Post Midterm: via Final review + more?
1/109
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
110 Terms
Describe systemic diseases related to cardiac manifestations: diabetes
Description:
hypo-secretion of insulin
Cardiac involvement:
poor systolic and diastolic function
LV remodelling, concentric LVH
Describe systemic diseases related to cardiac manifestations: Neuromuscular diseases (2)
Description:
Two main ones:
Friederich’s Ataxia
Ducheme muscular Dystophy
inherited, causes muscle weakness include heart muscle
Cardiac involvement:
associated with dilated cardiomyopathy
Describe systemic diseases related to cardiac manifestations: Ankylosing spondylitis
Description:
chronic inflammatory disease of the spine
Cardiac involvement:
aortic dilation
arrhythmias/atrial fibrillation
Describe systemic diseases related to cardiac manifestations: Rheumatoid arthritis
Description:
inflammation of joints
Cardiac involvement:
atherosclerosis risk
MI, stroke
atrial fibrillation
hypertension
heart failure
Describe systemic diseases related to cardiac manifestations: Scleroderma
Description:
autoimmune disease of the connective tissues → thickening and tightening of the skin, organs (lungs and heart)
Cardiac involvement:
pulmonary hypertension → can lead to right heart failure
Describe systemic diseases related to cardiac manifestations: Lupus Erythematosus
Description:
autoimmune disease
joints, skin, kidneys, blood, brain, heart, and lungs
Cardiac involvement:
effusions/pericarditis
myocarditis
valve thickening
heart failure
CAD
Describe acquired diseases related to cardiac manifestations: Chagas Cardiomyopathy - “kissing bugs”
Chagas Cardiomyopathy is dilated cardiomyopathy that forms 20-30 years post Chagas infection
can also lead to heart failure
Describe systemic diseases related to cardiac manifestations: hereditary connective tissue disorders
Description:
3 main types:
Marfan syndrome
Ehlers-Danlos syndrome
Loeys-Dietz syndrome
connective tissue diseases → leaky →weakens blood vessels
Cardiac involvement:
aortic dilation and dissections
What are the main characteristics of Marfan Syndrome? What heart abnormalities mainly occur in (3)
Characteristics
tall/scoliosis/hypermobility of joints
high palate/poor vision/ long limbs
Diseases:
mitral valve prolapse
aortic dilation or dissection
aortic regurgitation
Describe the main anatomy of aorta (5)
Aortic root: area between LVOT and ST junction
Ascending aorta: extends from ST junction to origin of brachiocephalic artery, roughly ~5cm long
Aortic arch: extends brachiocephalic artery to ligamentum arteriosum, which lies near the subclavian artery, roughly ~4cm long
Aortic isthmus: located at site of ligamentum ateriosum, where aorta is fixed to thoracic cage (cannot move bc attached to bone but vulnerable to trauma)
Descending aorta: extends from the aortic isthmus to diaphragm
What are the layers of the aorta? (3)
tunica externa
tunica media
tunica intima
Describe anatomy of aortic valve (4 components)
Annulus: provides structural support to cusps
Cusps: 3 half-moon (semilunar) in shape; right, left, non-coronary
Commissures: where the cusps come together
Interleaflet triangles: extensions of the ventricular outflow tract
Describe anatomy of Aortic Root/ Sinuses of Valsalva, includes 4 components
section between the LVOT and Asc. Ao
specifically the inferior attachment of the aortic cusps to the ST junction
Includes:
aortic cusps
Sinuses of Valsalva
Comissures
Interleaflet triangles
Describe the diseases of the great vessels/aorta (6)
Atherosclerosis – Plaque builds up in artery wall
Aortic aneurysm – Weakening or degeneration layers of wall → dilation
Aortic dissection – Intimal tear → blood splits wall
Intramural hematoma – Bleeding inside wall (no tear)
Blunt chest aortic trauma – Sudden force → aortic tear on isthmus
Coarctation of the aorta – Congenital narrowing of descending aorta
What are the 2 types of aortic aneurysm
Saccular: occurs due to weakening of vessel wall at one point, leading to an out pouching of vessel wall
Fusiform: uniform and symmetrical dilation of entire circumference of the vessel (most common)
What are some etiologies for aortic aneurysms?
