UNIT 7: BREAST, THORAX, LUNGS (SD; PROCEDURES)
1/86
Earn XP
Description and Tags
NOTES AND BOOK
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
87 Terms
centimeter ruler
small pillow
disposable gloves
client handout for BSE
slide for specimen
equipment for assessing the breast
shape
symmetry
nipples
masses
discharges
lymph nodes
what to assess for in breasts (in PE forms)
inspection:
have the client disrobe and sit with arms hanging freely
explain what you are observing to help ease client anxiety
(breast)
assessment procedure for size and symmetry of breasts
round and pendulous
one breast may normally be larger than the other
(breast)
normal finding for size and symmetry of breasts
round and pendulous
(breast)
sample documentation for shape of breasts
R (Right) Breast is slightly larger than L (Left) Breast. (FEMALE FINDING)
Symmetric on both sides. (MALE FINDING)
(breast)
sample documentation for symmetry of breasts
inspection:
be sure to note the client’s overall skin tone when inspecting the breast skin
note any lesions
(breast)
assessment procedure for color and texture of breasts
note the color, size, shape, and texture of the areolas of both breasts
(breast)
what to note for areolas of breasts
positions for assessing retraction & dimpling of breast tissue:
note size, direction, dryness, lesions, bleeding, discharge, retraction, dimpling & presence of supernumerary nipples; also note for areolas for color, size, shape, texture & presence of Montgomery tubercles
(breast)
what to note for nipples of breasts (INSPECTION)
dark pink to dark brown
round and may vary in size
small montgomery tubercles are present
(breast)
normal finding for areolas of breasts
nearly equal bilaterally in size and are in the same location on each breast
usually everted but may be inverted or flat
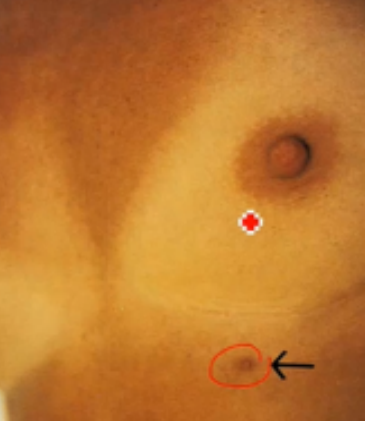
normal variation: supernumerary nipples (found at your embryonic milk line)
(breast)
normal finding for nipples of breasts
everted bilaterally (FEMALE FINDING), with light brown areola and Montgomery tubercles present. No dimplings, lesions, inflammations or retractions present.
(breast)
sample documentation for nipples of breasts
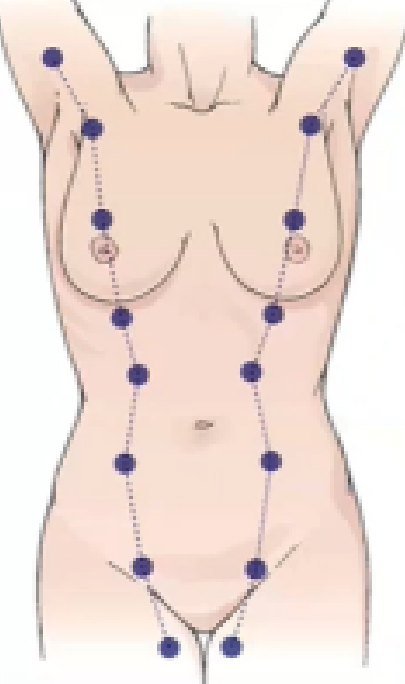
embryonic “milk” line
(breast)
landmarks to locate for supernumerary nipples
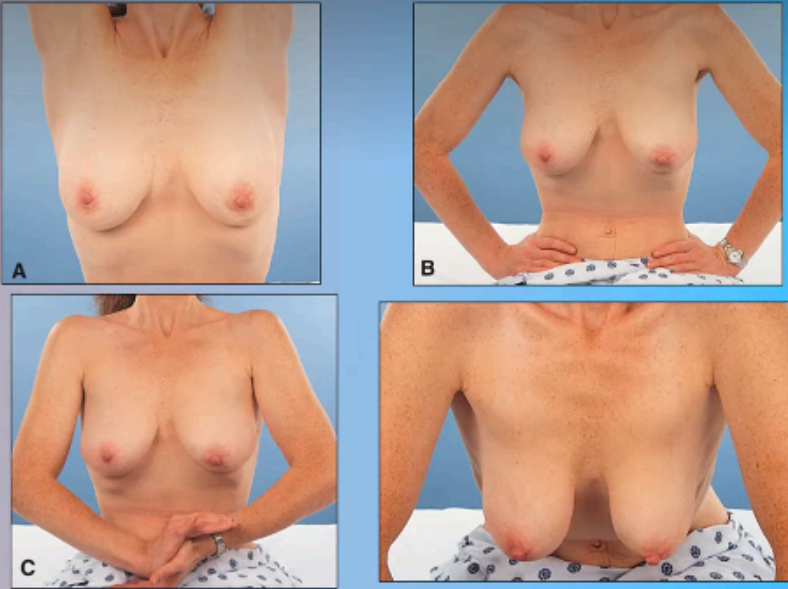
inspection:
ask the client to remain seated while performing several different maneuvers.
