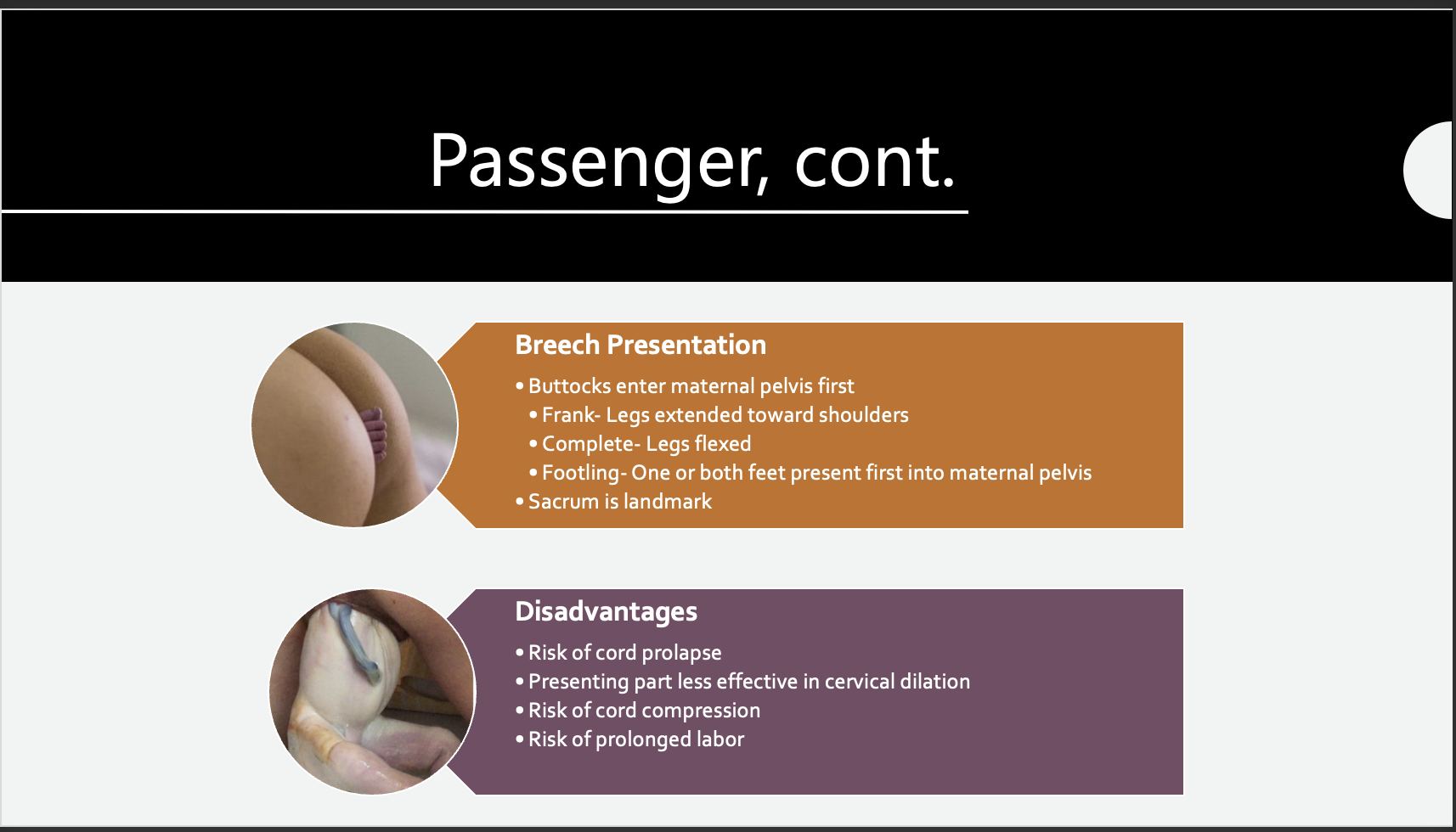
Passenger, cont.
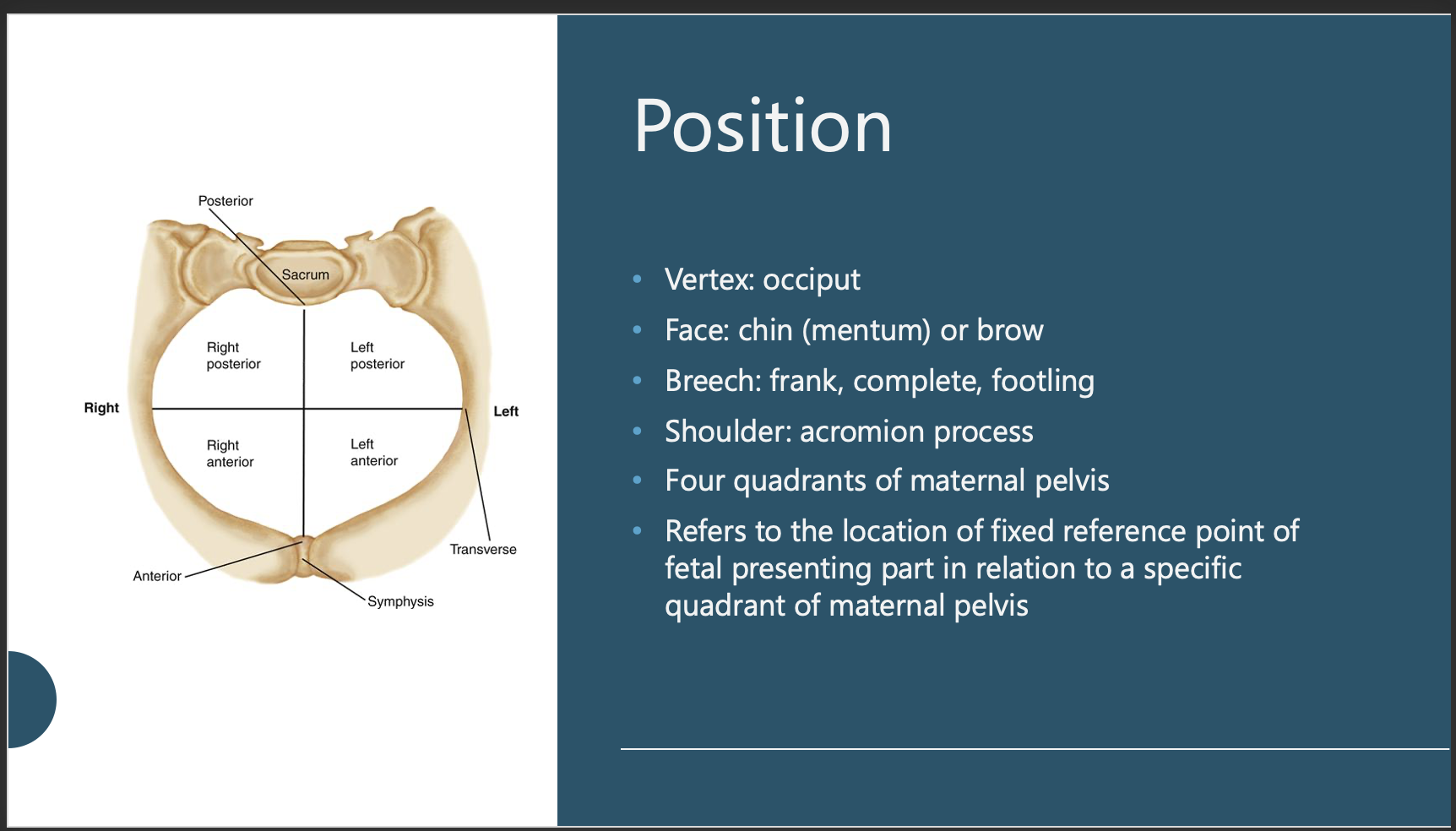
Position
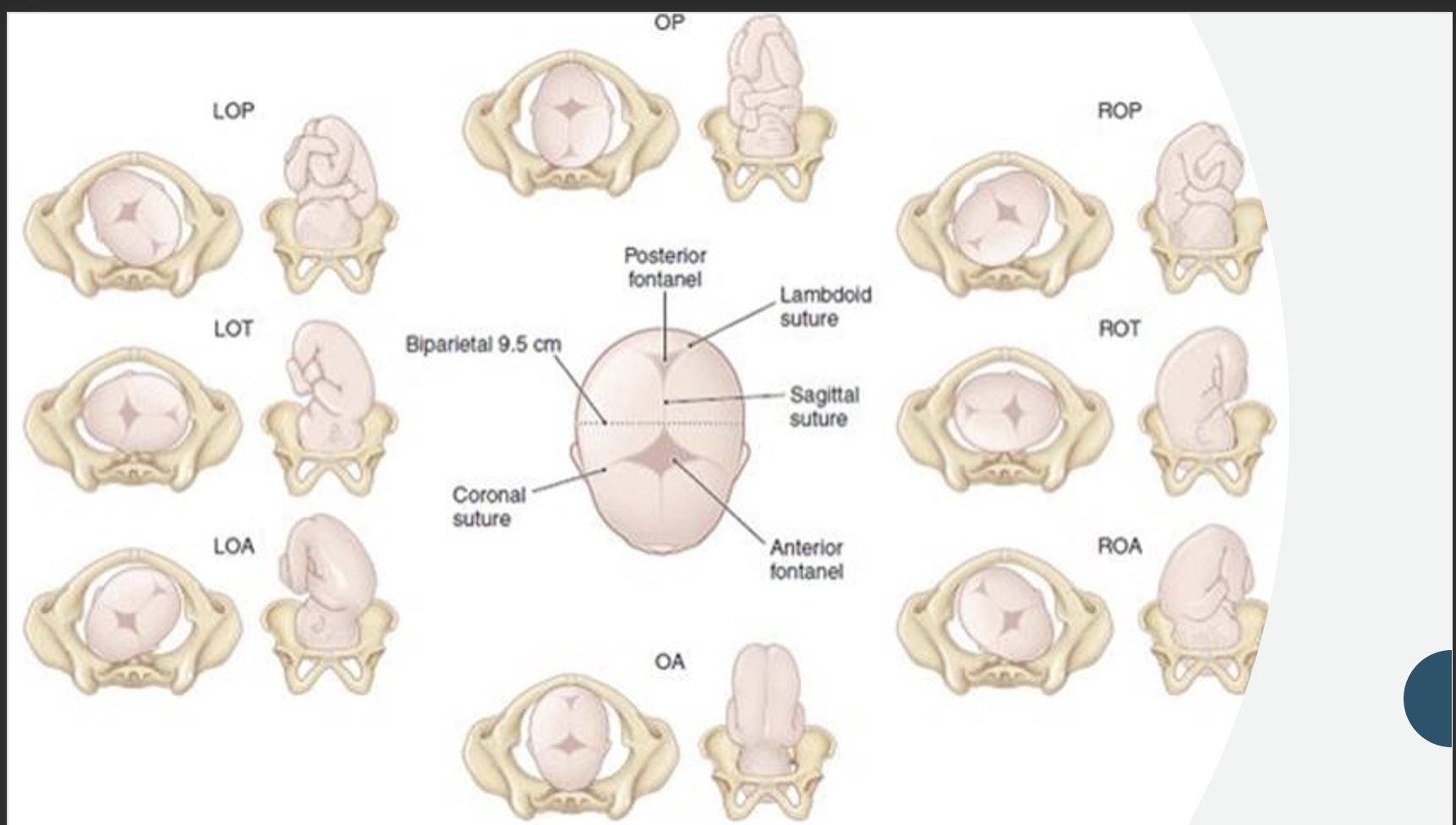
Position
Landmarks
Abbreviations used
First and last letter refer to maternal pelvis
Middle letter refers to presenting part of fetus
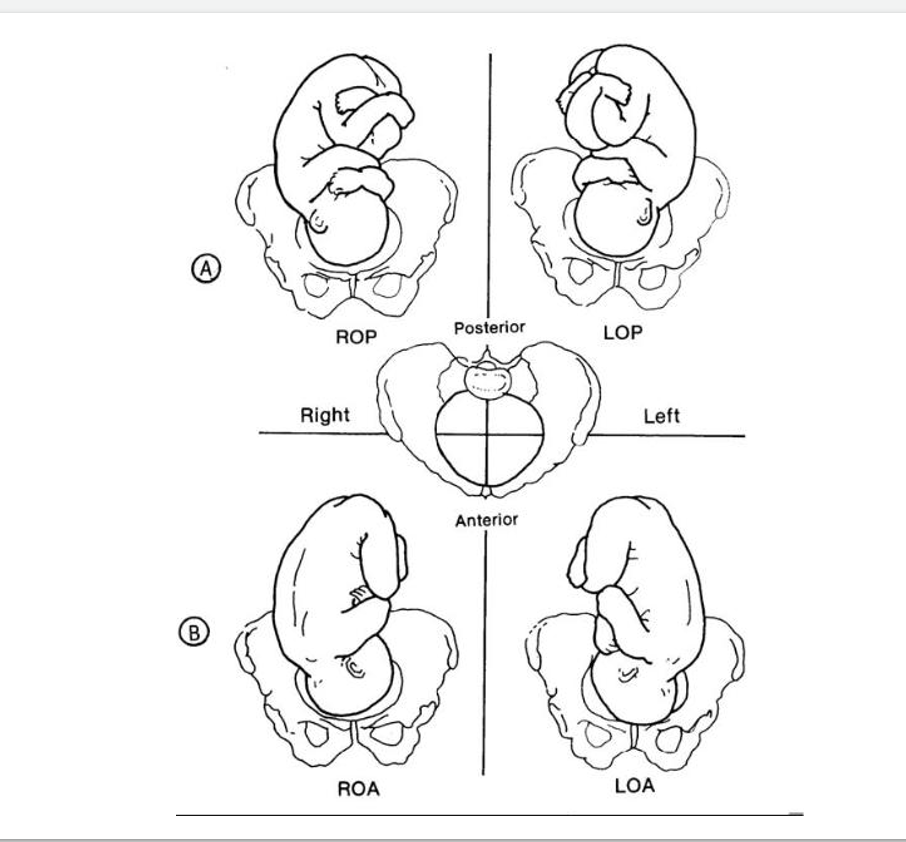
Examples:
ROA (right occiput anterior)
ROP (right occiput posterior)
LSP (left sacrum posterior)
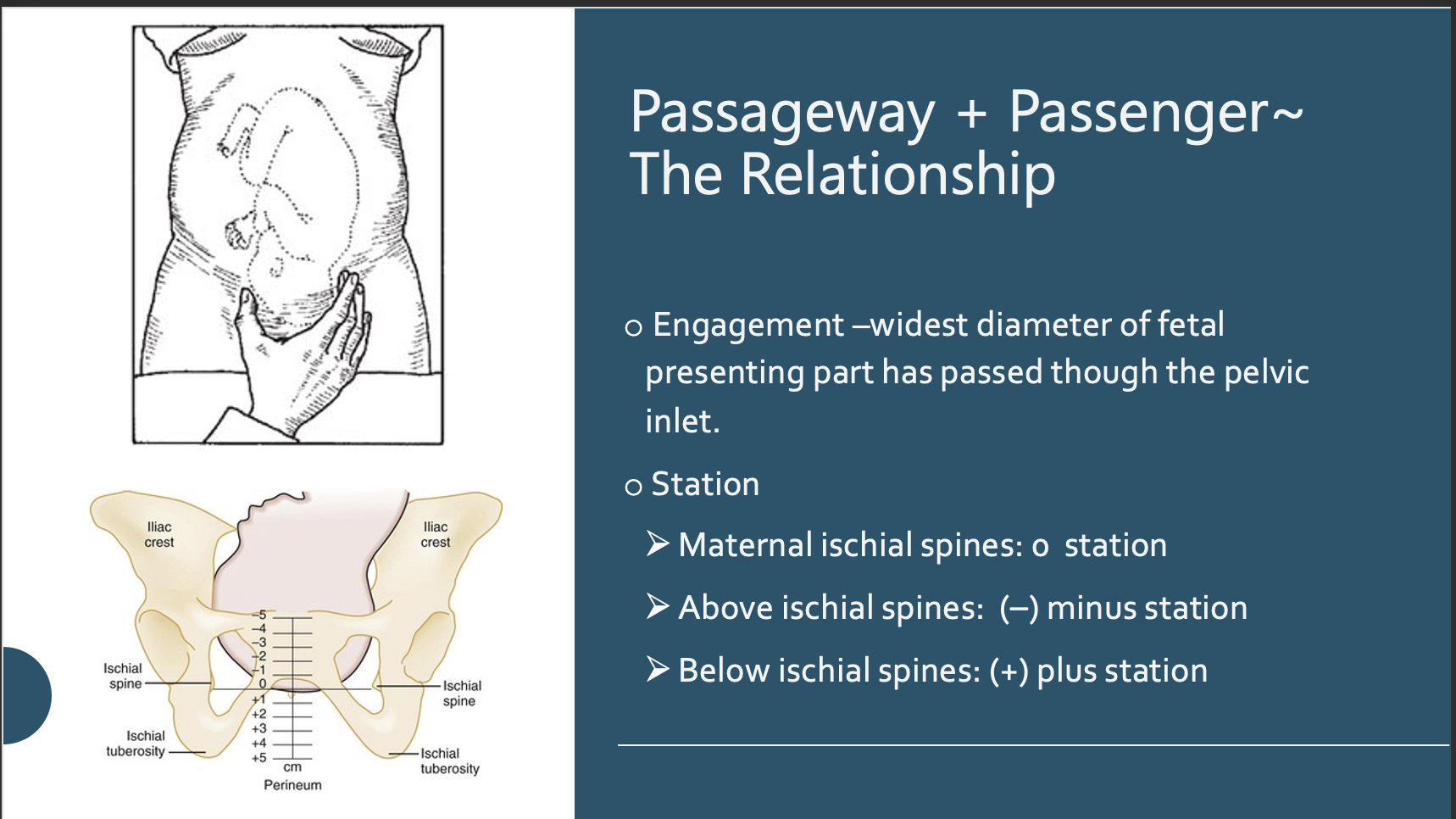
Passageway + Passenger~ The Relationship
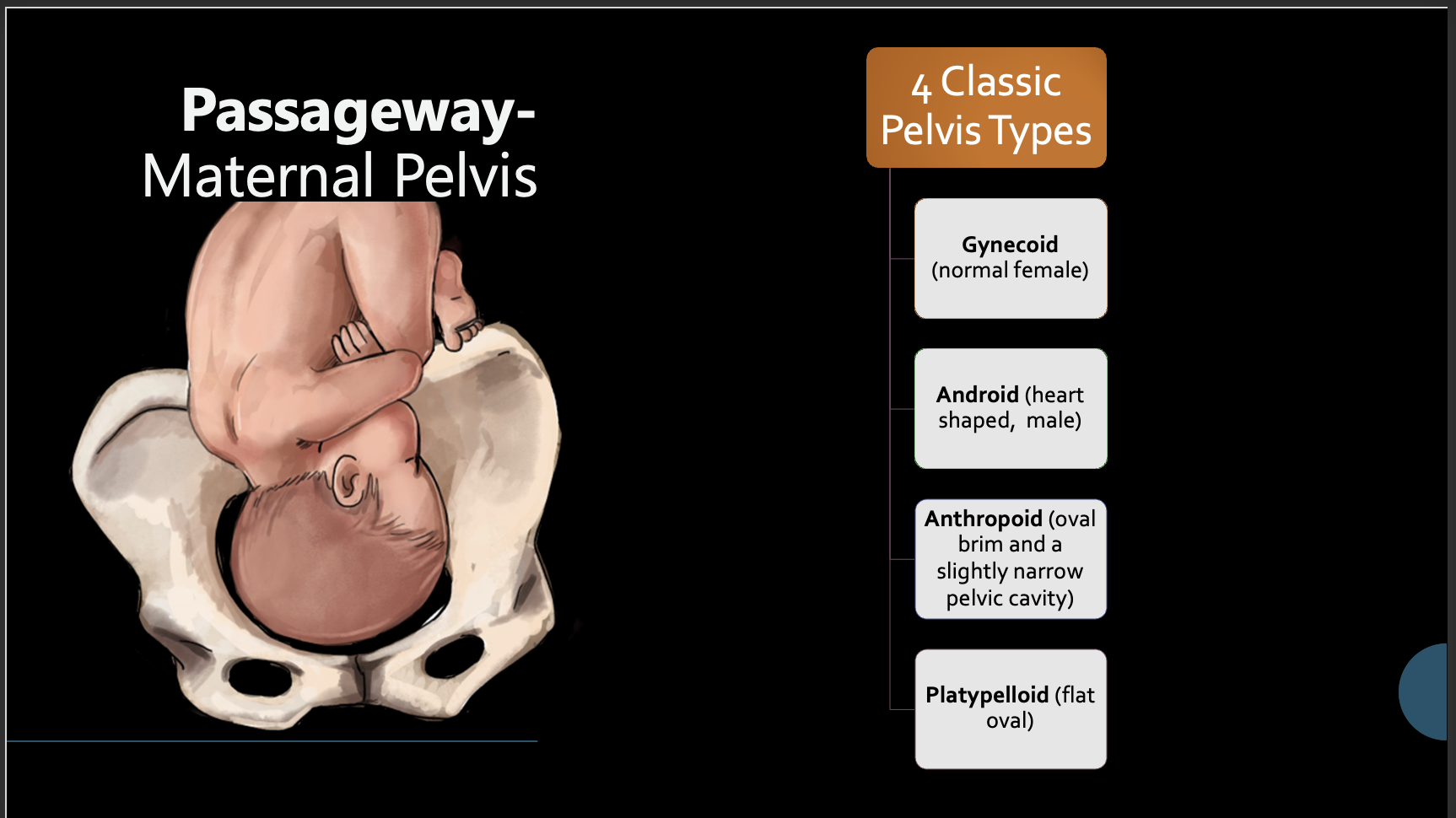
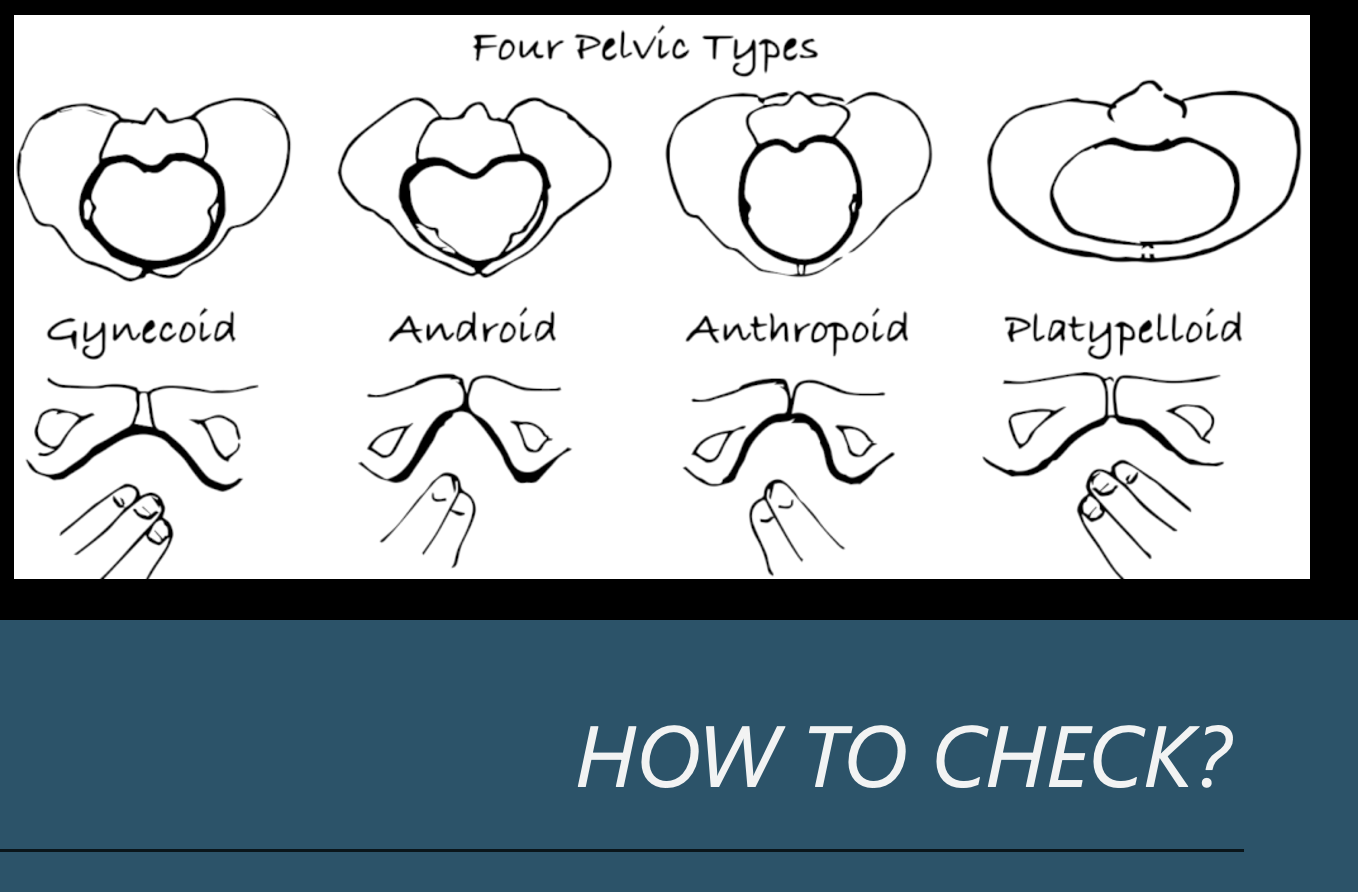
Passageway- Maternal Pelvis
Gynecoid Pelvis: Engagement in this type of pelvis occurs most frequently with the fetus in a transverse position, followed in frequency by the anterior and posterior positions.
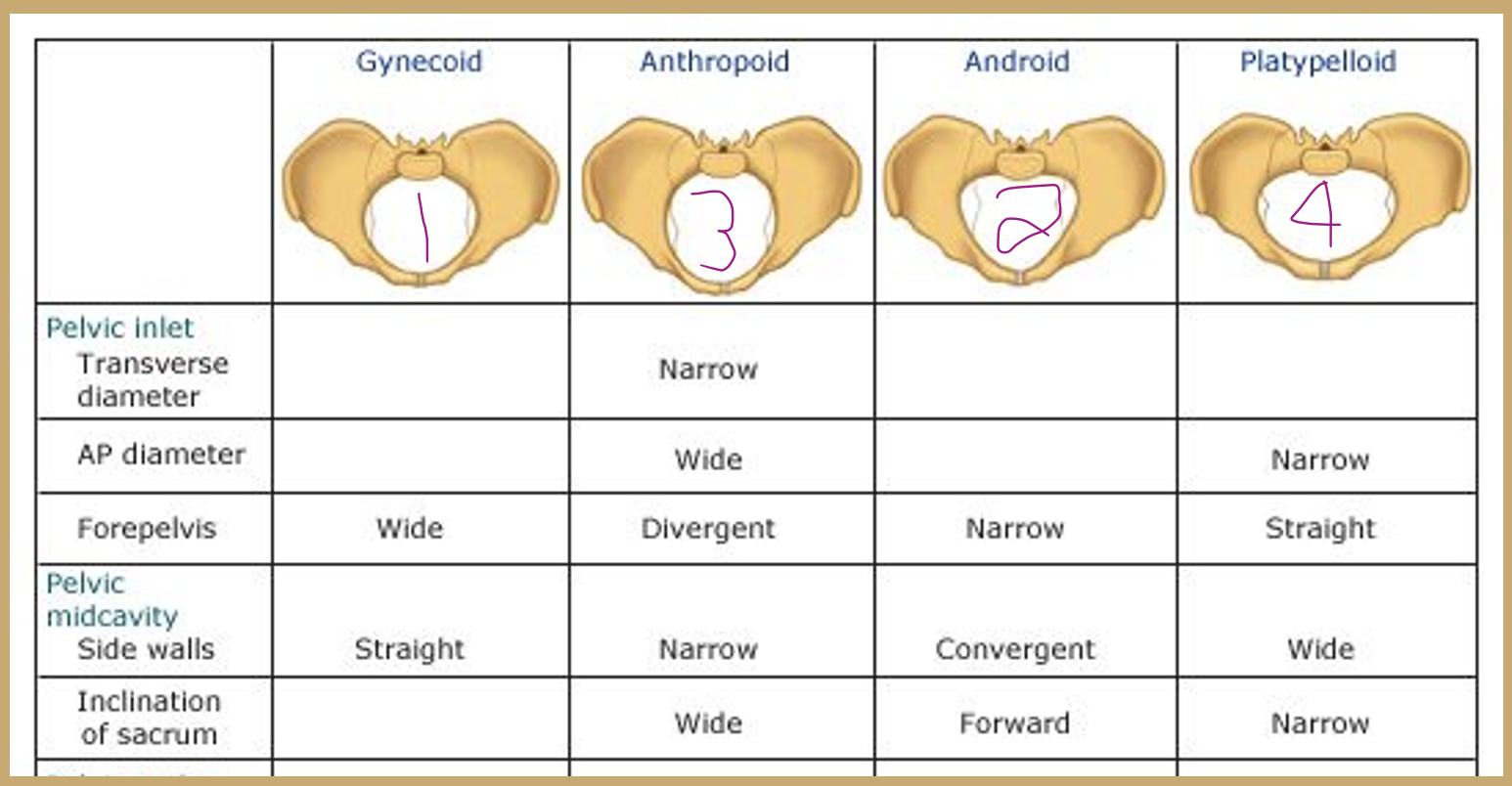
A spacious and well-rounded posterior segment A An inlet with a slightly ovoid or round shape A wide, well-rounded forepelvis (anterior segment) A sacrosciatic notch of medium size An average sacral inclination and curvature A wide subpubic arch Wide interspinous and intertuberous diameters Bones ranging from medium to delicate in structure
Android pelvis: Engagement in this type of pelvis occurs most frequently with the fetus in a transverse position, followed in frequency by the posterior and anterior positions. The clinician should be alerted by this type of pelvis that the possibility of posterior positions exists.
A wedge-shaped inlet A narrow retropubic angle (anterior segment) A flat, wide posterior segment A narrow sacrosciatic notch A forward sacral inclination A narrow wedge-shaped “Gothic” subpubic arch Converging side walls, narrow interspinous and intertuberous diameters Bones ranging from medium to heavy in structure
Anthropoid pelvis: Engagement in this type of pelvis occurs with the fetus in either an anterior or transverse position, but the anterior position appears to be more characteristic.
