Acute Care
1/156
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
157 Terms
Patient Safety - Basic Guidelines
Reduce the risk of health-care associated infections
Familiarity with alarm systems (code call buttons, staff assist, etc.)
Confirmation of the correct patient to treat
Proper body mechanics during patient treatment
Use equipment in good working condition
Keep the patient’s room clean and clutter free
Provide recommendations for the nursing staff
Fall - Definition
Defined as an event that results in a person coming to rest inadvertently on the ground/floor/other lower level
Patients may be conscious or unconscious
One of the more common adverse effects and accounts for increased
personnel needs, length of stay, cost, morbidity and mortality, especially of older adults
Fall risk assessment (advanced age, medications, visual acuity, muscle strength, functional abilities)
Medical conditions associated with falls
neurologic, orthopedic, cognitive, postural/orthostatic hypotension
Morbidity vs Mortality
Mortality = state of being dead / frequency of being dead
Morbidity = disease prevalence
Latex Allergy
Either allergic to the natural rubber in latex, or the chemicals used to produce latex
Includes gloves, stethoscopes, cuffs, airway and IV tubing, electrodes, etc.
Restraint Definition
Any manual method, physical, or mechanical device that reduces patient movements especially the extremities
Examples: wrist/ankle restraints, mitt restraints, vest restraints, enclosure bed
Restraints - Indication
For patients who are at risk for self-harm or harm to others
Restraints - downsides
increased agitation
nerve or muscle damage
alterations in skin integrity
Intensive Care Setting
It is a place of intensive medical-surgical care for patients who require continuous monitoring, usually in conjunction with other therapies or medical interventions such as vasoactive medications, sedation, circulatory assist devices, and mechanical ventilation
May be PICU, CICU, SICU, MICU depending on patient distribution
ICU - Intensive Care Setting
Patients are faced with environmental stressors such as physical restrictions, sleep deprivation, unfamiliar medical equipment, crowding, excessive lighting, odors, noises, and touch associated with procedures.
ICU - Psychological Stressors
diminished dignity and self-esteem, powerlessness, loss of autonomy, vulnerability, boredom, pain, fear, anxiety, isolation, uncertainty about the future, and spiritual distress
ICU Delirium or ICU Syndrome
increased with emergency surgery, polytrauma, organ failure, metabolic acidosis, coma, dementia, or advanced age
B-Type Natriuretic Peptide - Rationale
Assesses the biomarkers of heart failure, including natriuretic peptides
B-Type Natriuretic Peptide - Interpretation
Normal Levels - 100pg/mL,
Values above 500 are usually considered to be positive of heart failure, correlations between BMP and peak oxygen uptake
Blood urea nitrogen, plasma creatinine levels, urine output - Rationale
Assesses kidney function
N BUN values
6-30 mg/dL
N Creatinine Values
0.6-2.0 mg/dL
Oliguria values
<400 mL of urine in 24 hours
Anuria Values
<100mL of urine in 24 hours
Hemoglobin and hematocrit levels - Rationale
Assesses the oxygen carrying capacity within the system
N hemoglobin values
12-14 gm/mL of blood (males)
14-16 gm/100mL (women)
N Hematocrit values
45% men
45% women
Creatine Kinase - Myocardial band CK-MB index Rationale
Creatine Kinase MB Subunit is an isoenzyme, is released into the blood and elevates with acute MI
Creatine Kinase - Myocardial band CK-MB index Values
Normal level 0-3%
Minor cardiac dysfunction 5%
Major cardiac dysfunction 10%
Peak levels 14-36 hours post MI
Troponin I - Rationale
Most frequently used marker to assess the presence of an acute MI Troponin I
isotype found in the myocardium and is therefore 100% cardiac specific
Troponin I - Values
N levels 0-0.2 mcg/mL
Minor cardiac dysfunction 5 mcg/mL
Major cardiac dysfuntion 10 mcg/mL
Peak level 24-36 hours post MI
C-Reactive protein - Rationale
Measures the amount of protein in the blood that signals acute inflammation
For a more sensitive test = high- sensitivity C-reactive protein assay is available to check for risk of Hemodialysis
C-Reactive protein - Values
hs-CRP <1.0 mg/L = low risk
hi-CRP 1-3 mg/L = average risk
hi-CRP 3 mg/L = high risk
Electrolyte Assessment - Rationale
Appraise the levels of potassium, calcium, and magnesium to allow for normal electrical condition throughthe heart
Electrolyte Assessment - Interpretation
Hypokalemia - <3.5 mEq/L produces arrythmias with flattened T waves and depressed ST segments, as well as B LE muscle cramping
