CCRN Cardiovascular: ACS/Dysrrhythmias
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
What is ACS? What are the three (3) types?
Acute coronary syndrome- results from sudden reduction or blockage of blood flow to myocardium.
Three types: Unstable angina, Non-ST Elevated Myocardial Infarction (NSTEMI), and ST-Elevated Myocardial Infarction (STEMI)
Explain general ACS pathophysiology.
Starts with rupture of atherosclerotic plaque in a coronary artery- triggers platelet aggregation and adhesion, thrombin activation and fibrin formation, vasoconstriction and thrombus propagation
Results in in partial or total occlusion blocking coronary artery, reducing O2 and nutrients
Explain the 3 ACS type pathophysiology
UA- partial occlusion of coronary artery, but no myocardial necrosis- biomarkers (troponin/CK-MB) stay normal, ischemic symptoms present
NSTEMI- partial occlusion accompanied by elevated troponin, no ST elevation on ECG (infarctio n is subendocardial, or not full thickness)
STEMI- complete occlusion with ST elevation on ECG, needs immediate reperfusion therapy to save myocardium and prevent death
Key Differences (Chart): Type/ Biomarkers/ ECG findings/ Degree of Occlusion
UA- Normal Biomarkers/ ST depression, T-wave inversion/ partial, transient occlusion
NSTEMI- Elevated Biomarkers/ ST depression, T-wave inversion/ Partial, prolonged occlusion
STEMI- Elevated Biomarkers/ ST elevation, Q waves/ Complete
Signs/Symptoms
Mostly have some form of chest discomfort, can be atypical (older adults, diabetics, women)
Chest pain/pressure- retrosternal, may radiate to L arm, neck, jaw or back- crushing, squeezing, or heavy. Lasts ~20 mins, not relieved by rest or nitro
SOB (may also indicate HF/ pulmonary congestion)
Diaphoresis
Nausea/vomiting/anxiety or syncope- frequently reported in inferior wall MI
Fatigue/weakness
S/S: ECG Findings/ Diagnostics
ST elevation > 1mm = STEMI (transmural infarction)
ST depression = NSTEMI/ UA
T wave inversion = ischemia/ evolving infarct
Q waves (late sign) = Previous infarction or late STEMI
New LBBB = may be equivalent to STEMI
ST elevation on continuous leads + rise in troponin = STEMI > needs urgent PCI or thrombolytics
ST depression or T wave inversion + troponin rise = NSTEM > non-emergent PCI, medical therapy
Lab Markers/Tests
Troponin I/T (most specific) - rises 3-6 hours after symptom onset. Peaks at 12-24 hours, may stay elevated for 7-10 days. Elevated in NSTEMI/STEMI, normal in UA.
CK-MB (less specific)- rises earlier but returns normal faster. Can indentify reinfarction
BNP or NT-proBNP- may be elevated of LV dysfunction or HF is present
*If trop is negative, but symptoms persist and ECG suggestive of ischemia, repeat lab Q6 hours to capture delayed elevation
CXR- r/o other causes of chest pain (pneumothorax, aortic dissection)
Echocardiogram- may show wall motion abnormalities in affected area
Coronary angiography (LHC)- definitive test for dx and tx
Goal of Treatment/ Initial Tx
Goal: relieve ischemia, restore perfusion, and prevent further thrombus formation or myocardial damage.
Initial tx: MONA
Morphine- provides analgesia, reduces anxiety, and decreases sympathetic tone. Reduces preload via venodilation. Can cause hypotension or RV infarct
Oxygen- only administer if SpO2 <90%, respiratory distress is present or signs of hypoxemia present.
Nitrates- sublingual or IV can relieve CP and reduce preload. Contraindicated to those w/ hypotension, bradycardia, or recent use of phosphodieterase inhibitors (Sildenafil).
Aspirin- give immediately unless contraindicated (recent GIB/true allergy). Use 162-325 to inhibit platelet aggregation.
