ISP Lab Exams
0.0(0)
Studied by 1 personCard Sorting
1/140
There's no tags or description
Looks like no tags are added yet.
Last updated 6:05 AM on 5/28/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
141 Terms
1
New cards
The four respiratory tests of ISP lab 2
Measuring rest breath
Breath hold (time)
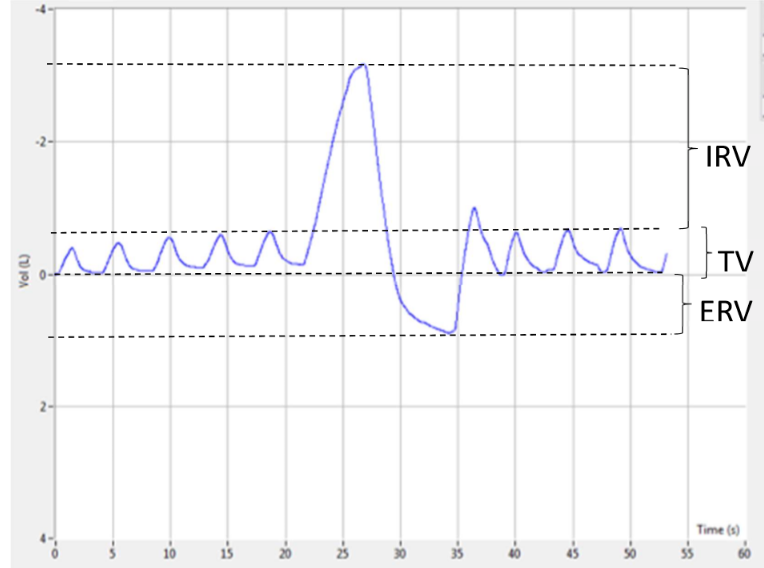
Lung volumes and capacity (**slow spirometry**)
Measuring FVC and expiratory flow volume curve (forced spirometry)
Breath hold (time)
Lung volumes and capacity (**slow spirometry**)
Measuring FVC and expiratory flow volume curve (forced spirometry)
2
New cards
VM, RF and VT meanings
Minute ventilation
Respiratory frequency
Tidal volume
Respiratory frequency
Tidal volume
3
New cards
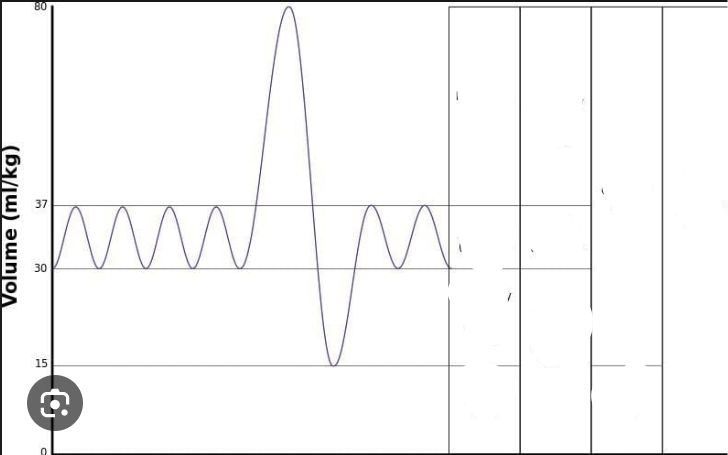
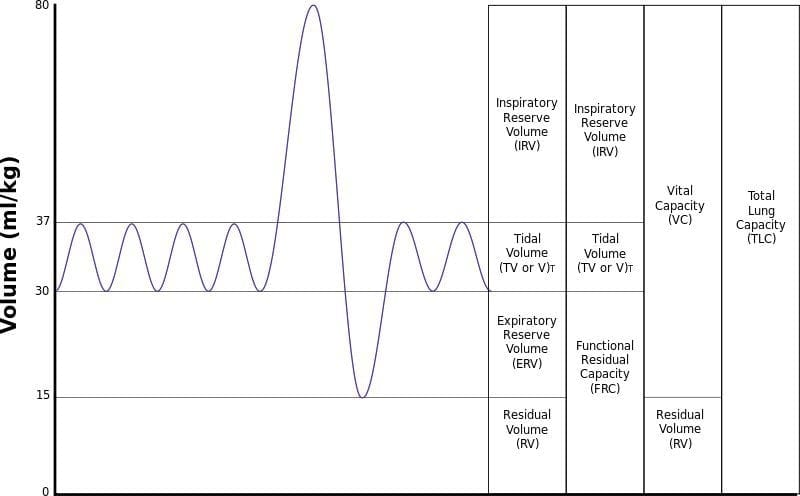
Label the following
4
New cards
What activities should be avoided prior to lung function testing? (lab 2)
Smoking within an 1hr
Alcohol within 4 hrs
Vigorous exercise within 30 mins
Clothing that is restrictive
Large meal within 2hrs of testing
Alcohol within 4 hrs
Vigorous exercise within 30 mins
Clothing that is restrictive
Large meal within 2hrs of testing
5
New cards
Concentratiosn of N, O and CO2 at atmosphere?
78% N
21% Oxygen
21% Oxygen
6
New cards
Henry’s law
Gas diffuses proportional to partial pressure of the gas
7
New cards
Central vs peripheral chemoreceptors
Central (of the brain) - sensitive to carbon dioxide (as measured via pH)
Peripheral - oxygen, carbon dioxide and pH of blood
Peripheral - oxygen, carbon dioxide and pH of blood
8
New cards
What is pulmonary ventilation?
The amount of air exhaled per minute
9
New cards
What does forced spirometry show?
