Components of the anaesthetic machine
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
what oxygen gas supply sources are available? (3)
cylinder, piped, oxygen concentrator
how are medical air and nitrous oxide supplied ?
by cylinder or pipeline
How are gas cylinders secured?
in yokes
what connects the cylinder to the regulator and what does it prevent?
a pin-index system which prevents accidental connection of a cylinder to the wrong machine yoke
describe the cylinder valve block
has an arrangement of holes, which fit pins protruding from the yoke
what is the regulator attached to?
schrader socket which plugs into the anaesthetic machine
what do pressure regulators and gauges do ?
the pressure regulators reduce the high pressure delivered from the cylinder preventing damage to the anaesthetic system and the patient.
the pressure gauage indicates the gas volume remaining in the cylinder.
What do the flow control valves separate ?
the high pressure circuit and low pressure circuit
where is the high pressure circuit ?
upstream of the flow control valves
Where is the low pressure circuit
downstream of the flow control valves
where does the gas mixture go once it leaves the tubes?
enters a common gas manifold and is directed to a calibrated vaporiser or directly to the common gas outlet, total fresh gas flow travels this way
what do the flow control valves do
control, measure and indicate the rate of gas passing through them to the patient
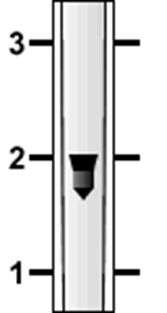
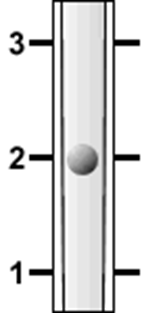
what does the ascending flow of gas support
a free moving float in a transparent tapered tube.
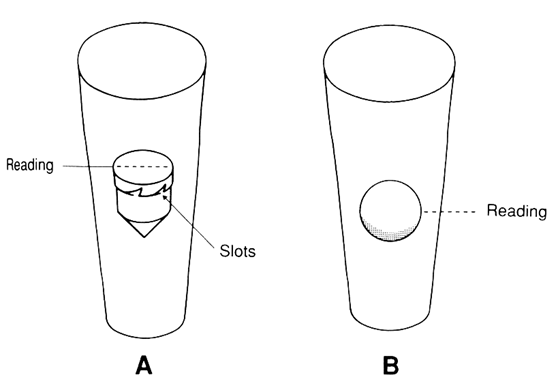
how is flow rate measured and read
The flow rate is measured in litres per minute (L/min) and is read from the top of the bobbin or the equator of the sphere
What happens when gas flows through the calibrated vaporiser?
a precise amount of volatile anaesthetic agent is mixed with the carrier gas, dependent on setting.
How do you read the gas flow rate ?
read from the middle of the float OR the top of the float dependent on where the mark is, the float rotates to show you it is not stuck
what can cause the flow-meter to not work accurately
dirt, static electricity, unlevelled surface
what are common gas outlets ?
breathing systems, ventilators, and oxygen supply - masks, usually on the right of the machine, can be fixed or swivelled
Why do we need emergency oxygen flushes?
oxygen concentrators are unable to supply high enough flow of oxygen for the flush to work, so they require back-up from cylinders
how do emergency oxygen flushes work?
they receive oxygen directly from the pipeline thus bypassing the vaporiser. don't use if patients are connected to the breathing system. too high pressure
patients are connected to the breathing system as the high pressure of the gas causes barotrauma leading to pneumothorax/ pneumomediastinum and potentially to cardiovascular collapse.
how many vaporisers be used at a time
only 1. and they are agent specific
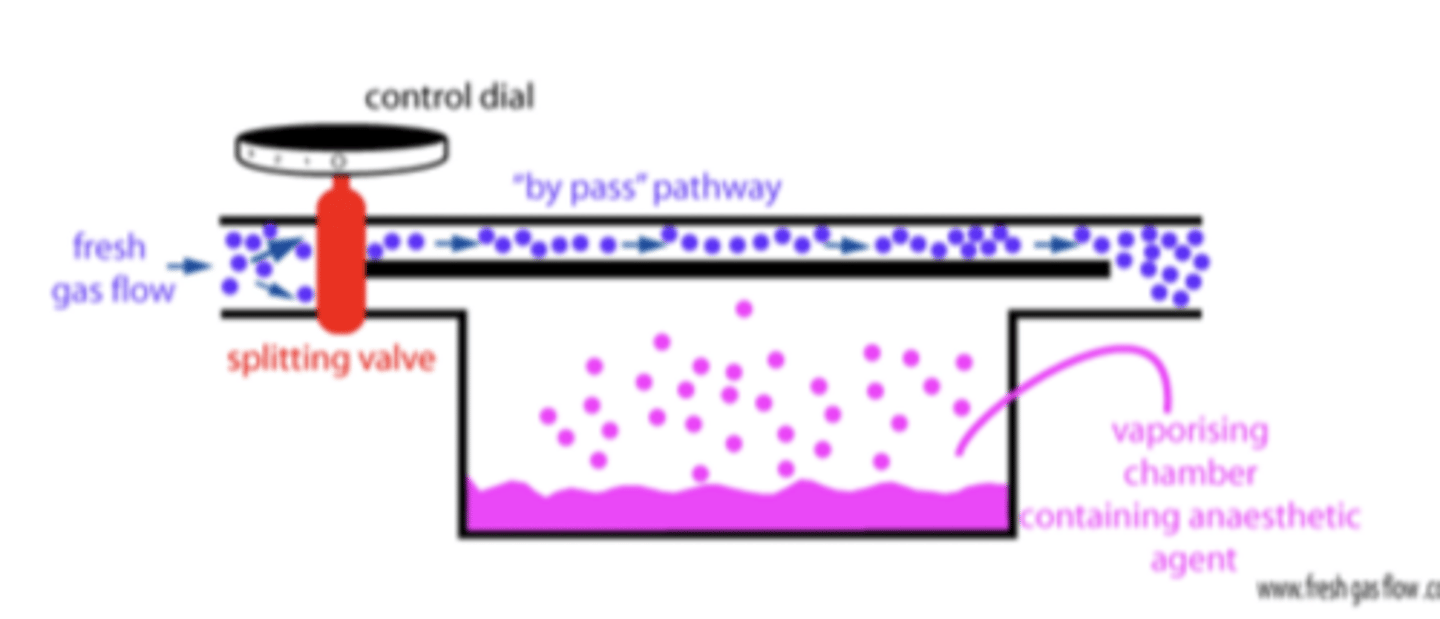
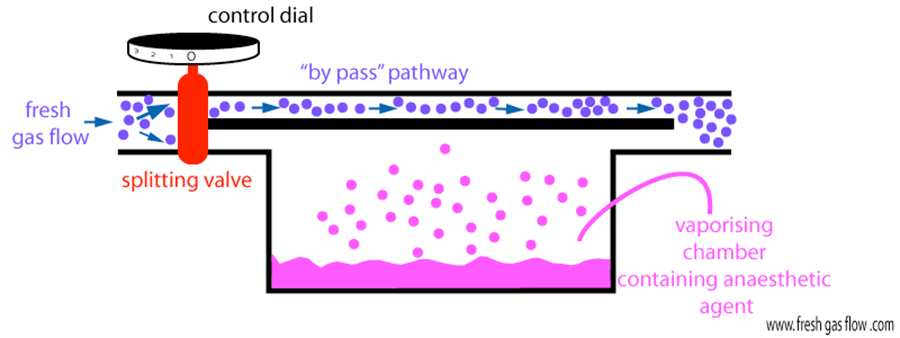
explain how vaporisers work
control dial is turned on
gas enters the through the vaporiser inlet
gas then passes a fixed flow splitter - which divides it into 2 streams
1. the bypass chamber flow passes a variable restrictor temperature-compensating valve, then rejoins the flow from the vaporising chamber
2. the stream that is diverted through the vaporising chamber passes through a wick system to become saturated with volatile anaesthetic vapour - the proportion of bypass to the vaporising chamber is controlled by the control dial - thereby determines the vaporiser output of volatile anaesthetic agent
describe the complications that can arise in regard to the vaporiser.
