S2W8: Patients with Learning Difficulties
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
Define the term learning difficulties
Reduced intellectual ability and difficulty w/ everyday activities, e.g: household tasks, socialising or managing money, which affects someone for their whole life.
People w/ a learning disability tend to take longer to learn + may need support to develop new skills, understand complex information + interact with other people.
The level of support someone needs depends on indiv factors, incl the severity of their learning disability
Which ocular conditions are people with learning difficulties 10x more likely to have?
amblyopia
blepharitis – common in people with Down’s syndrome
cataract
concomitant strabismus
cortical visual impairment
entropion – common in people with Down’s syndrome
field defects
high refractive error
impaired accommodation
keratoconus
nystagmus
reduced vision
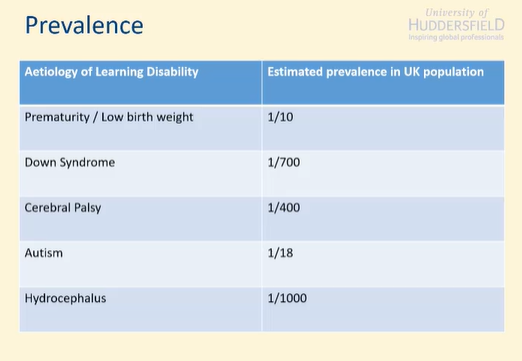
Prevalence of learning disabilities in the UK
Prematurity / Low birth weight 1/10
Down Syndrome 1/700
Cerebral Palsy 1/400
Autism 1/18
Hydrocephalus 1/1000
What is the difference between prematurity and low birth weight?
Prematurity –
<37 weeks
Full gestation period=40 weeks
Low Birth weight –
<2500g
Not to be confused w/ risks for retinopathy of prematurity!
Screen for ROP at 32 weeks + 1.5kg
What are the ocular associations of prematurity and low birth weight?
ROP
Refractive Error
More likely to develop myopia + strabismus
Strabismus
14% of infants born before 28 weeks
Overall childhood population is 2%
What is Down Syndrome?
Duplication of all or part of chromosome 21. (we have 23 normally)
3 copies instead of 2.
50% of Down syndrome patients have a congenital heart defect.
Mild to moderate learning disability
Short attention span
Poor judgement
Impulsive behaviour
Slow learning
Delayed language + speech development
What are the ocular associations of Down Syndrome?
Refractive error
Higher incidence
Oblique astigmatism more common
More likely to change over time.
VA and Contrast Sensitivity
Reduced VA + CS
Can be helped with early intervention
Strabismus
Incidence is ~35%
Later onset than general population
~4.5 years rather than 3
Accommodative weakness
Poor amplitude + accuracy in 80%
May req near addition.
Cataract
Either congenital or early onset
~45 years of age (normal =60-70 years)
Keratoconus
Incidence 5.5%, much higher than general population (0.27%)
What is cerebral palsy?
Brain injury
Before, during or shortly after birth.
May be due to maternal infection during pregnancy
Cytomegalovirus
Rubella
Chicken pox
Toxoplasmosis
Trauma
What are the classifications of cerebral palsy?
Spastic
Muscle weakness / Stiffness
Athetoid
Affects muscle tone / causes involuntary spasms
Ataxic
Affecting balance / coordination
Combination of factors
What are the systemic effects of cerebral palsy?
Difficulty with feeding
Drooling
Speech and language difficulties
Epilepsy
Hearing loss
Scoliosis
50% have learning difficulty
What are the ocular associations of of cerebral palsy?
RE
60-80%
Due to failure of emmetropisation process
Larger cyls
Higher incidence of reduced VA.
More severe Cerebral palsy leads to an inc’d likelihood of poorer VA.
Generally, two lines less than age matched control.
Strabismsus
50% incidence
XOT +SOT (non accommodative).
Incomitant strabismus and nystagmus (trauma)
Poor accommodative facility
May need Rx for close work
Might need an add
Multifocals not suitable due to limited head control.
Needs to have SV
Visual field defects
Depends on what part of brain affected: Occipital/parietal/temporal lobe
Abnormal optic nerve appearance
Cerebral visual impairment
Affecting visual pathway + visual cortex rather than eye
What is autism?
‘a lifelong developmental disability that affects how people perceive the world and interact with others.’
National Autistic Society
50-70% have a learning disability
Depression, Anxiety and OCD more common in people with autism
What are the ocular associations of autism?
Refractive error
High refractive error in 20-30%
Accommodative issues
3x more prevalent
Strabismus
Inc’d incidence by factor of 2
What is hydrocephalus?
Building up of cerebrospinal fluid inside the skull.