Connective tissue disease
Bicuspid AoV
Aortic stenosis
Atherosclerosis → intimal layer thickened due to fatty plaque and they destroy elastic fibres and muscle cells in medial layer → weaken
Describe Sinus of Valsalva Aneurysm (SVA)
rare congenital anomaly seen on PSAX or PLAX
not medical emergency because born with it! → still report
weakening or absence of the media layer
weakened sinus dilates and forms an aneurysm, can cause holes

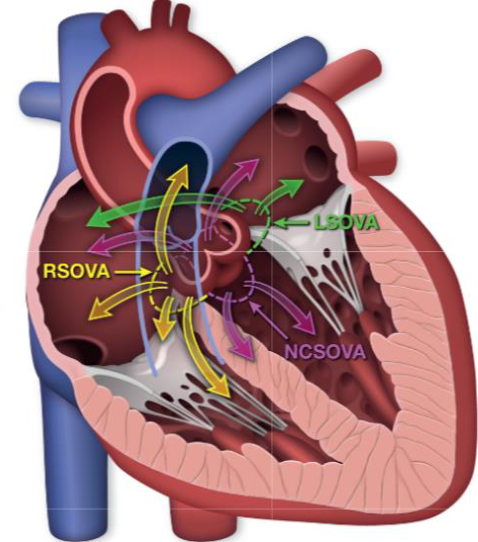
What are some complications of SVA (3)
LSOVA
may rupture into LA or RA
NCSOVA
may rupture into LA, RA, LV, or ventricular septum
RSOVA (most common)
may rupture into LV, RA, RV (across septum), pericardium, adjacent main pulmonary artery
can cause most problems: obstruction, dissection, compression, acute MI, heart block, tamponade
Overall: more blood is being moved back into the heart instead of being pumped out
Describe aortic dissection
dissection is a tear in the intimal layer that allows blood to enter the media layer
creates a blood filled lumen separated from the true lumen by an intimal flap
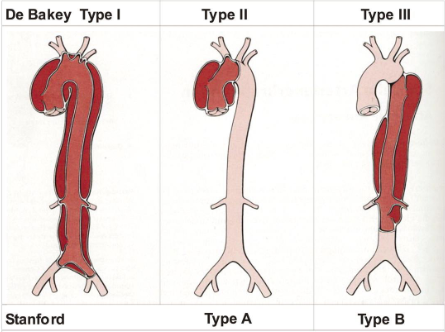
What are the 2 classifications of aortic dissections, and their sub types?
DeBakey:
Type I: originates in the proximal ascending aorta. Involves ascending aorta, arch, and variable lengths of descending and abdominal aorta
Type II: ascending aorta only
Type III: begins in the descending aorta
Standard:
Type A: any dissection that involves ascending aorta
Type B: any dissection that does not involve ascending aorta
Describe Kawasaki disease origin and complications
Etiology: usually via viral infection, auto-immune disease, inflamed blood vessels (coronary)
Complications:
vasculitis: inflammation of blood vessels, usually coronary arteries
coronary artery dilation
giant aneurysm
myocardial infarction
blood clots within coronary
coronary artery aneurysm
Describe the two main pulmonary artery disease and etiology (2)
dilation of pulmonary artery → Marfan syndrome
stenosis of pulmonary artery → congenital
Differentiate AoV stenosis and sclerosis
Aortic Stenosis: reduced (restricted) opening of the aortic valve in systole via calcium build up over time
valve appears brighter than normal, does not open well, has velocity over 2.5 m/s
Aortic Sclerosis: thickening of the valve leaflets with no restriction of blood flow
valve appears brighter than normal, still opens well, has velocity less than 2.5 m/s
Describe pathology causes of aortic stenosis (3) and how common
1) Congenital: roughly 30-40% of cases
bicuspid (but not all are stenotic)
unicuspid or quadricuspid
subvalvular or supravalvular
2) Acquired: Calcific: > 50% of cases
calcium deposits overtime (age) prevent opening
3) Acquired: Rheumatic: <10% of cases
history of rheumatic fever, the scar tissue creates rough surface → narrow opening + place for calcium to collect
Echo differentiation from calcific versus rheumatic valves?
calcific:
commissural fusion commonly absent
“chunks” of brightness (calcium) seen, uneven brightness
rheumatic/age:
commissural fusion is triangular systolic orifice
slightly brighter than normal, uniformly thickened leaflets
What are the two types of congenital bicuspid AoV?
Without a raphe
rare
cusps usually equal in size
With a raphe (seam/union)
more common
cusps unequal in size
RCC/LCC → RCC/NCC → NCC/LCC
What are the consequences of congenital bicuspid AoV? (4)
1) Aortic root dilation: higher risk for aortic aneurysm or dissections
2) Coarctation of aorta: narrowing in desc. ao
3) Supravalvular aortic stenosis
4) Ventricular septal defects (VSD)
Describe subvalvular stenosis
fibrous membrane or muscular ring in LVOT (below AoV) → obstruction in the outflow
Leads to: narrow LVOT → septal hypertrophy = thicker IVS → dynamic obstruction → mitral valve may get “sucked up”
What is dynamic obstruction?
