Unit 4: Circulatory Response to Exercise and Thermoregulation
1/111
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
112 Terms
Circulatory system’s purpose
¤Transport O2 and nutrients to tissues
¤Removal of CO2 wastes from tissues
¤Regulation of body temperature
How does the cardiorespiratory system regulate body temp
Vasoconstriction - ex: when cold, shunts blood away from periphery
Vasodilation- ex: when hot, there’s gradient from skin to atmosphere, heat is radiated to the environment
Two major adjustments of blood flow during exercise
¤Increased cardiac output
¤Redistribution of blood flow
The 3 regulation of MAP during exercise
¤Determinants
¤Exercise pressor reflex
¤Central command
Chordae tendinae
keeps the valves closed so NO regurgitation (backflow)
What happens if NO chordae tendinae or NO papillary muscles
blood will go to opposite direction of where it’s supposed to go, based on the press gradient
Heart does what
creates pressure and press gradient to drive blood flow
Arteries and arterioles
Carry blood away from the heart
Capillaries
Exchange of O2, CO2, and nutrients with tissues
Veins and venules
Carry blood toward the heart
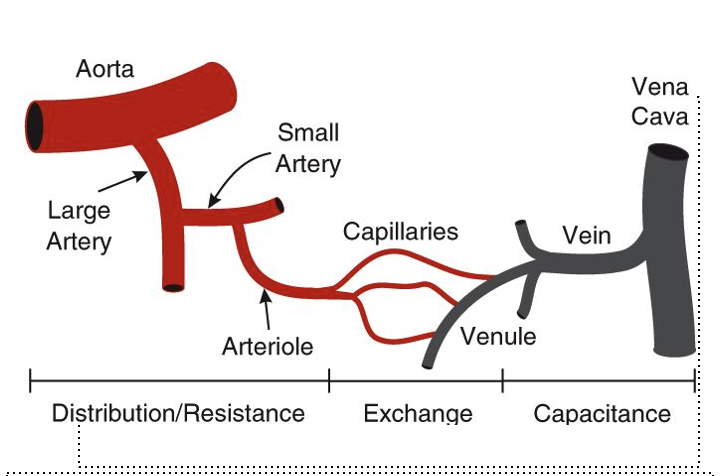
Describe this image
Aorta —> very compliant (meaning very stretchy)
Arteriole —> tiny but has mix of smooth muscles
small arteries —> have smooth muscle
Vein: temporay storage unit, and very compliant and could hold a lot of blood vol w/o significant change in blood press
Pulmonary circuit vs Systemic circuit
Pulmonary:
¤Right side of the heart
¤Pumps deoxygenated blood to the lungs via pulmonary arteries
¤Returns oxygenated blood to the left side of the heart via pulmonary veins
lower pressure + compliant due to not having to send blood to rest of the body
Systemic circuit:
¤Left side of the heart
¤Pumps oxygenated blood to the whole body via arteries
¤Returns deoxygenated blood to the right side of the heart via veins
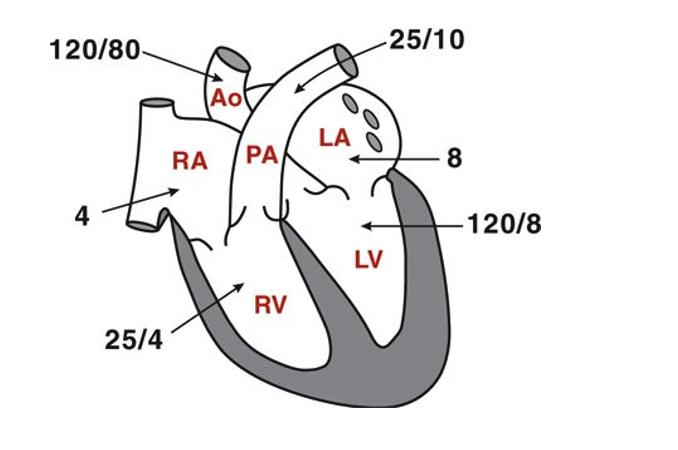
MAP of pulmonary circuit and why?
25 mmHg
b/c they are very compliant and have low resistance
MAP of systemic circuit and why?
90 mmHg
b/c it has to pump blood much farther and against more SVR
Normal resting cardio output and is it for sympathetic or pulmonary
5 L/min and it is both
both CO on each sides are the same
endocardium
innermost and closer to blood vessels
myocardium
smooth muscle
epicardium
upper layer of heart
Heart attack aka _________ is caused by what?