ask the client to raise her arms overhead then press her hands against her hips.
next ask her to press her hands together (these actions contract the pectoral muscles)
ask the client to lean forward from the waist.
the nurse should support the client by the hands or forearms (this is a good position to use in women who have large, pendulous breasts)
(breast)
assessment procedure for retraction and dumpling of breasts
clients breast should rise symmetrically, with no sign of dimpling or retraction.
breast should hang freely and symmetrically
(breast)
normal finding for retraction and dumpling of breasts
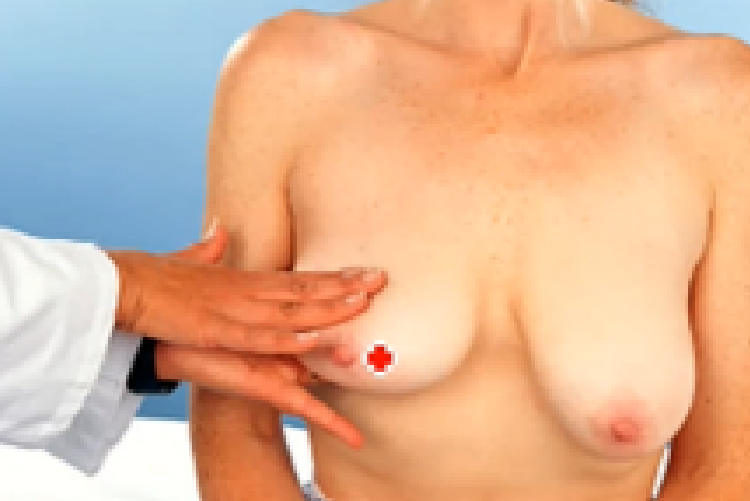
palpating the pectorals in a circular (start near sa nipple then going outwards in a circular manner)
wedge (from the area near nipple going outwards in a straight manner)
vertical Drip (basta ang pagpalpate kay magsugod ka laterally then padung medially sa near sa sternum, direction of palpation kay pinasnake).
bimanual Breast palpation is done for those na dako ug breasts (FEMALE).
put a small pillow or towel under the breast palpated.
use flat pads 3 fingers to palpate
(breast)
assessment procedure for masses of breasts (palpation)
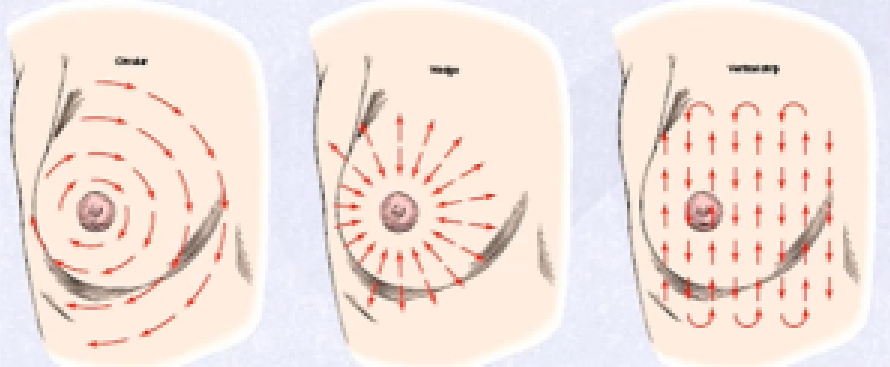
(breast)
patterns for breast palpation:
bimanual breast palpation (for large breasts):
(breast)
name of procedure
palpation:
note location, size in centimeters, shape, mobility, consistency, and tenderness
condition of the skin over the mass
if you detect any lump, refer client to further evaluation
(breast)
what to note for masses of breasts
no masses
a firm inframammary transverse ridge may normally be palpated at the lower base of the breasts.