A long, narrow, oval-shaped inlet A long, narrow, well-rounded anterior segment A long, narrow posterior segment A very wide, shallow sacrosciatic notch A long, narrow sacrum with average inclination and curvature A slightly narrow subpubic arch Straight side walls with below-average interspinous and intertuberous diameters Medium to delicate bones
Platypelloid pelvis: Engagement in this type of pelvis will almost always occur with the fetus in a transverse position. Because of the flatness of the shape of this pelvis, the internal rotation of the vertex can be limited, causing a deep transverse arrest. C/S
A transverse, oval-shaped inlet A very wide, round retropubic angle A very wide, flat posterior segment A narrow sacrosciatic notch Average sacral inclination A very wide subpubic arch Straight side walls with very wide interspinous and intertuberous diameters Bones ranging from medium to delicate in structure
Pelvis
Position
Psyche
Signs and Symptoms of Labor
Braxton Hicks contractions
Lightening (approx. 2 weeks before onset)
Loss of mucus plug
Bloody show
Cervical changes
Rupture of membranes
Energy spurt
Weight loss, GI disturbances
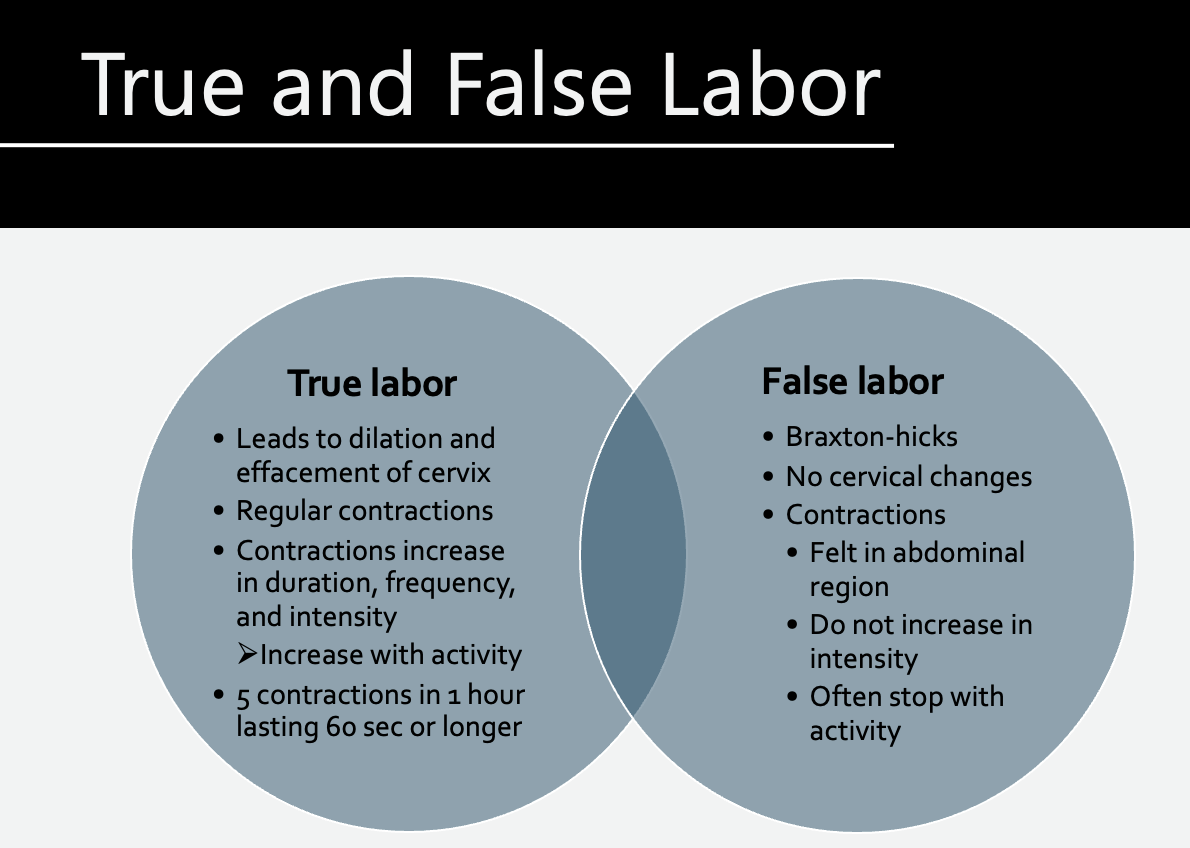
True and False Labor
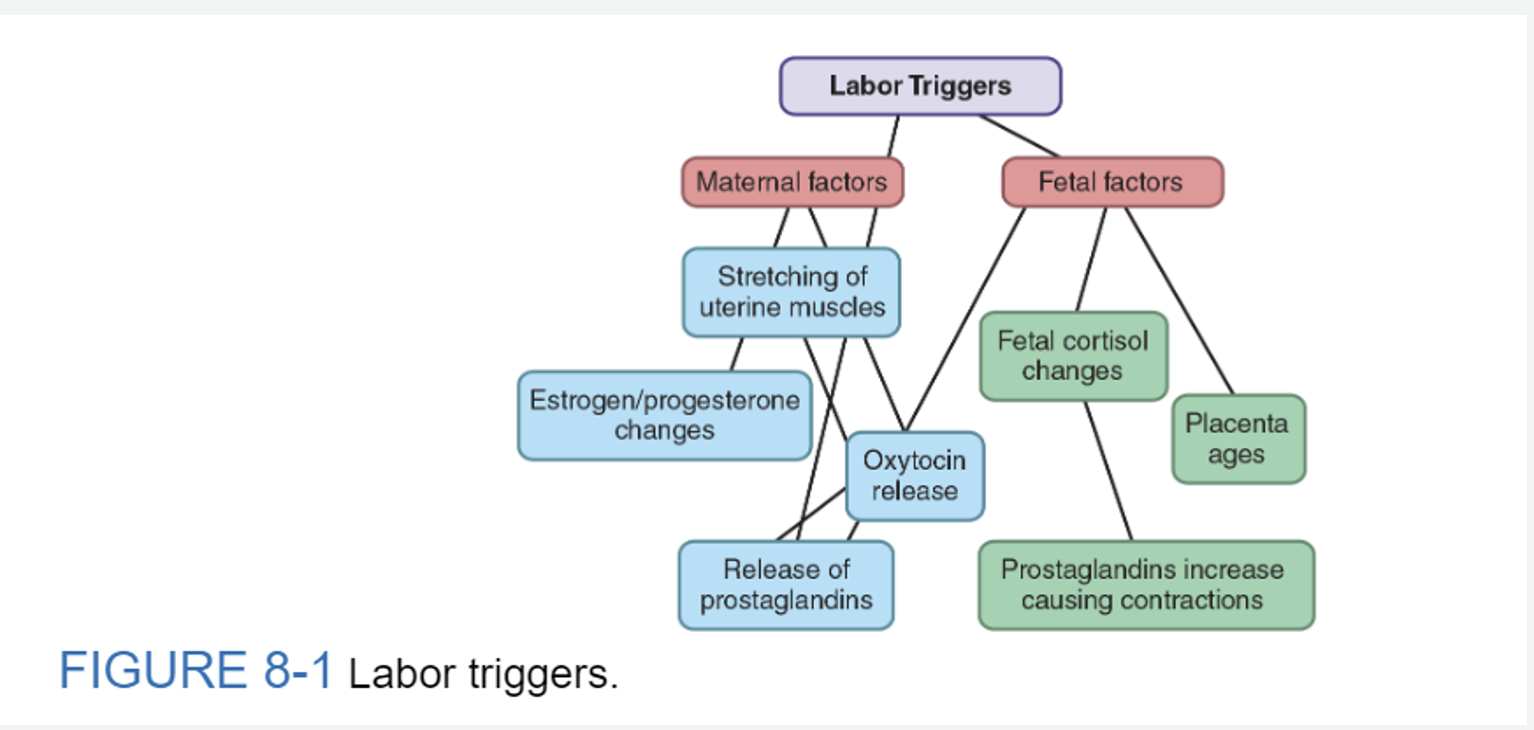
Labor triggers
Maternal Factors
• Uterine muscles are stretched to the threshold point, leading to the release of prostaglandins and oxytocin that stimulate contractions.
• Increased pressure on the cervix stimulates the nerve plexus, causing the release of oxytocin by the maternal pituitary gland, which then stimulates contractions.
• Estrogen levels increase, enhancing the ability of uterine myometrium to produce contractions.
• Progesterone is functionally withdrawn.
• Oxytocin and prostaglandins, which have been previously inhibited by progesterone, together soften the cervix and stimulate myometrial contractions.
Fetal Factors
• Prostaglandin synthesis by the fetal membranes and the decidua stimulates contractions.
• Produced by the fetal hypothalamic-pituitary-adrenal axis, fetal cortisol levels increase, and, acting on the placenta, cause an inflammatory response and an increased level of prostaglandins, stimulating the uterus to contract.
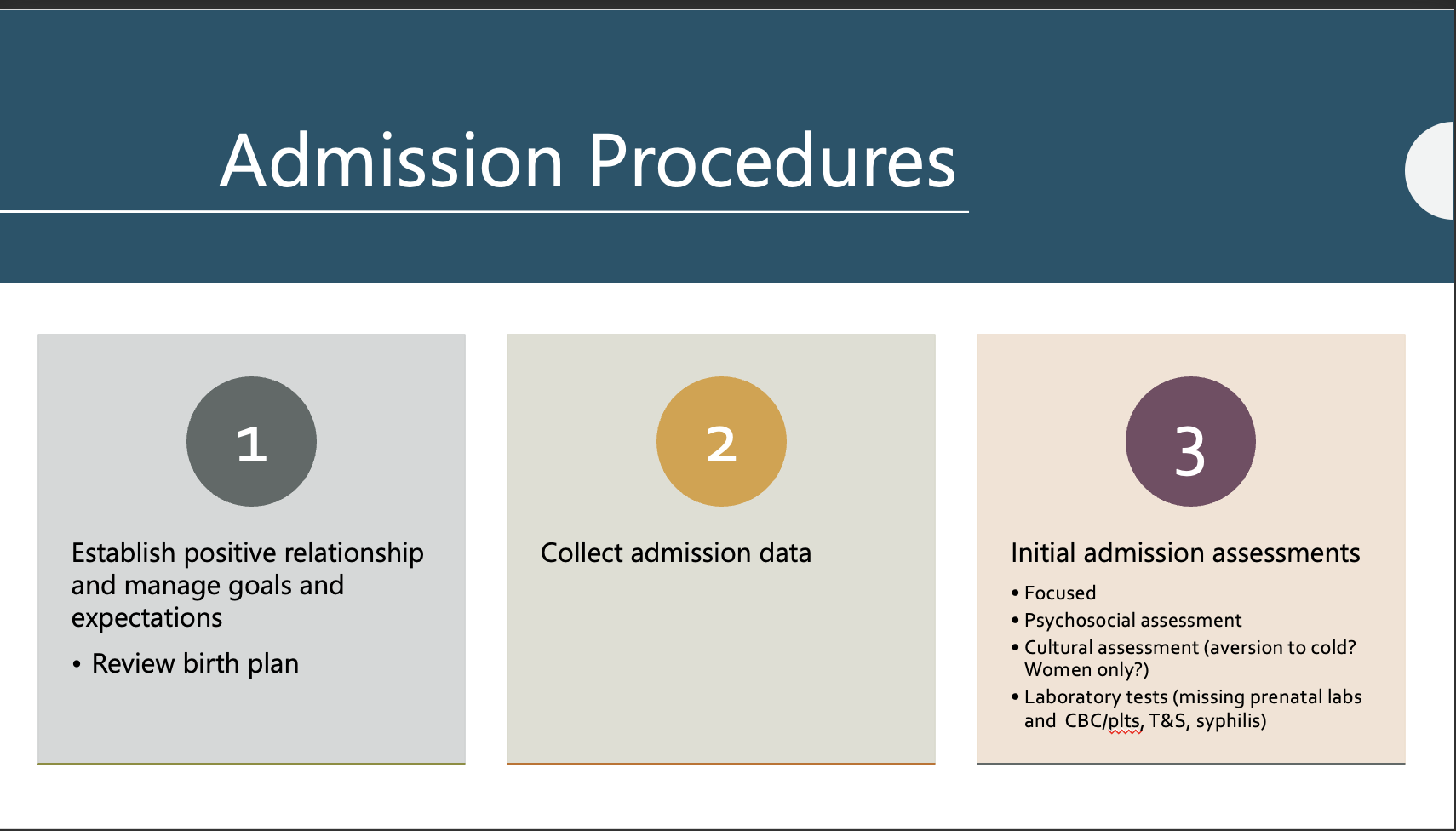
Admission Procedures
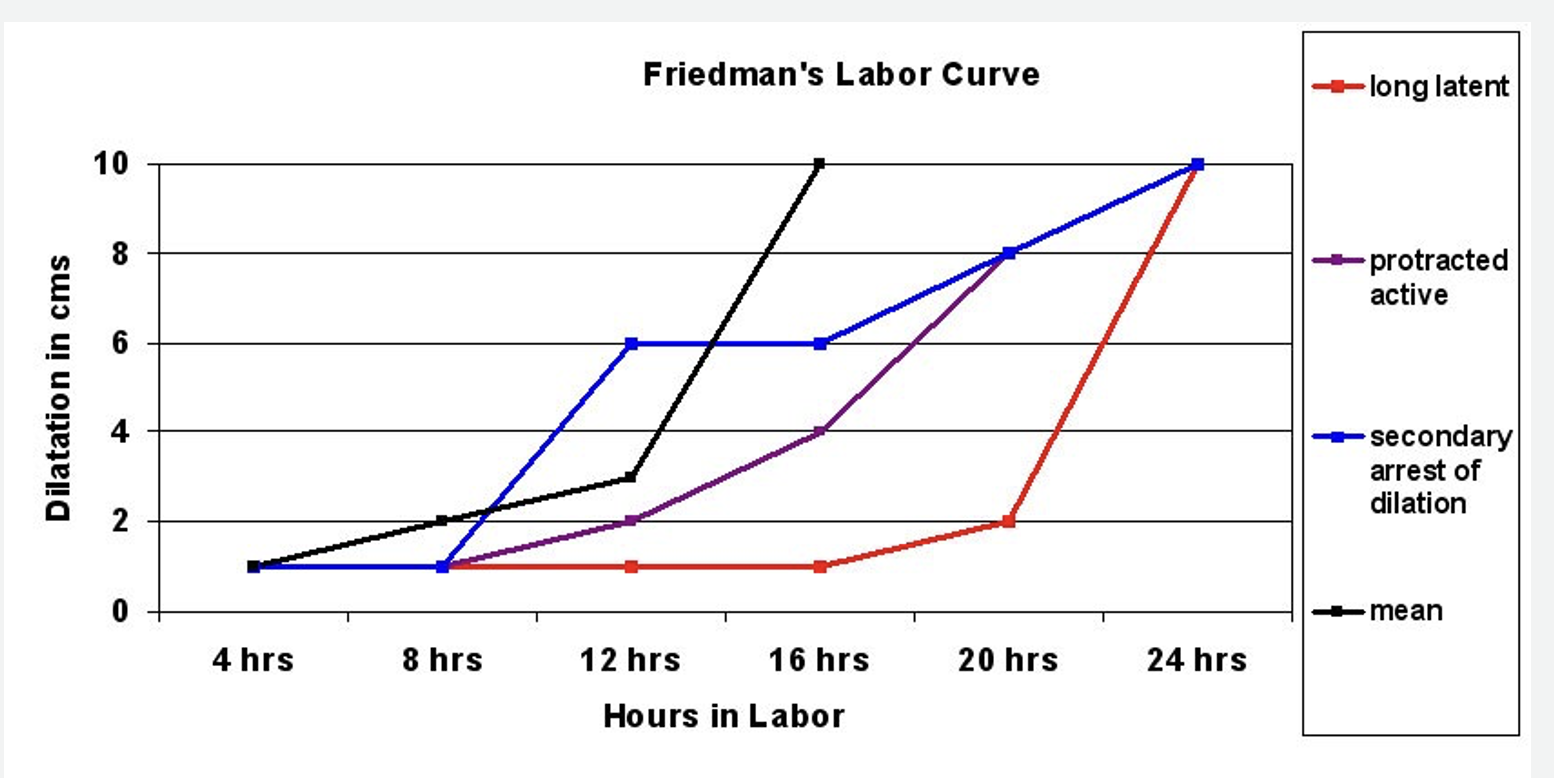
Labor
Protracted labor is a labor abnormality that occurs when labor progresses more slowly than expected.
Secondary arrest of dilation is a condition that occurs when cervical dilation stops for a period of two hours or more, following a history of normal dilation.