aka myocardial infarction
caused by blood clotting (myocardial ischemia) which if prolonged causes the death of myocardial cells (myocardial infarction)
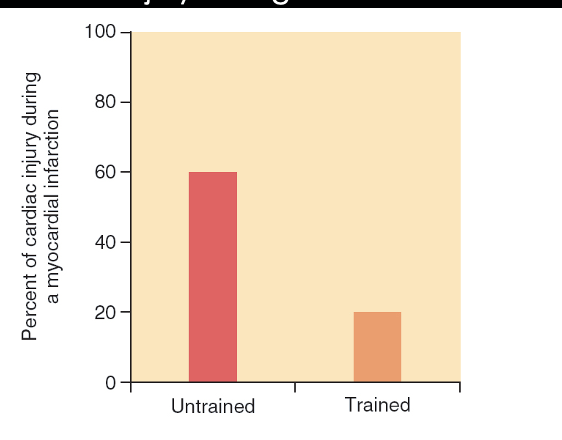
Exercise training protects heart b/c
¤Reduce incidence of heart attacks
¤Improves survival from heart attack
¤Exercise reduces the amount of myocardial damage from heart attack b/c
Improvements in heart’s antioxidant capacity
Endurance Exercise Protects Against Cardiac Injury During Heart Attack
lowered risk of myocardial infarction for trained/endurance athletes
also if trained athletes does have myocardial infarction, they experience less symptoms
Resistance training can ______ cardiovascular health
enhanced
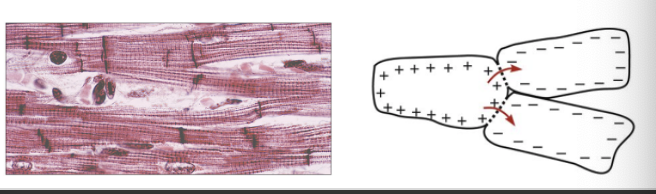
Myocardium structure
¤Only one fiber type (similar to type I)
High capillary density
High number of mitochondria
Striated
¤Cardiac muscle fibers connected by intercalated discs
Desmosomes: hold cells together
Gap junctions: rapidly conduct action potentials
Myocardium vs Skeletal Muscle
¤Skeletal muscle cells
Large, long, unbranched, multinucleated
Intermittent, voluntary contractions
Na+ induced Ca++ release from SR
¤Myocardial cells
Small, short, branched, one nucleus
Continuous, involuntary rhythmic contractions
Ca++ induced Ca++ release
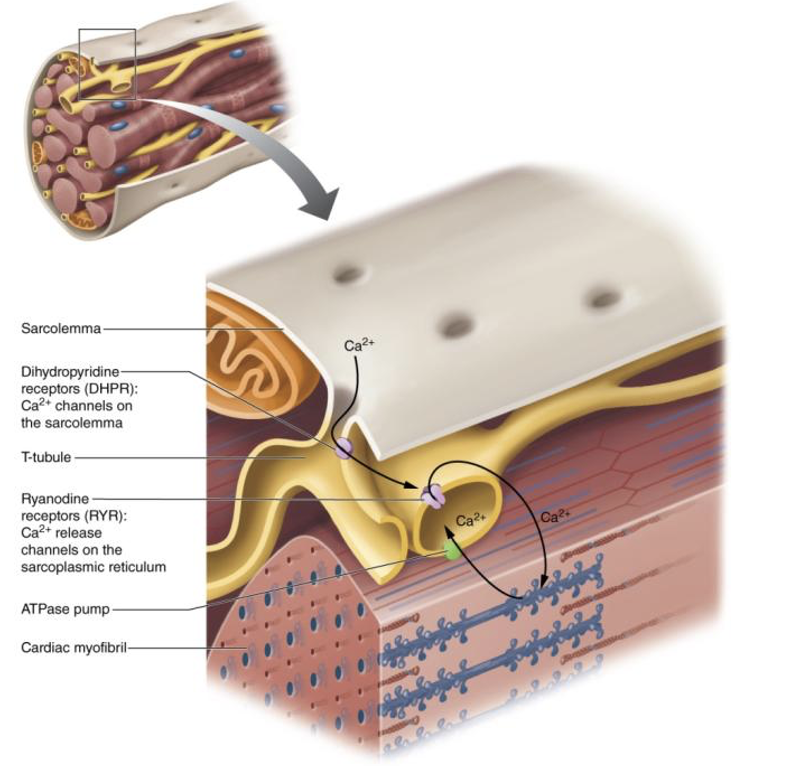
Ca2+ induced release
Ca2+ from SR floods the heart and is key signal of depolarization in the heart
improved Ca2+ handling results in more forceful contraction
What signals depolarization for Skeletal muscles
Na+
damage to myocyte
No help or repair
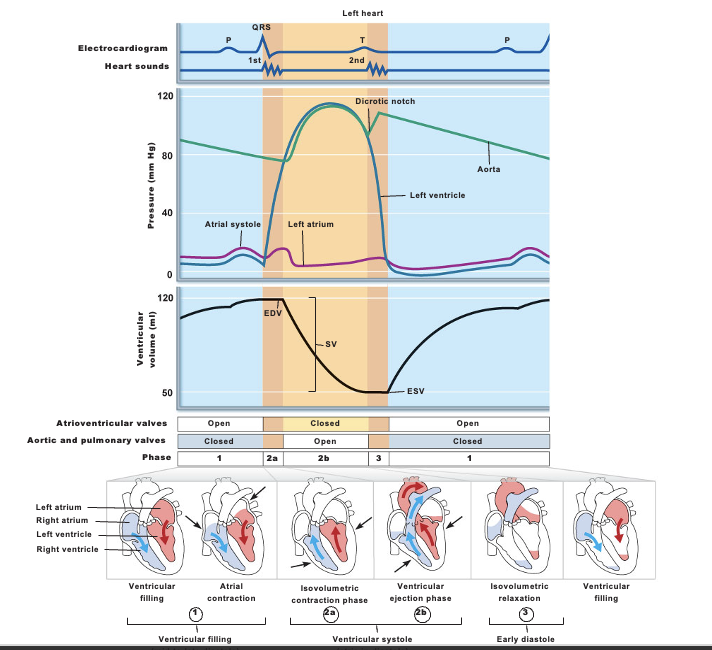
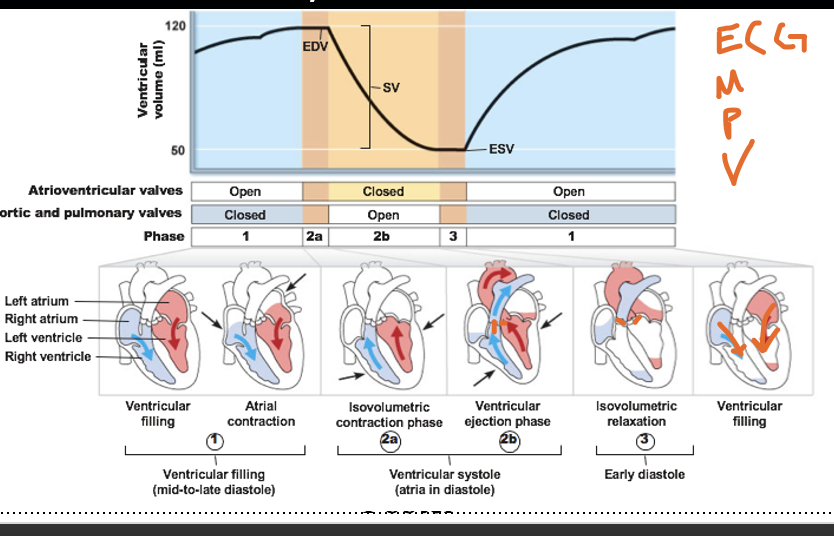
Events of Cardiac cycle in order
1) Ventricular filling (mid-to-late diastole)
ventricular filling + atrial contraction
2) Ventricular systole (atria in diastole)
Isovolumetric contraction + Ventricular contraction
3) Early diastole
Isovolumetric relaxation
4) back to Ventricular filling
then the process repeats itself
systole
¤Contraction phase
¤Ejection of blood
~2/3 or 60% blood is ejected from ventricles per beat
Diastole
¤Relaxation phase
¤Filling with blood