Maximum air exhaled in a single breath and resistance to air flow
10
New cards
What information is required for spirometry (personal info)
*Ethnic group*
*Gender*
*Date of Birth*
*Height*
*Weight (not important tho?)*
\
*Gender*
*Date of Birth*
*Height*
*Weight (not important tho?)*
\
11
New cards
How to measure breath hold?
After a minute of quiet breath (or two minutes), hold breath at end of next quiet inspiration
12
New cards
When did the breath hold time become the highest?
After hyperventilating
Shortest after rebreathing from paper bag (where Co2 is higher to start with)
Hypercapnic drive was low to start with
Shortest after rebreathing from paper bag (where Co2 is higher to start with)
Hypercapnic drive was low to start with
13
New cards
When did you stop breathing when performing an FVC?
Noseclip was on, end of quiet expiration- exhale maximally until 6S timer turns green.
Should have repeated three times w one minute rest.
Should have repeated three times w one minute rest.
14
New cards
MV, TV and FR?
MV = TV and FR
15
New cards
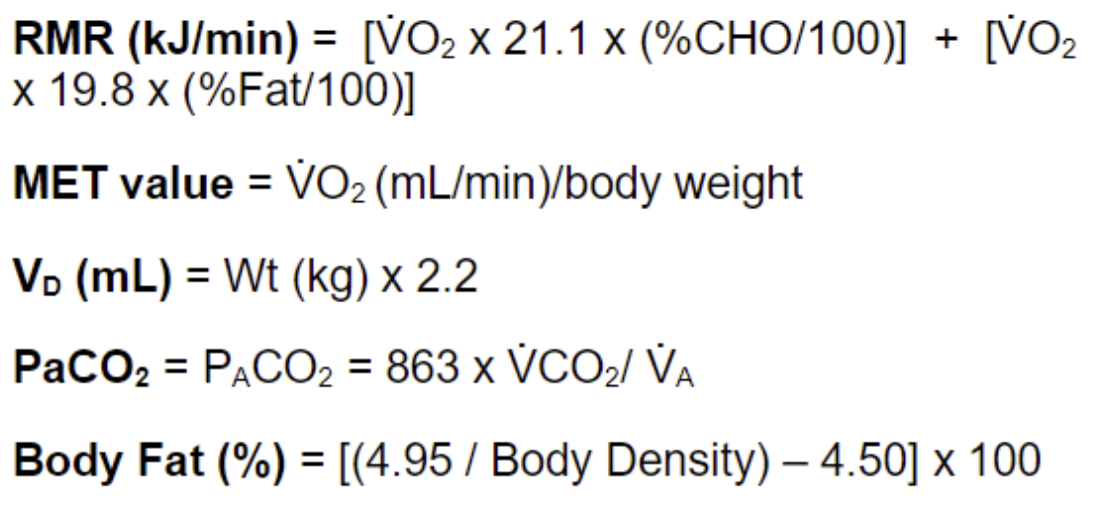
Estimate dead space volume for a 50kg woman.
50\*2.2 + 30ML
140mL (Or 110mL)
140mL (Or 110mL)
16
New cards
Alveolar vs minute ventilation
Alveolar excludes dead space (FRC)
17
New cards
PaCO2
partial pressure of carbon dioxide in arterial blood
VCO2 \* 0.863/VA (L/min)
= rate of CO2 production \* 0.863 / alveolar ventilation
VCO2 \* 0.863/VA (L/min)
= rate of CO2 production \* 0.863 / alveolar ventilation
18
New cards
How to assume VCO2?
2\.8\*weight = mL/min
19
New cards
Normal range for PaCo2
40-45 mmHg
* high = hypoventilation
* low = hyperventilation
* high = hypoventilation
* low = hyperventilation
20
New cards
im confused… ask joanne!
Calculate VC, TLC (53kg person), FRC and IC
Calculate VC, TLC (53kg person), FRC and IC
3\.6, 4.8 (estimate RV to be 1.2L), 1.7 and 3.1
21
New cards
What are medikro values based on
Height, age, sex, ethnicity
(**not weight, weight is not part of the parameters?**)
(**not weight, weight is not part of the parameters?**)
22
New cards
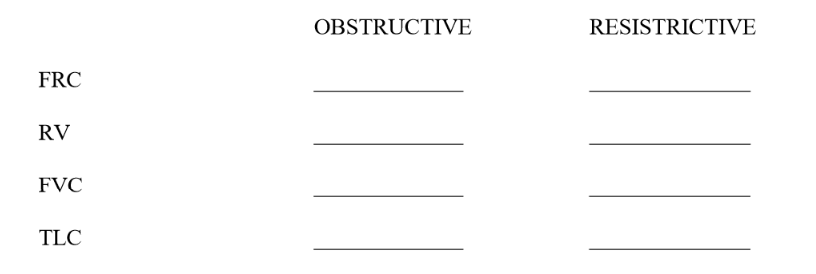
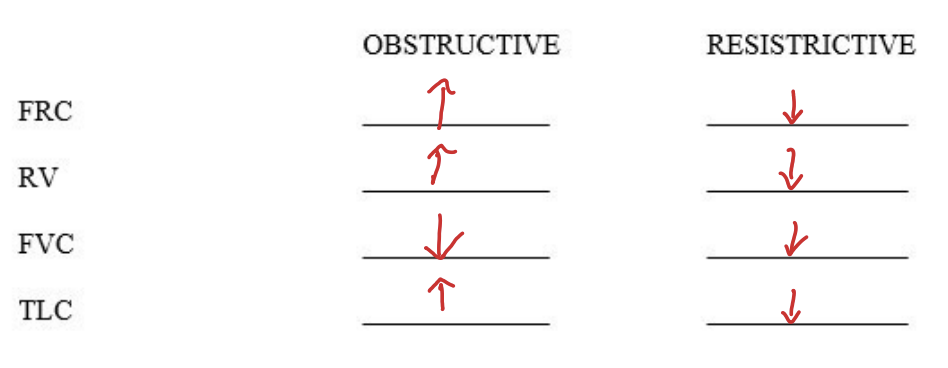
fill this out
23
New cards
What are acceptable measurements/trials for a expiratory flow volume curve?