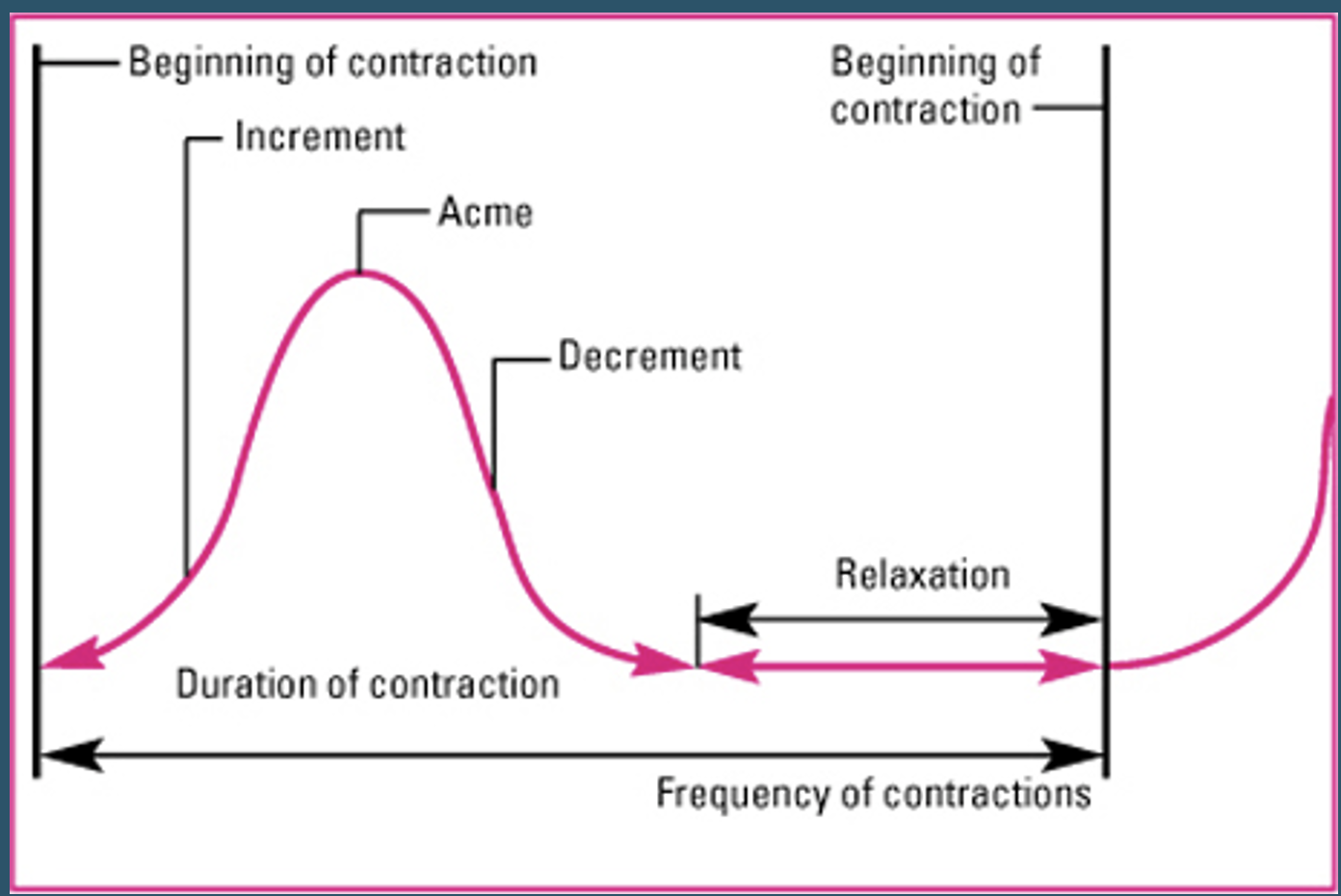
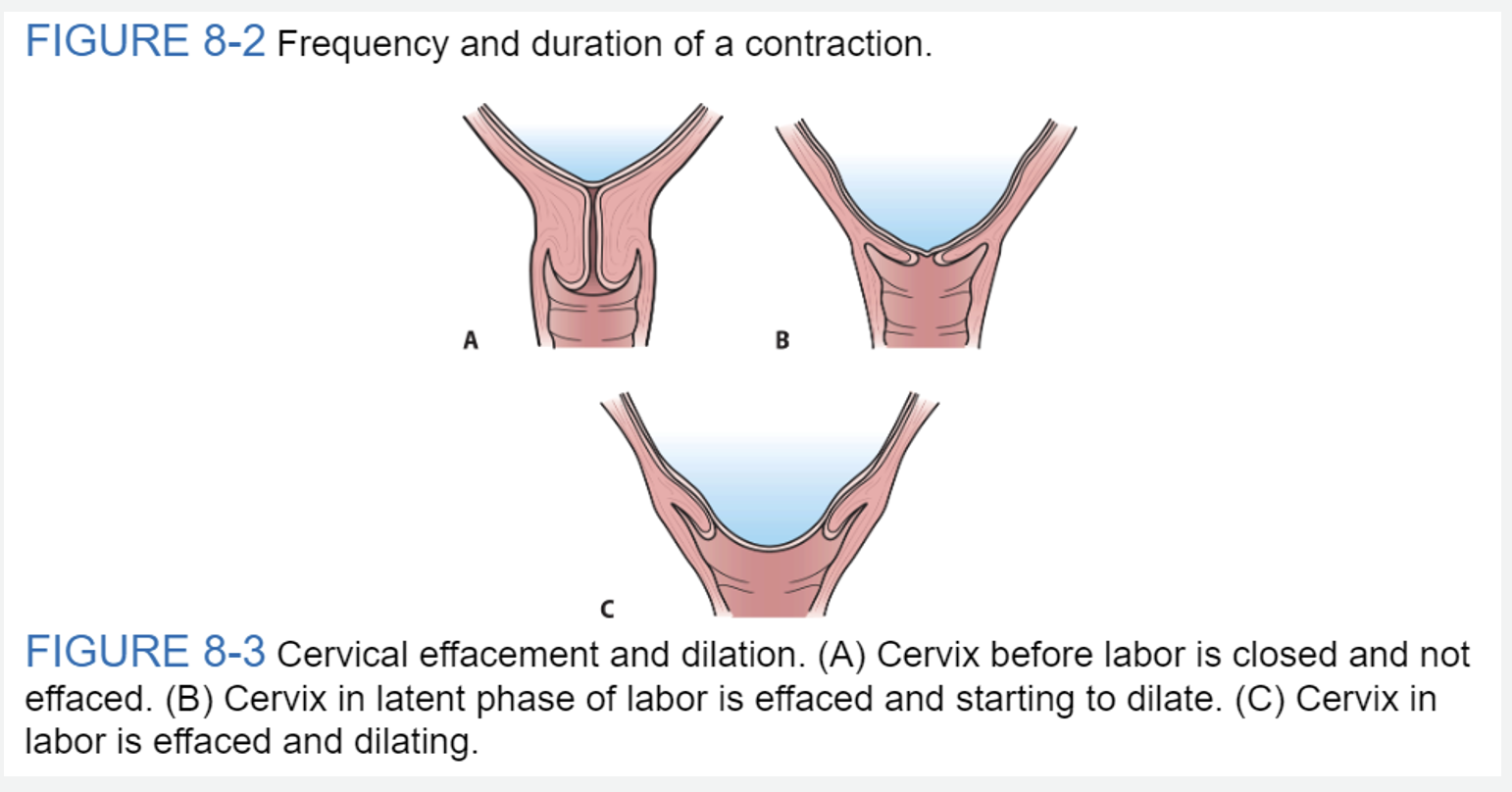
Contraction

Nursing Care
Labor Support
Fetal Assessment
Baseline Fetal Heart Rate (FHR):
The baseline FHR is the heart rate during a 10-minute segment rounded to the nearest 5 beat per minute increment excluding periods of marked FHR variability, periodic or episodic changes, and segments of baseline that differ by more than 25 beats per minute.
The minimum baseline duration must be at least 2 minutes. If minimum baseline duration is < 2-minutes, then the baseline is indeterminate.
Bradycardia :Mean FHR < 110 BPM
A rate of 100-119 BPM in the absence of other non reassuring patterns is not usually a sign of compromise
Etiologies: Heart block (little or no variability), occiput posterior or transverse position, serious fetal compromise.
Tachycardia: Mean FHR>160 BPM
In the presence of good variability tachycardia is not a sign of fetal distress
Etiologies: Maternal fever, fetal hypoxia, fetal anemia, amnionitis, fetal tachyarrhythmia (usually > 200 BPM with abrupt onset little to no variability) SVT (200-240 BPM), fetal heart failure, drugs (beta sympathomimetics, vistaril, phenothiazines) , rebound ( transient tachycardia following a deceleration accompanied by decreased variability)
Baseline change: The decrease or increase in heart rate lasts for longer than 10 minutes.
Etiologies of decreased variability: Fetal metabolic acidosis, CNS depressants, fetal sleep cycles, congenital anomalies, prematurity, fetal tachycardia, pre-existing neurologic abnormality, and betamethasone.
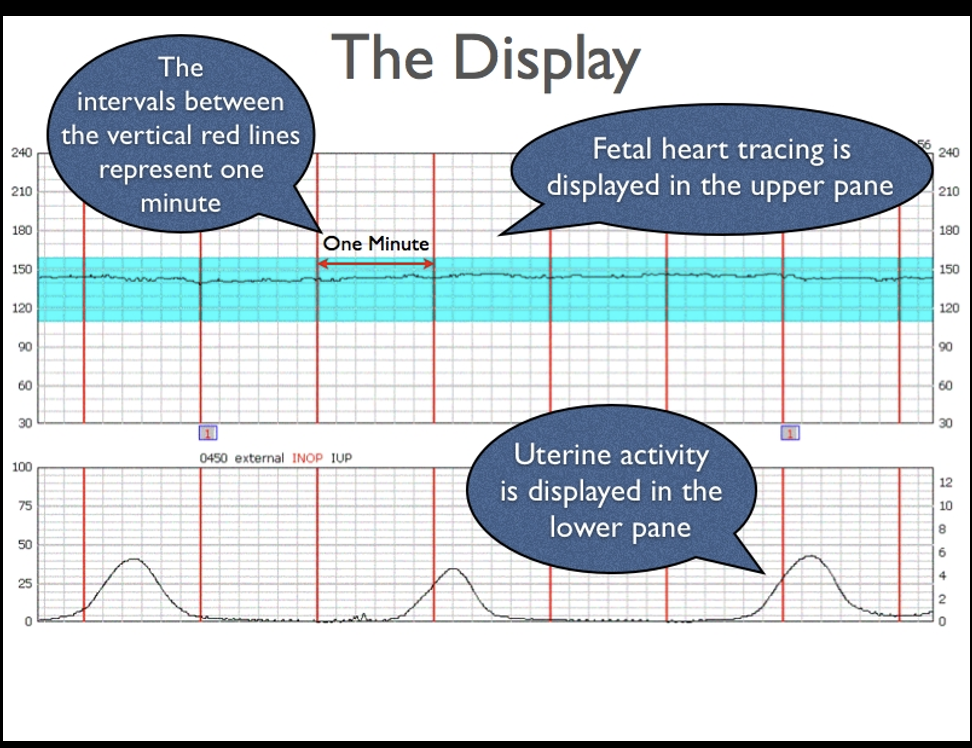
Fetal Monitoring
The interpretation of the fetal heart rate tracing should follow a systematic approach with a full qualitative and quantitative description of the following:
Baseline rate
Baseline fetal heart rate (FHR) variability
Presence of accelerations
Periodic or episodic decelerations
Changes or trends of FHR patterns over time
Frequency and intensity of uterine contractions
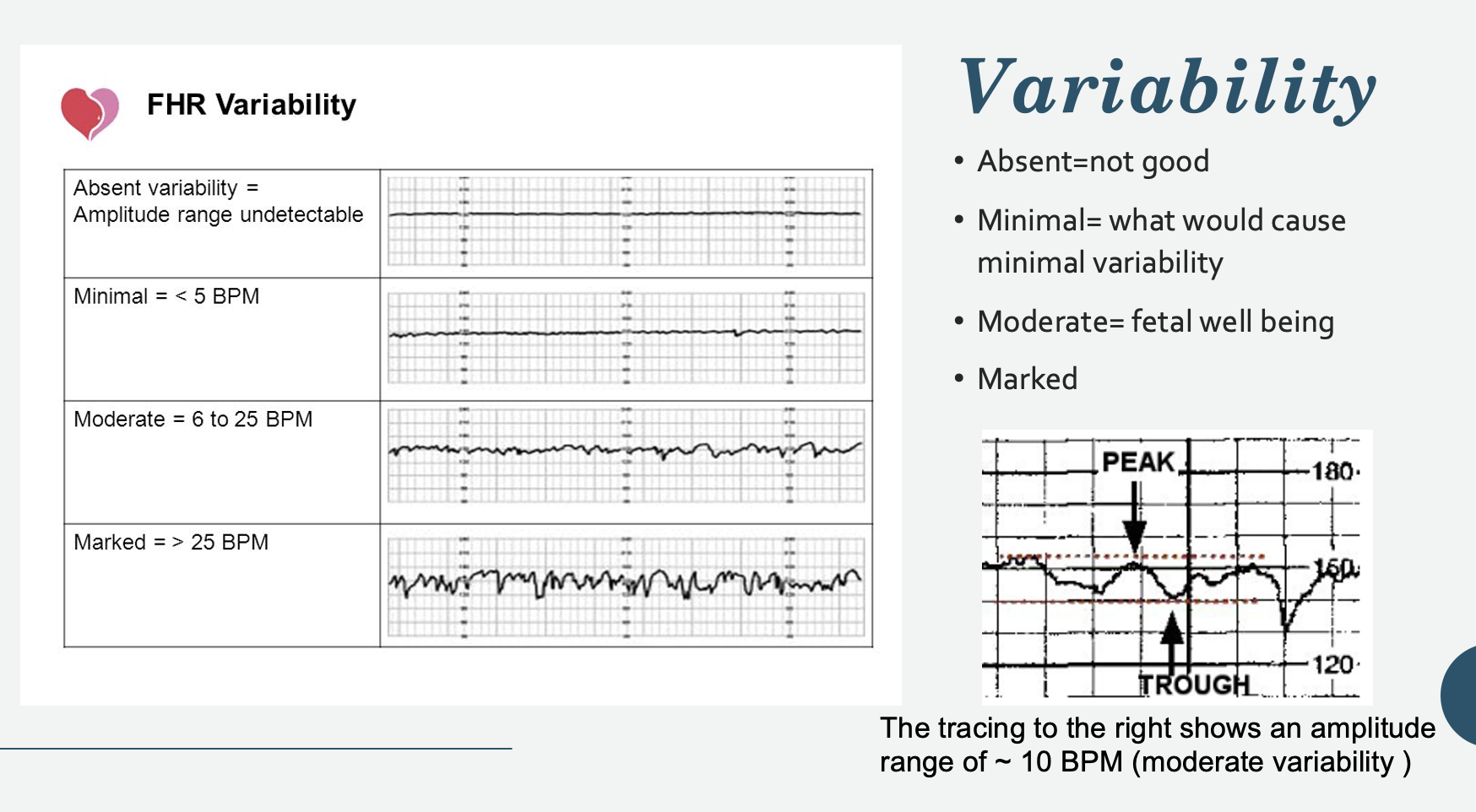
Variability
Persistently minimal or absent FHR variability appears to be the most significant intrapartum sign of fetal compromise.
On the other hand, the presence of good FHR variability may not always be predictive of a good outcome.
Etiologies of decreased variability: Fetal metabolic acidosis, CNS depressants, fetal sleep cycles, congenital anomalies, prematurity, fetal tachycardia, pre-existing neurologic abnormality, and betamethasone.