At rest diastole is _____ than systole
During exercise both systole and diastole are ______
¤At rest, diastole longer than systole
@ rest you’re in diastole for 2/3 of overall cardiac cycle
¤During exercise, both systole and diastole are shorter
b/c HR increases —> makes the cardiac cycle go faster
Ventricular filling (mid-to-late diastole)
1) Ventricular filling
AV valves are open b/c Patrial >> Pvent
passive Blood flow goes atria —> ventricles
Ventricles are at diastole, Aortic + Pulmonary valves closed
2) Atrial contraction
pace maker stimulates + depolarization of atria
causes atrial contract
this atrial contraction gives more boost/ more blood to ventricle (atrial kick)
this boost is good for exercise
Ventricular systole (atria in diastole)
3) Isovolumetric contraction
ventricles depolarize then causes contraction
all valves are closed.
4) Ventricular ejection
since Ventricular press >> aortic press + pulmonary press
it causes Aortic/semilunar valve (left) and Pulmonary/semilunar valve (right) to bust open
This causes ejection of blood
we then lose blood volume. —→ SV = EDV - ESV
Isovolumetric relaxation (early diastole)
Not enough pressure and gradually relaxes myocytes
all valves are closed
Ventricular filling
return to it and higher BV
what type of pressure is close to BP?
aortic pressure when it is 120/80
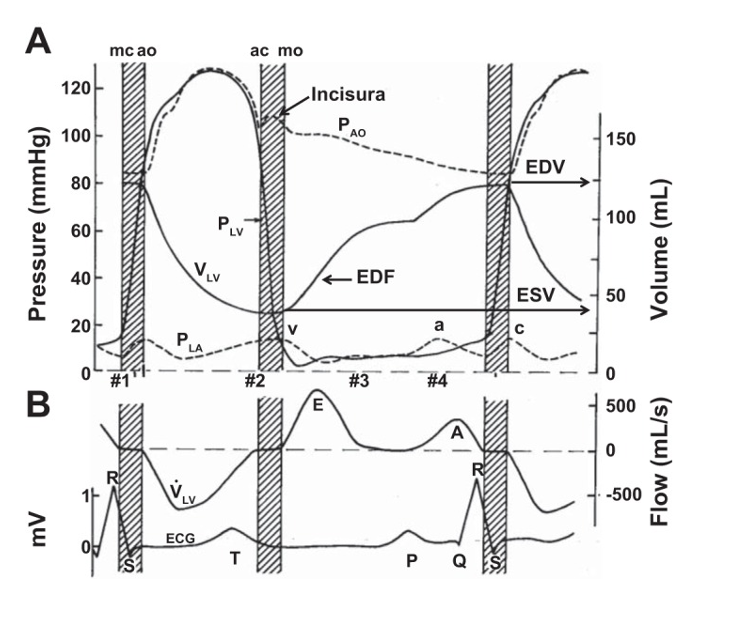
x-descent
downward wave, reflecting right atrial relaxation and the AV valve moving down during ventricular contraction
C-wave
Since ventricular contraction squeezes against all closed gates
there’s pressure build up that causes the bump in atrial pressure
(this is due to bulging of AV values back into atrial chamber)
V-wave
final pulling/increasing atrial press before AV valves open and pushing blood to ventricles
occurs btw late ventricular systole and early diastole
which wave has highest atrial volume
v-wave
Dicrotic notch
Reverberation, incisura/dicrotic notch
Reverberation:
makes dicrotic point
Dicrotic notch/ incisura
a small dip or notch on the arterial blood pressure
marks the closure of the aortic valve as systole ends, causing a brief backward flow of blood
Explain EMPV