degree of stenosis varies depending on loading conditions, or variable blockage of blood flow instead of fixed narrowing
severity changes based on: cardiac cycle, HR, volume, movement of leaflets
Describe supravalvular stenosis
uncommon narrowing of aorta just above AoV
Dysplasia (abnormal) aortic wall → hour glass type
membrane with central orifice
Hypoplasia (underdeveloped) ascending aorta
Describe hemodynamic consequences of aortic stenosis (2)
Concentric LVH
narrowed AoV → increased pressure load → LV wall thickens to compensate (concentric LVH) → LV stiff + lower compliance
lead to diastolic dysfunction → LV does not relax well → poor filling
increased LAP → back into lungs → increase pulmonary pressures → SOB
Usually, normal EF, but will drop in severe cases
Ischemia
increased muscle mass due to LVH → increase oxygen demand
compressed coronary vessels due to LVH → decrease oxygen supply
angina: decrease oxygen → decrease LV contractility → systolic dysfunction
Dilated ascending aorta
high velocity jet hitting aortic wall → weakens and stretches wall
Signs and symptoms of aortic stenosis (4)
Systolic Ejection Murmur (SEM)
Angina (may be w/ CAD)
myocardial ischemia (LVH →↑ demand + ↓ supply)
Syncope (fainting)/ presyncope (feeling light-headed)
fixed cardiac output → ↓ cerebral perfusion during exertion
forward failure → not enough blood flow to brain
Shortness of breath and fatigue
reduced cardiac output → ↓ systemic perfusion
backward failure → lung problem cause by pressure backup
Role of Sonography in Aortic Stenosis (6)
Determine presence of aortic stenosis vs sclerosis
Determine etiology
Assess LV wall thickness
Measure aorta
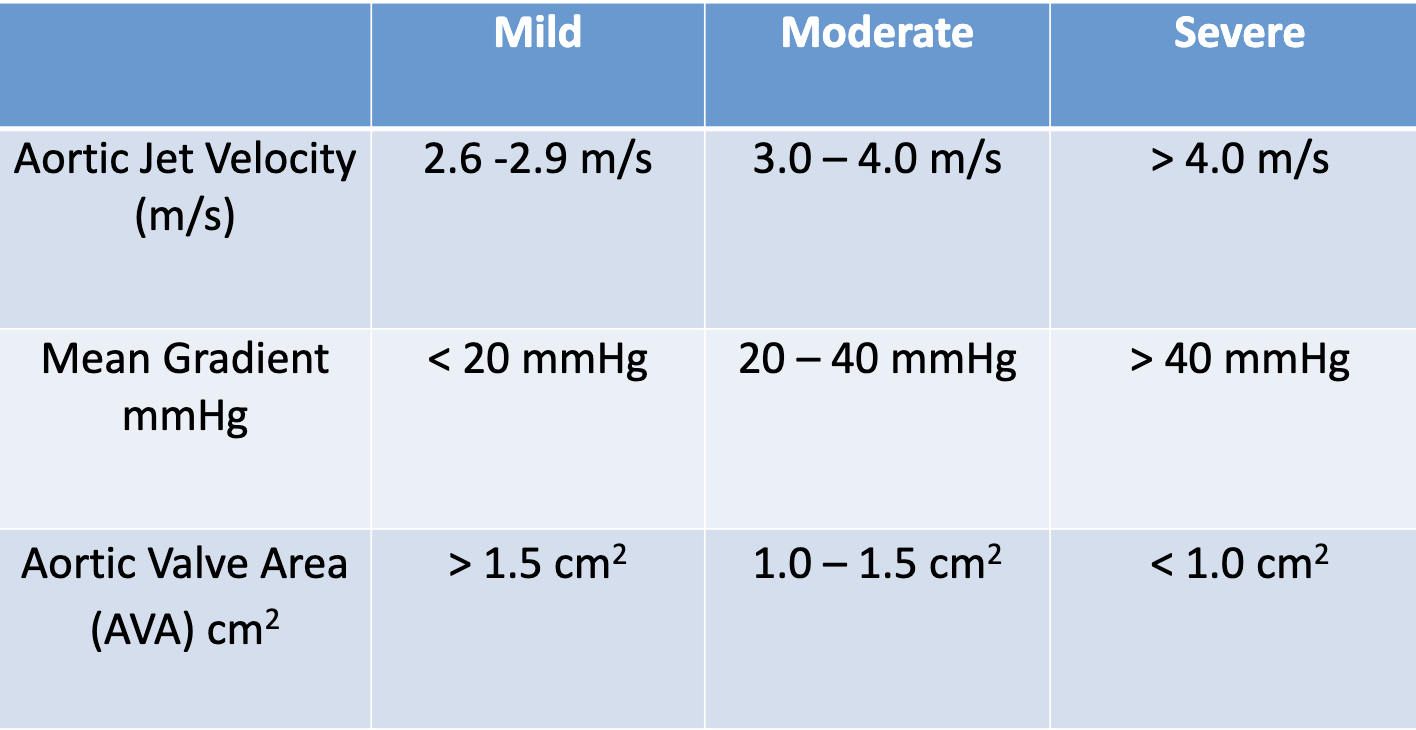
Estimate severity of aortic stenosis
Identify associated abnormalities (regurgitation)
How to estimate severity of aortic stenosis (3)
Mean gradient (mean PG)
AoV VTI trace (from CW in 5Ch)
Maximum Jet Velocity (Vmax)
AoV VTI trace (from CW in 5Ch)
Continuity equation for AVA:
LVOT diameter
LVOT VTI (from PW in 5Ch)
AoV VTI (from CW in 5Ch)
Extra: double check with PEDOF to find peak Vmax through the valve in different windows (small enough that you can go anywhere)
What is the continuity principle? How is it related in normal vs stenotic valve?
states what flows in, must flow out
in normal valves: the velocity should be the same before and after the valve
in stenotic valves: blood will have to speed up past the valve due to narrowing
What is VTI and why do we use it?