complications may lead to under or overdosing of volatile anaesthetic agent:
- tipping of vaporisers - results in movement of liquid to the bypass chamber and this may mean very high concentrations of volatile concentrations are released to the patient.
- filling errors - keys were developed to minimise this
what is the first thing to check on the anaesthetic machine before use?
ensure the oxygen concentrator is plugged into an electric wall socket and the lead is plugged into the back of the machine. check the cylinder is securely attached to the regulator - this is for the emergency oxygen button
what is the second thing to check on the anaesthetic machine before use?
switch on the oxygen concentrator and allow it to warm up for 5 minutes - blue light comes on when ready, red light indicates no power supply
check isolation ball valve is in the isolate position. only opened in powercut
what is the third thing to check on the anaesthetic machine before use?
turn on oxygen clinder and ensure sufficient gas remains - use the cylinder key turn clockwise, see pressure gauge

what is the fourth thing to check on the anaesthetic machine before use?
check the emergency o2 flush when cylinder is connected - press red button on the common outlet and audible gas flow should occur. this can be used to purge the system of anaesthetic, without patient connected
what is the fifth thing to check on the anaesthetic machine before use?
flowmeter on concentrator and anaesthetic machine - turn the anaesthetic flow meter up and the concentrator will also go up and vice versa with down
turn the anaesthetic flowmeter to the calculated fgf for your patient and breathing system and don't change it - it will not register flow until the anaesthetic machine is on
how do you turn the flow meter on and off
To turn flowmeter on, gently turn knob anticlockwise
To turn flowmeter off, use gentle pressure clockwise
Use light finger pressure only – never apply any force)
what should the flowmeter concentrator be left open at
at about 5L/min
and should not be adjusted for the entire procedure/day.
