Mesenteric
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
Protocol for Mesenteric Study
RUQ first - eliminate GB as pain source
Pre and post-prandial images - 2D, color, spectral
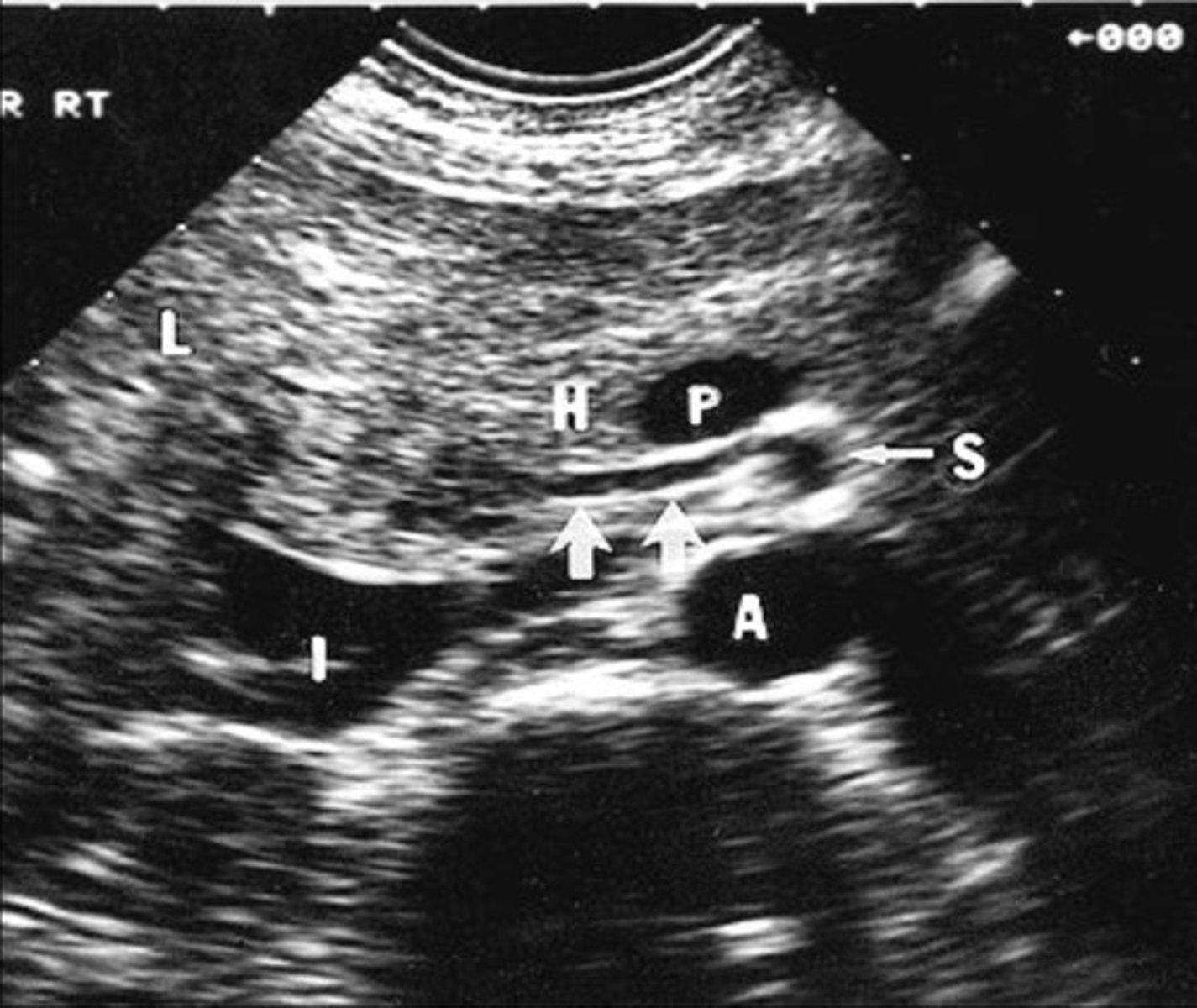
Aorta at level of celiac axis and SMA