Produce two attempts that are within 0.15L of each other
24
New cards
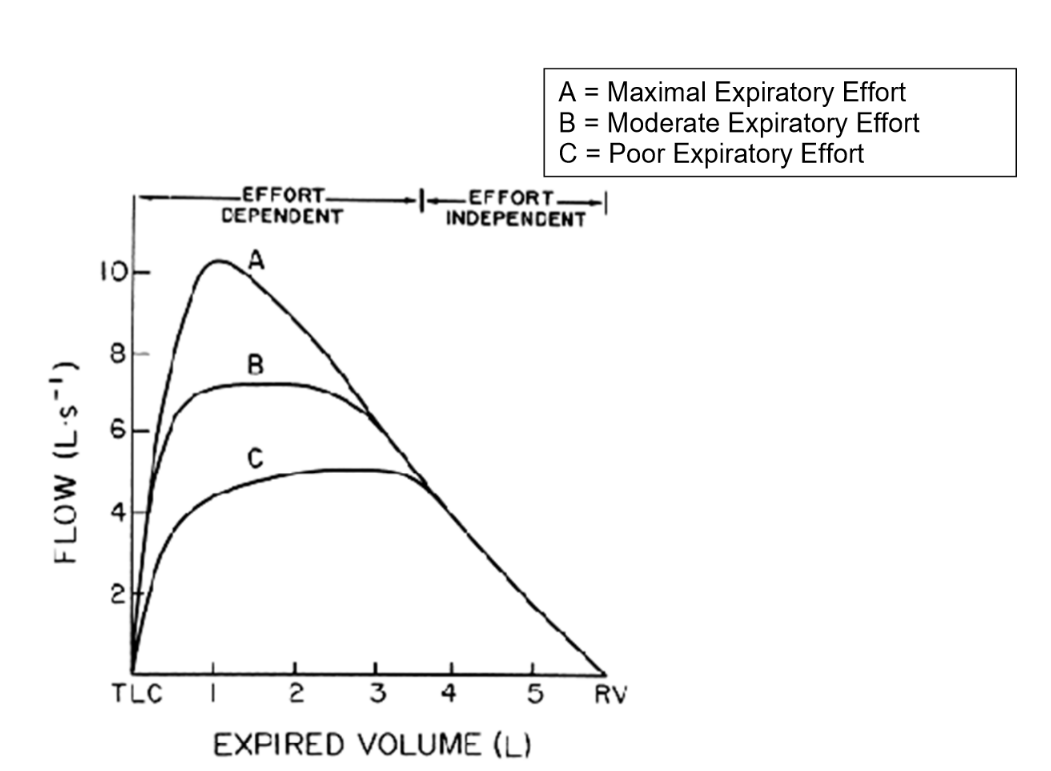
Why is FEF50 useful
Can identify flow in effort dependent stage (when half volume is expired and its hard to get air out)
\
Shows obstructive disease
\
Shows obstructive disease
25
New cards
Estimate PaCo2 for a 65 kg man, assuming
VCo2 = 2.8\* weight and
PaCo2 = VCO2 x 0.863/VA
RF = 12
TV = 0.6 V
VD = 0.1
VCo2 = 2.8\* weight and
PaCo2 = VCO2 x 0.863/VA
RF = 12
TV = 0.6 V
VD = 0.1
26\.18 mm Hg = hypocapnic
26
New cards
The first Korotkoff sound correlates with __ BP
systolic
27
New cards
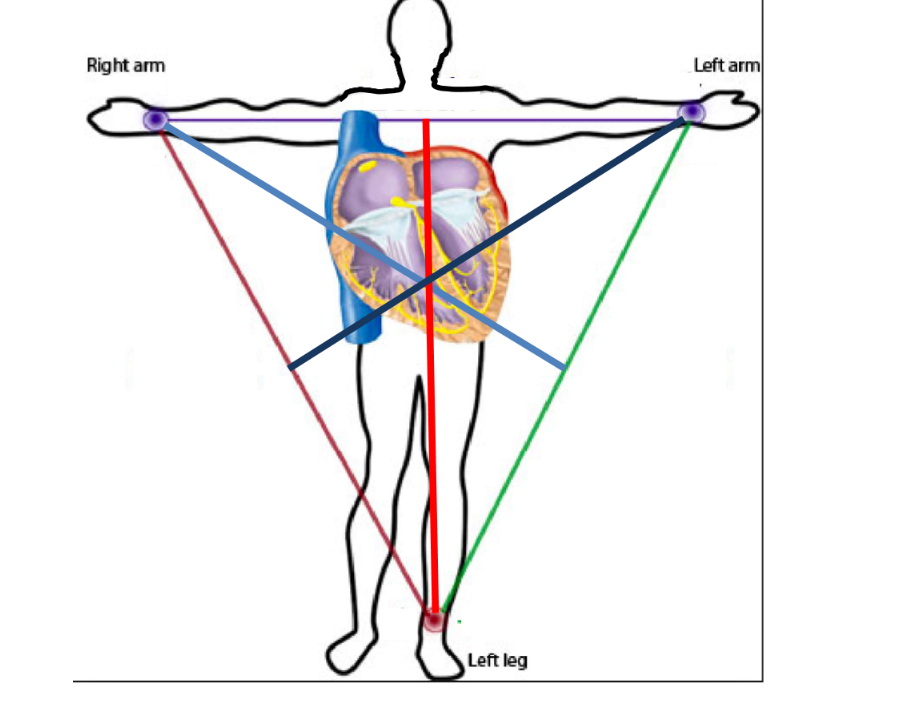
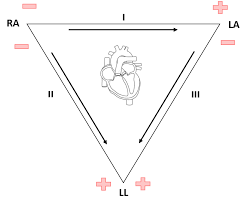
A 12 lead ECG is obtained from the placement of ___ electrodes.