The concentrator flowmeter will not register any flow until the anaesthetic machine flowmeter is turned on.
what is the sixth thing to check on the anaesthetic machine before use?
check that the vaporiser dial lock is in the locked position to allow gas to pass though it. check vaporiser has sufficient agent and smooth dial movement - when gas is off!
what is the seventh thing to check on the anaesthetic machine before use?
attach chosen breathing system and scavenging. check breathing system for leaks. leave APL valve open once you have checked this
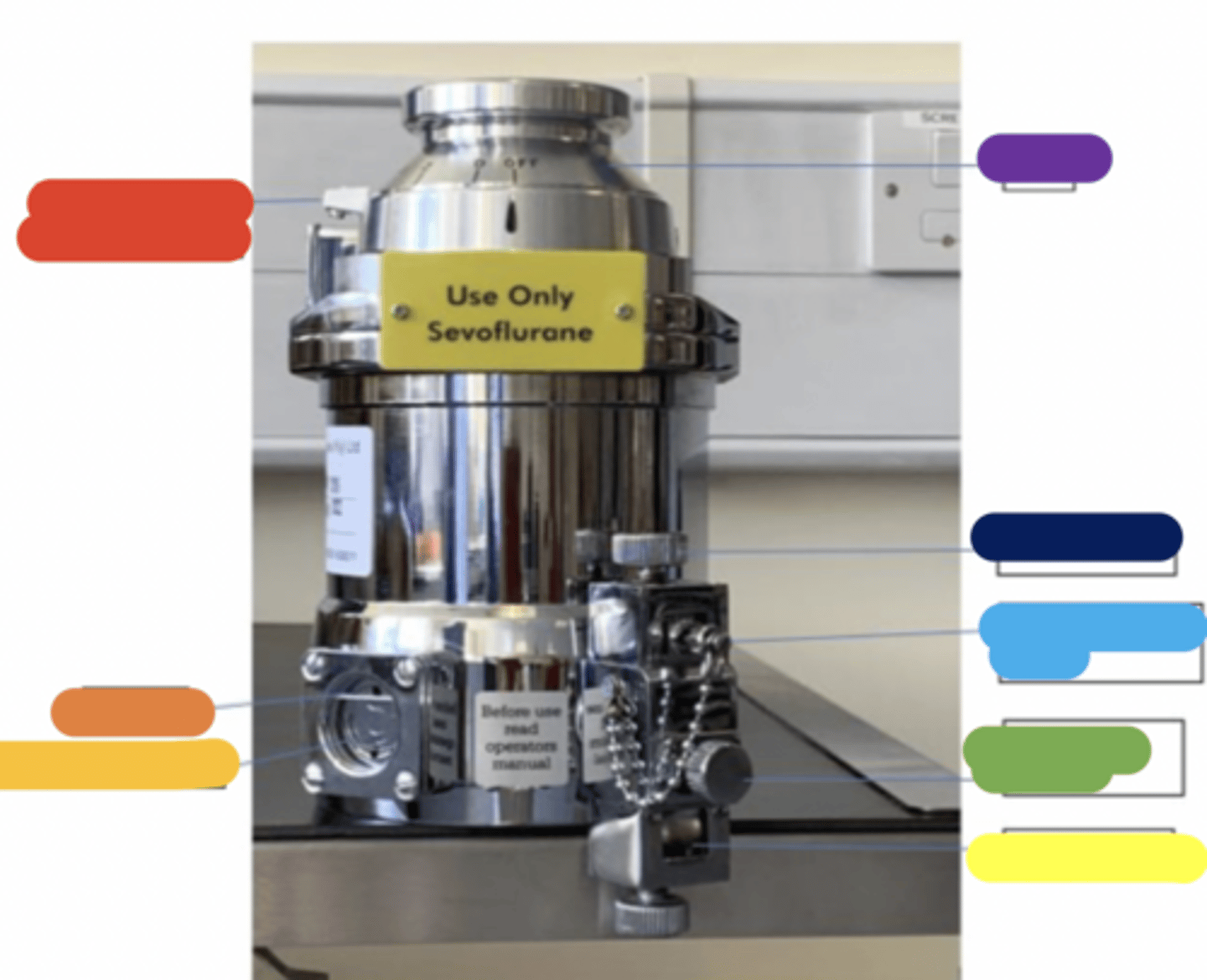
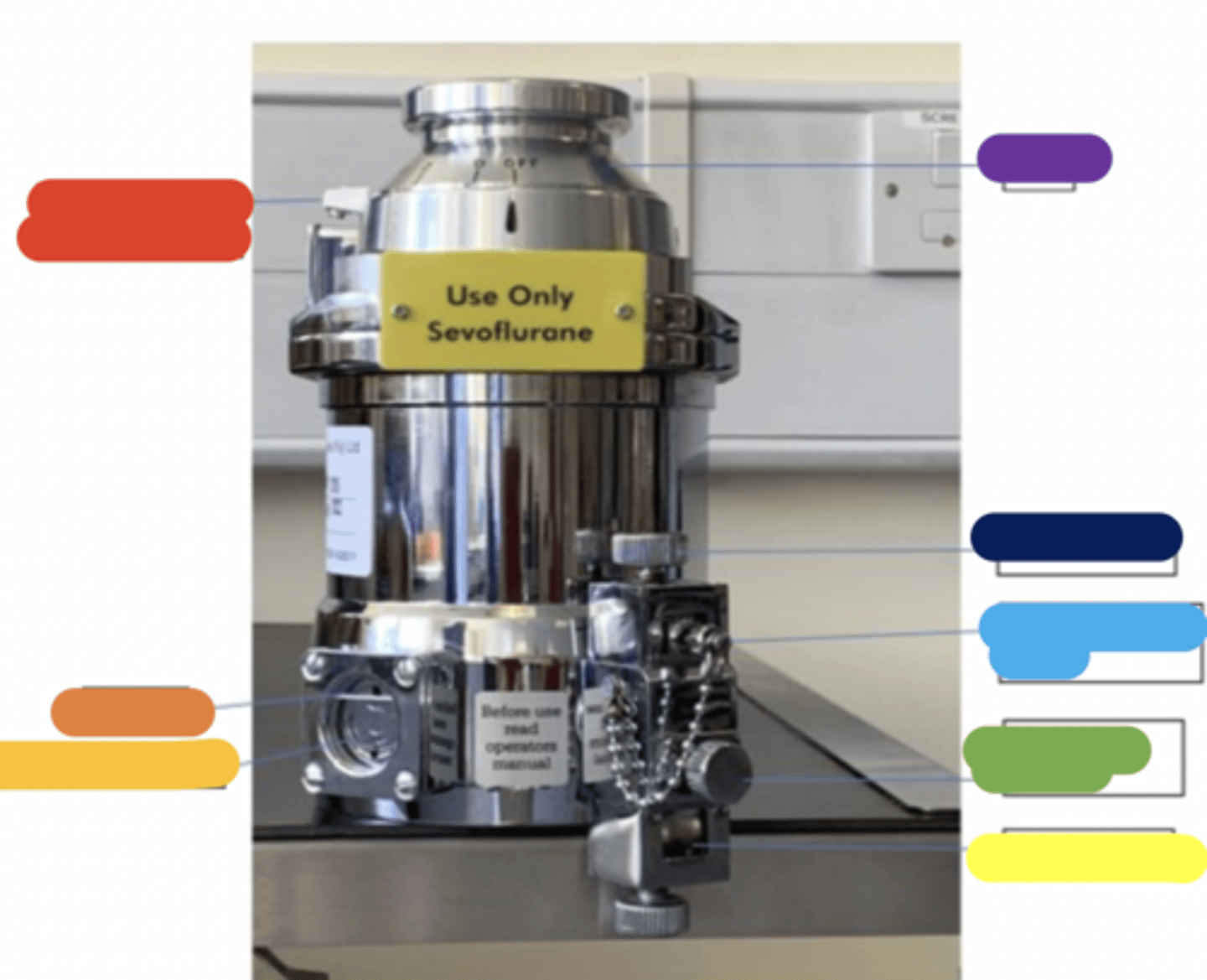
Label the vaporiser
red = depress lever to release dial
orange = fill line
gold = viewing chamber
yellow = draining port
green = loosen to drain
light blue = filling port and block
dark blue = filling knob
purple = dial
what should be done at the end of the session and at the end of day
At end of session
Anaesthetic machine flowmeter should be left at 0.1L/min.
Concentrator flowmeter should be left on (at 5L/min although it will not register a flow)
At end of day
Leave flowmeters turned on as above before switching off the concentrator at the on/off Power button
what should eb done if mains power is lost
Supply needs to be switched from concentrator to cylinder by turning the isolation ball valve open i.e. horizontal, (parallel to tubing). The cylinder will need to be switched on using a spanner.
how do you refill a vaporiser
Select the correct key filler
Take the lid off the bottle and screw on the key filler
Remove the upper most block from the vaporiser filling port by unscrewing the knob on top of the filling port. Insert the key (keeping the bottle lower than the key), making sure the holes are aligned between the key and in the filling port.
Screw down the knob you first loosened, then invert and lift up the bottle of volatile agent. The liquid should now flow into the vaporiser.
Fill up the chamber to the top line. Do not overfill. Nothing should leak out!
Lower the bottle, unscrew the knob, take out the key, re-insert the block and screw up the knob.