What: area under Doppler curve
Unit is cm because VTI = velocity/time
Why: In human body, velocity is not constant at any given time and varies at different parts of the vessel
VTI sums up all the individual velocities over time to find a representative overall velocity
What are the normal values for the Vmax, meanPG, and AVA (VTI)?
Can you use continuity equation of AoV when there is LVOT obstruction?
no, bc equation compares normal flow to stenotic flow
with LVOT obstruction → velocity is already high in LVOT and the velocity in AoV will still be high since there was no time to slow down
Have to assess visually or perform a valve planimetry in SAX
What is 2D Planimetry of AVA
PSAX view, trace opening in mid systole
not routinely performed due to many pitfalls (hard to be consistent)
could be used to double check the AVA if clearly seen
What is dimensionless velocity ratio (DVI)?
removes error associated with LVOT diameter by removing CSA from the continuity equation
velocity ratio = VLVOT/ VAoV
closer to 0 = more severe
closer to 1 = more normal
What is aortic insufficiency (AI) / aortic regurgitation (AR) ?
inability of the aortic valve leaflets to remain closed during diastole, resulting in some stroke volume leaking back into LV
increase in left ventricular end-diastolic volume
Role of Sonography in Aortic Insufficiency
Determine etiology
Assess LV size and systolic function
Measure aorta
Estimate severity of regurgitation
List the common etiologies of AI/AR (4)
aortic annulus/ aortic root dilation: congenital, AS, athero. infection, trauma
cusp abnormalities: bi/quad-cuspid, calcific, infection, rheumatic fever
annular or aortic root distortion: aortic root inflammation
loss of aortic cusp (commissural) support: VSD or dissection
Whats are some causes of acute vs chronic AI?
causes of acute AI (emerg.):
trauma
dissection
endocarditis
causes of chronic AI:
bicuspid AoV
rheumatic AoV
calcific AoV
Difference between aortic dilation and aneurysm
Aortic aneurysm:
dilation involving all layers of the aorta 1.5x greater than normal diameter
Aortic dilation:
dilation involving all layers of the aorta, larger than accepted normal values, but not large enough to be considered an aneurysm
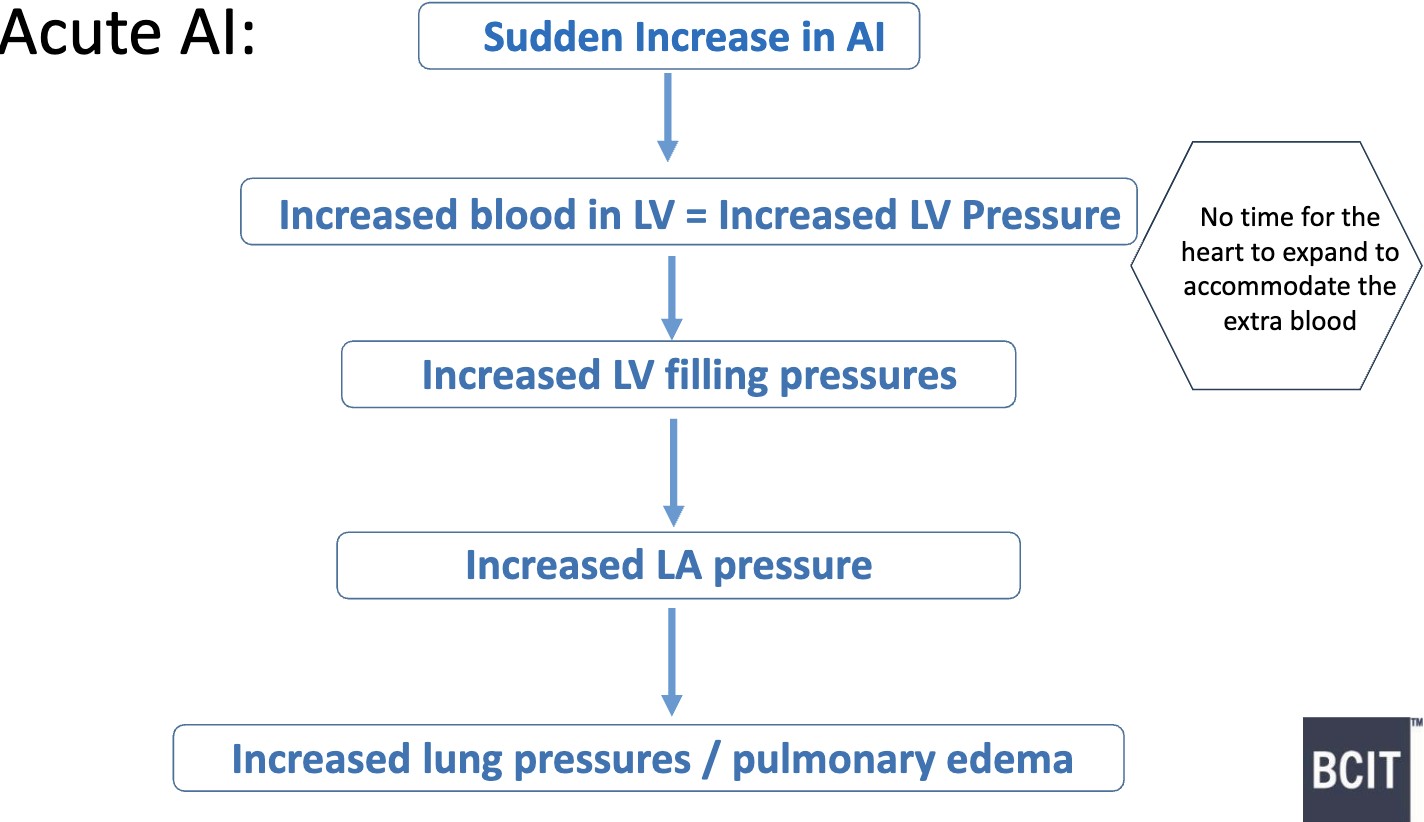
What are some hemodynamic consequences for Acute AI?
if severe enough → medical emergency & immediate valve replacement needed
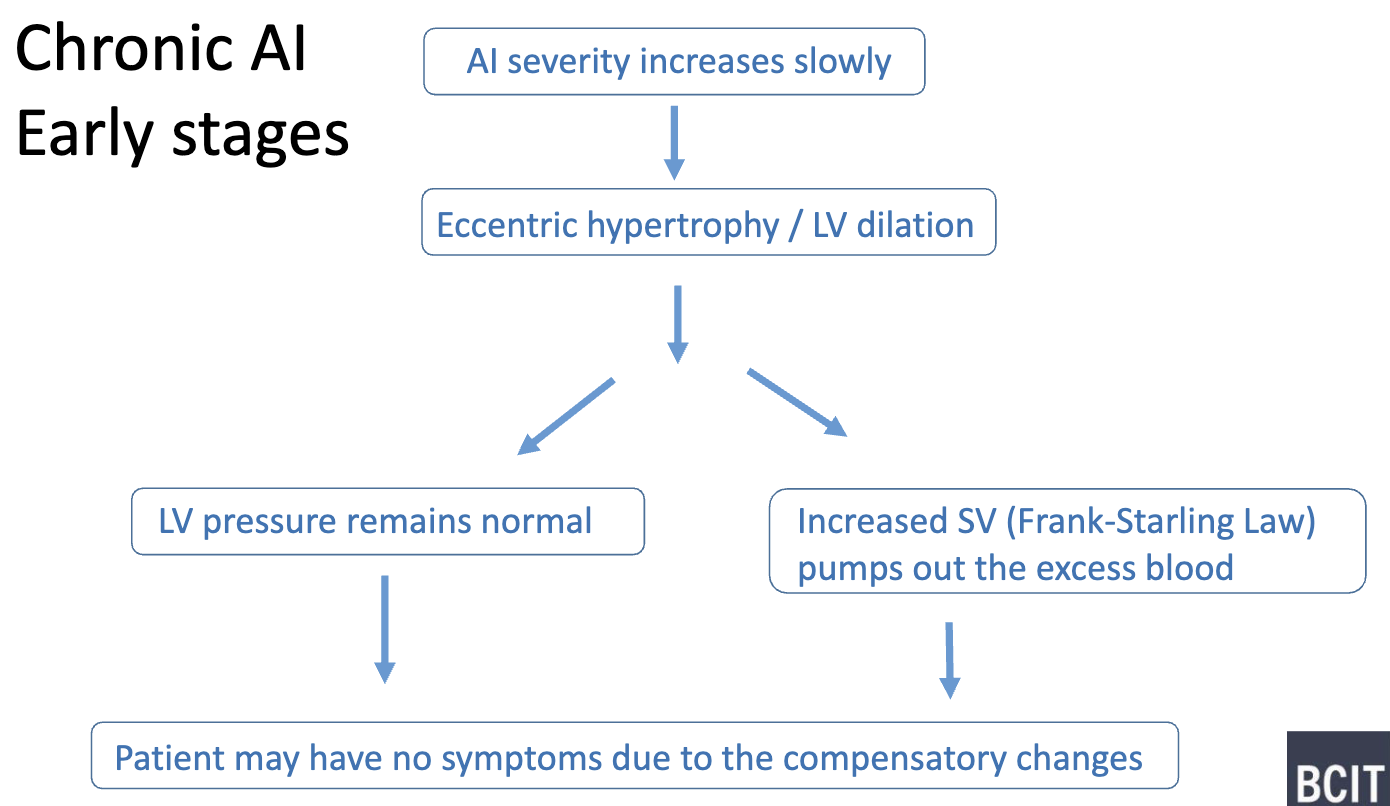
What are some hemodynamic consequences for Chronic AI- early stages?