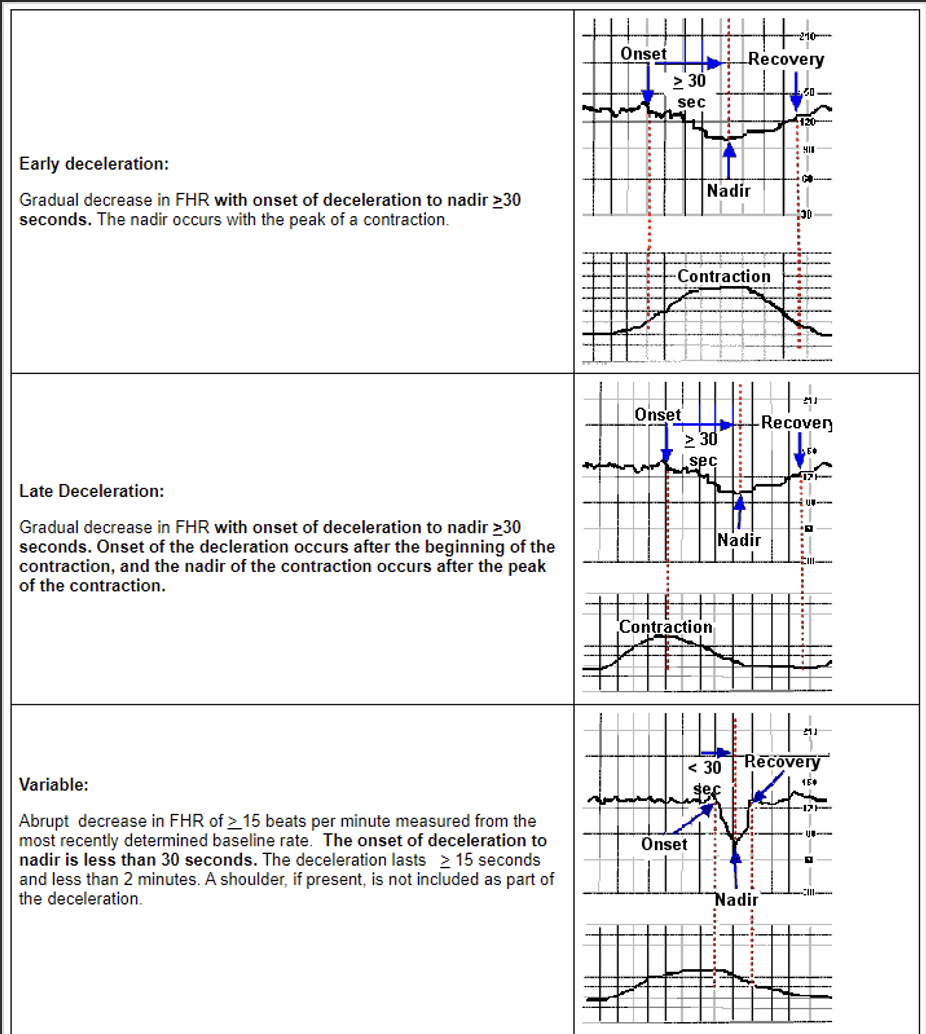
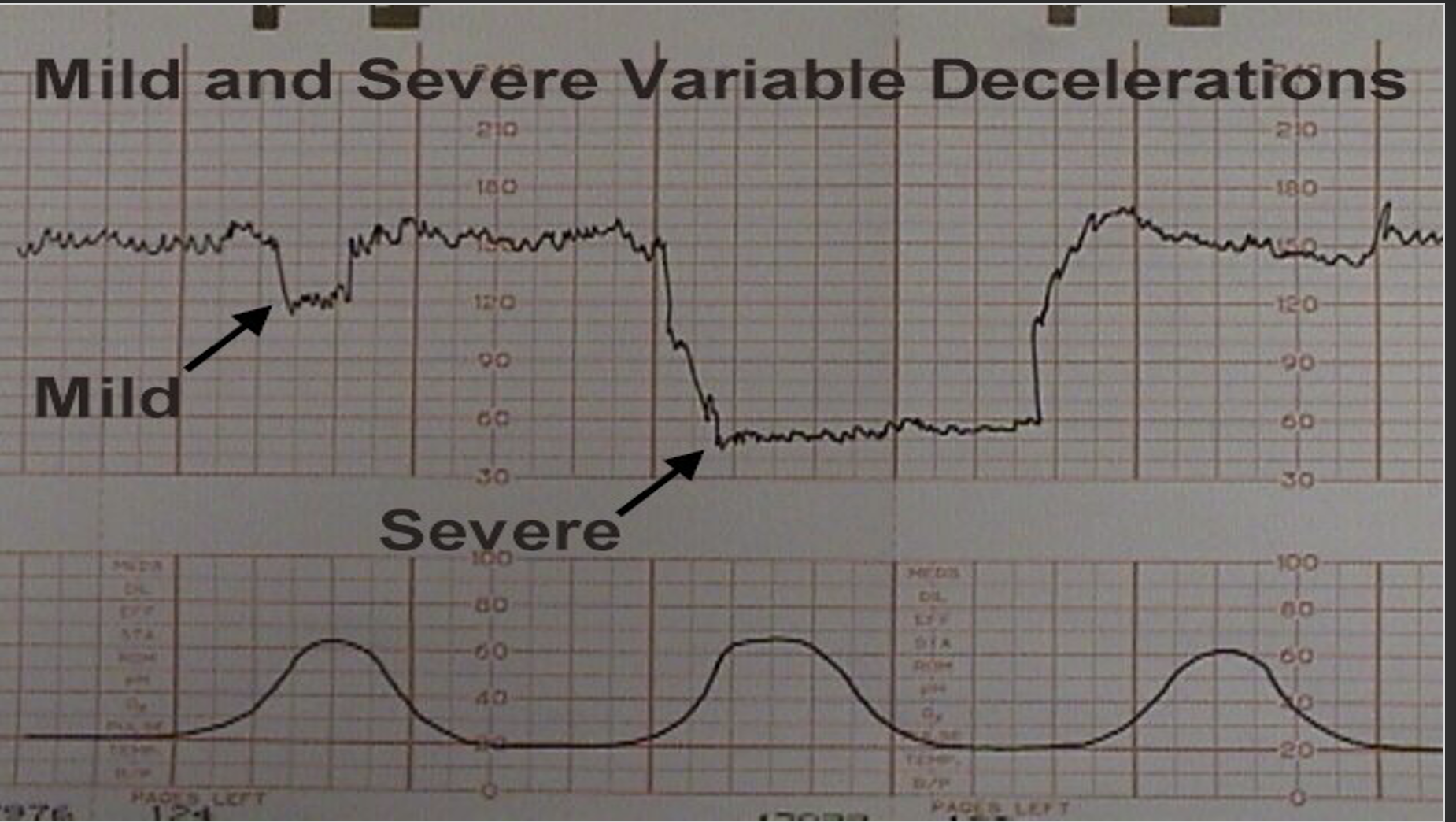
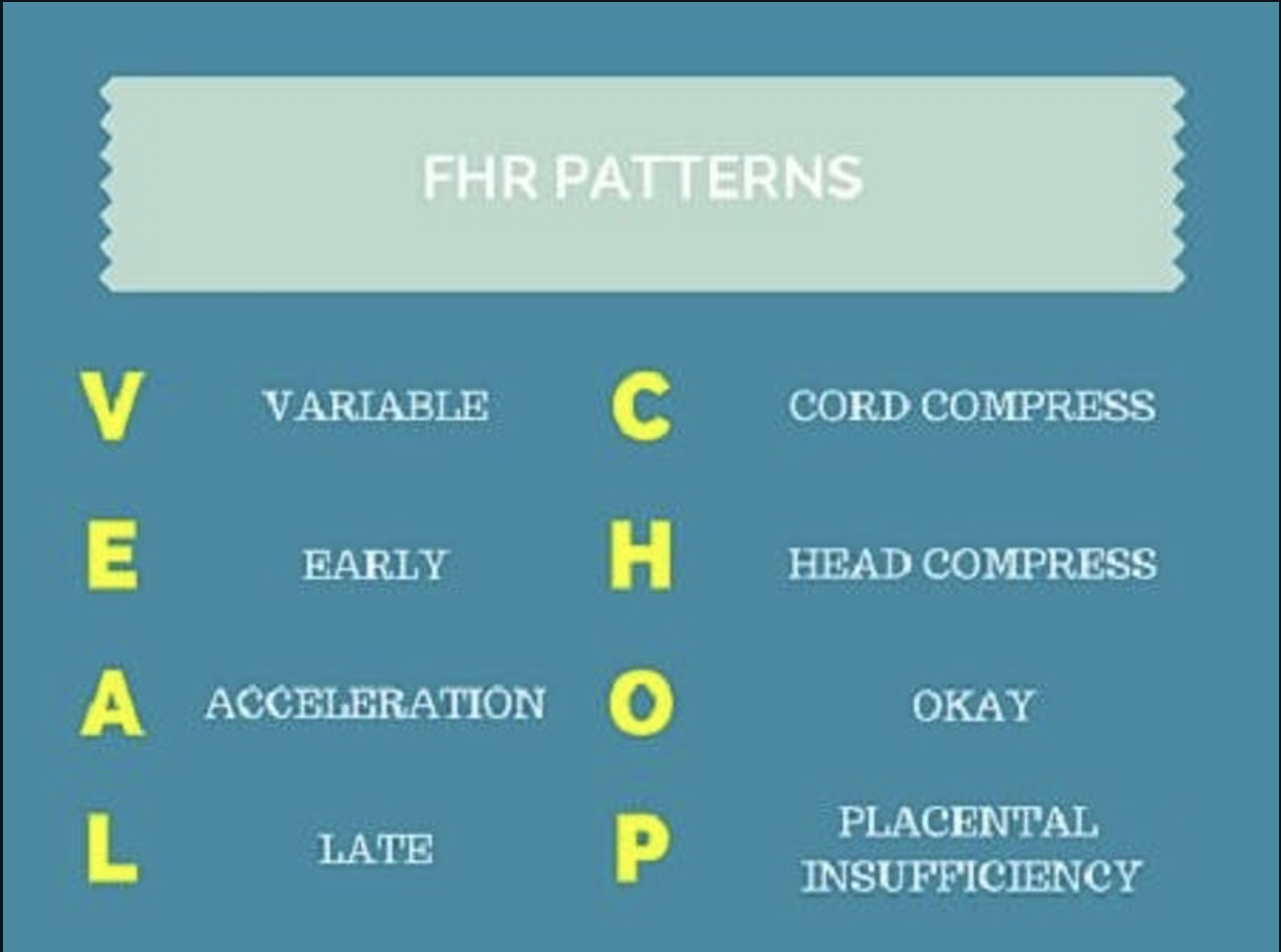
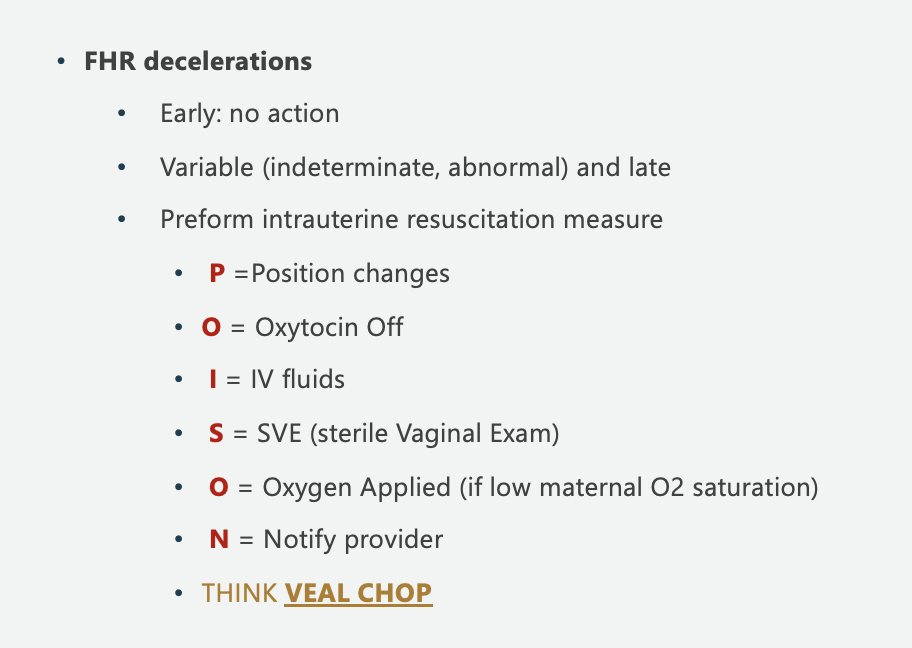
Types of Decelerations
Early- head compression
Late- placental insufficiency
Variable- cord compression
Variable must be 15 beats below the baseline, early/late is only 10 beasts below baseline.
Early decels are good ones
Variable decels as bad ones
Late decels are ugly never want to see them
Periodic or Episodic Decelerations
Episodic pattern- are not associated with uterine contractions
Variable decelerations
Late deceleration r/t supine hypotension
Periodic pattern- associated with uterine contractions
Early and late decelerations
Variables decelerations
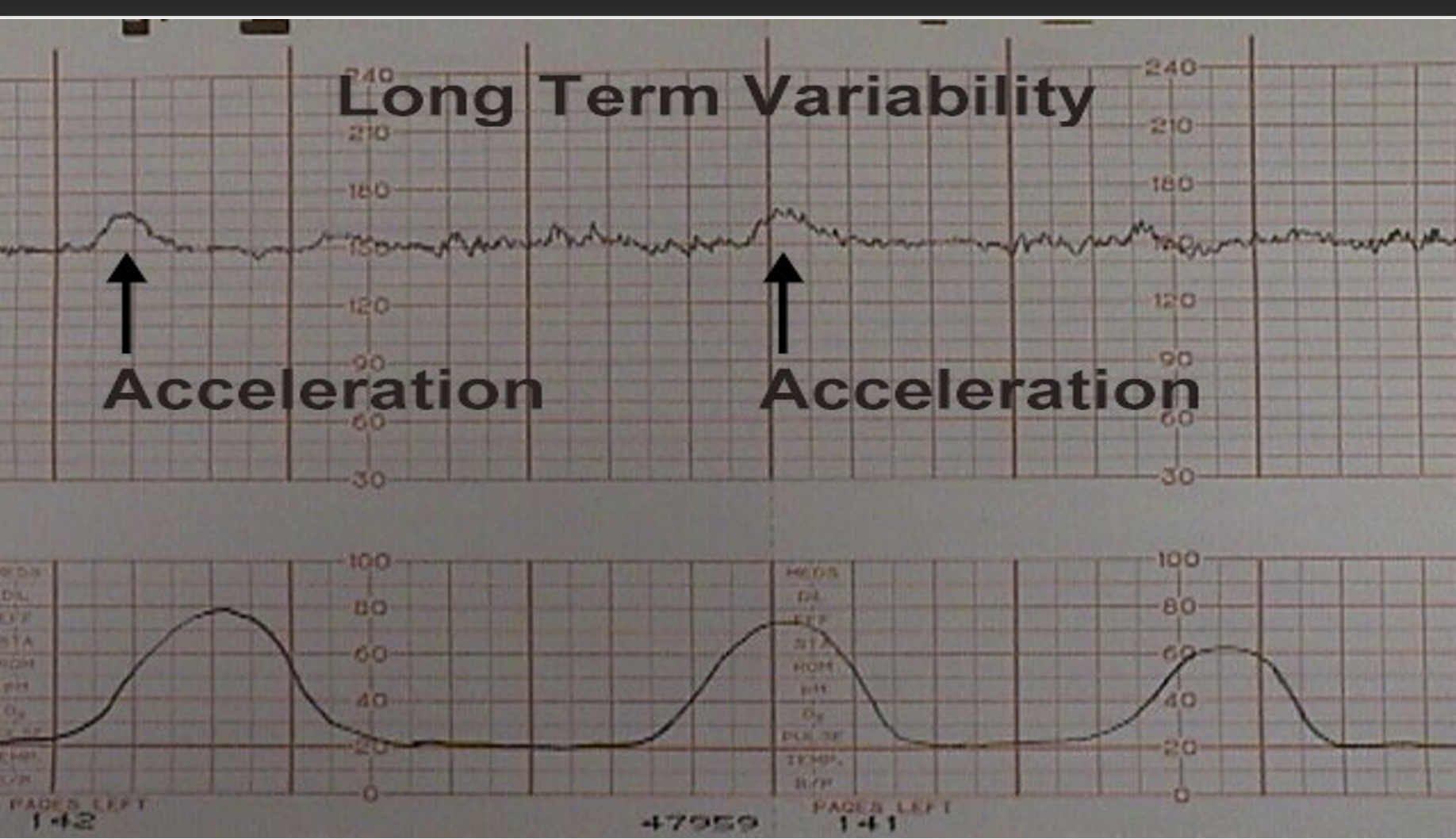
Accelerations
Accelerations
An acceleration is an abrupt increase in FHR above baseline with onset to peak of the acceleration less than <30 seconds and less than 2-minutes in duration. The duration of the acceleration is defined as the time from the initial change in heart rate from the baseline to the time of return to the FHR to baseline.
Adequate accelerations are defined as:
<32 weeks' : >10 BPM above baseline for >10 seconds
>32 weeks' : >15 BPM above baseline for > 15 seconds
Prolonged acceleration: Increase in heart rate lasts for 2 to 10 minutes.
The absence of accelerations for more than 80 minutes correlates with increased neonatal morbidity.
Fetal scalp stimulation can be used to induce accelerations. There is about a 50% chance of acidosis in the fetus who fails to respond to stimulation in the presence of a non-reassuring pattern. This technique should not be used to verify the absence of acidemia during a deceleration of the FHR since there is insufficient literature to support its use during a deceleration.