Congenital
Often have a learning difficulty
Acquired
Caused predominantly by spina bifida.
Incomplete closure of tissues around spinal cord.
What are the ocular associations of hydrocephalus?
Optic atrophy
15-40% of those with congenital condition
Inc’d incidence of strabismus, eye movement anomalies + RE
What should you do when examining patients with learning difficulties?
a) make reasonable adjustments to the patient’s eye care, for example by using a range of tests and procedures that are appropriate to the needs of the patient
b) seek their consent to get a briefing from a relative or carer, if necessary
Encourage pt to attend with a relative or carer if they are unlikely to be able to give full and accurate details, history + RFV
Learning difficulties -Consent
You must…
You must respect the rights of pts to be fully involved in decisions about their care.
You must obtain consent from pts who have capacity before starting treatment.
Mental Capacity Act 2005
Learning difficulties -Consent
To make a decision about care the patient should be able to:
a) understand and remember the information provided
b) weigh up the information provided
c) tell you their decision.
What are your responsibilities regarding presumption of capacity and determining lack of capacity?
You must work on the presumption that every adult pt (over 18) has the capacity to make decisions about their care, and to decide whether to agree to, or refuse, an examination, investigation or treatment.
You must regard a patient as lacking capacity only once it is clear that, having been given all appropriate help and support, they cannot understand, retain, use or weigh up the information needed to make that decision, or communicate their wishes.
You must not assume that a pt lacks capacity to make a decision solely bc of their age, disability, appearance, behaviour, medical condition (incl mental illness), beliefs, apparent inability to communicate, or the fact that they make a decision with which you disagree
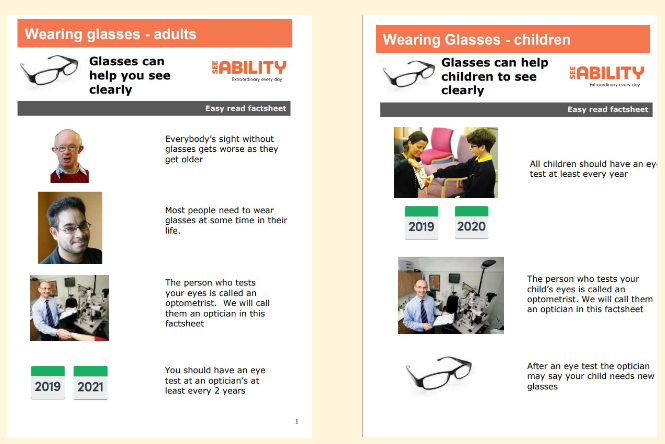
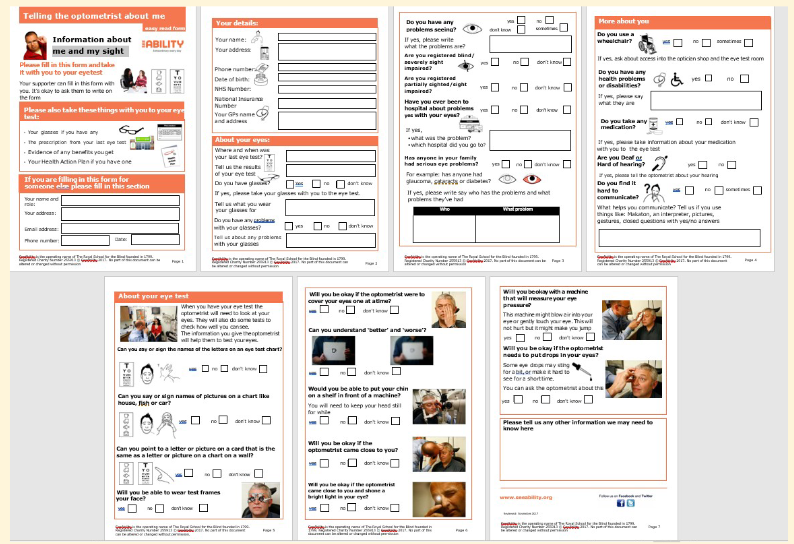
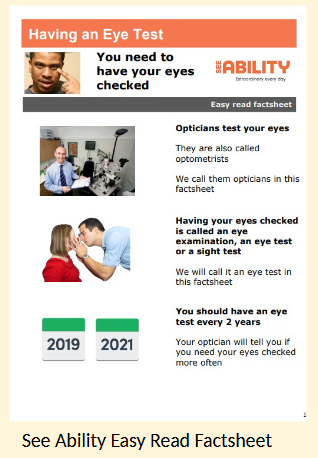
Discuss the materials available to support optometrists, patients and carers during eye care procedures
Discuss the amendments made to a sight test for patient with learning difficulties.