LVH also help reduce wall stress (LaPlace’s Law)
wide pressure pulse bc still AI
EF remain normal
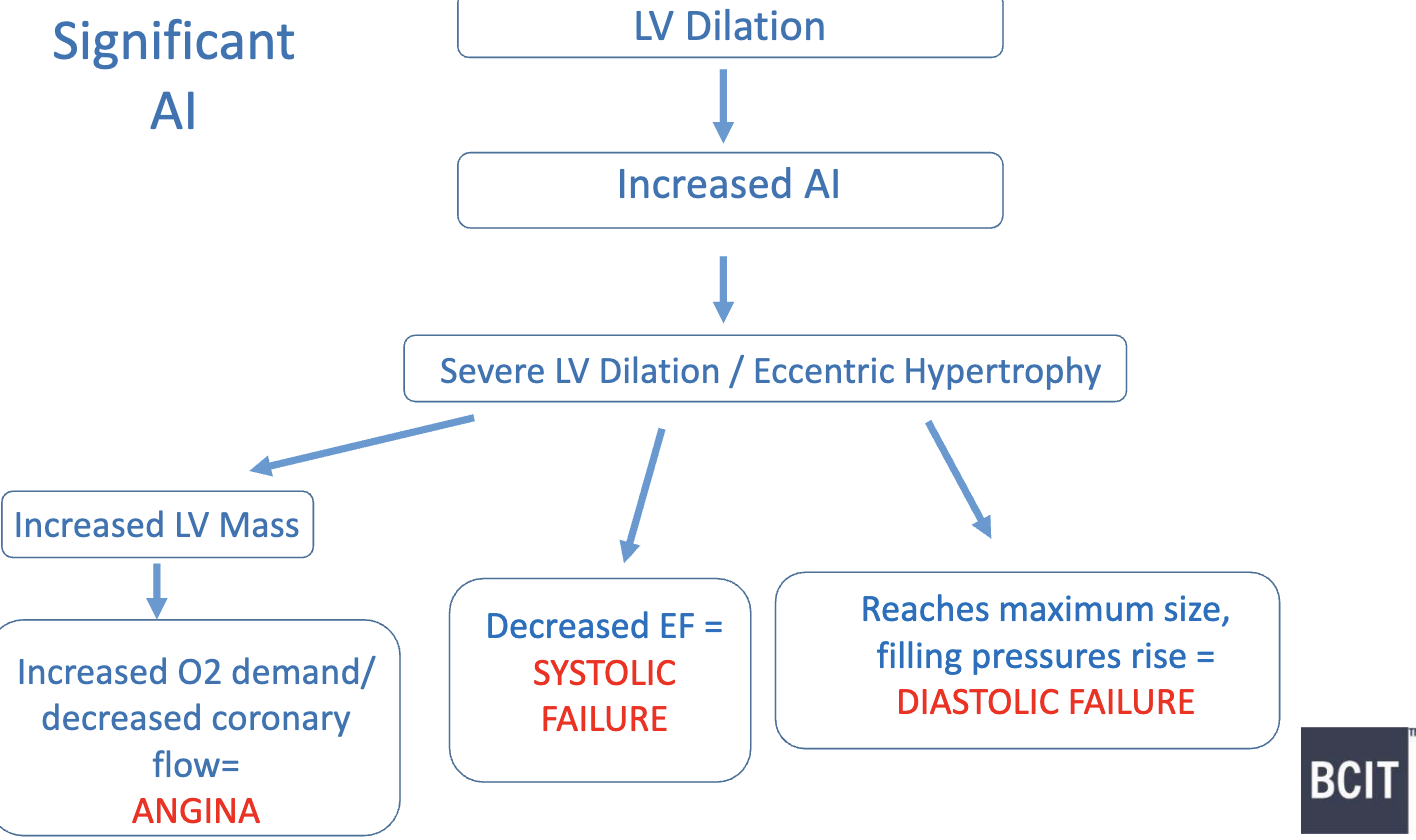
What are some hemodynamic consequences for Chronic AI- long standing?
even wider pulse pressure
low diastolic aorta pressure → coronary artery perfusion drops → decreased oxygen supply to heart muscles
How to estimate severity of Aortic Insufficiency? (5)
Visual assessment
Flow reversal in Desc. Ao
Pressure Half-Time (PHT)
Jet-width and Vena Contracta
PISA/EROA
What is PHT?
time it takes for the initial pressure gradient to drop to half of its initial value
“how fast blood is flowing backward through the AoV”
unit: msec
How do you measure PHT for Aortic Insufficiency?