Origin of celiac axis
Origin of SMA
Origin of IMA
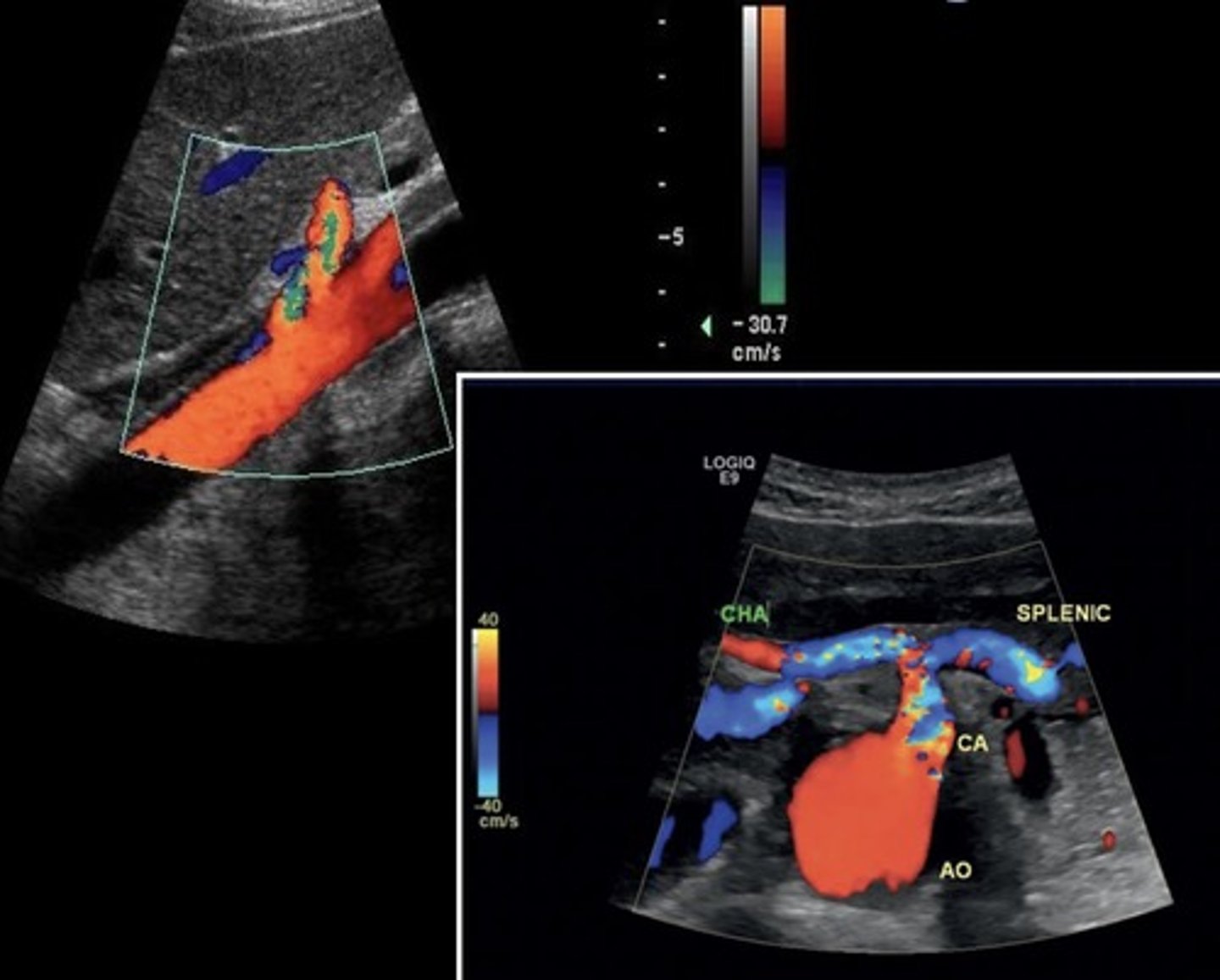
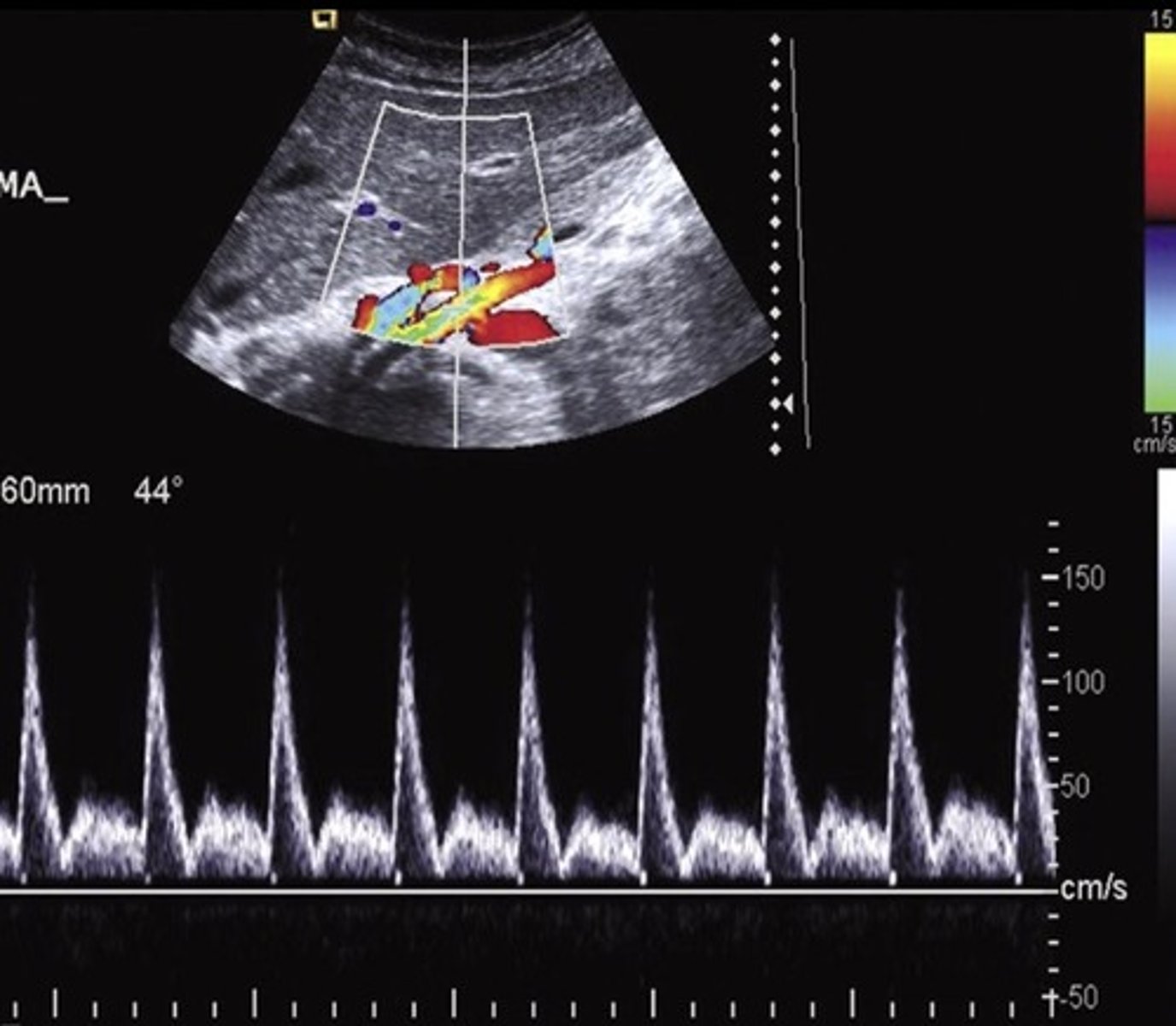
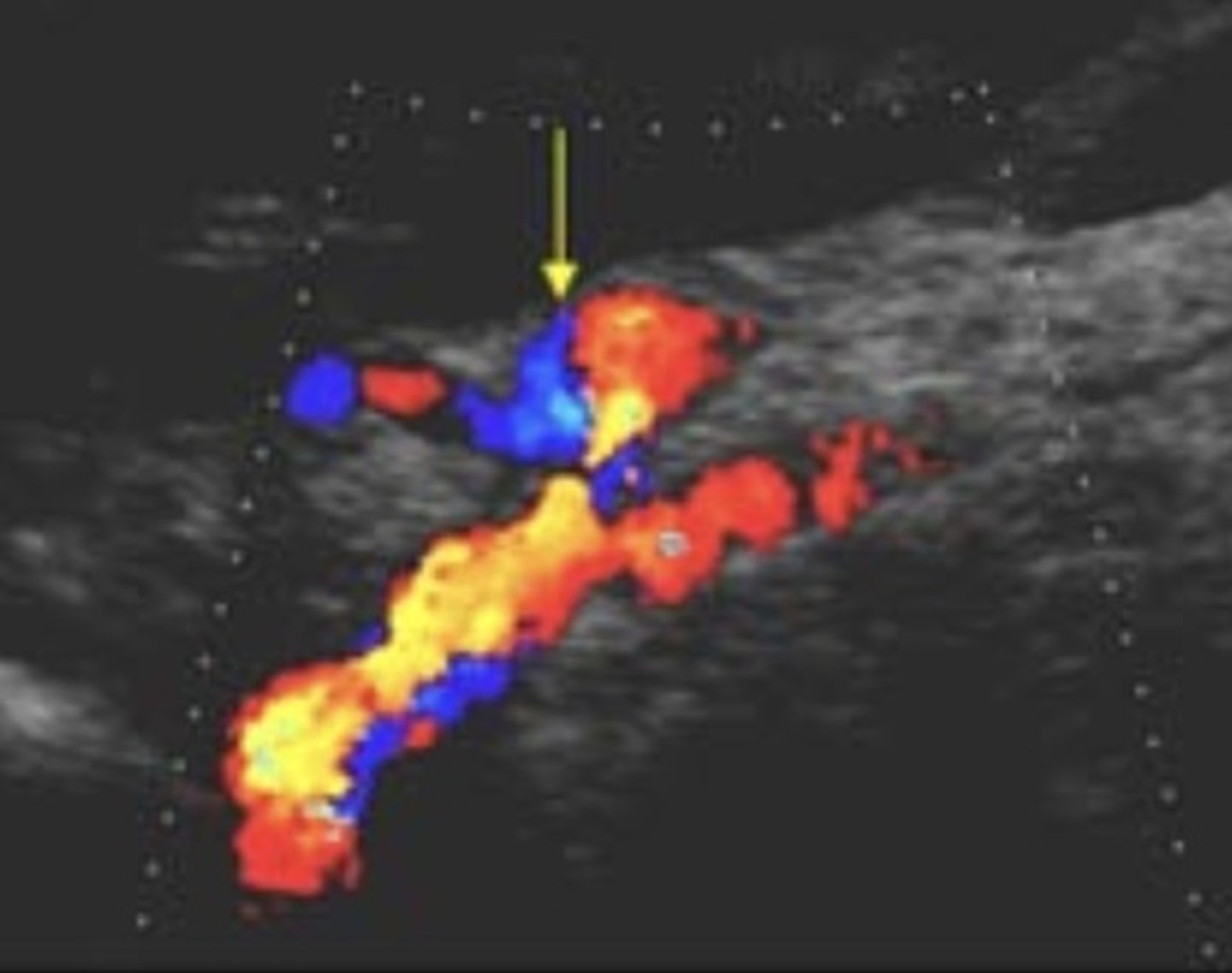
Celiac Artery
Celiac Artery Doppler Waveform
Low resistant
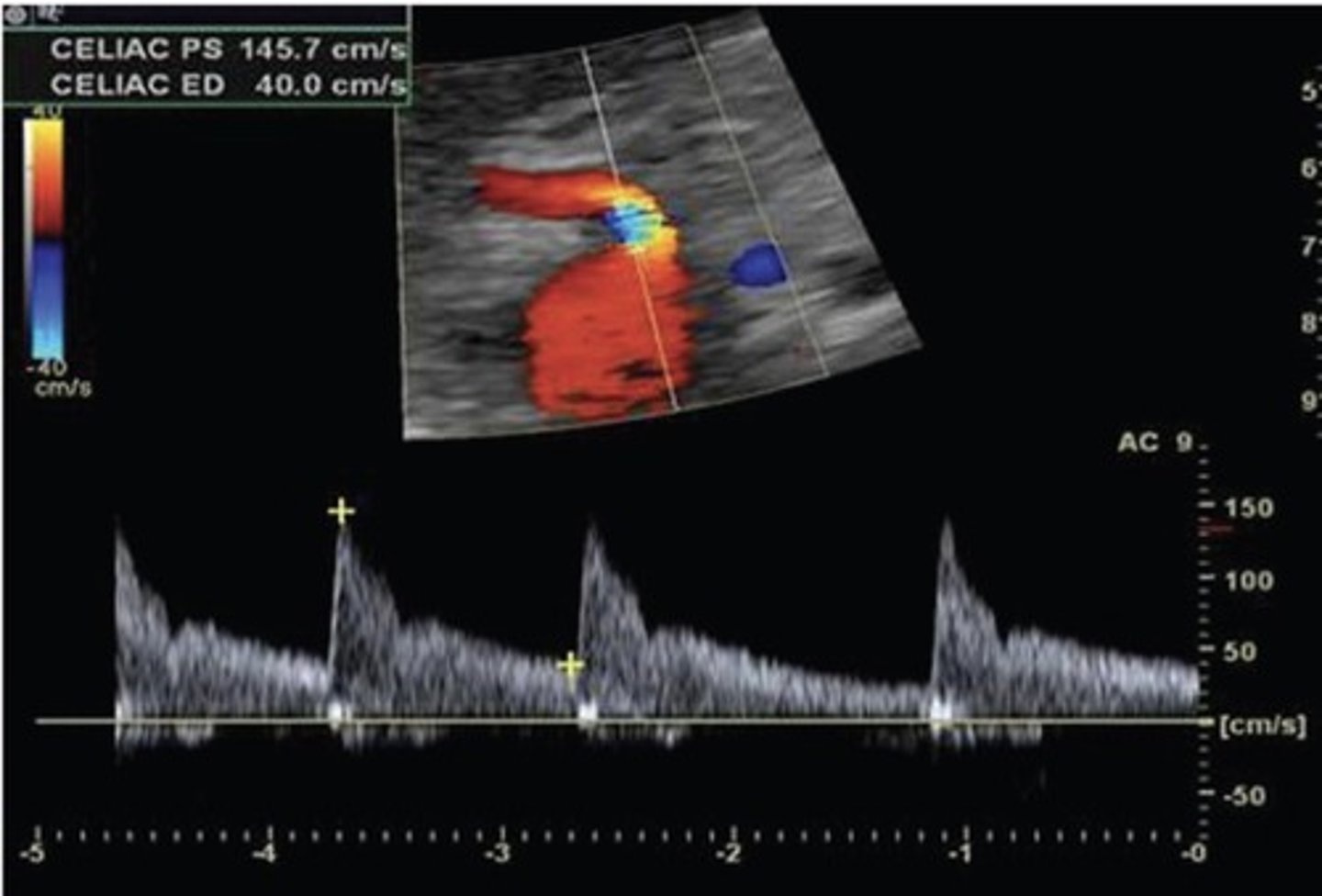