fibrocystic breast tissue that feels ropy, lumpy, or bumpy in texture is referred to as "nodular" or "glandular" breast tissue.
benign breast disease consists of bilateral, multiple, firm, regular, rubbery, mobile nodules with well-demarcated borders.
pain and fullness occurs just before menses
(breast)
normal finding for masses of breasts
no masses or tenderness present
(breast)
sample documentation for masses of breasts
palpation:
note any discharge
if spontaneous discharge occurs from the nipple, a specimen must be applied to a slide and the smear sent to the laboratory for cytologic evaluation
(breast)
what to note for nipples of breasts (palpation)
wear gloves to compress the nipple gently with your thumb and index finger
(breast)
assessment procedure for nipples of breasts (palpation)
nipple may become erect and the areola may pucker in response to stimulation.
milky discharge is usually normal only during pregnancy and lactation.
however, some women may normally have a clear discharge
(breast)
normal finding for nipples of breasts (palpation)
slightly pinching the nipples
(breast)
assessment procedure for discharges of breast
minimal amount, clear discharge (FOR FEMALES).
no discharge (FOR MALES)
(breast)
sample documentation for discharges of breasts
note for palpable axillary lymph nodes & epitrochlear node & note characteristics
(breast)
what to note for lymph nodes of breast
non-palpable,
it is only palpable if the patient is suffering from an illness or if the patient is undergoing menstruation (FOR FEMALES)
(breast)
sample documentation for lymph nodes of breasts
let px raise arm and palpate all lymph nodes
(breast)
assessment procedure for lymph nodes of breast

(breast)
palpating axillary lymph nodes:

(breast)
palpating epitrochlear lymph nodes:
examination gown & drape
gloves
stethoscope
light source
mask
skin marker
metric ruler
equipment for assessing the thorax & lungs
configuration
retraction & bulging
depth, rhythm, & quality of respiration
tenderness & sensation
crepitus
fremitus
chest expansion
diaphragmatic excursion
breath sounds
adventitious sounds
voice sounds:
egophony
bronchophony
whispered pectoriloquy
what to assess for in chest & lungs (in PE forms)
inspection:
while client sits with arms at the sides,
stand behind client and observe the position of scapulae and the shape and configuration of the chest wall
some clinicians prefer to inspect the entire thorax first, followed by palpation of the anterior & posterior thorax, then percussion and auscultation of the anterior & posterior thorax
(chest & lungs)
assessment procedure for configuration
note anterior & posterior thorax for shape, symmetry, anteroposterior to transverse diameter, position of scapulae, sternum & slope of ribs
(chest & lungs)
what to note for configuration
scapulae are symmetric and non-protruding
(more in book pg 138)
(chest & lungs)
normal finding for configuration
symmetric, non-protruding Scapulae, Anteroposterior is less than the transverse diameter, Sternum is straight and located at the midline, Ribs slope downward with symmetric Intercostal spaces. The costal angle is within 90 degrees.
(chest & lungs)
sample documentation for configuration
watch as client breathes and note use of muscles
(chest & lungs)
assessment procedure for use of accessory muscles
the client does not use accessory (muscle/shoulder) muscles to assist breathing
(chest & lungs)
normal finding for use of accessory muscles
diaphragm
(chest & lungs)
major muscle at work
this is evidenced by expansion of the lower chest during inspiration
inspection:
examine the sternum and intercostal spaces
(chest & lungs)
assessment procedure for retractions & bulging
not noted
(chest & lungs)
sample documentation for retractions & bulging
inspection:
note breathing characteristics as well as rhythm, & depth;
also note use of accessory muscles & client’s positioning
(chest & lungs)
what to note for depth, rhythm & quality of respiration
regular, relaxed, effortless, quiet without use of accessory muscles
– these are the sternocleidomastoid and scalene.