What to do when testing patients with learning difficulties?
Encourage the pt to visit your premises before their eye examination to help them become familiar and comfortable with the environment.
Encourage the pt + carer to complete SeeAbility’s ‘Telling the optometrist about me’ form and bring it to the eye examination
Find out how the patient likes to communicate and how their disabilities affect them, incl if they are particularly sensitive to touch, lights and sounds.
Find out about any recent signs, symptoms or behavioural changes that might be relevant
Ask to refer to the patient’s health action plan or communication passport, if they have one.
Be prepared to spend longer on the examination and to arrange repeat visits to obtain full and valid results
How to test Vision/Visual Acuity in patients with learning difficulties?
Preferential looking tests may be needed if patients can’t recognise letters / shapes.
Demonstrate with carer.
When testing, how should accommodative function, visual fields, refraction and internal examination be assessed in patients with learning diffculties?
Use an objective measure of accommodative function (e.g. dynamic retinoscopy) to determine the accuracy of the patient’s accommodation
Attempt VF assessment, even if only by using confrontation techniques
Use cycloplegic examination, if necessary, to determine the full RE, esp if problems with fixation
Use mydriasis, if necessary, to internally examine the eye
Give clear information to the patient or their carer about the effects of eye drops
e.g will sting when they go in, how long they last, what to expect
When testing, how should examination limitations and potential referrals be managed?
Record any reasons for limitations on the examination + results obtained
Consider whether you need to refer the patient for further tests (e.g. examination under anaesthetic or electrophysiological tests)
If referring, involve learning disability health professionals for advice about access to health care and treatment
How should you communicate with patients with learning difficulties?
Talk directly to the patient, rather than their carer.
Take time to speak clearly.
Explain what you are doing in plain English.
Communication
Warn the patient before you touch them.
Explain and show them the equipment you are using.
Communication
You must provide information to patients in a way that they understand.
GOS contractors need to ensure that patients receive information in a suitable, accessible format, unless the provision of this would be at disproportionate or unreasonable cost.
How should feedback be provided to the patient and their carer?
You should provide the patient + their carer with a written, as well as a verbal, report
This should be copied to the pt’s GP if the pt consents
Feedback from my optometrist form
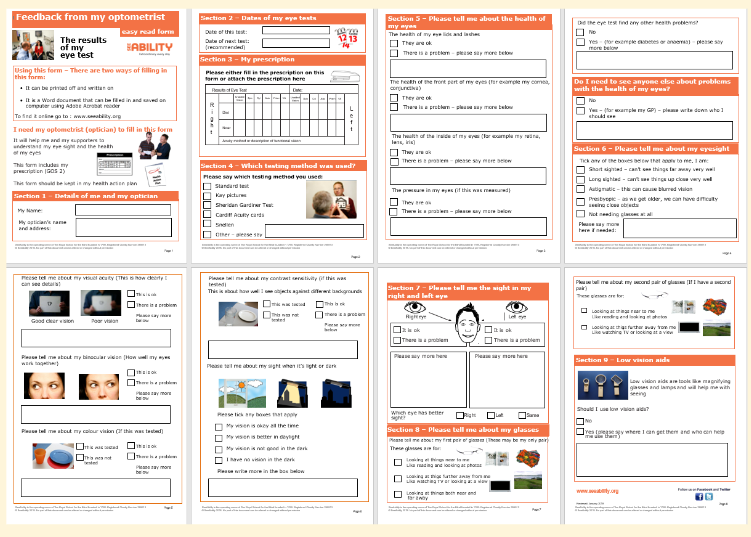
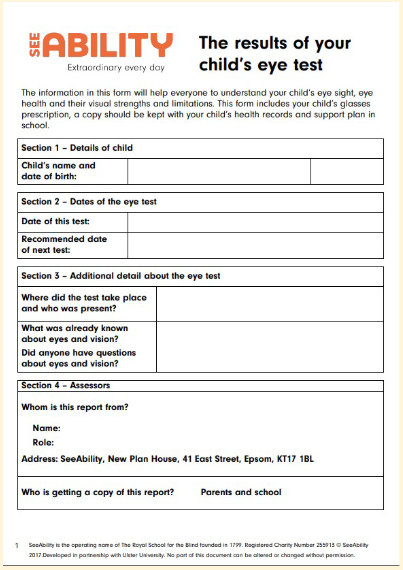
Child’s Form
See ability: Results of your Child’s eye test
What should be considered when supplying spectacles to a patient with a learning disability?
Consider labelling spectacles with the patient’s name, date of supply and whether they are for distance or near tasks
Labelling should be suitable in terms of the patient’s dignity, infection control and type of frame supplied