Celiac Artery PSV
101 cm/sec
Celiac Artery Occlusion
Results in SMA collaterals diverting blood through gastroduodenal artery toward the liver and spleen
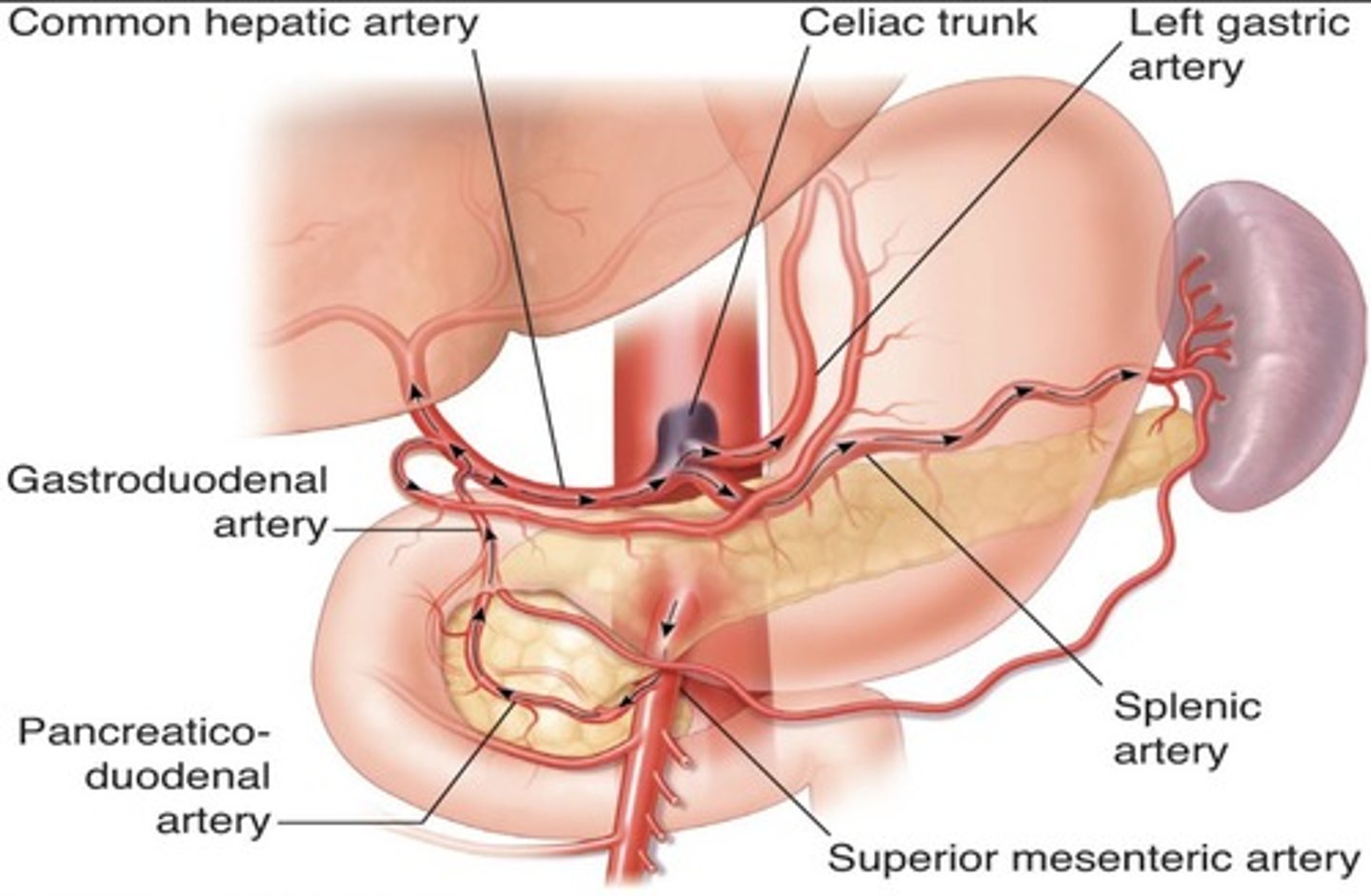
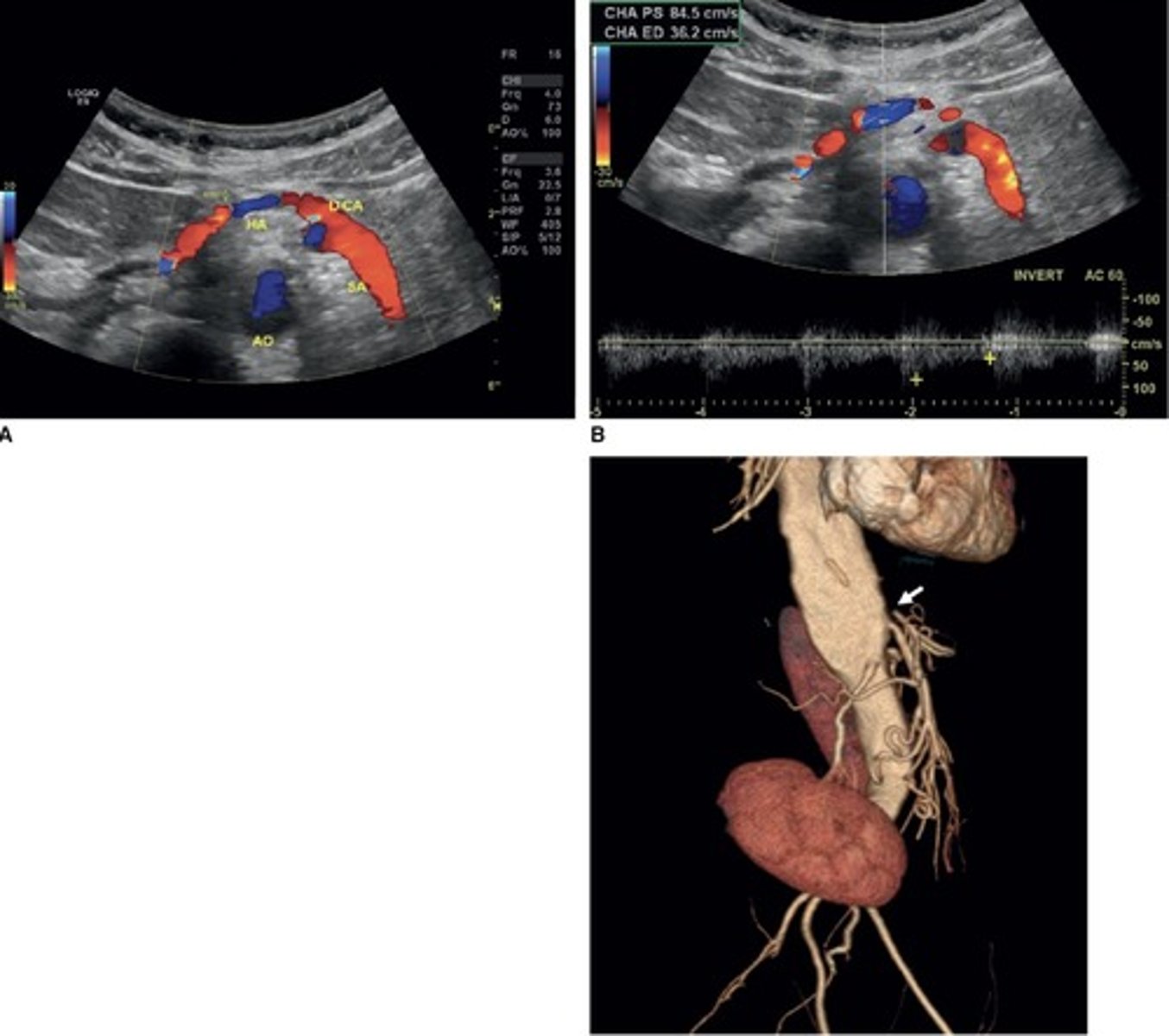
Replaced Right Hepatic Artery