The lower block is for draining the vaporiser
what colour is iso adn what is sevo
iso= purple
sevo= yellow
what is intermittent positive pressure ventilation (IPPV)
is the process of manually or mechanically ventilating a patient.
non rebreathing systems
lack
bain
y piece
what size patients can go on lack
over 10kg
It is also available in a mini form for animals 2-10kg (smooth bore tubes-less turbulence and resistance)
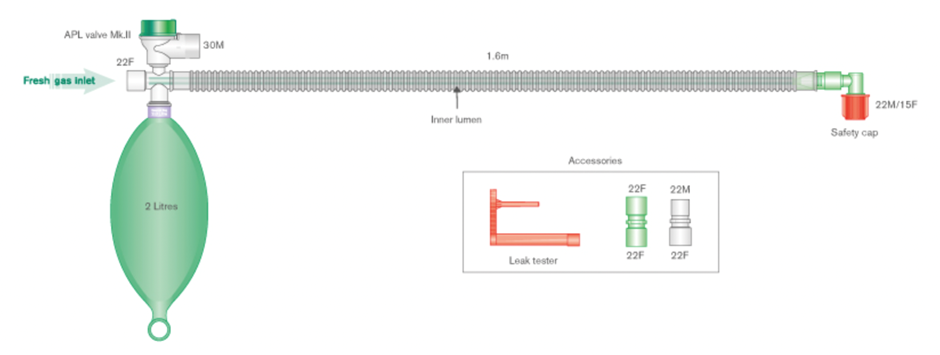
describe the lack
It is a parallel system i.e. has two tubes, one inspiratory (often green) and one expiratory (clear). The adjustable pressure limiting (APL) valve is on the expiratory limb and the reservoir bag is situated on the inspiratory limb.
what is the fgf on the lack system
Fresh gas flow is equal to patient minute volume i.e. 1 x MV.
why is the lack not efficient for ongoing IPPV
as rebreathing of carbon dioxide can occur at 1 x MV
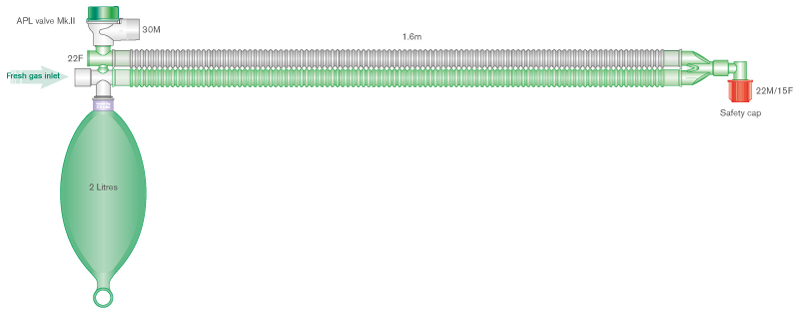
what is this one
parallel lack breathing system
what size patient can go on bain
over 10kg
describe the bain
It is a coaxial system (tube within a tube). The inner narrow tube delivers fresh gas to the patient and the wider corrugated tube conveys the gas away from the patient to the reservoir bag and expiratory (APL) valve so in this system both the APL valve and the reservoir bag are on the expiratory limb.
what is the fgf for the bain
rebreathing is mostly eliminated with flow rates of 2.5 x MV in spontaneously breathing patients.
which non rebreathing system is preffered for IPPV
bain
whats this
bain
what size patients can go on t piece
under 10kg (is a low resistance system)
what is the fgf for t piece
Gas flow rates of 2.5 x MV are sufficient to prevent rebreathing.
why is positioning important for t piece
Twisting of the reservoir bag is a common and potentially fatal complication so careful positioning of the system is important
can you do ippv with t piece
yes
whats this
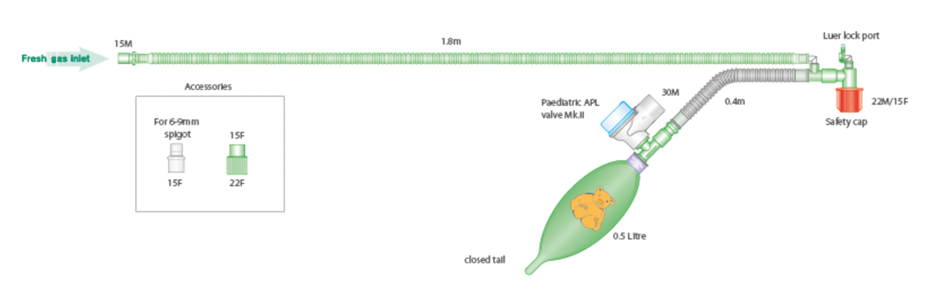
t piece
how do you calculate FGF
MV X System factor
what d rebreathing systems contain
These systems contain soda lime, a carbon dioxide absorbent, so lower fresh gas flows can be used.
what system is the circle
rebreathing
what are pros and cons of the circle
The circle conserves heat and moisture and anaesthetic gases.
However, circles impart more resistance to ventilation.
what are the basic compoenents of a circle
a Y piece,
breathing tubes (smooth or corrugated),
two unidirectional valves,
fresh gas (FG) inlet,
a APL valve,
reservoir bag
absorber.
what is the absorbent in rebreathing systems
calcium hydroxide (soda lime and barium hydroxide lime)
why should you check soda lime granules before use
can revert back to normal colour
when should you change soda lime
If inspired carbon dioxide is not being measured the soda lime should be exchanged when the indicator has changed colour in approximately two thirds of the absorbent or when a certain number of hours of anaesthesia have been completed depending on the size of the cannister.
what does active soda lime do
emit heat
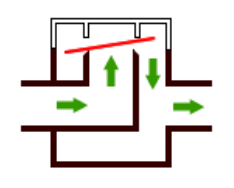
what does the turret type valves in some circle absorbers mean and what can happen to them
The unidirectional inspiratory and expiratory valves in some circle absorbers are of the turret type, in which the pressure generated by the patient's breathing causes the disc to rise and allow gas to pass in one direction only. In some circles a transparent dome allows the anaesthetist to observe the valve moving up and down.
The disc material may warp/stick and allow the valve to become incompetent. Incompetence may also be caused by the valve sticking in the open position, owing to condensation of water vapour. Incompetent inspiratory or expiratory valves will reduce the efficiency of gas circulation and result in rebreathing and consequent carbon dioxide retention.
what size patients can use circle
over 10kg
why cant standard circle absorbers used in smaller patients
because of dead space.
Small patients have small tidal volumes and not enough pressure to open the valves is generated.
The effective dead space of the Y-piece is larger than it appears.