ECG
SA node fires (electrical activity) to stimulate heart to contract or relax
Mechanical event
shortening or enlarging of chamber
systole or diastole (contraction)
Pressure event
pressure created + squeeze on chamber
Volume
after pressure gradient, it is the blood flow
P-wave
atrial depolarization (contraction)
T-wave
ventricular repolarization (diastole/relaxation)
QRS wave complex
ventricular depolarization (contraction)
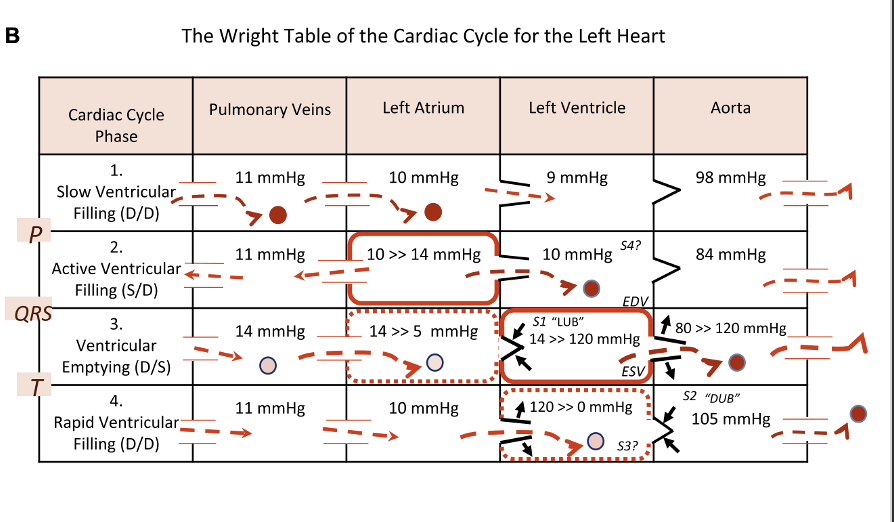
Heart sounds
First: closing of AV valves —> lub
Second: closing of A + P valves —> dub
Pulse pressure
difference btw systolic + diastolic
Clinical MAP
MAP = DBP + 0.33 (SBP - DBP)
it is 1/3 of pulse pressure b/c @ rest, you are in diastole for 2/3 of overall cardiac cycle
meaning 1/3 of the time you are generating high pressure
Systolic BP
pressure generated during Ventricular contraction
turbulent flow
Diastolic BP
pressure in arteries during cardiac relaxation
disappearing sound —> which then reestablishes lamellar flow
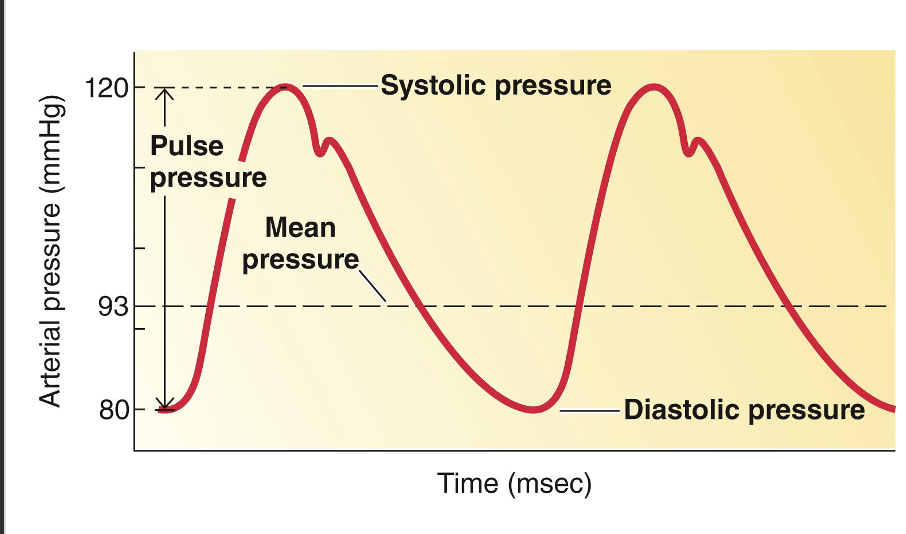
this a graph of what?
graph of Aortic
Stroke volume equation
SV = EDV - ESV
EDV is measured after isovolumetric relaxation
ESV is measured after isovolumetric contraction
What sounds are we hearing when measuring BP w/ occlusion
korotkoff sounds (turbent flow)
No sound is produced meaning the flow is
lamellar
Physiological MAP
MAP = CO x SVR
SVR = TPR = TVR
Cardiac Output
delivery
HR x SV
Short term regulation of MAP
Sympathetic NS (
Baroreceptors in aorta and carotid arteries
sensed Increase in BP → decreased SNS act
which then decreases CO and poss Resistance → higher BP
sensed Decrease in BP → Increased SNS act
which then increases CO and poss Resistance → lower BP
Long-term regulation of MAP
In days, weeks, years
Kidneys
control BV
Ex: low BV → low SV x low CO → low BP
More trained person has ____ HR and ___ SV
lower HR and higher SV due to using less energy
Regulation of HR
Parasympathetic NS
thru Vagus nerve / parasympathetic tone (like a break on a car)
inhibits SA and AV node —> slows HR
Sympathetic NS
thru cardiac accelerator nerves
stimulates SA + AV node → increases HR (chronotropy)
