MODA Drugs
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
X is a use-dependent drug against HCN. It blocks the pore when it is opened. It does not cross the blood brain barrier which reduces side effects.
Ivabradine
X acts as insulin secretagogues by binding to ATP-sensitive potassium channels on pancreatic beta cells, causing channel closure. This action depolarizes the membrane, opening calcium channels, stimulating calcium influx, and triggering insulin secretion, regardless of blood glucose levels, thus reducing serum
Sulphonylurea
X is classified as a Ib drug of Vaughan’s classification. It exhibit voltage- and use-dependent properties. It blocks voltage gated sodium channels at their inactivated state.
Lidocaine
X is classified as a Ic drug of Vaughan’s classification. It binds to the open state of Nav1.5 channels and dissociates very slowly during the diastolic interval. Because of this slow dissociation, a steady-state level of block is achieved during chronic administration. The drug shows use-dependent (or rate-dependent) blockade. Besides Na+ channel inhibition, it also weakly inhibits potassium channels, specifically the rapid component of the delayed rectifier K+ current (Ikr) channels. It is highly effective at preventing premature beats, particularly premature ventricular contractions (PVCs). It increases mortality and the risk of ventricular fibrillation (VF) in patients with a history of myocardial infarction (MI).
Flecainide (encainide withdrawn)
X is classified as a Ia drug of Vaughan’s classification. It binds to the pore of open fast sodium channels during phase 0, slowing conduction velocity in both atrial and ventricular myocardium. Beyond its Class I action, X is a potent inhibitor of several repolarizing outward potassium currents. The excessive prolongation of the QT interval (prolonged repolarization) creates a large transmural gradient, leading to early afterdepolarizations (EADs) and triggered activity in Purkinje fibers.
Quinidine
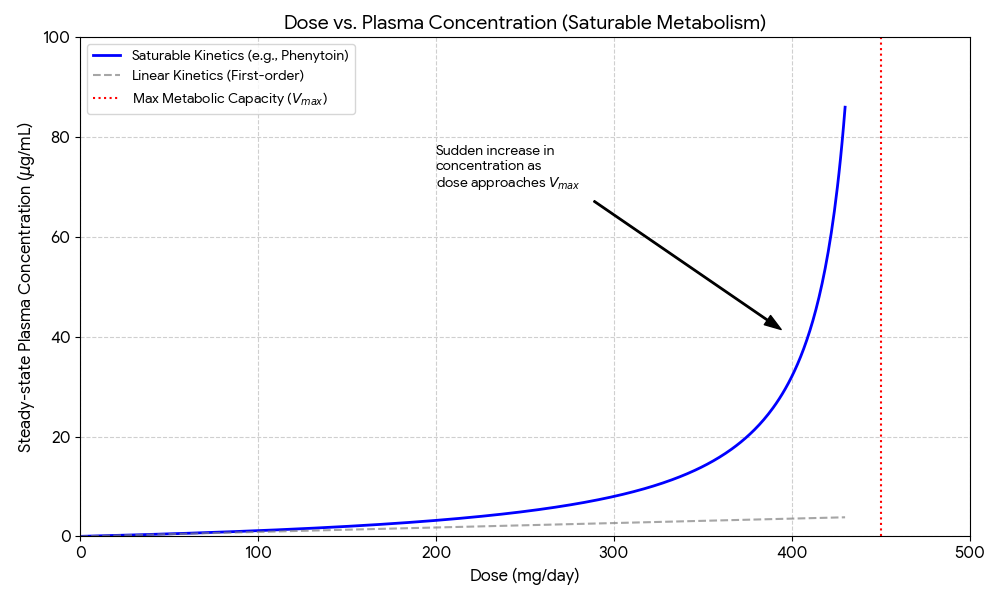
X binds to the inactive state of voltage-gated sodium channels, prolonging the refractory period and preventing repetitive neuronal firing. It can enhance the activity of inhibitory neurotransmitters such as GABA and reduce the excitatory effects of glutamate, although sodium channel blockade is the primary mechanism. Class 1b antiarrhythmic. It is metabolized by the liver (CYP2C9 and CYP2C19). It exhibits saturable metabolism, meaning that as the dose increases, the liver enzymes become saturated, leading to a sudden, disproportionate increase in plasma concentration.