Reperfusion Strategies
PCI (Percutaneous Coronary Intervention)- Gold Standard in STEMI if available within 90 minutes (door-to-balloon time). Also considered in high risk NSTEMI
Thrombolytics (fibrinolytics)- Used only in STEMI if PCI unavailable within time frame. Most effective within 3 hourse of symptom of onset. Contraindicated in recent surgery, bleeding disorders, or stroke
NSTEMI/UA- medically managed first, the assess risk for need for PCI
Antithrombotic & Anti-Ischemic Therapy
Antiplatelets-
Asa- continue indefinitely
P2Y12 inhibitors (Clopidogrel/ticagrelor)- added to asa for dual anti-platelet therapy (DAPT), especially post-PCI
Anticoagulants
Heparin- reduced clot propagation
Bivalirudin/fondaparinux
Beta-Blockers
Reduce myocardial O2 demand by decreasing HR and BP
Contraindicated in acute decomp. HF, bradycardia, or severe hypotension
Statins
Started early regardless of cholesterol level. High intensity statin therapy improves outcomes
ACE Inhibitors/ARBS
Started within 24 hours if LV dysfunction, HF or anterior MI present
Nursing Priorities
Monitor for recurrent CP or ECG changes
Serial troponins to assess infarct progression
Continuous telemetry for arrhythmias
Watch for signs of bleeding if thrombolytics or anticoagulants are used
Educated pts on importance of medication adherence and risk factor modification
Complications (3 Major)
A. Arrhythmias- most common
Ventricular- VT/VF, common in first 48 hours most-MI d/t myocardial irritability. Defib if pulseless
Bradyarrhythmias- seen especially in inferior wall MI d/t AV node ischemia, may require atropine or pacing
Afib- may occur from atrial ischemia or increased left atrial pressure; can compromise cardiac output of rapid or persistent
PVCs- may precede more serious arrhythmias, monitor closely
B. Pericarditis- inflammation of pericardial sac following MI
Typically occurs 2-4 days post-MI (early) or weeks later (Dressler’s syndrome)
Pleuritic CP (worse when lying down), pericardial friction rub, and diffuse ST elevation on ECG (not localized like in STEMI)
Tx include NSAIDs for inflammation and pain, avoid AC unless strongly indicated, d/t bleeding risk. | *recognize pattern as it can mimic reinfarction, but different ECG pattern and tx approach
C. Pappilary Muscle Rupture- rare but catastrophic mechanical complication, typically occuring within 3-7 days post-MI, spec. an inferior MI > post papillary muscle
Leads to acute mitral regurgitation > sudden pulmonary edema, hypotension, cardiogenic shock
Physical exam may reveal new, loud systolic murmur at apex, often accompanied by signs of Left HF.
DX confirmed by echo
Requires urgent surgical intervention- mortality extremely high w/o repair
HF and cardiogenic shock- d/t to large size of infarct and poor contractibility
Ventricular septal rupture- causes new harsh systolic murmur and biventricular failure
Left ventricular aneurysm- may form weeks after MI, can lead to embolic events or HF
*If post-MI pt develops hypotension, dyspnea and new murmur > think papillary muscle rupture or vent. septal defect | If chest pain with diffuse ST elevation and friction rub > pericarditis
Explain dyshythmia pathology
Result from disturbances from hearts electrical conduction system. They may involve the following:
Automaticity- cells firing when they shouldnt (ectopic pacemakers in VT)
Conductivity- failure or delay in signal transmission (i.e. AV blocks)
Reentry circuits; impulses looping repeatedly through cardiac tissue (i.e. SVT)
Can also result from underlying myocardial ischemia, electrolyte imbalances (esp. in K/Mg/Ca levels), hypoxia, or medication effects (digoxin, antiarrythmics)
Common precipitating factors include acute coronary syndrome, heart failure, and post cardiac surgery states.
What can arrhythmias affect and how?