Inevitably, some portion of the expired gas goes down the inspiratory limb of the system, and some portion of the inspired gas comes from the expiratory limb and so mixing of inspired and expired gases occurs.
what can be used for circle systems so patients less than 10kg can use them
Paediatric tubing and Y-pieces
what must the volume of the breathing bag be
greater than the patient's inspiratory capacity
what does the rateof change of anaesthetic conc in the circuit depend on
the fresh gas flow rate as a high fresh gas flow rate will achieve equilibration much faster than if a low fresh gas flow rate is used.
what is the humphrey ade circle system
This is a hybrid system which can be used in different modes and with or without sodalime. The advantage of the different modes is that it can be used in both large and small patients and can be used efficiently for spontaneously breathing animals and for controlled ventilation.
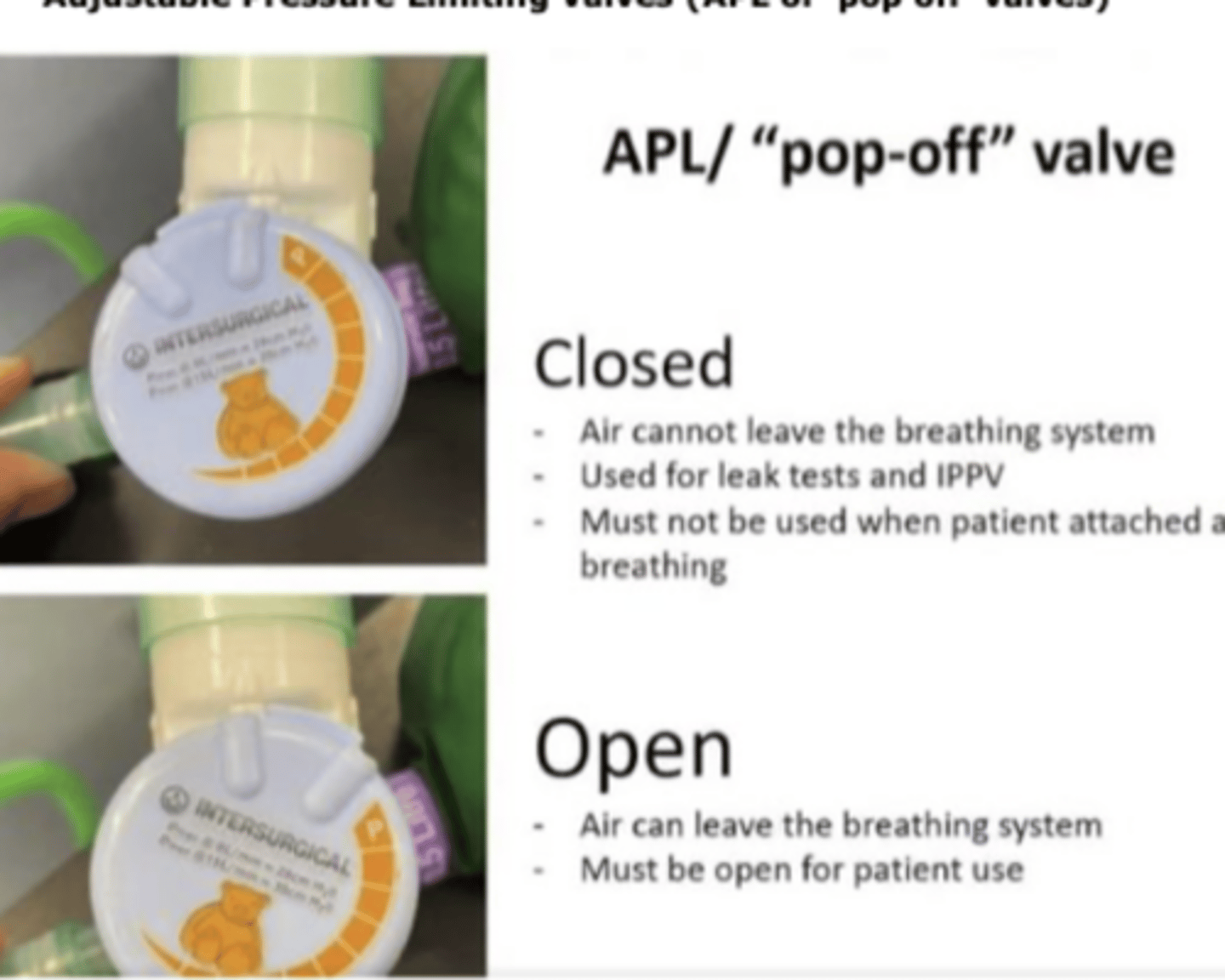
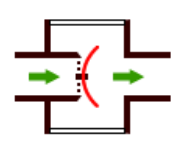
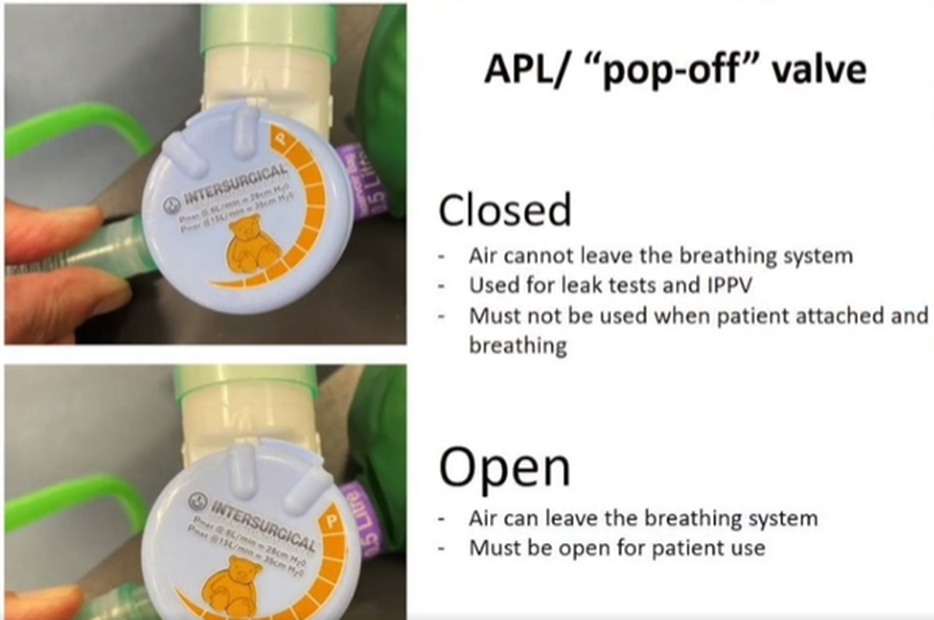
when the adjustable pressure limiting (APL) valve is closed what happens
air cant leave the breathing system
used for leak tests and IPPV
must not be used when patient is attached and breathing
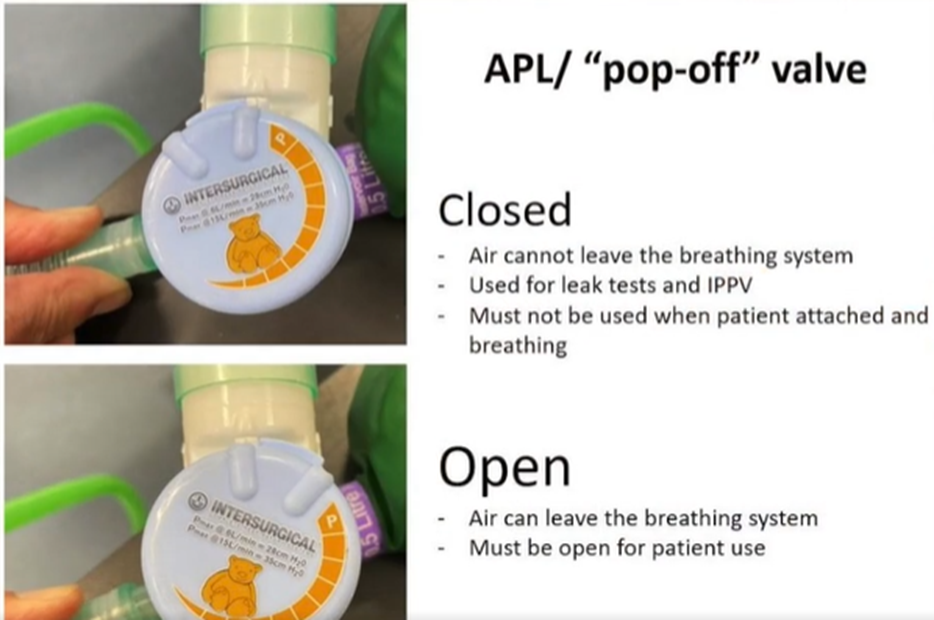
when the adjustable pressure limiting (APL) valve is open what happens
air can leave breathing system
must be open for patient use
how do you leak test the breathing system
Attach the circuit to the machine and occlude the end of the breathing system with either a cap or your hand.

Turn on the fresh gas flow meter.

Close the APL valve