(chest & lungs)
sample documentation for depth, rhythm & quality of respiration
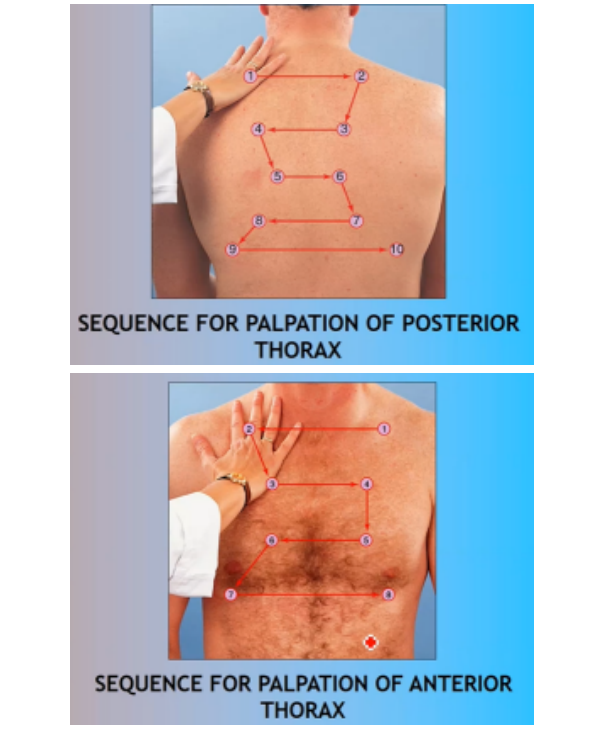
(chest & lungs)
sequence for palpating:
(palpation):
use your fingers to palpate for tenderness and sensation.
start with your hand positioned over the left clavicle (over the apex of the left lung) and move your hand left to right, / comparing findings bilaterally.
move your hand systematically downward toward the midline at the level of the breasts and outward at the base to include the lateral aspect of the lung.
the established sequence for palpating the anterior thorax serves as a guide for positioning your hands.
anterior thoracic palpation is best for assessing the right lung's middle lobe.
(chest & lungs)
assessment procedure for tenderness, sensation, and surfaces masses
no tenderness, pain or unusual sensation reported.
temp. equal bilaterally.
(chest & lungs)
sample documentation for tenderness, sensation, and surfaces masses
(palpation):
use your fingers and follow the sequence when palpating
(chest & lungs)
assessment procedure for crepitus
not noted
no palpable crepitus
(chest & lungs)
sample documentation for crepitus
(palpation): palpate with your ulna of wrist
use the ball or ulnar edge of one hand to assess for fremitus
(vibrations of air in the bronchial tubes transmitted to the chest wall).
as you move your hand to each area, ask the client to say "ninety-nine."
assess all areas for symmetry and intensity of vibration.
the ball of the hand is best for assessing tactile fremitus because the area is especially sensitive vibratory sensation.
(chest & lungs)
assessment procedure for fremitus
(palpation):
note symmetry & intensity of vibration
(chest & lungs)
what to note for fremitus
symmetric; easily identified in the upper region of the lungs & decreased intensity at the bases.
(chest & lungs)
sample documentation for fremitus
(palpation) let px have deep breaths and (Pa)
place your hands on the posterior chest wall with your thumbs at the level of T9 or T10 and pressing together a small skin fold.
as the client takes a deep breath, observe the movement of your thumbs.
(chest & lungs)
assessment procedure for chest expansions
symmetric at 5cm apart anteriorly and posteriorly
(chest & lungs)
sample documentation for chest expansions
when the client takes a deep breath, the examiner's thumbs should move apart symmetrically.
because of calcification of the costal cartilages and loss of the accessory musculature, the older client's thoracic expansion may be decreased, although it should still be symmetric.
(chest & lungs)
normal finding for chest expansions
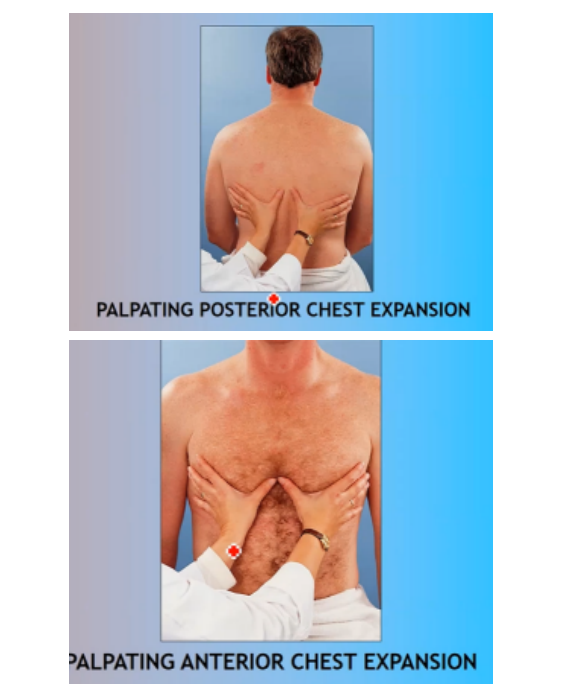
(chest & lungs)
palpating for chest expansion:
(pecussion)
start at the apices of the scapulae and percuss across the tops of both shoulders.
then percuss the intercostal spaces across and down, comparing sides.
percuss to the lateral aspects at the bases of the lungs, comparing sides.