It can affect cardiac output by increasing or decreasing heart rate, reducing stroke volume (loss of atrial kick in afib) or cause uncoordinated contractions (V-fib)
Explain pathophysiology of the following key rhythms: Tachyarrhythmias (SVT/VT)/, Bradyarrhythmias (Sinus Bradycardia/ High grade AV blocks), Pulseless rhythms (VF/Pulseless VT/ asystole/PEA), Atrial arrhythmias (A-fib/flutter), Heart Blocks
Tachyarrhythmias- increase myocardial O2 demand, reduce ventricular filling time = decrease in CO, increase ischemic risk
Bradyarrhythmias- slow HR = decrease in CO → HYPOperfusion
Pulseless Rhythms- No effective circulation, requires ACLS protocols
Atrial arrythmias- loss of atrial kick = decrease in preload, risk of thromboembolism
Heart blocks- delay/block signal from atria to ventricles → bradycardia of AV dissociation, depending on type
Signs/Labs (General/Brady/Tachy)
Hemodynamic instability
Altered mental status
Based on HR, rhythm origin, and impact on cardiac output
Bradycardia (HR <60 BMP)
Fatigue, dizziness, lightheadedness
Syncope/presyncope
Hypotension, especially in high AV grade block/SN dysfunction
Possible altered mental status → drop in cerebral perfusion
Tachycardia (HR >100 BPM)
Palpitations, anxiety, chest discomfort
SOB → decreased filling time
Hypotension/signs of hypoperfusion
Syncope if unstable/poorly tolerated rhythms
Syncope/sudden colllapse
Seen in VT, complete HB, torsades, VF
Always investigate arrhythmic causes in unexplained syncope in ICU pts
Pulses may be weak/irregular and perfusion markers (urine output, cap refill may deteriorate)
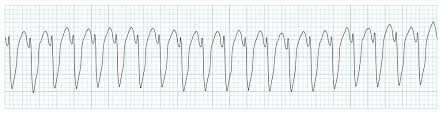
ECG Patterns: VT
Wide QRS complex (>0.12 sec), regular rhythm
May have pulse or pulseless
Monomorphic or polymorphic (Torsades)
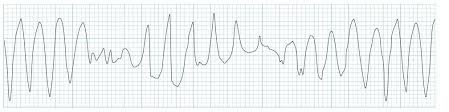
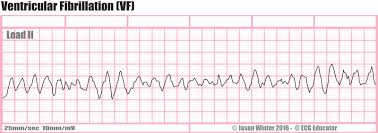
ECG Patterns: VF
Chaotic, irregular no identifiable waves
No cardiac output → immediate defibrillation required
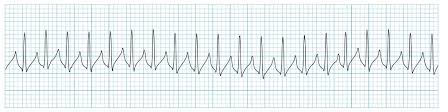
ECG Patterns: SVT
Narrow QRS
HR >150
P waves often hidden in T waves
Sudden onset and termination
ECG Patterns: Afib/Aflutter
Afib
Irregularly irregular rhythm
No discernable P waves, variable ventricular response
Risk of thromboembolism
Aflutter
Sawtooth flutter waves (best seen in leads II, III, aVF)
Ventricular rate often REGULAR and FAST (2:1 or 4:1 conduction)
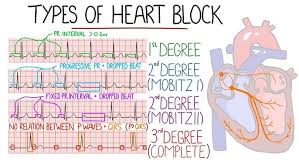
ECG Patterns: AV Blocks
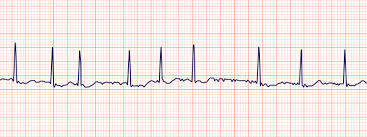
First Degree
Prolonged PR interval (>0.20 sec)
Second Degree Mobitz I
Wenkebach)- Progressive PR prolongation → dropped beat
Longer, longer, longer, drop, now we have a Wenkebach
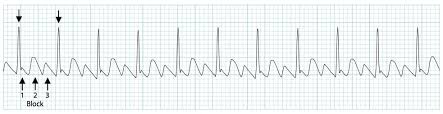
Second Degree Mobitz II
Dropped beats WITHOUT PR change
Third Degree (Complete)
Atria and ventricles beat independently (AV dissociation)
If your P’s and Q’s dont agree, now you have a third degree
Rhythm Insight: What to look for
Assess rate and regularity, QRS width, P wave presence, and PR interval
Is this rhythm perfusing the patient? What is the immediate intervention?