Allow the bag to fill completely so there are no wrinkles remaining.

Turn the fresh gas flow off and watch the bag to ensure no creases form.
Open the APL valve.

Once you’re happy open the APL valve and squeeze the contents of the bag into the scavenge.
Remove the cap from the end of the breathing system.
what does the intial high rate of the fgf do in circle systems
The initial high rate removes nitrogen from (denitrogenates) the system and facilitates a rapid increase in end tidal volatile agent concentration which will ensure the patient remains anaesthetised as the induction agent wears off.
how do you do manual IPPV
Close the APL valve on the breathing system, pause to allow the bag to fill a bit,
squeeze the reservoir bag and watch the chest wall move, filling the lungs.
The movement of the chest wall should replicate a normal breath amount.
To close the valve, you need to turn it to the right and to open it you turn it to the left.
When you have finished delivering the breath, open the APL valve.
The chest will passively recoil.
Aim for a normal respiration rate. In most patients the time allowed for expiration will be about two to two and a half times the length of inspiration (I:E 1:2 or 1:2.5). Repeat as required.
on some circle systems what is there to provide a breath
there is a button on top of the control knob which can be held down and released to open and close the valve avoiding the need to turn the knob each time you provide a breath
On other systems, an IPPV button valve can be added to the set up allowing single button IPPV. Push the button to deliver the breath and release the button after. Repeat as required.