Phenytoin
X binds specifically to the benzodiazepine site on the receptor complex, which is distinct from the GABA binding site. It increases the frequency of the chloride channel opening in response to GABA (gamma-aminobutyric acid), the major inhibitory neurotransmitter in the brain. It has a short elimination half-life of 1.5 to 2.5 hours, allowing for quicker recovery compared to diazepam.
Midazolam
X is a first-in-class, highly selective, non-competitive AMPA receptor antagonist approved for treating epilepsy. It acts post-synaptically to block glutamate-mediated synaptic excitation, which reduces neuronal hyperexcitability and prevents the spread of seizure activity. Approved as adjunctive therapy for partial-onset seizures (ages 4+) and primary generalized tonic-clonic seizures (ages 12+).
Perampanel
X is a potent, broad-spectrum (Class III) antiarrhythmic agent used to treat serious ventricular and supraventricular arrhythmias. It works primarily by blocking potassium rectifier currents (phase 3) to prolong the cardiac action potential, while also displaying sodium channel blocking (class I), non-competitive beta-blocking (class II), and calcium channel blocking (class IV) properties.
Amiodarone
X is an inodilator used for acute decompensated heart failure that increases cardiac contractility without raising intracellular calcium, thus limiting arrhythmia risks. It acts primarily by sensitizing troponin C to calcium, enhancing cardiac output, and opening ATP-sensitive potassium channels, causing systemic and coronary vasodilation. It is also a PDE inhibitor.
Levosimendan
X is a fully human monoclonal antibody (IgG2) that acts as a RANKL inhibitor, treating osteoporosis and bone metastasis by binding to RANKL (Receptor Activator of Nuclear Factor kappa-B Ligand). By blocking RANKL, it prevents the maturation, function, and survival of osteoclasts, thus stopping bone resorption and increasing bone density.
Denosumab
X is a first-in-class, nonhormonal, selective neurokinin-3 (NK3) receptor antagonist used to treat menopausal hot flashes (vasomotor symptoms). It works by blocking the binding of neurokinin B (NKB) to the NK3 receptor, restoring thermoregulatory balance in the hypothalamus disrupted by falling estrogen levels.
Fezolinetant (Veoza)
X is a potent loop diuretic that acts by inhibiting the sodium-potassium-chloride cotransporter (NKCC2) in the thick ascending limb of the loop of Henle in the kidney. By blocking this transporter, it prevents the reabsorption of sodium, chloride, and potassium, resulting in increased excretion of water, sodium, chloride, magnesium, and calcium.
Furosemide
X diuretics (e.g., hydrochlorothiazide, chlorthalidone) primarily lower blood pressure and reduce edema by inhibiting the sodium-chloride (Na+/Cl-) cotransporter (NCC) in the distal convoluted tubule (DCT) of the kidneys. By blocking this channel, they increase sodium and water excretion (diuresis), initially reducing plasma volume, while long-term management involves decreased vascular resistance.
Thiazide
X opens ATP-sensitive potassium channels in vascular smooth muscle cells, leading to vasodilation (widening of blood vessels).
Minoxidil
This class of drug inhibits the entry of calcium ions through L-type channels (dihydropyridine), relaxing vascular smooth muscle, lowering blood pressure, and increasing cardiac blood flow.
Nifedipine, Amlodipine (longer plasma half life). Ending in dipine.
X acts as a mineralocorticoid receptor antagonist, blocking the action of aldosterone, which causes the kidneys to increase water and sodium excretion while retaining potassium (potassium-sparing).
Spironolactone
A combination drug that treats heart failure through a dual mechanism: X inhibits the enzyme neprilysin, increasing beneficial vasodilatory peptides (ANP, BNP) that reduce blood pressure and fibrosis, while Y blocks the angiotensin II receptor (AT1R), countering vasoconstriction, sodium retention, and maladaptive remodeling.
ARNi (angiotensin-receptor and neprilysin inhibitor)
X = sacubitril
Y = valsartan
These drugs block the sodium-glucose co-transporter 2 (SGLT2) protein in the kidneys, preventing the reabsorption of glucose into the blood. They may improve renal haemodynamics: increased sodium sensing at the macula densa will lead to afferent arteriole constriction. This constriction reduces excessive blood flow into the glomerulus (hyperfiltration), thereby lowering glomerular capillary pressure and providing long-term protection against renal damage.
Glifozins