(chest & lungs)
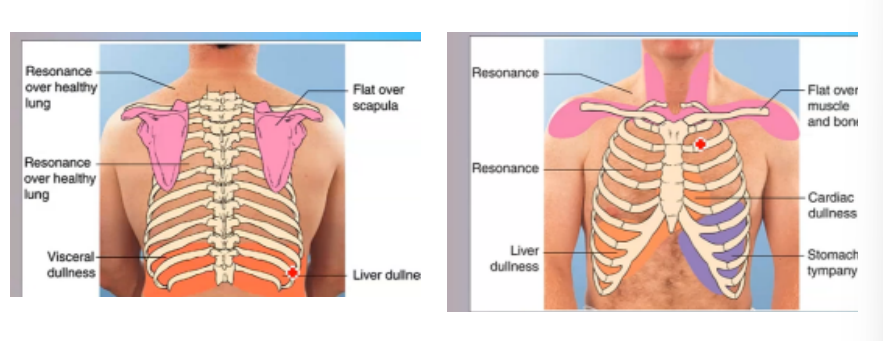
assessment procedure for percussion (of tone)
resonance is the percussion tone elicited over normal lung tissue
percussion elicits flat tones over the scapula
(chest & lungs)
normal finding for percussion (of tone)
resonant over all lung fields.
(chest & lungs)
sample documentation for percussion (of tone)
note for percussion tone of anterior & posterior thorax
(chest & lungs)
what to note for percussion (of tone)
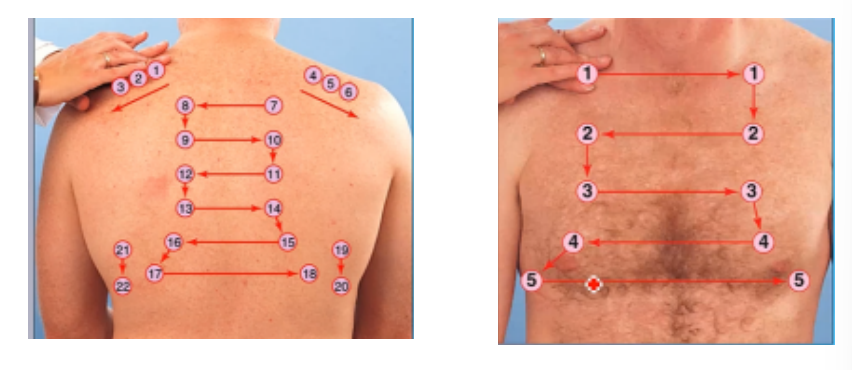
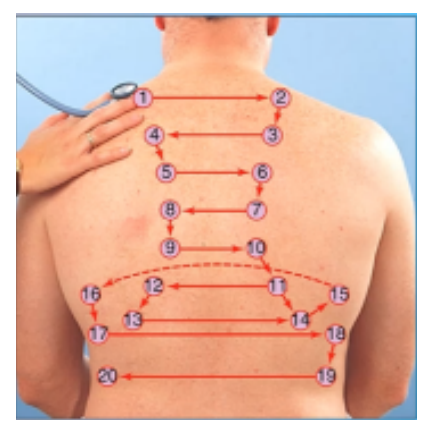
(chest & lungs)
sequence of percussion posterior & anterior thorax:
(chest & lungs)
normal percussion tones for posterior & anterior thorax:
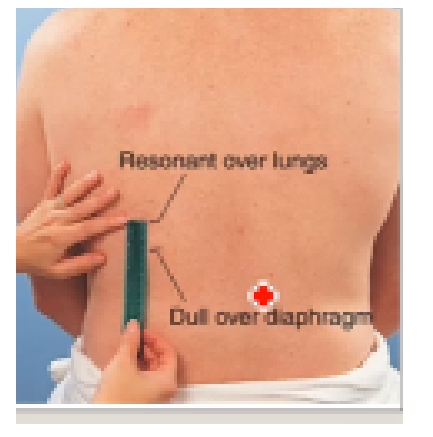
(percussion)
ask the client to exhale forcefully and hold the breath,
beginning at the scapular line (T7), percuss the intercostal spaces of the right posterior chest wall
percuss downward until the tone changes from resonance to dullness. Mark this level and allow the client to breathe:
next ask the client to inhale deeply and hold it.
percuss the intercostal spaces from the mark downward until resonance changes to dullness.
mark the level and allow the client to breathe.
measure the distance between the two marks.
perform this assessment technique on both sides of the posterior thorax.