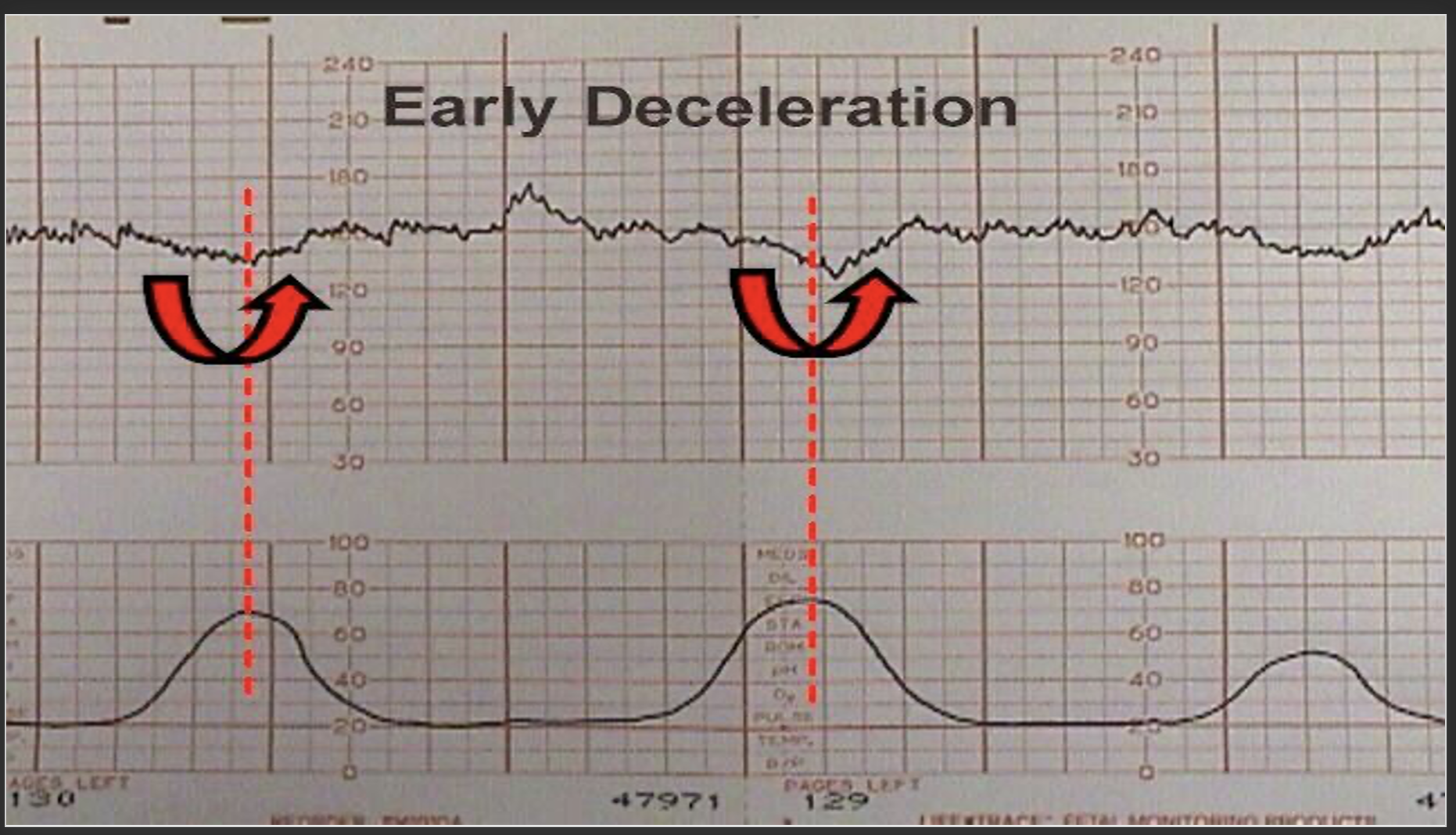
Early Deceleration
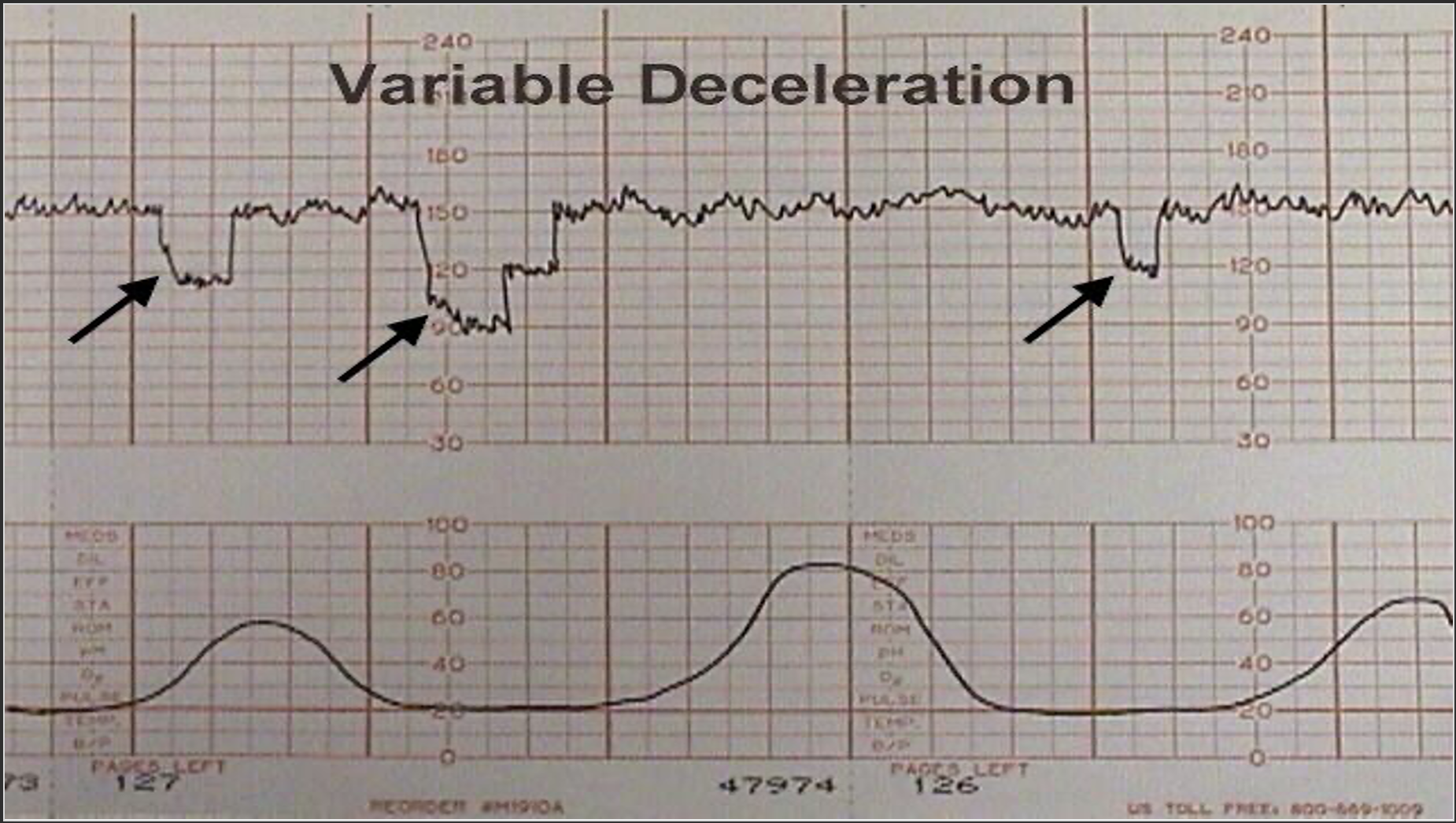
Variable Deceleration
Management of Variables
Change position to where FHR pattern is most improved.
Trendelenburg may be helpful.
Discontinue oxytocin if infusing.
Check for cord prolapse or imminent delivery by vaginal exam.
Consider amnioinfusion if r/t ROM.
Administer 100% O2 by non-rebreather face mask.
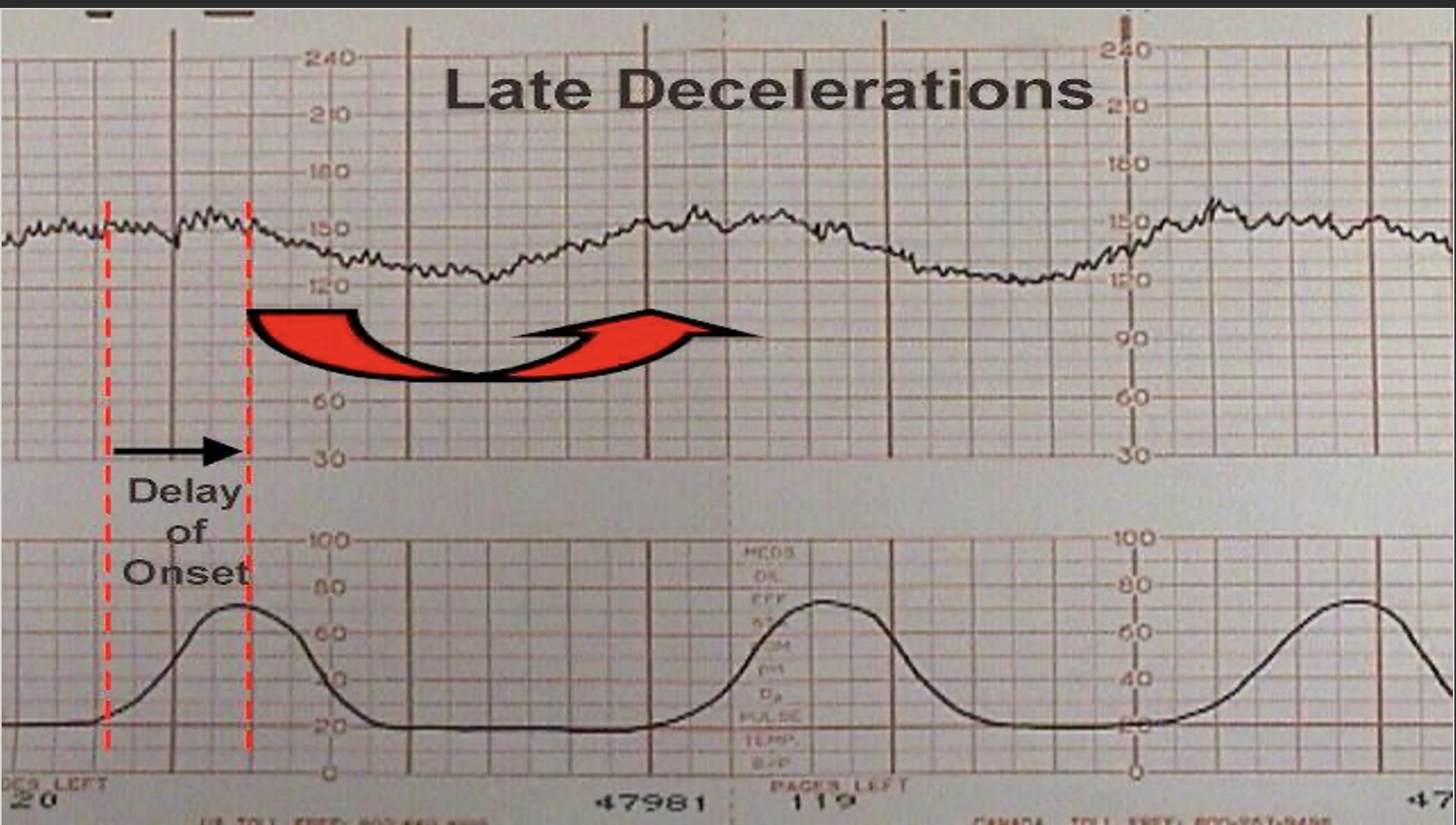
Late Decelerations
Etiologies of Late Decelerations
Excessive uterine contractions, maternal hypotension, or maternal hypoxemia.
Reduced placental exchange as in hypertensive disorders, diabetes, IUGR, abruption.
Management of Late Decelerations - These maneuvers are primarily intended to alleviate "reflex" lates.
Place patient on side.
Discontinue oxytocin.
Correct any hypotension IV hydration.
If decelerations are associated with tachysystole consider terbutaline 0.25 mg SC
Administer O2 by tight face mask.
If late decelerations persist for more than 30 minutes despite the above maneuvers, fetal scalp pH is indicated.
Scalp pH > 7.25 is reassuring, pH 7.2-7.25 may be repeated in 30 minutes.
Deliver for pH < 7.2 or minimal baseline variability with late or prolonged decelerations and inability to obtain fetal scalp pH.
The observation of recurrent late decelerations with minimal or absent variability should lead to consideration of expeditious delivery (C/S) unless the abnormal results are believed to be the result of a reversible maternal condition such as diabetic ketoacidosis or pneumonia with hypoxemia.
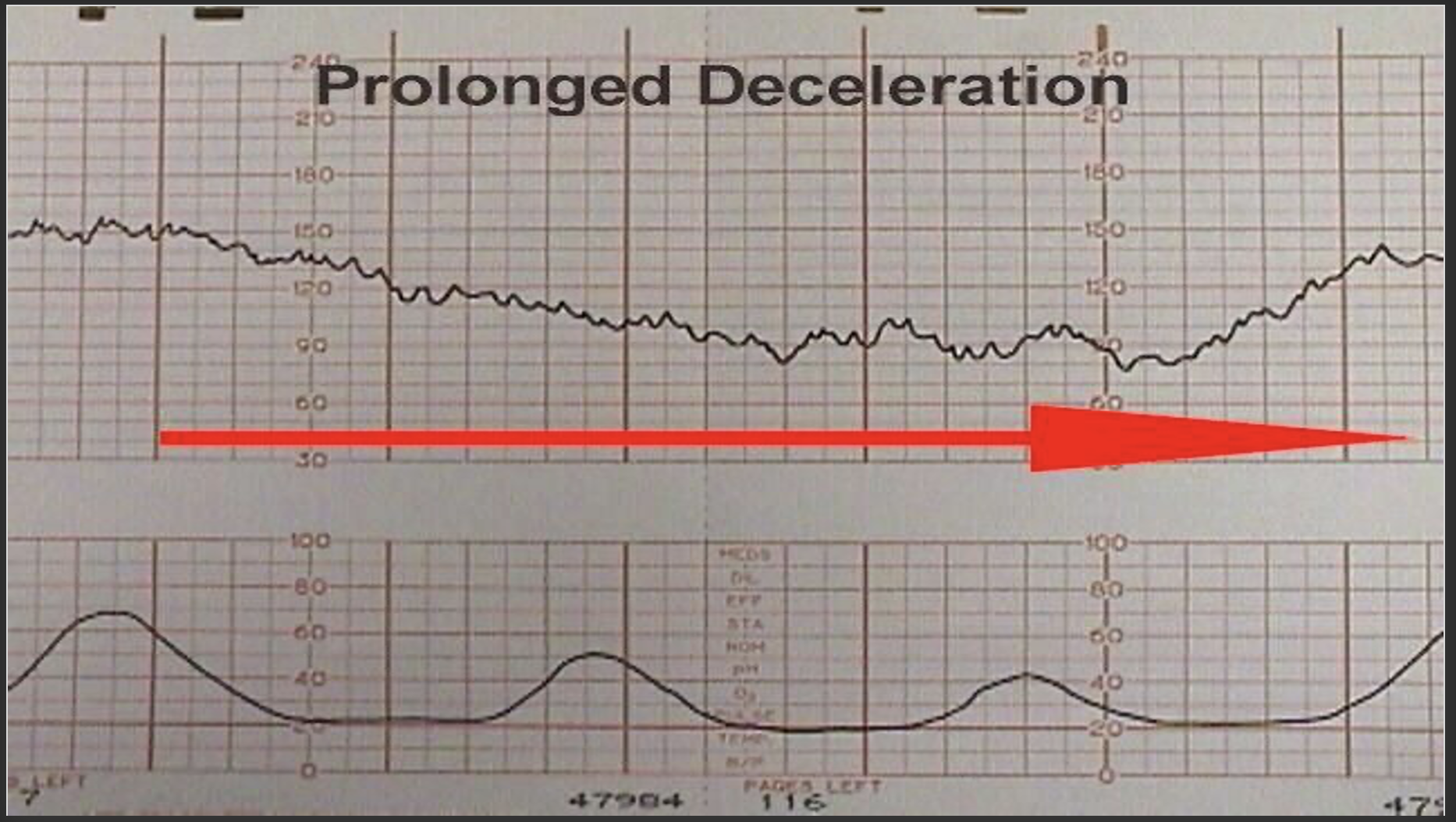
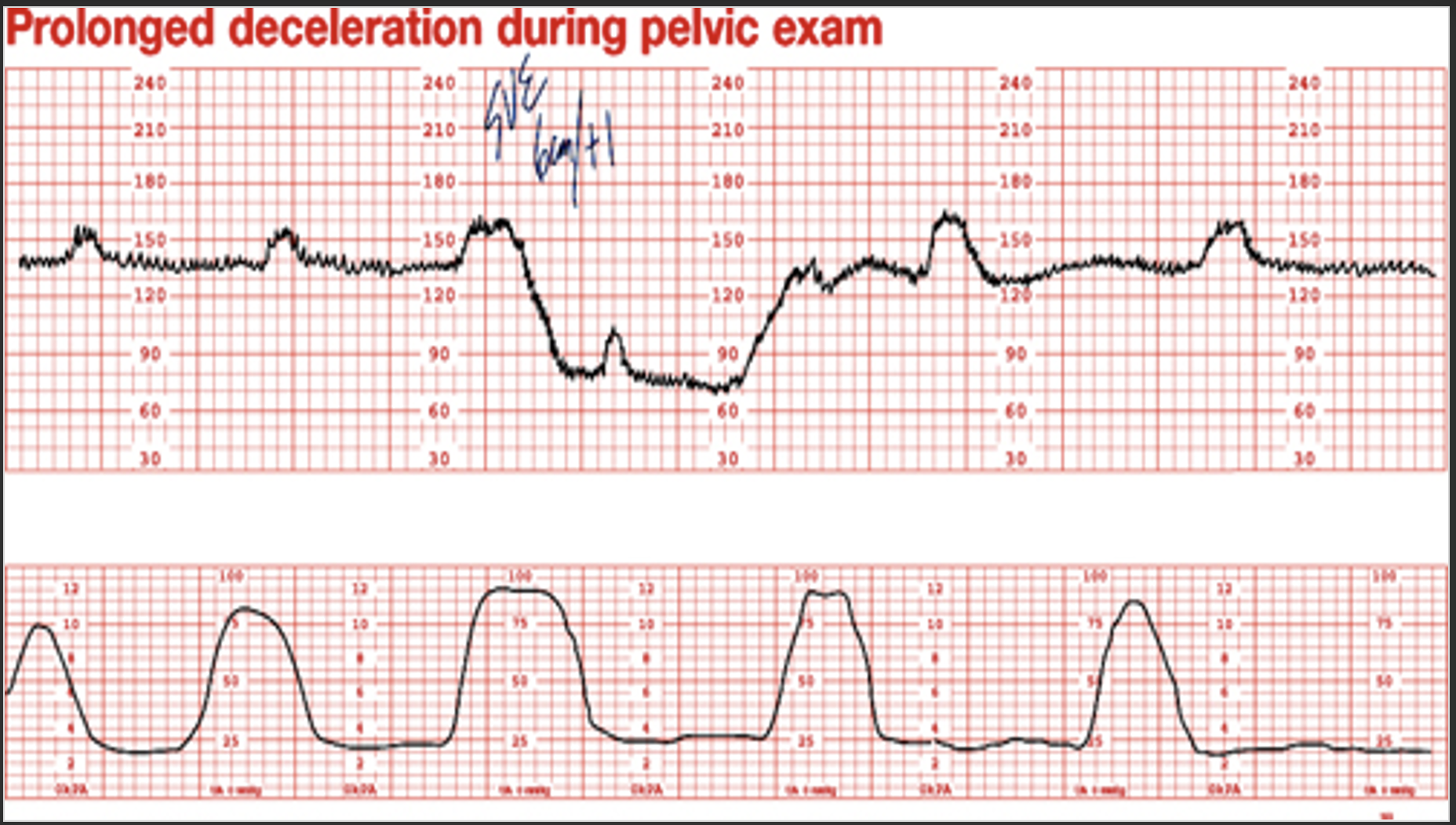
Prolonged deceleration
Prolonged deceleration : A decrease in FHR of > 15 beats per minute measured from the most recently determined baseline rate. The deceleration lasts >= 2 minutes but less than 10 minutes.