__ leads recording between 2 single electrodes
___ lead recordings between a single electrode + avg of 2 others
___ lead recordings from a single electrode on the chest
__ leads recording between 2 single electrodes
___ lead recordings between a single electrode + avg of 2 others
___ lead recordings from a single electrode on the chest
10, 3 (bipolar limb leads) ,3 (augmented limb leads), 6 (unipolar precordial/chest leads)
28
New cards
How many ECG rhythms have the word sinus in them?
5
29
New cards
Normal RR, HR, PR interval
RR- 0.6s-1.0s
HR- 60-100bpm
PR- 0.12-0.2s
HR- 60-100bpm
PR- 0.12-0.2s
30
New cards
Normal QRS duration and QT interval
QRS < 0.12
QT = 0.36-0.44s (for resting HR 60-70bpm)
\
QT = 0.36-0.44s (for resting HR 60-70bpm)
\

31
New cards
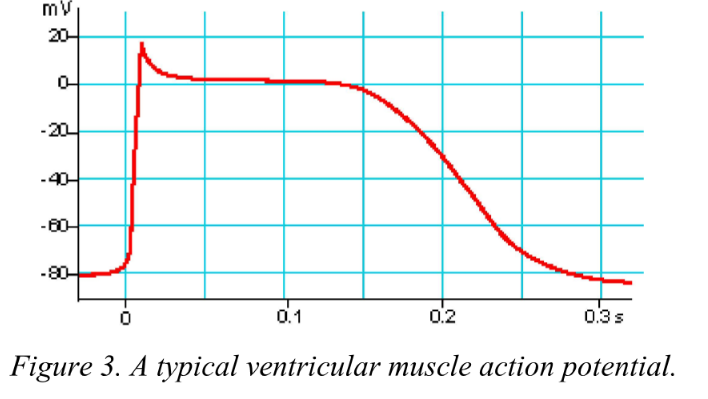
What are the three phases of cardiac action potential?
Rapid depolarisation, plateau depolarisation and repolarisation
32
New cards
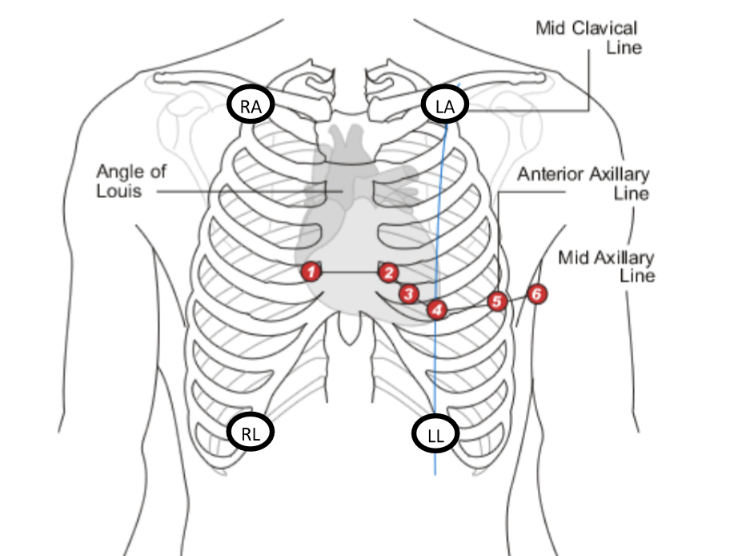
Where should RA and LA electrodes be placed?
Below mid clavicle
33
New cards
Where should V1-V6 be placed?
V1- palpate down to sternal angle and go to right sternal border (IC2) and down two spaces (IC space 4)
V2 - left sternal border (IC space 4)
V3- half way between V2 and V3
V4- IC space 5 in left mid clavicle line
V5- anterior axillary line
V6- mid axillary line
V2 - left sternal border (IC space 4)
V3- half way between V2 and V3
V4- IC space 5 in left mid clavicle line
V5- anterior axillary line
V6- mid axillary line
34
New cards
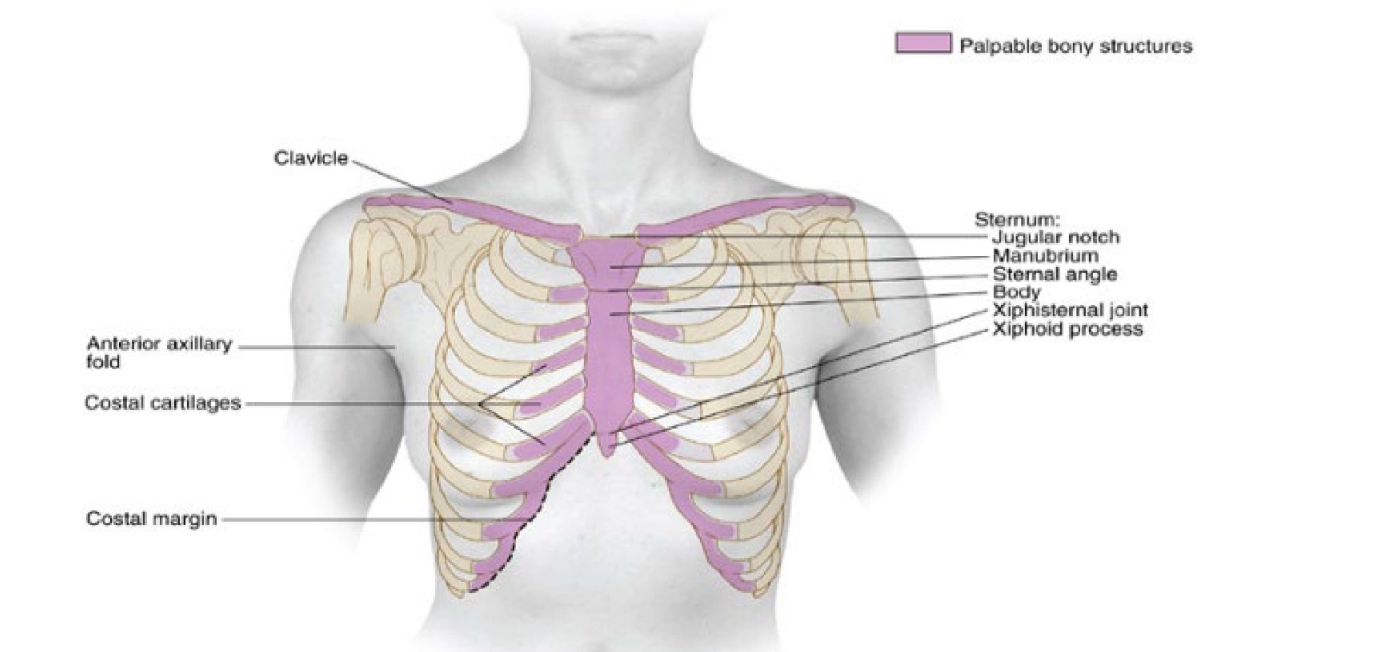
What forms the sternal angle?