indicatiosn for ippv
· Apnoea
· Hypoventilation (causes hypercapnia)
· Cardiorespiratory arrest
· Thoracotomy
· Laparotomy for diaphragmatic rupture repair
· Regulation of ventilation for delicate surgical procedures
· Neuromuscular blockade
how can you monitor patients thorugh ippv
using capnography, pulse oximetry and blood pressure measurement. Gauges are also available which can be fitted into the breathing system and allow you to monitor peak inspiratory pressure (PIP).
what can hyperventilation lead to
bradypnoea or apnoea. When excessive carbon dioxide is vented the arterial partial pressure of carbon dioxide falls. Arterial carbon dioxide concentration is the main driver of respiration.
complications of ippv
- Hypercapnia from inadequate ventilation
- Hypocapnia from excessive ventilation
- Hypotension resulting from decreased cardiac output due to intrathoracic pressures decreasing venous return to the heart
- Barotrauma from over inflation
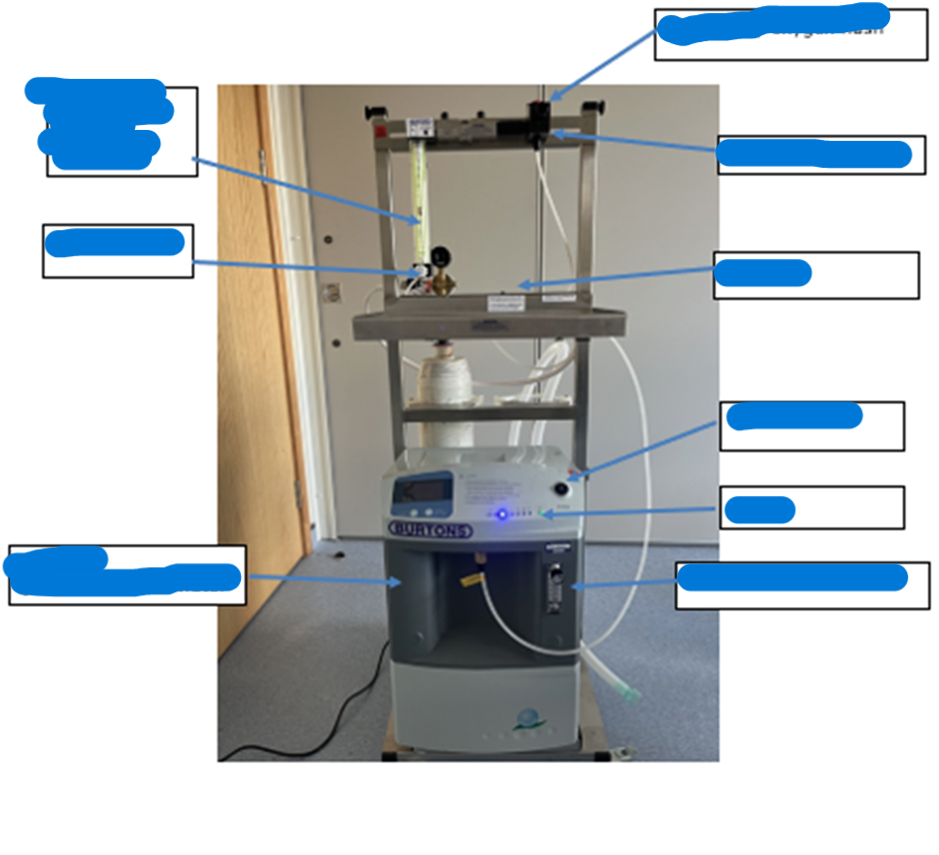
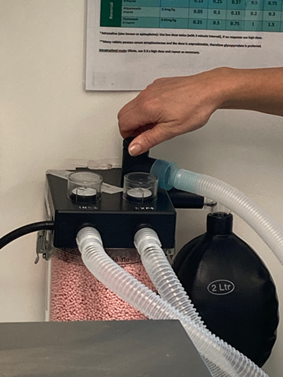
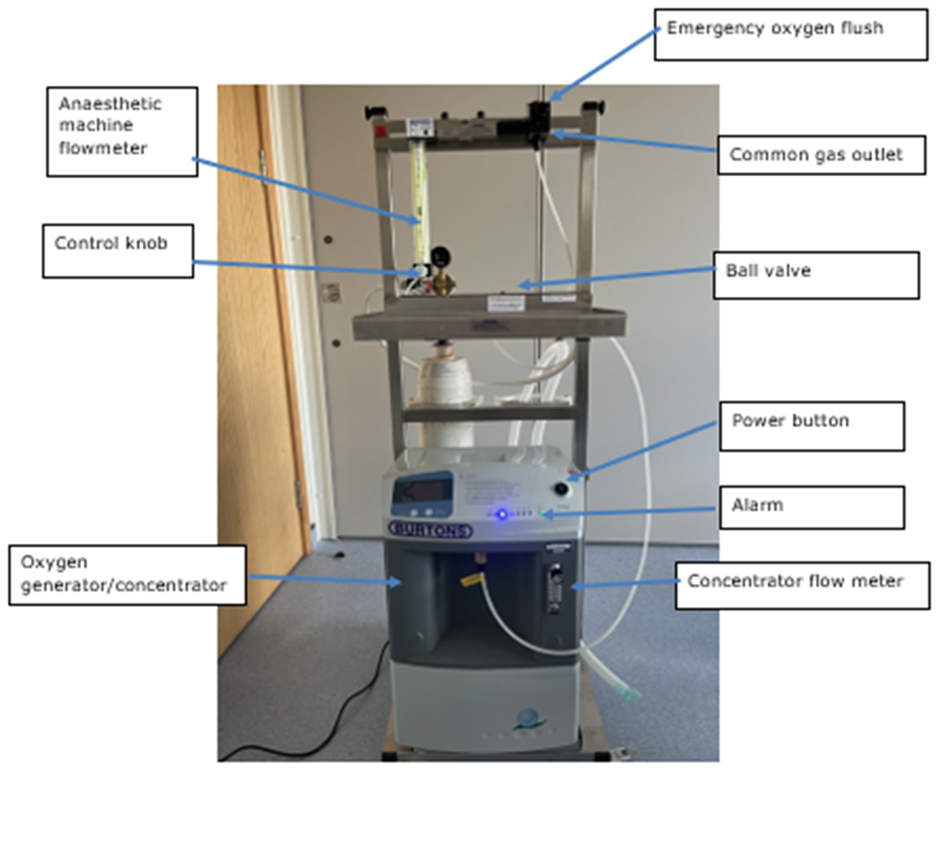
label the anaesthetic machine
emergency o2 flush
anaesthetic machine flow meter
control knob
common gas outlet
ball valve
power button
alarm
oxygen generator/ concentrator
concentrator flow meter
where is the oxygen cylinder and pressure guage

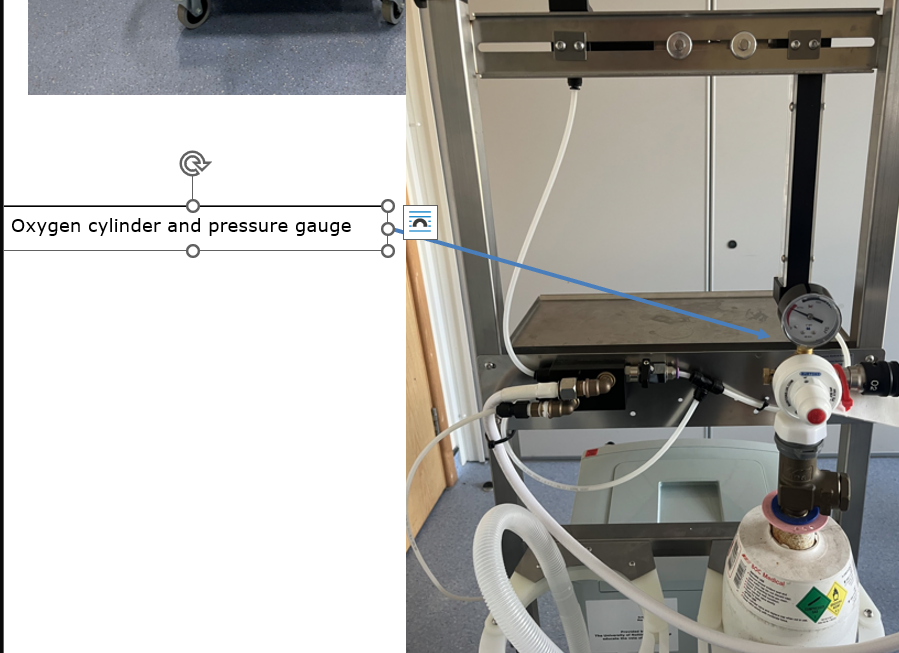
when is the ball valve isolated/ closed
when using concentrator (with O2 cylinder for emergency oxygen flush). The concentrator must be running, and the cylinder opened with the key. The lever is perpendicular to the pipe.