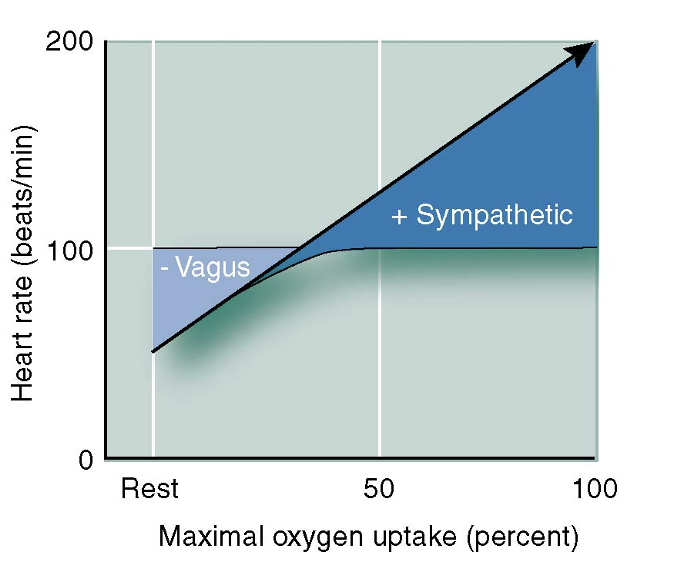
LOW resting HR is due to ______ tone
parasympathetic tone
_____ in HR at start of exercise and why?
increase in HR @ start b/c of parasympathetic withdrawal
up to 100 bpm
later increase is due to increase activation of SNS
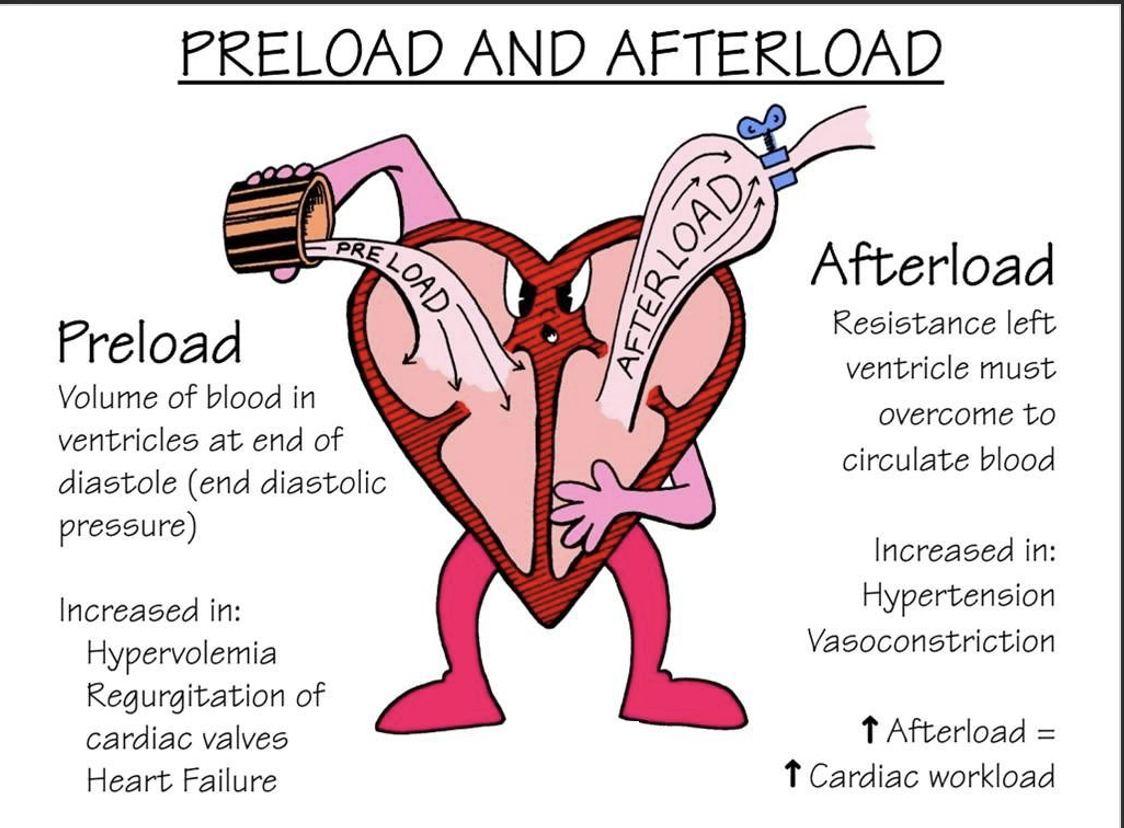
Regulation of SV
1.End-diastolic volume (EDV)
¤Volume of blood in the ventricles at the end of diastole (“preload”)
getting more blood —> higher SV
Average aortic blood pressure
¤Pressure of the heart that be overcome for ventricles to eject blood (“afterload”)
Mean arterial pressure
higher afterload —> lower SV
Strength of the ventricular contraction (contractility)
¤Enhanced by circulating Epi/Noepi and direct sympathetic stimulation of heart
more contractility —> more blood ejected —> Higher SV
HR
Hypertension ____ afterload, which results in _______ ESV, and _____ SV
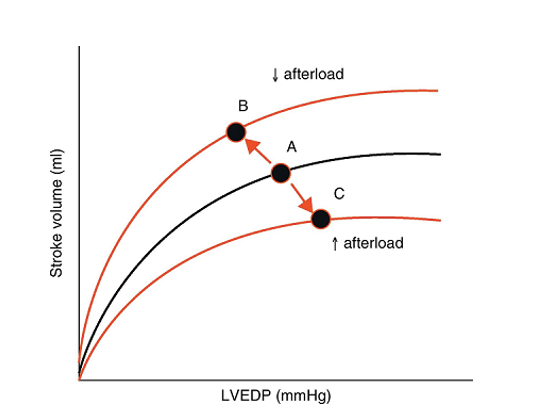
Frank- Starling Law of Heart
¤Preload: degree of stretch of cardiac muscle cells before they contract (Frank-Starling law of the heart)
¤Cardiac muscle exhibits a length-tension relationship
¤At rest, cardiac muscle cells are shorter than optimal length
¤Slow heartbeat and exercise increase venous return
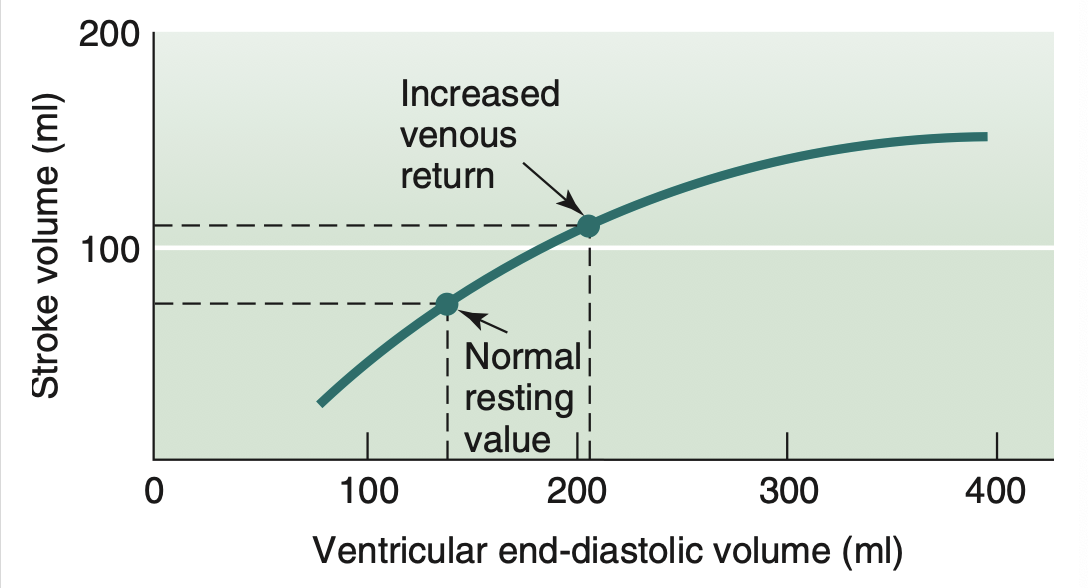
VR increased by
1.Venoconstriction
¤Via SNS —> reduces compliance and capacitance (storage) of veins → increases blood flow to the heart
2.Skeletal muscle pump (helpful during exercise)
¤Rhythmic skeletal muscle contractions, squeeze on veins to let blood flow in the extremities toward the heart
¤One-way valves in veins prevent backflow of blood
increases SV too
generates more force via gaining more contractile proteins —> further increasing VR
3.Respiratory pump (NOT helpful @ rest due to not intensely breathing)
¤Changes in thoracic pressure pull blood toward heart
inhalation →
increased vol and decreased press of thoracic cage compared to abdominal cavity —> blood flows to thoracic cage to the heart
(due to blood flow HP → LP)