Etiologies: Maternal hypotension, uterine hyperactivity, cord prolapse, cord compression, abruption, rapid decent of the fetal head, and maternal seizure
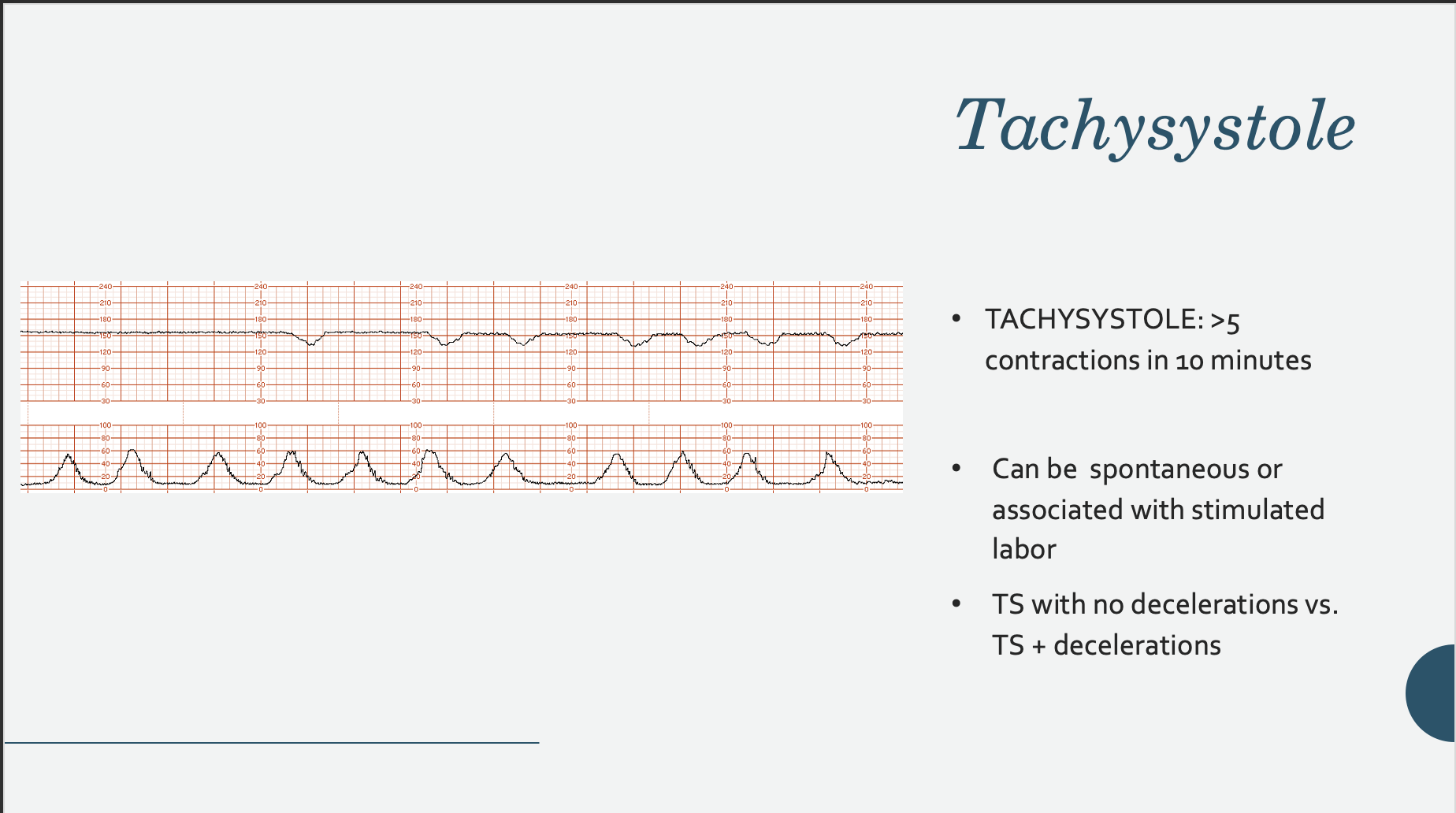
Tachysystole
Uterine Contractions
Uterine contractions are quantified as the number of contractions present in a 10-minute window, averaged over 30 minutes.
Normal: 5 or less contractions in 10 minutes, averaged over a 30-minute window.
Tachysystole: More than 5 contractions in 10 minutes, averaged over a 30-minute window. Applies to both spontaneous or stimulated labor (Pitocin/oxytocin). Tachysystole should always be qualified as to the presence or absence of associated FHR decelerations.
Interpretation of FHR Patterns
Goal: assess adequacy of fetal oxygenation during labor
Described as: contraction frequency , duration, intensity ( per patient or palpation),how long that contraction pattern has been occurring, stage of labor, and earlier FHR pattern
Understanding of FHR physiology and influences on FHR is essential
Nursing Care
Fetal Heart Rate Patterns
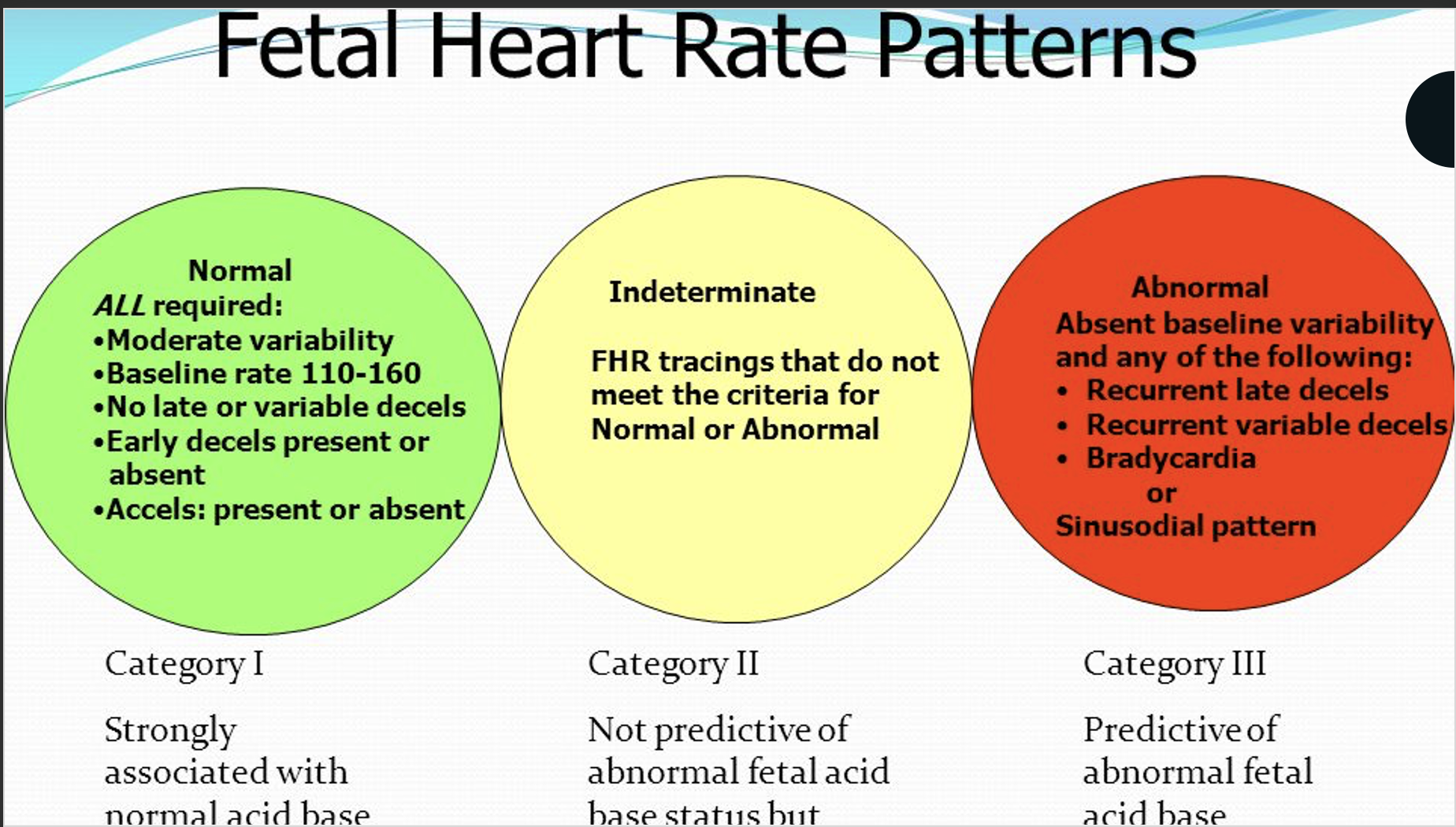
Three-Tier Fetal Heart Rate Interpretation System
Category I : Normal
The fetal heart rate tracing shows ALL of the following:
Baseline FHR 110-160 BPM, moderate FHR variability, accelerations may be present or absent, no late or variable decelerations, may have early decelerations.
Strongly predictive of normal acid-base status at the time of observation. Routine care.
Category II : Indeterminate
The fetal heart rate tracing shows ANY of the following:
Tachycardia, bradycardia without absent variability, minimal variability, absent variability without recurrent decelerations, marked variability, absence of accelerations after stimulation, recurrent variable decelerations with minimal or moderate variability, prolonged deceleration > 2minute but less than 10 minutes, recurrent late decelerations with moderate variability, variable decelerations with other characteristics such as slow return to baseline, and "overshoot".