Angle of louis- manubrium of sternum and body of sternum (lines up w IC 2)
35
New cards
Where should RL and LL be placed? (ECG)
mid clavicular lines at costal margin
36
New cards
What to do if ECF trace is noisy?
Subject relaxes, check adhesion to skin and secure connection to cable
37
New cards
What are the 4 ECG recordings taken?
1. Subject completely relaxed
2. Subject breathing slowing (Sinus arrhythmias)
3\.+4 Subject lying of left and right lateral sides (for MEA analysis)
38
New cards
What are hallmarks of a normal sinus rhythm?
1. Regular RR intervals
2. Identical P waves (lead II)
3. Narrow and identical QRS (lead II)
1. Every p wave is followed by QRS (lead II)
39
New cards
What is the QT interval corrected for?
HR and sex?
40
New cards
If PR interval was lengthened consustently
, this would indicate
, this would indicate
heart block type I
41
New cards
If QRS was lengthened, what could this be?
PVC, VTAC, 3rd degree heart block
42
New cards
What is Long QT syndrome?
heart signaling disorder that can cause fast, chaotic heartbeats (arrhythmias). A heart signaling disorder is also called a heart conduction disorder
43
New cards
Which leads show inferior, LL and anterior?
Inferior - II, III, a VF
LL: I, v5, v6, aVL
Anterior - V1 → V4
LL: I, v5, v6, aVL
Anterior - V1 → V4
44
New cards
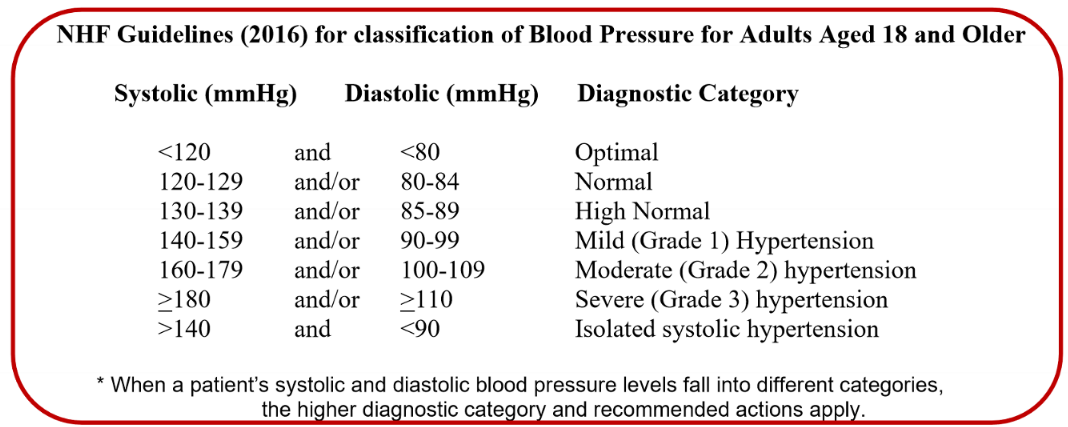
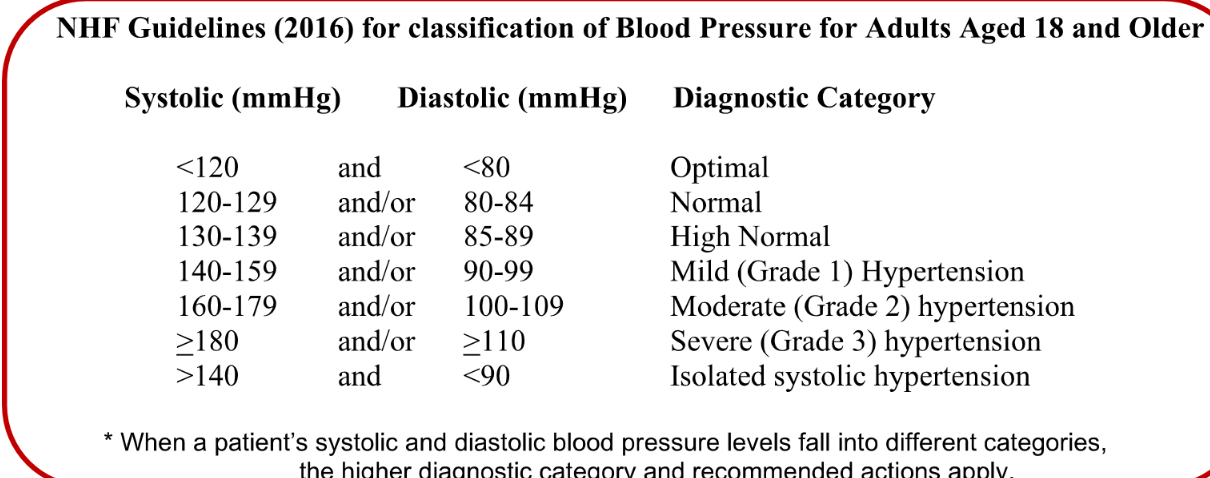
What are the national guidelines for BP?