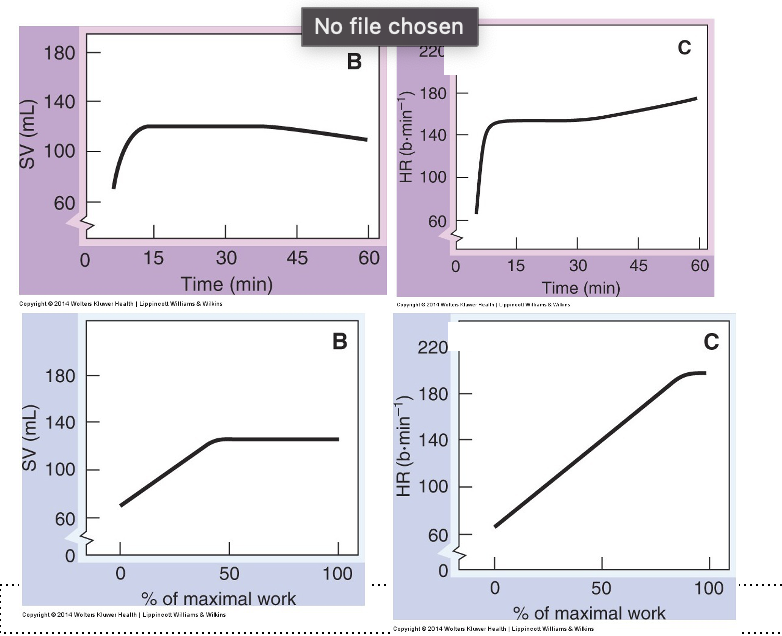
Heart Rate
purple: steady state exercise
blue: high intensity exercise
Effects of Sympathetic Stimulation on Stroke Volume
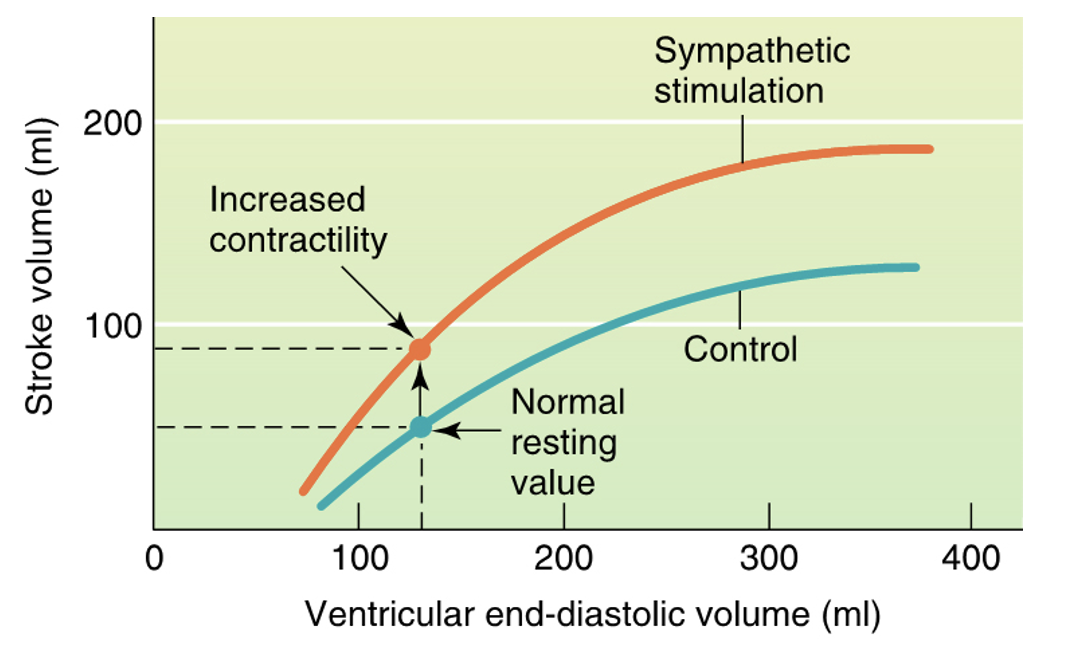
Strength of Contraction
¤Contractility (Inotropy): contractile strength at a given muscle length, independent of muscle stretch and EDV
Positive inotropic agents increase contractility
Increased Ca++ influx due to sympathetic stimulation
Hormones (thyroxine, glucagon, and epinephrine)
¤Negative inotropic agents decrease contractility
Acidosis (too much acid / decrease in pH)
this is dangerous b/c it will cause the aerobic heart to rely on anaerobic processes
Increased extracellular K+
Calcium channel blockers
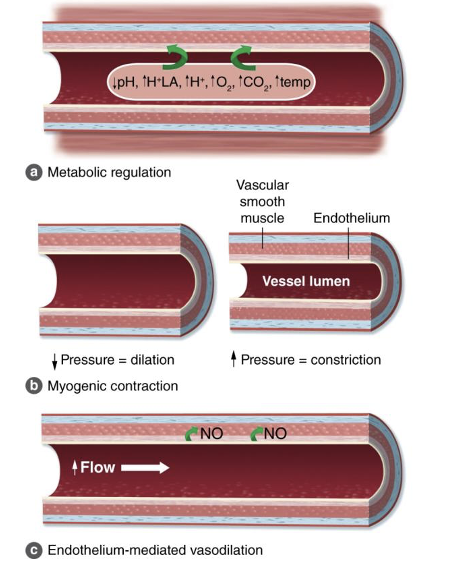
Intrinsic Control of Blood Flow
Ability of local tissues to constrict or dilate arterioles that serve them
alters regional flow based on needs
¤Metabolic mechanisms (VD) —→ (IMPORTANT FOR EXERCISE)
Buildup of local metabolic by-products
decrease in O2
Increase in CO2, K+, H+, lactate
causes Functional sympatholysis
¤Endothelial mechanisms (mostly VD)
Substances secreted by vascular endothelium
Nitric oxide (NO), prostaglandins, EDHF
¤Myogenic mechanisms (VC, VD)
Local pressure changes can cause Vasoconstriction (VC), Vasodilation (VD)
Increase in P → Increase VC
Decrease in P → increase VD
Central Command
initial signal to drive cardiovasc sys and reset the set point coming from higher brain centers b/c of centrally generated motor signals
Anticipation that you’ll exercise —> your set point is reset to higher set point
Central command is fine-tuned by feedback from
¤Heart mechanoreceptors
¤Muscle chemoreceptors
Sensitive to muscle metabolites (K+, lactic acid)
¤Muscle mechanoreceptors
Sensitive to force and speed of muscular movement
¤Baroreceptors
Sensitive to changes in arterial blood pressure
Exercise Pressor Reflex (EPR)
¤Metaboreflex
Chemicals (metabolites) released from contraction stimulate chemoreceptors