Obtain CW Doppler Trace in AI jet
5 or 3-chamber as parallel as possible
2 points:
highest velocity on trace (around 5 m/s in early diastole regardless of severity)
line along the slope on the AI profile
machine calculates PHT
What is the general idea of PHT for Aortic Insufficiency?
Mild/Trival AI:
Long PHT → flat slope → slow pressure equalization
LV P rises slowly (blood from LA) → stays low → Ao P slowly falls → thus equalized slower
Moderate/Severe AI:
Short PHT → steep slope → fast pressure equalization
LV P rises faster (blood from LA + Ao) + Ao P falls faster (less blood ejected) → thus equalized faster
How to determine Flow Reversal in descending aorta in Aortic Insufficiency?
for moderate/severe AI → diastolic flow reversal seen in descending and/or abdominal aorta
Assess PW from both suprasternal and subcostal window:
if only SSN → suggest moderate AI
if both SSN and subcostal → suggest severe
Compare abnormal retrograde flow compare to normal antegrade flow
Describe the abnormal flow (flow reversal) in SSN and subcostal view for Aortic Insufficiency
Suprasternal/SSN Window:
Flow reversal seen above the baseline during diastole
Subcostal Abdominal Window:
Flow reversal seen below the baseline during diastole
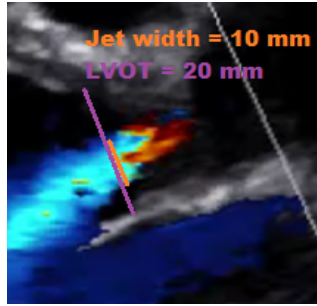
How do you assess Jet Width to Height Ratio for Aortic Insufficiency?
Jet width: width of AI jet as it travels through LVOT area
Steps:
Zoom in LVOT with colour
Freeze frame with AI jet
measure width of AI jet in LVOT area (same location as LVOT diameter)
Divide jet width by LVOT diameter to get percentage:
Calculate: (Jet width)/(LVOT diameter) * 100
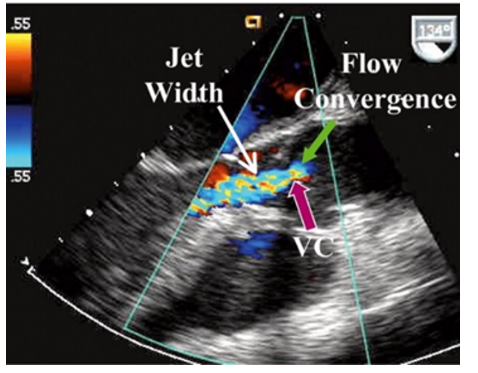
How do you assess Vena Contracta for Aortic Insufficiency?
Vena contracta: narrowest part of the jet in the area between the proximal flow convergence zone and the regurgitant jet
Steps:
measure in PLAX
Zoom in on the aortic valve and LVOT
store cine that shows flow convergence dome, VC, and regurgitant jet
freeze and measure the narrowest portion of the AI jet
How do you assess PISA/EROA for Aortic Insufficiency?
Proximal Isovelocity Surface Area (PISA): measures the effective regurgitant orifice area (EROA), which is the size of the “hole” that the regurgitant blood flows through
bigger EROA, the worse regurgitation
Steps:
Find the regurgitant jet on CDI
Change Nyquist limit in same direction as jet
Align CW Doppler and measure aliasing radius of PISA:
r = radius of the regurgitant orifice to aliased velocity
Measure peak velocity of regurgitant jet (Vmax)
Calculate EROA using the 3 bolded values
What is flow convergence zone and isovelocities?
Iso-velocities: series of hemispheric shells of uniform velocity
Flow convergence zone: where regurgitant blood rushes backwards towards the regurgitant orifice, there is flow acceleration just proximal to the orifice (just before the valve)
made up of iso-velocities
area of increased velocity
Describe the anatomy of mitral valve (5)
annulus: structural support, D-shaped
leaflets:
anterior: short & wide, 1/3 of annulus
posterior: long & narrow, 2/3 of annulus
Scallops: subdivision (A1-A3, P1-P3)
commissures: where leaflets meet labeled by location
chordae tendineae: connecting leaflets for pap muscles, prevent prolapse during systole
papillary muscles: prevent prolapse during systole
anterolateral and postermedial
What are some etiologies of mitral stenosis (3)
congenital mitral stenosis
parachute mitral valve → chordae attached to single papillary muscle
supravalvular ring
rheumatic mitral valve stenosis
rheumatic fever earlier in life → hockey stick, commissural fusion
mitral annular calcification (MAC)
calcium build up as you age and starts at PMVL
What is one of the differentiation between MAC or rheumatic mitral stenosis?
absence of commissural fusion in MAC differentiates it from rheumatic mitral valve stenosis
it is fused in rheumatic !