45
New cards
What does RPP measure?
Rate pressure product- looks at amount of stress placed on heart
* AT rest: RPP shows if heart is under excessive strain
* During exercise: RPP examines response to physical exertion (MI or abnormal rhythm may be detected)
* AT rest: RPP shows if heart is under excessive strain
* During exercise: RPP examines response to physical exertion (MI or abnormal rhythm may be detected)
46
New cards
Label the diagram ^^
47
New cards
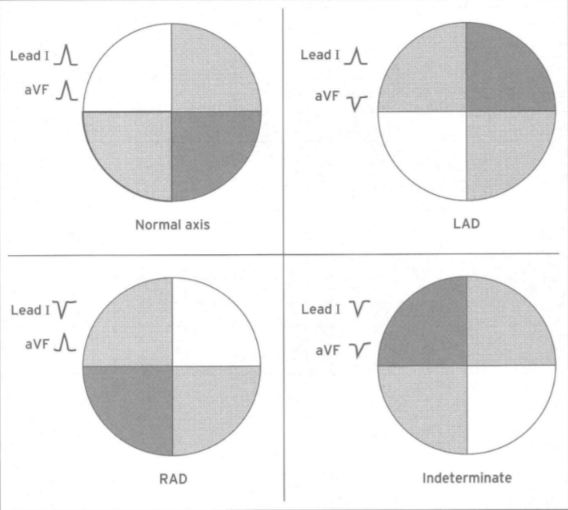
What is the normal axis range? (MEA)
\-30 to 120 degrees
48
New cards
draw the four different MEAs
49
New cards
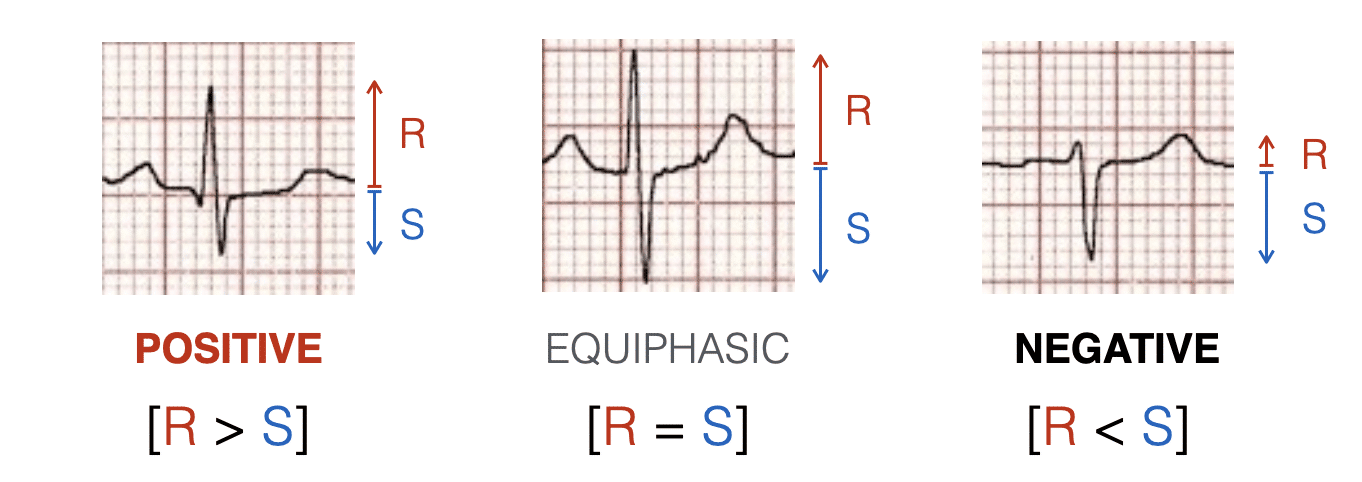
What does looking at the leads with the largest positive R waves show?
MEA is somewhere in between
50
New cards
What is a biphasic limb lead? (lab 1)
If QRS is biphasic = MEA is approx at right angles
51
New cards
Purpose of taking right and left sides (lying laterally) for ECGs?
Technique called a "right lateral decubitus ECG" and a "left lateral decubitus ECG”
* Right side: look at right ventricular hypertrophy, right heart block problems
* Left side: same deal
Helps identify rhythms that are not identifiable when lying supine
* Right side: look at right ventricular hypertrophy, right heart block problems
* Left side: same deal
Helps identify rhythms that are not identifiable when lying supine
52
New cards
What causes LVH?