Stimulation of chemoreceptors send afferent information to the medullary CV centers via group IV afferent nerves.
This causes a “shift” in MAP control: baroreflex resetting
¤Mechanoreflex
Mechanical deformation (movement) from contracting/moving limbs stimulate mechanoreceptors (propioceptors)
Stimulation of mechanoreceptors send afferent information to the medullary CV centers via group III afferent nerves
This causes a “shift” in MAP control: baroreflex resetting
Our set point if everyone’s around 120/80 BP, is
MAP (90 mmHg)
Isolation of mechanoreceptors
lay down on ground, you are inactive
but, if diff person puts your feet in a bicycle-like pedal and that person is connected to you, but in a diff bicycle
every time that person moves the pedals, it moves your pedal
b/c of this mechanoreceptors would fire b/c they detect that your legs are moving
then BP increases
isolation of chemoreceptors
occluding blood flow in arm and make person do forearm grip exercise
you will accumulate metabolites
since you occluded blood flow → metabolites do NOT deposit anywhere
but as soon as you release them —> BP increases
even if NO body movement
This is due to chemoreceptors firing
Functional sympatholysis
SNS's vasoconstrictive response is lowered in exercising skeletal muscles, allowing for optimized blood flow to meet metabolic demands
During exercise MAP = CO x SVR
increase MAP = increase CO x SVR
skin
do intense in hot environment
vasodilates skin (lowers SVR)
can be up to 8 L/min for CO in hot environment
muscles
engaging more muscle + doing harder exercise
metabolites accumulate in the active muscles
causes functional sympatholysis → vasodilating muscle → increase blood flow to muscles
lower SVR
Cardiovascular Adjustments to Exercise ( in order)
Central command
anticipation of exercise withdraws parasympathetic tone
Mechanical
mechanoreceptors detect movement, activating part of the exercise pressor reflex to reset MAP to a higher set point
skeletal muscle pump increases venous return, which increases SV.