(chest & lungs)
assessment procedure for diaphragmatic excursion
excursion should be equal bilaterally and measure 3-4 cm in adults.
the level of the diaphragm may be higher on the right because of the position of the liver.
in well-conditioned clients, excursion can measure up to 7 or 8 cm
(chest & lungs)
normal finding for diaphragmatic excursion
4cm & equal bilaterally
(chest & lungs)
sample documentation for diaphragmatic excursion
(auscultate)
do not attempt to listen through clothing or a drape, which may produce additional sound or muffle lung sounds that exist.
place the diaphragm of the stethoscope firmly and directly on the posterior chest wall at the apex of the lung at C7.
ask the client to breathe deeply through the mouth for each area of auscultation (each placement of the stethoscope) in the auscultation sequence so that you can hear the inspiratory and expiratory sounds
be alert to the client's comfort and offer times for rest and normal breathing if fatigue is becoming a problem
deep breathing may be especially difficult for the older client, who may fatigue easily.
thus offer rest as needed.
auscultate from the apices of the lungs at C7 to the bases of the lungs at T10 and laterally from the axilla down to the seventh or eighth rib.
listen at each site for at least one complete respiratory cycle
(chest & lungs)
assessment procedure for breath sounds
three types of normal breath sounds may auscultated— bronchial, be bronchovesicular, and vesicular
breath sounds are considered normal only in the area specified.
heard elsewhere, they are you can best hear inspiratory considered abnormal sounds.
for example, bronchial breath sounds are abnormal if heard over the peripheral lung fields
sometimes breath sounds may be hard to hear with obese or heavily muscled clients due to increased distance to underlying lung tissue.
(chest & lungs)
normal finding for breath sounds
bronchial Sounds noted over trachea, Bronchovesicular sounds noted over major bronchi and vesicular noted over peripheral lung fields.
(chest & lungs)
sample documentation for breath sounds
note for presence & location of bronchial, bronchovesicular, & vesicular breath sounds
(chest & lungs)
what to note for breath sounds
(chest & lungs)
sequence for auscultating posterior thorax:

(chest & lungs)
sequence for palpation of anterior thorax:
by intensity, pitch, and duration during inspiration and expiration.
(chest & lungs)
how are normal breath sounds classified as:
(auscultation)
adventitious sounds are sounds added or superimposed over normal breath sounds and heard during auscultation.
be careful to note the location on the chest wall where adventitious sounds are heard as well as the location of such sounds within the respiratory cycle.
(chest & lungs)
assessment procedure for adventitious sounds
no adventitious sounds, such as crackles (discrete and discontinuous sounds) or wheezes (musical and continuous, are auscultated.
(chest & lungs)
normal finding for adventitious sounds
not noted
(chest & lungs)
sample documentation for adventitious sounds
note for presence & location of crackles pleural friction rub or wheezes
(chest & lungs)
what to note for adventitious sounds
note for bronchophony, egophony & whispered pectoriloquy
(chest & lungs)
what to note for voice sounds
ask the client to repeat the letter "E” while you listen over the chest wall.
(chest & lungs)
assessment procedure for egophony
soft & muffled; letter “E”
(chest & lungs)
sample documentation for egophony
voice transmission will be soft and muffled but the letter "E" should be distinguishable
(chest & lungs)
normal finding for egophony
ask the client to repeat the phrase "ninety-nine" while you auscultate the chest wall.
(chest & lungs)
assessment procedure for bronchophony
soft and muffled; indistinct
(chest & lungs)
sample documentation for bronchophony
voice transmission is soft, muffled, and indistinct.
the sound of the voice may be heard but the actual phrase cannot be distinguished.
(chest & lungs)
normal finding for bronchophony
ask the client to whisper the phrase " 1, 2, 3" while you auscultate the chest wall.
(chest & lungs)
assessment procedure for whisper pectoriloquy
very faint & muffled
(chest & lungs)
sample documentation for whisper pectoriloquy
transmission of sound is very faint and muffled.
it may be inaudible.
(chest & lungs)
normal finding for whisper pectoriloquy