Not predictive of abnormal fetal acid-base status but requires continued surveillance and reevaluation.
Category III: Abnormal
The fetal heart rate tracing shows EITHER of the following:
Sinusoidal pattern OR absent variability with recurrent late decelerations, recurrent variable decelerations, or bradycardia.
Predictive of abnormal fetal-acid base status at the time of observation. Depending on the clinical situation, efforts to expeditiously resolve the underlying cause of the abnormal fetal heart rate pattern should be made.
Second Stage of Labor
Full dilation through birth of neonate
Urge to push (rectal pressure)
Promote effective pushing
Closed glottis (discourage breath-holding)
Open glottis (encourage release of air)
Position of comfort - side, hands and knees, standing, squatting
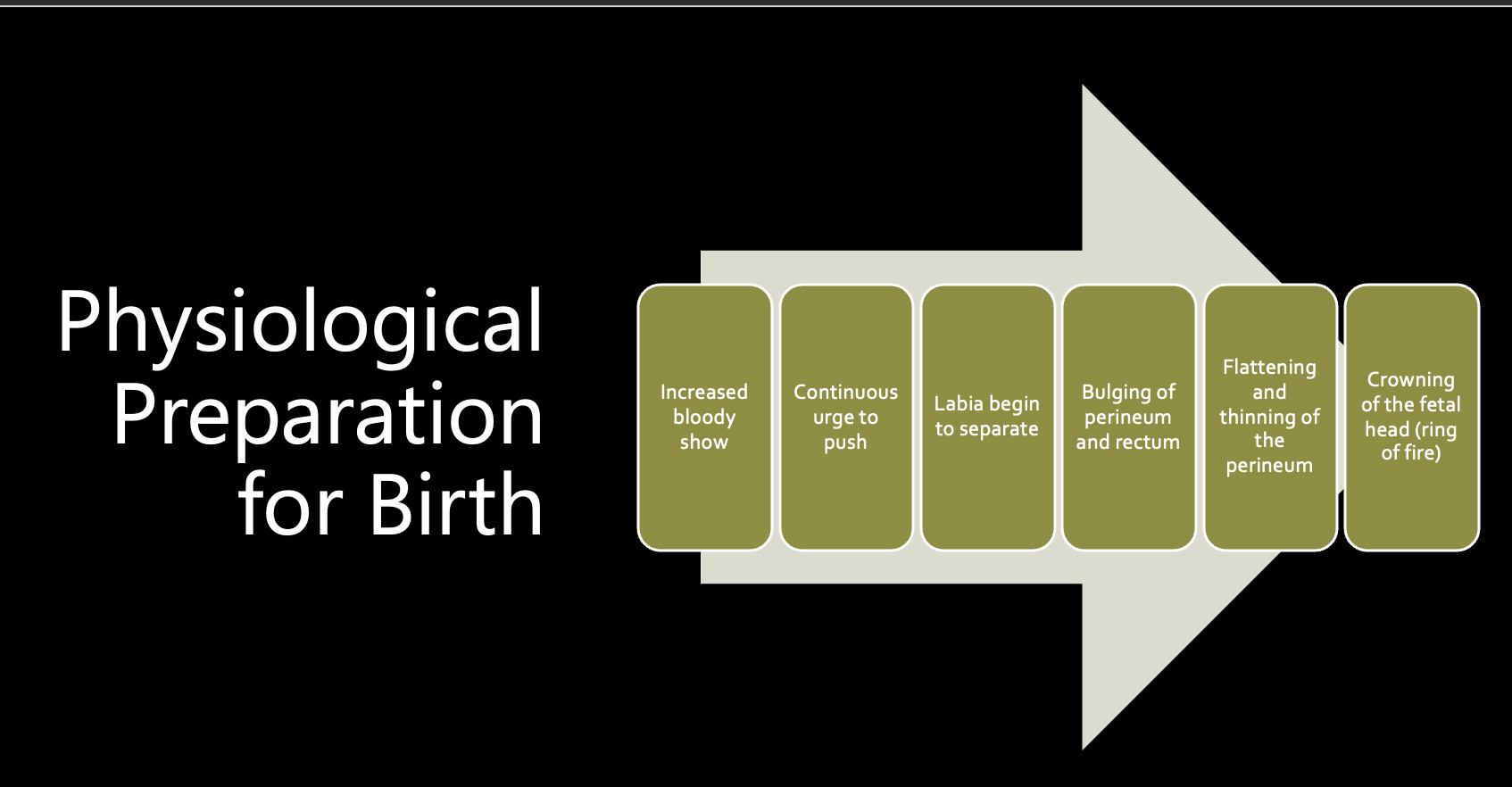
Physiological Preparation for Birth
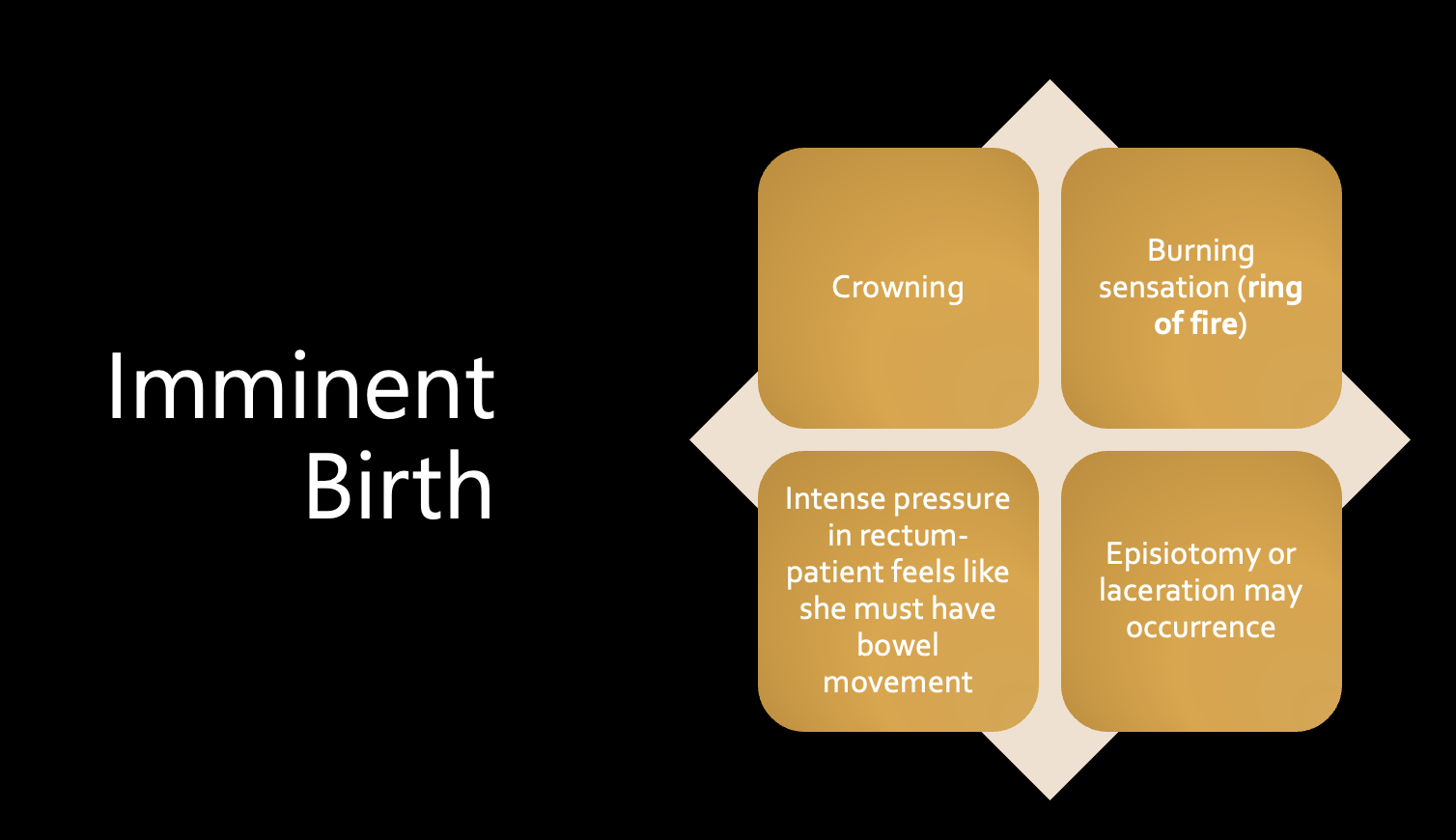
Imminent Birth
Seven Cardinal Movements of Birth
The typical sequence of positions assumed by the fetus as it descends through the pelvis during labor and delivery
Every- Engagement
Day- Descent
Fine- Flexion
Infants- Internal rotation
Enter-Extension
Eager &- External rotation
Excited- Expulsion
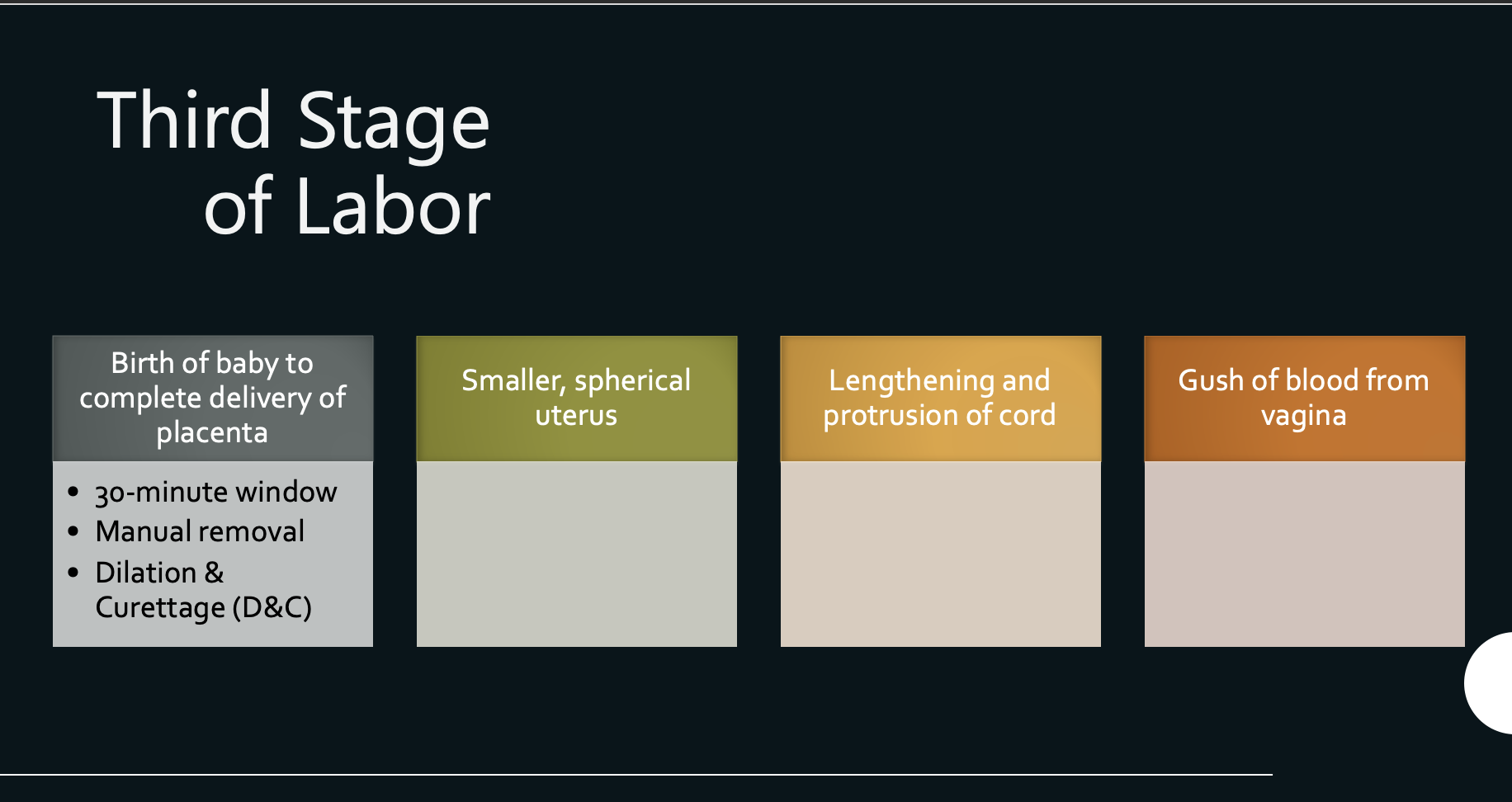
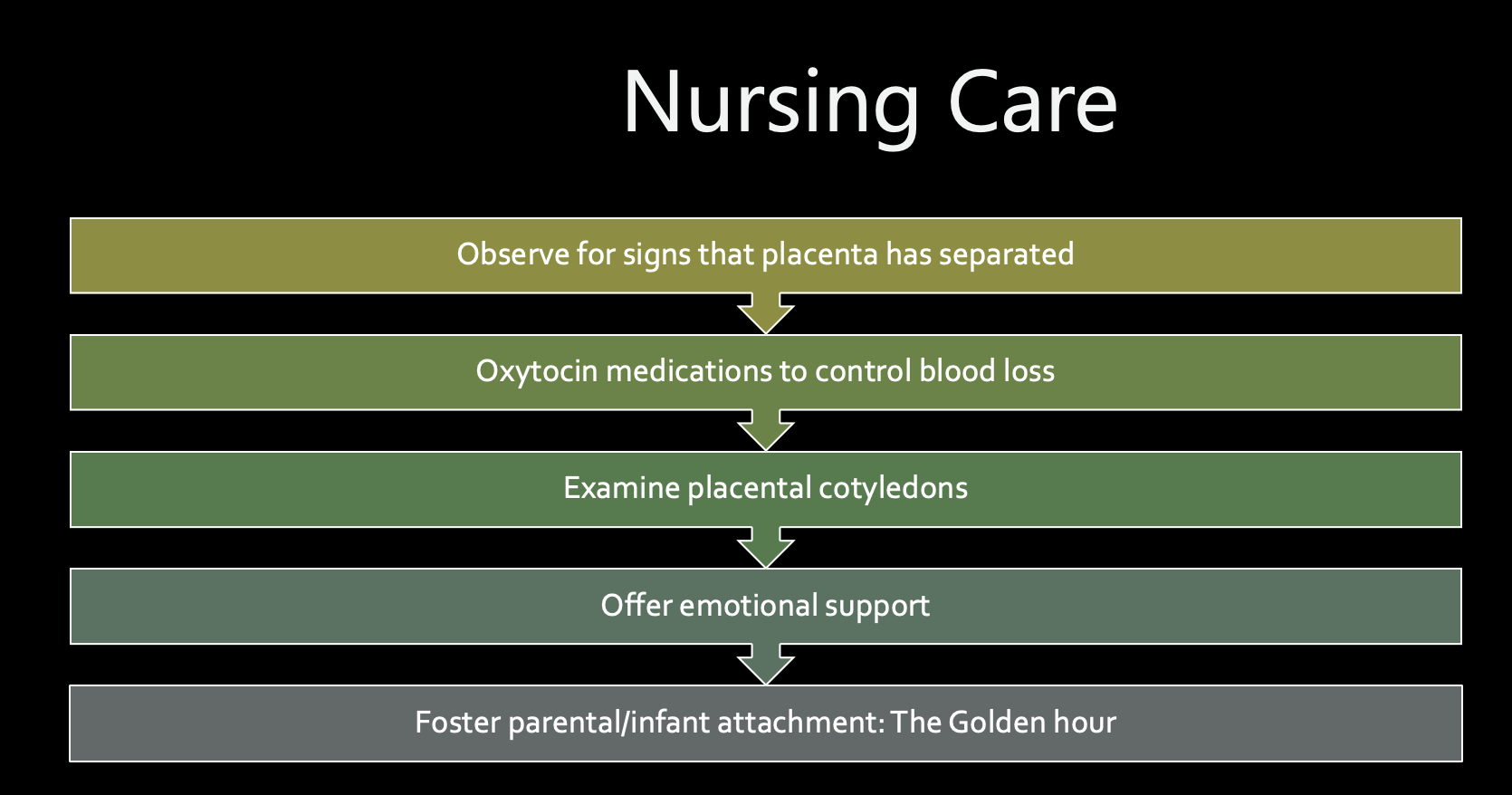
Third Stage of Labor
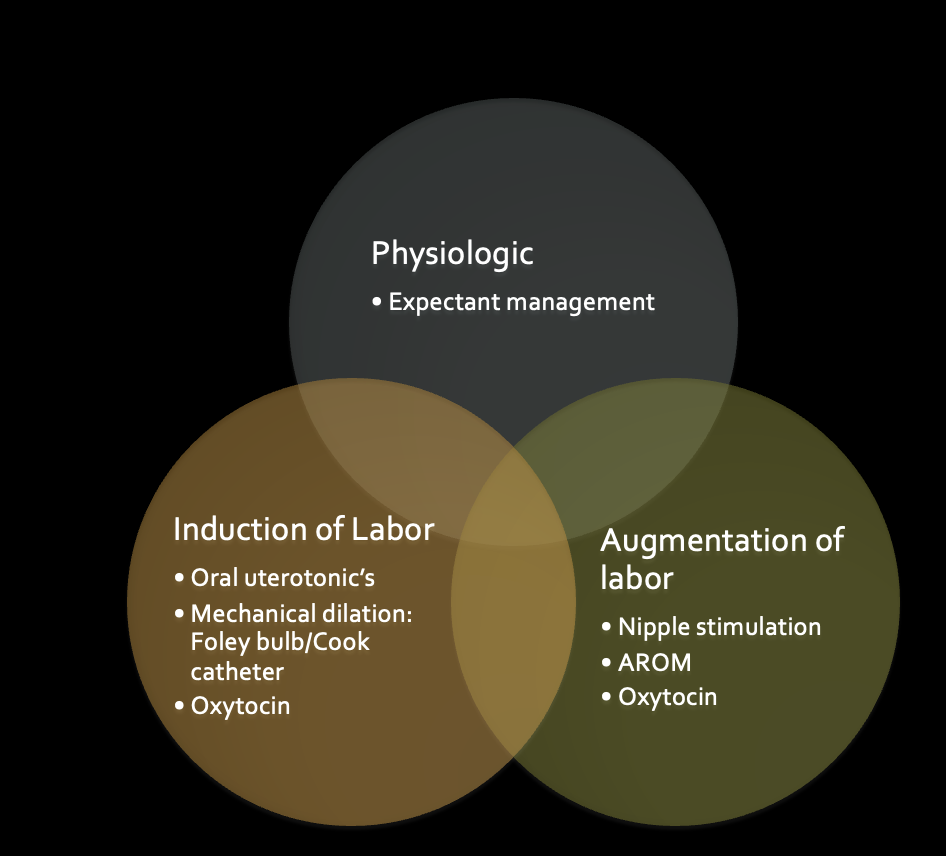
Physiologic vs. Intervention
Eating and Drinking During Labor
Early labor light meals
Active labor clear fluids
Scheduled C/S- NPO
Nursing Care
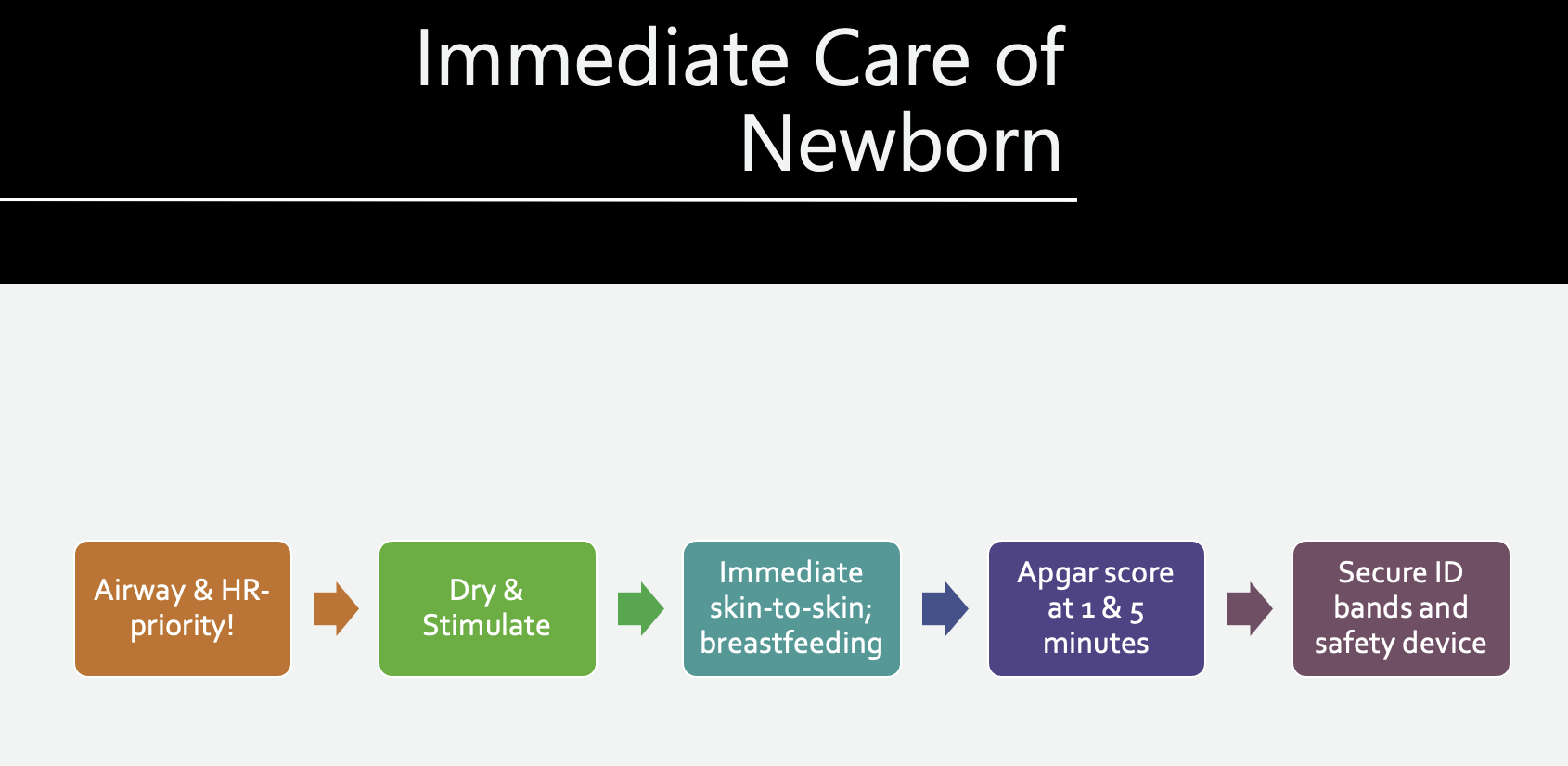
Immediate Care of Newborn
Fourth Stage of Labor