Hypocalcemia and hypomagnesemia have the potential to increase ventricular ectopy within the heart
Effects of Hypokalemia
produces arrythmias with flattened T waves and depressed ST segments
B LE muscle cramping
Effects of Hypocalcemia and hypomagnesemia
potential to increase ventricular ectopy within the heart
Systemic Effects of Prolonged Bed Rest - Cardiac
Increased heart rate at rest and with submaximal exercise
Decreased stroke volume, VO2 Max, Left ventricular volume, and cardiac output
Myocardial thinning
Orthostatic hypotension
Systemic Effects of Prolonged Bed Rest - Hematologic
Decreased total blood volume, red blood cell mass, and plasma volume
Increased hematocrit
Venous stasis, hypercoagulability, blood vessel damage
Systemic Effects of Prolonged Bed Rest - Respiratory
Decreased lung volumes and capacities, (FRC, FVC, FEV1)
Decreased mucocilliary clearance
Increased risk of pneumonia, atelectasis, and pulmonary embolism
Decreased arterial oxygen saturation
Systemic Effects of Prolonged Bed Rest - GI
Decreased appetite, fluid intake, bowel motility, and gastric bicarbonate secretion
GERD
Difficulty swallowing
Systemic Effects of Prolonged Bed Rest - Genitourinary
Increased mineral excretion, kidney stones, difficulty voiding, and urinary retention
Increased risk of urinary tract infection
Systemic Effects of Prolonged Bed Rest - Endocrine
Altered temperature and sweating responses, circadian rhythm, regulation of hormones, increased cortisol and glucose intolerance
Decreased overall metabolism
Systemic Effects of Prolonged Bed Rest - MSK
Increased muscle weakness (especially antigravity muscles), atrophy, decreased muscle endurance, risk of contracture,
weakened myotendinous junction
Disuse osteoporosis
Degeneration of cartilage, synovial atrophy, and ankylosis
Systemic Effects of Prolonged Bed Rest - Neurologic
Sensory and social deprivation
Decreased dopamine, noradrenaline, and serotonin levels
Depression, restlessness, insomnia
Decreased balance, coordination, and visual acuity
Increased risk of compression neuropathy
Reduced pain threshold
Systemic Effects of Prolonged Bed Rest - Integumentary
pressure injury formation
Systemic Effects of Prolonged Bed Rest - Immune
Increased risk of reactivation of latent viruses
Reduced immune response and immunity
Systemic Effects of Prolonged Bed Rest - Psychological
Impaired self worth and self esteem
Increased risk of delirium, depression, and post-traumatic stress syndrome
Systemic Effects of Prolonged Bed Rest - Body composition
Increased sodium, potassium, calcium, phosphorus, and nitrogen loss
Increased body fat and decreased lean body mass
Fluid shift from legs to abdomen/thorax/head, diuresis
PT Considerations
Be aware of the psychosocial aspects of prolonged bed rest including sensory deprivation, boredom, depression, and sense of loss of control
Expect fear when patients get out of the bed for the first time especially if they are aware of their impairments
Leave necessities and commonly used items near the patient to minimize the feeling of confinement
Use chair alarm systems or restraints, if ordered, to minimize the risk of falls and other untoward incidents
Infectious Diseases - Antibody
Highly specific protein that is manufactured in response to antigens and defends against subsequent infection
Infectious Diseases - Antigen
Agent that is capable of producing antibodies when introduced into a body of a susceptible person
Infectious Diseases - Communicable
The ability of an infective organism to be transmitted from person to person, either directly or indirectly
Infectious Diseases - Health Care Associated Infection
Localized or systemic condition resulting from an adverse reaction to the presence of an infectious agents(s) or its toxin(s); there must be no evidence that the infection was present or incubating at the time of admission to the acute care setting
Infectious Diseases - Immunocompromised
An immune system that is incapable of a normal response to pathogenic organisms and tissue damage
Infectious Diseases - Immunodeficiency
The prevention or diminution of the immune response, as by drugs or radiation
Infectious Diseases - Immunosuppression
The prevention or diminution of the immune response, as by drugs or radiation
Infectious Diseases - Nosocomial Infection
Infection acquired in the hospital setting; note that this has been replaced by the term HAI
Infectious Diseases - Opportunistic
An infectious process that develops in immunosuppressed individuals (Opportunistic infections normally do not develop in individuals with intact immune systems.)