Pressure overload - aortic stenosis or hypertension or in extreme athletes
\
\
53
New cards
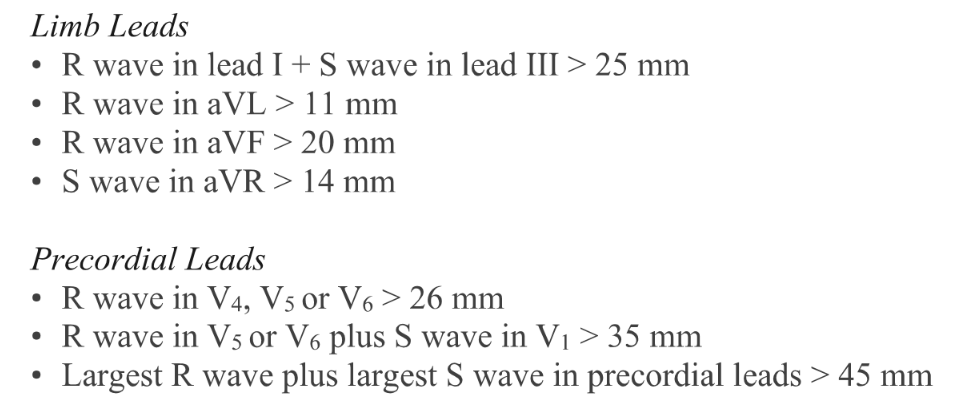
How to characterise LVH?
Left side leads will show increased R wave amplitude (I, avL, V4-V6)
Right side leads will show increased S wave depth (III, aVR, V1-3)
**Further: classifications/ECG voltage criteria**
**(where 10mm = 1 mV)**
Right side leads will show increased S wave depth (III, aVR, V1-3)
**Further: classifications/ECG voltage criteria**
**(where 10mm = 1 mV)**
54
New cards
How to prepare for BP measurement?
Seated for 5 minutes w ith elbow flexed
Chair has back support, feet on ground
Subject should not have ingested food or drugs within last 30 minutes
No exercise the hour prior
\
Chair has back support, feet on ground
Subject should not have ingested food or drugs within last 30 minutes
No exercise the hour prior
\
55
New cards
What are the 5 different korotkoff sounds? which are clinically significant?
1- beginning of repetitive tapping (SBP)
2- soft/swishing (no important)
3- sharper and maybe louder tapping than 1st (not important)
4 - sound becomes muffled
5- sound disappears (DBP)
2- soft/swishing (no important)
3- sharper and maybe louder tapping than 1st (not important)
4 - sound becomes muffled
5- sound disappears (DBP)
56
New cards
How to take BP
Wrap cuff around arm with arm supported at level of heart (cuff aligned w brachial artery)
Inflate to 160 mm Hg (\~20 mmHG above systolic)
Release at 2-3 mm Hg/sec
Inflate to 160 mm Hg (\~20 mmHG above systolic)
Release at 2-3 mm Hg/sec
57
New cards
How many BP readings?
2 measurements (Min 1 min apart)
Average
Take 3rd if systolic differents by more than 10 mm Hg
Average
Take 3rd if systolic differents by more than 10 mm Hg
58
New cards
Potential errors in BP reading
Inaccurate sphygmomanometer
Improper cuff size
Auditory acuity of tech
Rate of inflation/deflation
Experience/reaction time
Improper placement or max inflation
background noise
subject holding onto something
physiological abnormalities (damaged brachial artery)
Improper cuff size
Auditory acuity of tech
Rate of inflation/deflation
Experience/reaction time
Improper placement or max inflation
background noise
subject holding onto something
physiological abnormalities (damaged brachial artery)
59
New cards
What does NIBP stand for?
Non invasive blood pressure devicie
60
New cards
MAP should be estimated using which arm?
Non dominant-
diastolic + (systolic-diastolic) / 3
diastolic + (systolic-diastolic) / 3
61
New cards
FOrmula for RPP
RPP = HR \* SBP
62
New cards
What are the NHF classifications for BP
yayyyy don’t need these
yayyyy don’t need these
63
New cards
correct pressure for initial cuff inflation
160mmHg (clinically, 200 mmHg)
\
\
64
New cards
Correct rate of cuff deflation
2-3 mmHg per minute
65
New cards
Why measure BP in both arms?
To identify peripheral artery disease
damage of aorta
atherosclerosis
Stenosis of subclavian artery
damage of aorta
atherosclerosis
Stenosis of subclavian artery
66
New cards
Why measure BP in different positions?
Orthostatic hypertension: significant drop in blood pressure upon standing (accompanied with dizziness/faintness)
Drop in blood pressure could also suggest hypovolemia (dehydration)
Drop in blood pressure could also suggest hypovolemia (dehydration)
67
New cards
What is the auscultatory gap? What happens if it is not recognised?
Period of diminished or absent Korotkoff sounds during the manual measurement of blood pressure. It is associated with reduced peripheral blood flow caused by changes in the pulse wave.
Silent interval that may occur between the initial appearance of Korotkoff sounds (phase I) and their re-appearance after a temporary absence (phase II).
**If the auscultatory gap is not recognized, it can result in underestimating the true systolic blood pressure and overestimating the diastolic blood pressure.**
Silent interval that may occur between the initial appearance of Korotkoff sounds (phase I) and their re-appearance after a temporary absence (phase II).
**If the auscultatory gap is not recognized, it can result in underestimating the true systolic blood pressure and overestimating the diastolic blood pressure.**
68
New cards
One small square = _ s (ECG)
0\.04 secs
69
New cards
What would a beta blocker do to heart rate?
Decrease BP and HR to reduce CO (response to hypertension)
70
New cards
Physiological basis of sinus arrhythmia?