Right hepatic artery branches off something else besides celiac artery - usually SMA
Hepatic Artery Retrograde Flow
Due to celiac artery occlusion
Blood flows towards splenic artery - RABT color pattern
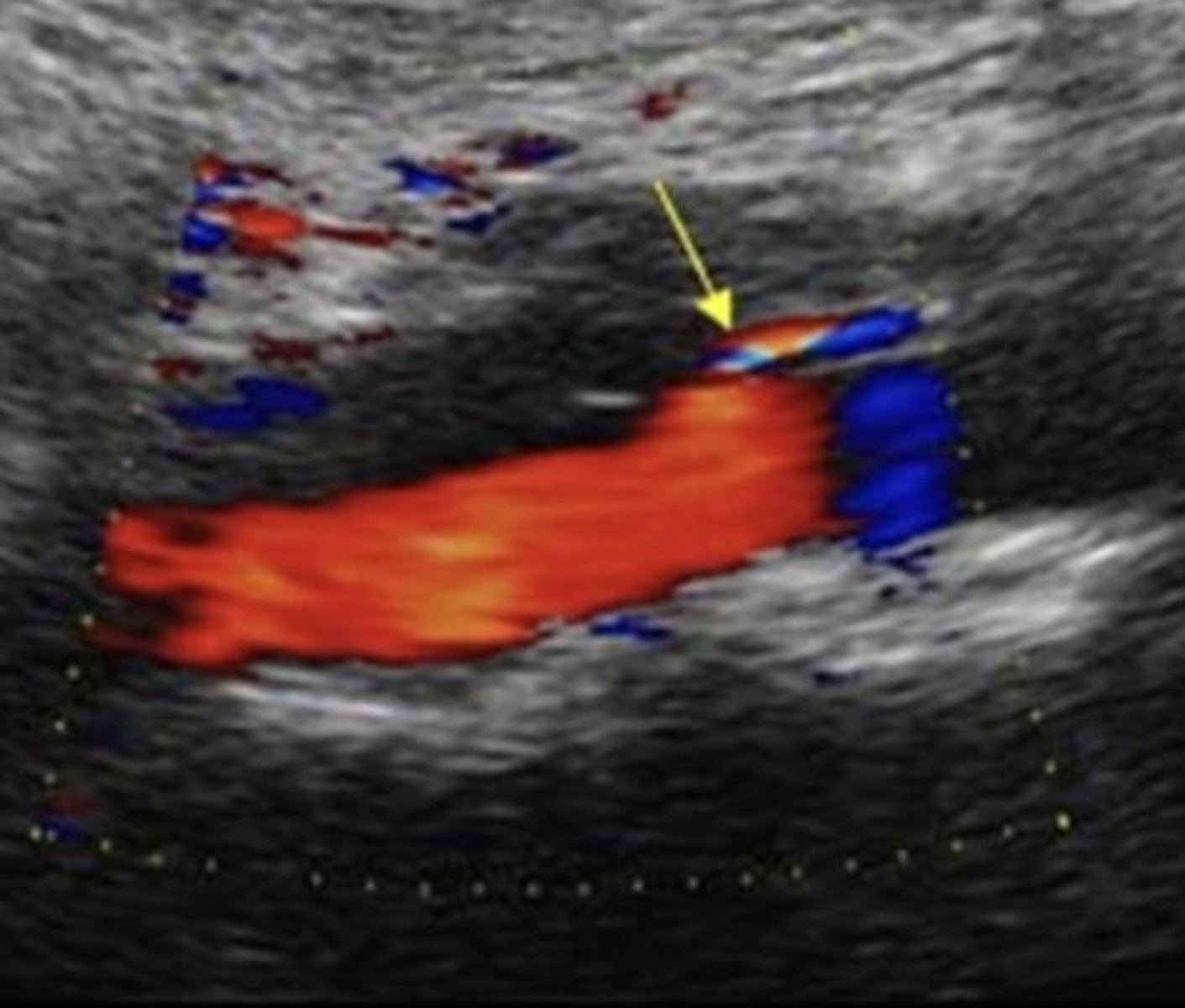
SMA