Infectious Diseases - Subclinical Infection
A disease or condition that does not produce clinical symptoms, or the period before the appearance of disease specific symptoms
Factors Affecting the Immune System
Pregnancy
Preexisting infections
Malignancies (Hodgkin’s disease, acute or chronic leukemia, nonlymphoid malignancy, or myeloma)
Stress (emotional or surgical-anesthesia)
Malnutrition
Age
Chronic diseases
Lymph node dissection
Immunosuppressive treatment (corticosteroids, chemotherapy or radiation therapy)
Indwelling lines and tubes
Corticosteroid Use - Immunosuppressive
Reduction of WBC activity to the site of infection or injury
Decrease T cell proliferation
Weakens adaptive immunity
Impaired antigen presentation
Macrophages and dendritic cells are less effective in recognizing pathogens
Corticosteroid Use - Susceptibility to Infections
Tuberculosis and herpes
Corticosteroid Use - Wound healing
Delayed
inhibition of fibroblast activity
Summary of Precautions to Prevent Infection - Standard
Wash hands before and after each patient contact. Wear a different set of gloves with each patient.
Also, equipment or items in the patient environment likely to have been contaminated with infectious body fluids must be handled in a manner to prevent transmission of infectious agents (e.g., wear gloves for direct contact, contain heavily soiled equipment, properly clean and disinfect or sterilize reusable equipment before use on another patient).
Summary of Precautions to Prevent Infection - Airborne
A respirator (preferable) or mask is required in situations in which contagious pathogens can be transmitted by airborne droplet nuclei, which can stay in the air for more than an hour and can travel >10 feet because of their small size (<5 μm).
The preferred placement for patients who require Airborne Precautions is in an airborne infection isolation room (AIIR).
An AIIR is a single-patient room that is equipped with special air handling and ventilation capacity (e.g., negative pressure)
Summary of Precautions to Prevent Infection - Droplet
A mask or face shield, or both, are required when large-particle (>5 μm in size) droplet transmission (usually 3 ft or less) is likely.
Droplets can be generated from coughing, sneezing, and talking.
Spatial separation of ≥3 feet and drawing the curtain between patient beds is especially important for patients in multi-bed rooms
Healthcare personnel should wear a mask (a respirator is not necessary) for close contact with infectious patients, and the mask is generally donned upon room entry
Summary of Precautions to Prevent Infection - Contact
Gown and gloves are required when pathogens are transmitted bydirect person-to-person contact or person-to-object contact.
It is important to use disposable or dedicated patient-care equipment (e.g., gait belt), don PPE upon room entry, and discard it before exiting the patient room.
Patients on Contact Precautions who must be transported outside of the room should have the infected or colonized areas of the patient’s body covered or contained.
Contact (enteric)
Agents spread by direct or indirect contact
Example agents: MRSA, Gram-negative bacterial infections, Clostridium difficile
Hand hygiene (Chlorhexidine soap), gloves, gown
Mask not required
Droplet
Agents spread through mucous membranes and respiratory secretions
Example agents: Mumps, Neisseria meningitidis
Hand hygiene, mask
Patient must wear surgicalmask when out of room
Airborne
Agents that remain infectious and suspended in the air over long distances
Example agents: Varicella virus, Rubeola virus, Mycobacterium tuberculosis, SARS-COV-2
Hand hygiene, fit-tested N95
Patient must wear surgical mask when out of the room
Antibiotic Reisstant Infections are due to?
Due to inappropriate antibiotic use in healthcare institutions and hospitals
Antiobiotic Resistant Infections - Multidrug-resistant
At least one agent in three or more antimicrobial categories
Antiobiotic Resistant Infections - Extensively Drug Resistant
At least one agent in all but two or fewer categories
antibiotic resistant infections – pandrug resistant
Non-susceptibility to all agents in all antimicrobial categories
Antibiotic resistant infections – examples
methicillin resistant staphylococcus (MRSA)
Multidrug resistant microbacterium tuberculosis (MDR – TB)
Vancomycin resistant enterococcus (VRE)
Extended spectrum beta lactamass (ESBL) bacteria
Escherichia Coli and Klensiella pneumoniae
Multidrug resistant pseudomonas aeroginosa
Multi drug resistant Acinetobacter baumanni (MDRAB)
Clostridoides difficile (C. Diff)
Proper hand washing technique
Hand washing with soap and water is the best method to remove pathogens, including highly contagious pathogens (e.g. Norovirus, C. Diff,) from your hands
What your hands with clean, running water (warm or cold), and apply soap
Lather your hands by rubbing them together with the soap. Be sure to lather the back of your hands, between your fingers, and under your nails.
Scrub your hands for at least 20 seconds. Some pathogens such as norovirus, require a longer time at least 60 seconds to remove stool contamination from hands
Rinse your hands well under running water (stool contaminated norovirus hands should be rinsed for at least 20 seconds)
Dry your hands using a clean, disposable tower, or air dry them.