respiratory pump increase venous return and SV, but the increased breathing rate is caused by metabolite buildup
Metabolic
metabolite buildup triggers metaboreceptors to activate part of the exercise pressor reflex to raise MAP to a higher set point, increases breathing rate (increasing respiratory pump), and triggers functional sympatholysis (vasodilation to working muscles)
Autonomic
parasympathetic withdrawal and sympathetic nerve activity increases from increased firing of metaboreceptors: increased HR, increased contractility of heart, increased SVR (except skin and muscles), increased afterload, increased venoconstriction (increases venous return and SV)
Humoral
increased norepinephrine and epinephrine, which also increase HR, contractility, venoconstriction
During exercise
your muscles work harder, meaning more O2 than @ rest
in order to deliver O2, heart beats faster → faster pulse
Why is it good to exercise regularly
your heart gets used to moving more blood thru body
left ventricle hypertropies and stronger contraction
w/ each heart beat pumping more blood-
the heart beats less often → lower HR during exercise and lower HR during rest
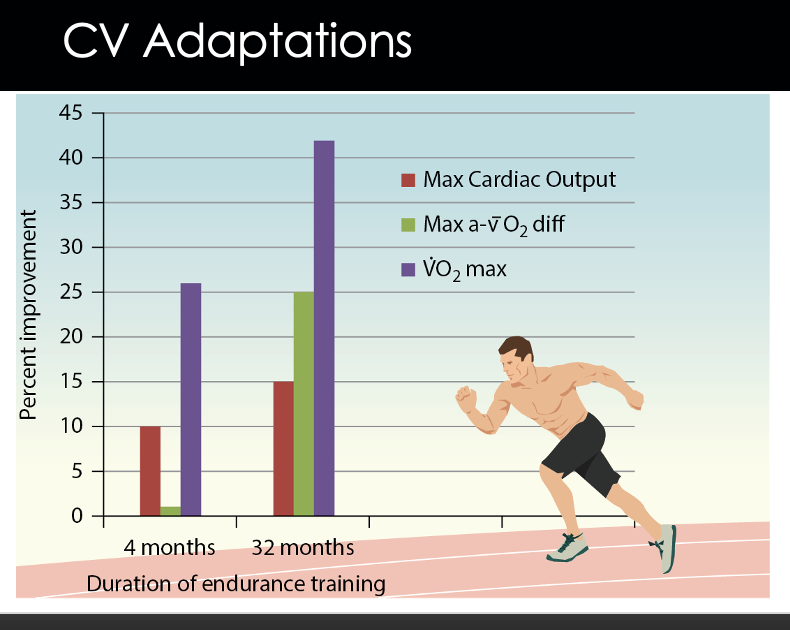
Calculation of VO2 max
VO2 max = CO X a-VO2 difference max
CO = delivery
HR x SV
a-VO2 difference max = extraction
Short-term vs Long-term exercise CV adaptation
Short term exercise ( w/in 1-4 months)
initial VO2 max increases by 26%
this is due to retaining more plasma volume → increases SV → increases CO
increasing SV > increasing a-vO2 → not good @ extraction
Long term exercise ( w/in 28-32 months)
VO2 max increases by 42%
increasing a-vO2 > increasing SV → Get better @ extraction
Training-induced increased maximal SV
Increased Preload (EDV)
increased plasma volume @ start
increased VR
b/c increased plasma
increased Ventricular volume
b/c increased plasma
Decreased Afterload (TPR)
decreased arterial constriction
increased max muscle blood flow w/ NO change in MAP
This is all b/c you get better @ blood flow distribution, where you’re more conditioned to vasodilate and do functional sympatholysis in appropiate places
this then lowers resistance → causing low afterload
Increased Contractility
eccentric hypertrophy (expansion of chamber) good in exercise b/c it is accompanied by concentric hypertrophy (thicker, stronger muscle around chamber)
Left ventricular hypertrophy w/o exercise is good or bad?
bad b/c it is a response to hypertension
What is concentric hypertrophy a response to?
to higher pressure (from resistance training or chronic hypertension, which increases afterload and puts more stress on left ventricle), it wants to overcome the pressure
it does this by the walls thickening —> sarcomeres added in parallel
ex: constantly picking up heavier weight
What is eccentric hypertrophy a response to?
due to volume overload that occurs w/ aerobic training → increased Vr → increases filling of LV → sarcomeres add in series
based on increased VR (filling a lot)
needing more vol
Thickened muscle w/o expansion of chamber volume, what happens
you get smaller size of chamber vol → smaller size of chamber
since the chamber size is small → you get smaller preload
Resistance exercise
gray area
b/c it has some eccentric hypertrophy, but def has concentric hypertrophy
Arteriovenous O2 difference
Increased Muscle blood flow
decreases SNS vasoconstriction
Improved ability of the muscle to extract oxygen from the blood
increased capillary density (more SA)
better extraction
fast blood flow via muscle
increased mitochondrial # @ SK muscle
increased metabolism
better extraction
For exercise training and diffusion distance
exercise training
increases more blood vessel to drop off stuff → reducing pressure on diffusion
Diffusion distance
Increased diffusion distance causes innermost layer of the heart to be more @ risk of ischemia
smaller diffusion distance causes innermost layer of the heart to be less @ risk of ischemia