Pre-Prandial SMA Doppler

Post-Prandial SMA Doppler
SMA PSV
113 cm/sec
Common Trunk Variant
Celiac and SMA come off common trunk
IMA
IMA PSV
141 cm/sec
Prominent IMA
Due to SMA occlusion
Median Arcuate Ligament Syndrome (MALS)
Compression of celiac axis during exhalation by median arcuate ligament
Pain relieved by inhalation
Evaluate in supine & upright positions and with inspiration & expiration
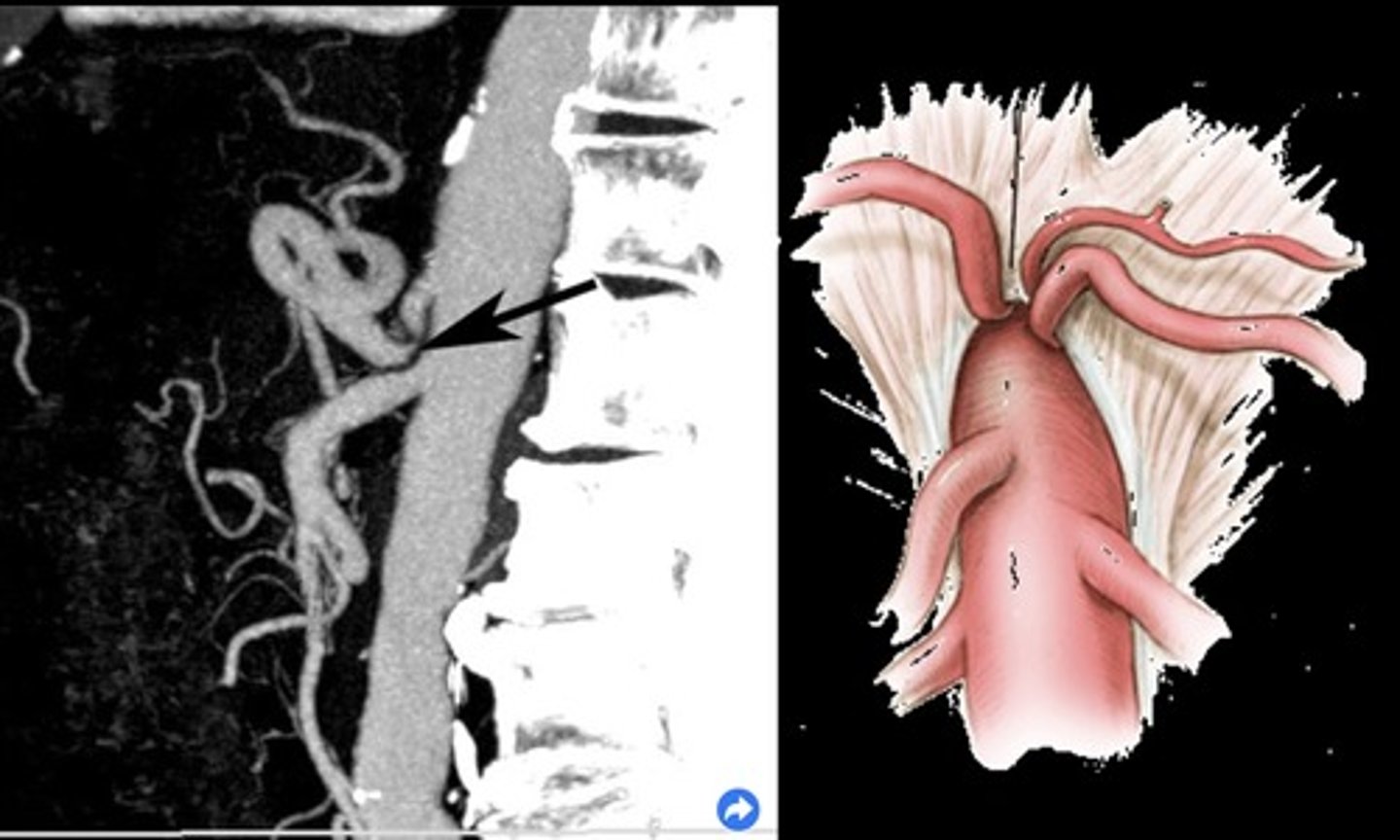
Celiac Artery PSV with MALS
> 250 cm/sec during expiration that normalizes with inspiration