Describe underlying hemodynamic changes associated with mitral stenosis
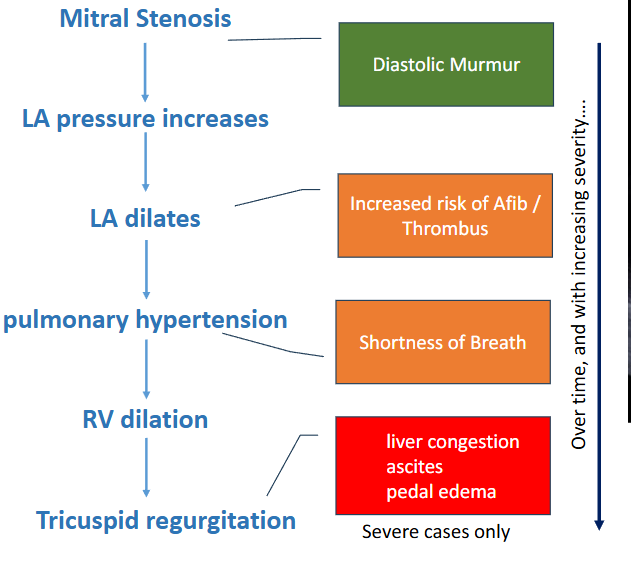
Role of Sonography for Mitral Stenosis (6)
Determine presence of MS
Determine Etiology
Assess LA: size (dilated?), presence/absence of thrombus
Identify associated lesions (MR or AS)
Estimate severity of stenosis
Other factors to consider → assess degree of hypertension bc as MS increases, pulmonary pressures increase
Two ways to determine presence of Mitral Stenosis
Colour Doppler: LV inflow jets may be eccentric, looks like a candle flame
M-Mode: mitral EF slope refers to the function of the rate of LA emptying and LV filling → hallmark is that slope more flat because blood flow is slower
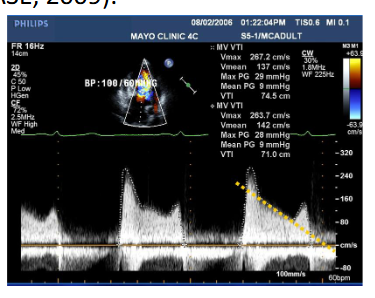
How to assess severity of mitral stenosis? (3)
Mean pressure gradient
MV VTI Trace (from CW in 4Ch)
Mitral valve area (MVA) via:
PHT
Tip to baseline of trace (from CW in 4Ch) → MVA = 220/PHT
Continuity equation:
LVOT diameter
LVOT VTI (from PW in 5Ch)
MV VTI (from CW in 4Ch)
Planimetry (not BC)
PISA (not BC)
Describe PHT on normal versus stenotic mitral valve
Flow through the MV is affected by both diastolic filling patterns and by the health of the MV
normal valve → the predominant factor that affects flow through the valve is diastolic filling patterns.
Short PHT → steep slope
stenotic valve → the predominant factor that affects flow through the valve is the health of the valve
Longer PHT → flatter slope
When is MVA via PHT not valid? (4)
Tachycardia
shortens diastole/ changes shape of trace, E & A merge
Significant aortic regurgitation
increases LV pressure / affects MV inflow patterns
Changes in diastole
increases LV pressure / affects MV inflow patterns
Post valve surgery
no longer “stenotic” and this measurement is no longer valid
Describe determination of PHT in Bimodal Doppler Spectrums for Mitral Stenosis
deceleration slope is sometimes bimodal, the decline of mitral flow velocity being more rapid in early diastole than during the following part of the E wave
recommended to trace deceleration slope in mid-diastole rather than early-diastole
Define mitral regurgitation
retrograde (backward) flow of blood from the left ventricle into the left atrium during systole
What differentiates primary/organic vs secondary mitral regurgitation?
Primary/organic
mitral valve leaflets and/or the mitral valve apparatus is abnormal, leading to mitral regurgitation
Secondary:
diseases that affect another part of the heart, but cause MR → example: dilated LV
valve itself is normal but leaks due to other problems with the heart
Describe flail leaflet
ruptured chordae tendineae causes loss of stability of leaflet → leaflet tip points in towards the LA when valve is closed
Describe ruptured pap
rare
pap muscle ruptures off the LV wall → causes flail leaflet with the entire pap muscle seen traveling between both the LA and LV every time the valve opens and closes
Describe cleft leaflet
congenital hole in MV leaflet → usually in AMVL
Describe SAM
systolic anterior motion of AMVL
AMVL moves up into the LVOT during systole when valve is closed
causes posteriorly directed MR
Describe tethered leaflet
Remodelling of the LV causes chordae tendineae to be mal-positioned and causes MR
Describe how dilated LV cause MR
leaflets can no longer fully close
Describe mitral valve prolapse