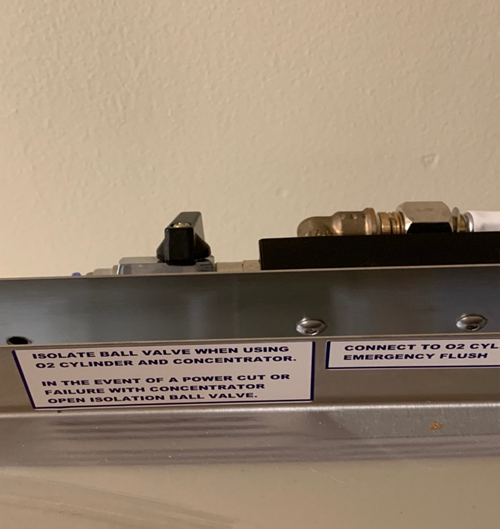
when is the ball valve open

when only using oxygen from a cylinder (e.g. during a power cut). The concentrator must not be running when the ball valve is switched to ‘open’. The lever is horizontal, or in line with the pipe.
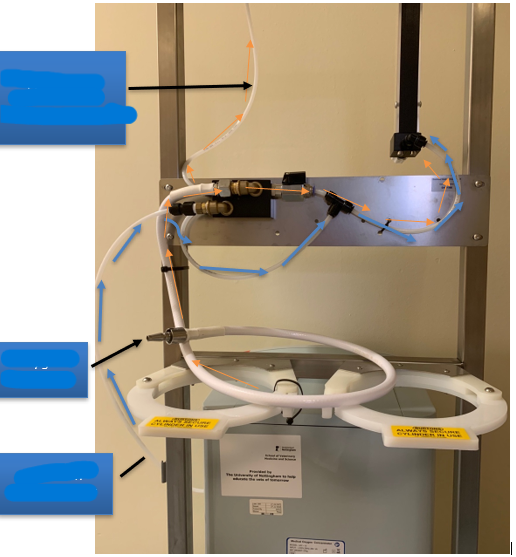
label
oxygen from cylinder to emergency button
oxygen connector
o2 from concentrator
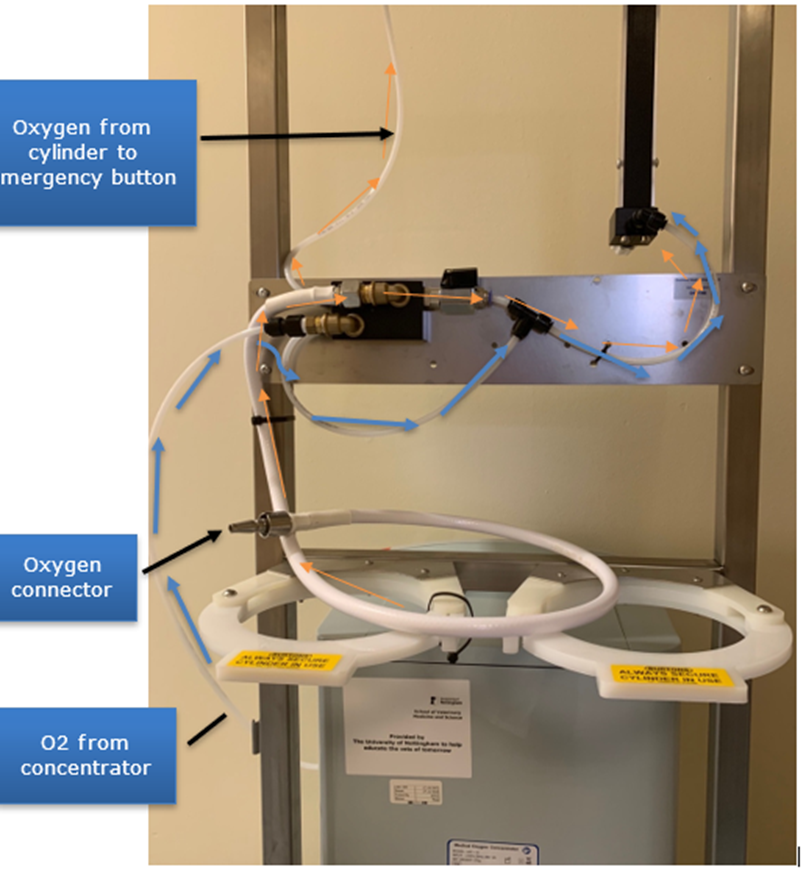
where does oxygen flow from and to
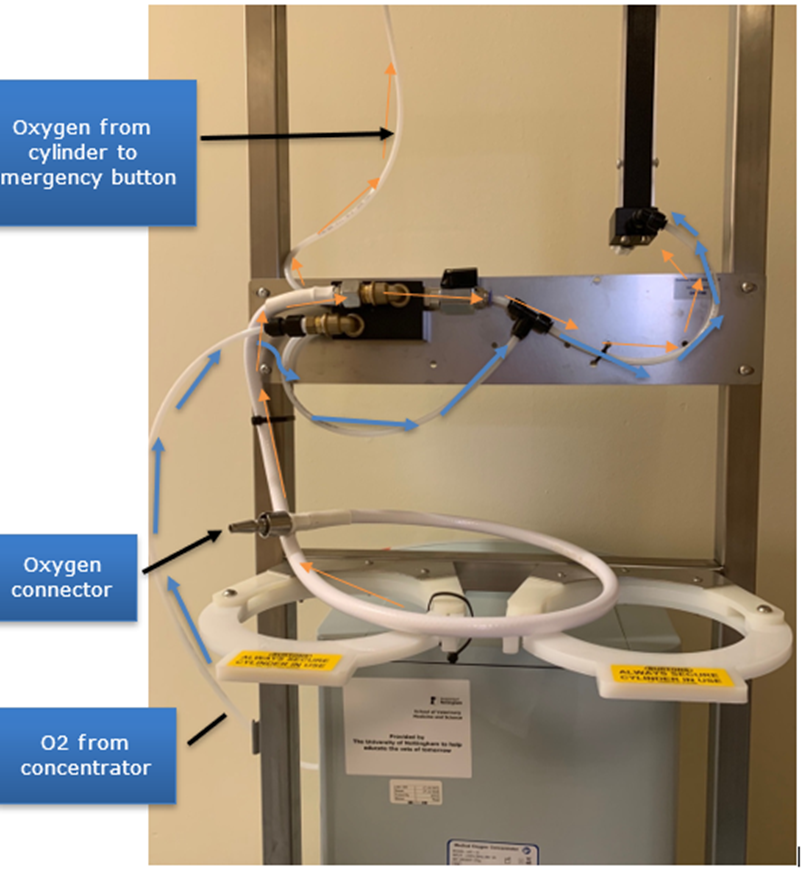
Oxygen travels from the concentrator to the anaesthetic machine flowmeter (blue arrows). At this point the ball valve is in isolation (closed) position i.e. perpendicular. Oxygen from the cylinder travels via the white tube to the emergency oxygen button (orange arrows)