Inspiration = increase HR
Expiration = decrease HR
Vagus nerve can influence
Expiration = decrease HR
Vagus nerve can influence
71
New cards
ECG criteria for clinically significant ST depression/elevation
greater than or equal to 1mm
72
New cards
ischemia vs infarction on an ECG
ischemia = ST depression (subendocardial injury)
infarction = ST elevation (transmural/epicardial injury)
infarction = ST elevation (transmural/epicardial injury)
73
New cards
Sinus arrest vs sinus exit block
Sinus exit block - skip a beat but comes back at same HR
Sinus arrest- stop and new HR start
Sinus arrest- stop and new HR start
74
New cards
Main electrophysiological different between atrial tachycardia and atrial fibrililation
Tach = regular
fibrill = irregular
fibrill = irregular
75
New cards
Difference between second degree type I and type II AV block
type I - PR interval gets progressively longer
type II - more P waves than QRS
type II - more P waves than QRS
76
New cards
Is VFib or VTAC worse?
VGib = rhythm and rate are both affected
77
New cards
Unifocal vs multifocal in PAC/PVC
When describing premature atrial contractions (PACs) or premature ventricular contractions (PVCs), "unifocal" and "multifocal" refer to the pattern or origin of these abnormal heartbeats.
Unifocal=premature beats that arise from a single ectopic focus or site within the atria (in the case of PACs) or ventricles (in the case of PVCs). This means that all the abnormal beats have the **same morphology or appearance**
multifocal= multiple ectopic foci or sites within the atria or ventricles. This means that the abnormal beats have varying morphologies or appearances
Unifocal=premature beats that arise from a single ectopic focus or site within the atria (in the case of PACs) or ventricles (in the case of PVCs). This means that all the abnormal beats have the **same morphology or appearance**
multifocal= multiple ectopic foci or sites within the atria or ventricles. This means that the abnormal beats have varying morphologies or appearances
78
New cards
Premature ventricular contraction vs complex
“premature ventricular contraction" emphasizes the timing aspect,
"premature ventricular complex" highlights the complex nature of the abnormal beat.
"premature ventricular complex" highlights the complex nature of the abnormal beat.
79
New cards
Calculate BMI for 183cm male who wear 82kg
24\.49 (average health risk)
80
New cards
What is used to estimate BSA?
Weight and height
81
New cards
What does STPD stand for?
Standard temperature and pressure (dry)
82
New cards
What is definitive method for estimating body density?
Skin fold measurements
83
New cards
What does BIA stand for?
Bioelectrical impedance analysis (used for body fat estimate)
84
New cards
Four sites to measure skinfold thickness
Triceps, biceps, subscapular, iliac crest
85
New cards
What is BMR?
Basal metabolic rate = amount of energy to function on complete rest (just wake up, not eat for 12 hours, lie in dark room w no external stimuli)
86
New cards
What is RMR?
Surrogate for BMR (lying down for two hours, eyes closed and not eaten for previous 2 hours)
87
New cards
What does measuring oxygen consumption help with for indirect calorimetry?
Help estimate energy expenditure (aerobic metabolism)
88
New cards

Write this expression in words/fully expanded
Rate of oxygen consumed= rate at which oxygen is inspired - rate at which oxygen is expired
\
Oxygen inspired= estimate rate w VE \* fraction oxygen in inspired air (0.2093)
Oxygen expired = VE (gas meter) \* oxygen in expired air (o2 analyser)
\
Oxygen inspired= estimate rate w VE \* fraction oxygen in inspired air (0.2093)
Oxygen expired = VE (gas meter) \* oxygen in expired air (o2 analyser)
89
New cards
What is the value for FIO2?
0\.2093 (fraction of oxygen in inspired air)
90
New cards
What does RQ help with ?
Respiratory quotient: helps give balance between CHO and fat burning (generate different amount of energy for each litre of oxygen consumed)
CHO RQ = 1
Fat RQ = 0.7
(ignore proteins, % is small and RQ is between CHO and fat)
CHO RQ = 1
Fat RQ = 0.7
(ignore proteins, % is small and RQ is between CHO and fat)
91
New cards
Why can we ignore FICO2 in VCO2?
Its so small (0.0004), can be considered 0
92
New cards
How to measure FeCO2
CO2 analysis of expired air
93
New cards
What state must VCO2 and VO2 be measured?
steady state= metabolic and respiratory gas exchange being in equilibrium
94
New cards
Why is RER considered the RQ?
Respiratory exchange ratio (RER) is RQ estimated by metabolic gas exchange
95
New cards
LAB 3: How long should volunteer being lying down before beginning measurements
(5) 10 minutes, breathing through facemask
96
New cards
Process of lab 3 + using the taps
\
\
Tap should be turned to **the bag so expired air is diverted into it for 5 minutes (closing tap at end of expiration). Record pulse rate (eyes should have been closed)**
97
New cards
How to analyse expired air? (Lab 3)
Room temp and barometric pressure
Gas analyser- turn tap to connect sampling line and inlet tube and start stopwatch. 60 seconds of sampling (record exact time for both O2 and Co2)
**Note sampling rate = 280ml/min**
**close tap to the bag**
Go to volume measuring station, connect, read initial reading and turn tap to connect bag to gas meter
Gas analyser- turn tap to connect sampling line and inlet tube and start stopwatch. 60 seconds of sampling (record exact time for both O2 and Co2)
**Note sampling rate = 280ml/min**
**close tap to the bag**
Go to volume measuring station, connect, read initial reading and turn tap to connect bag to gas meter
98
New cards

What does the expiratory volume calculation (converting STPD to ATPS) assume?
RT = 22 degrees and Pbar = 760 mmHg
99
New cards

Calculate RMR if RER = 0.84 and VO2 is 0.2542
%CHO = (RQ - 0.7) / 0.003
46\.67%
(Fat % 53.33%)
RMR = 5.19 kJ/min
To convert to kJ/hour/m2 divide by BSA and \* 60
46\.67%
(Fat % 53.33%)
RMR = 5.19 kJ/min
To convert to kJ/hour/m2 divide by BSA and \* 60
100
New cards
Average male and female RMRs
Female =150
Male = 160 kJ/hour/m2
Male = 160 kJ/hour/m2