Acute Mesenteric Ischemia
Thrombosis of one or more mesenteric vessels
Life threatening - requires immediate intervention
Severe cramping/pain - disproportional pain
Chronic Mesenteric Ischemia
Low resistant pre-prandial doppler signals
70% occlusion of 2/3 splanchnic arteries required for diagnosis (celiac, SMA, IMA)
Epigastric pain after eating - fear of food, weight loss, decreased nutrition
Small Vessel Disease
Fasting low resistant waveform
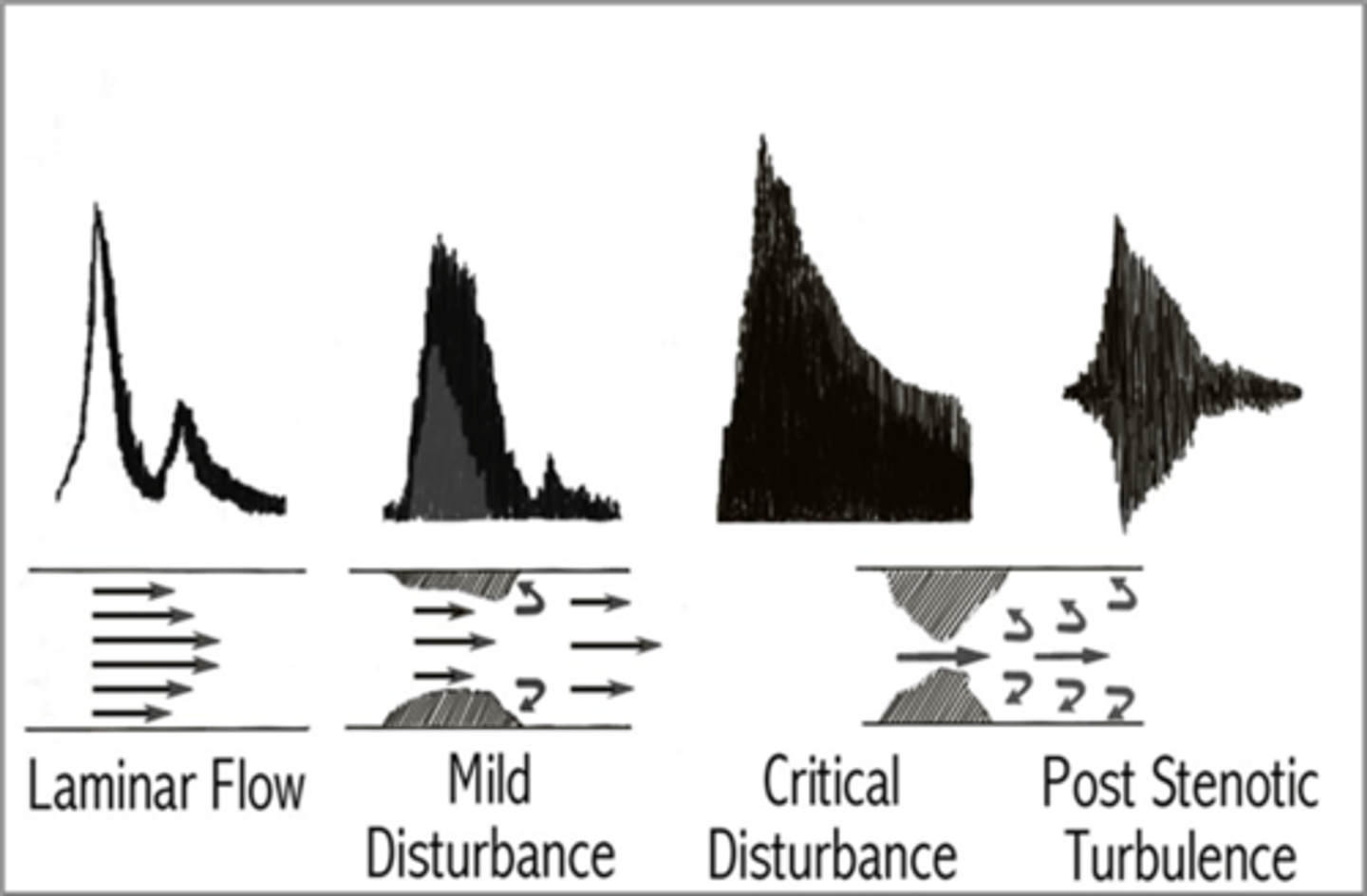
Stenosis
Stenotic profile
Treated with stents