Hand washing - if soap and water are not available
If soap and water are not available, use an alcohol based hand sanitizer that contains at least 60% alcohol. (continue to rub the sanitizer overall hand and finger surfaces until dry). Alcohol based hand sanitizers can quickly reduce the number of pathogens, but do not remove all pathogen types e.g. Norovirus, C. Difficile spores
Medical surgical equipment
Medical surgical equipment is used in all areas of the hospital. Some type types of equipment are used only in specialty areas, such as the intensive care unit.
The presence of certain types of equipment in a patient’s room can provide the physical therapist with a preliminary idea of the patient’s general medical condition and the appropriateness of therapeutic physical therapy intervention, prophylactic physical therapy intervention, or both
Oxygen therapy
The general indication is hypoxemia
Increase O2 levels in the blood and alveoli to improve oxygenation
Hypoxemia
SaO2 <90% (Some cases <88%)
Arterial blood O2 partial pressure is <60 mmHG
Oxygen therapy indications
severe trauma, shock, acute myocardial infarction, surgery, carbon monoxide/cyanide
Variable Oxygen Delivery for SBA - FiO2
Fraction of inspired oxygen
The concentration of oxygen in the gas mixture.
The gas mixture in room air has a fraction of inspired oxygen of 21%, meaning that the oxygen concentration in room air is 21%.
FiO2 - COPD
<88%
FiO2 - MI or stroke
Min <93%
Variable oxygen delivery For SBA - Nasal Canula
Delivers supplemental O2 mixed with RA (21%), usually 1–6 lpm
Fio2 - 24 to 44%

Variable oxygen delivery for SBA – open face tent
Provides humidified, supplemental O2 mixed with RA
Can also be used for nebulized medications
Fio2 - 30 to 55

Variable oxygen delivery for SBA – Closed face mask
Delivers supplemental O2 mixed with RA
Mask capacity is limited but does allow for the collection of O2 about the nose and mouth
Fio2 - 40 to 60%

Variable oxygen delivery for SBA – Transtracheal oxygen catheter
Used for long-term O2 therapy
Indicated when there are complications with or suboptimal nasal cannula use, nocturnal hypoxemia despite nasal cannula

Variable Oxygen Delivery for SBA - Tracheostomy mask or collar
Provides supplemental, humidified O2 or air at a tracheostomy site
Fio2 - 28 to 100%

Variable Oxygen Delivery for SBA - Partial non-rebreather mask
Mix of supplemental O2 and RA
Provides a high FiO2 to the patient while conserving the O2 supply
Two-way valves in the mask allow for RA inhalation in addition to supplemental O2.
Fio2 - 40 to 60%

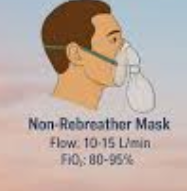
Variable Oxygen Delivery for SBA - non-rebreather mask
Provides the patient with the highest concentration of supplemental
O2 available via a face mask in a variable-performance system
One way valves control inflow of supplemental O2 and outflow of exhaled air so that the patient is only breathing the supplied O2
FiO2 - 60-80%
Fixed Performance Oxygen Delivery - Air entrapment Mask
Provides a specific concentration of supplemental O2 using color- coded diluter pieces to ensure accurate FiO2 delivery
Fio2 - 24 to 50%
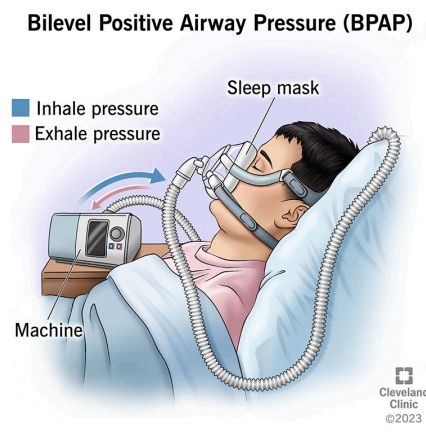
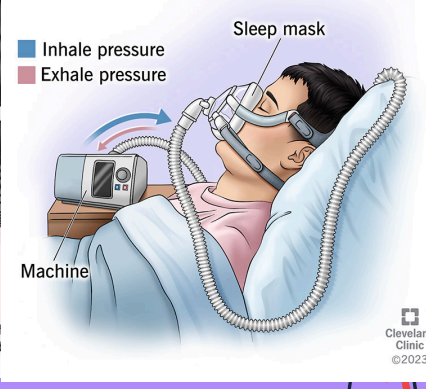
Fixed Performance Oxygen Delivery - BiPAP
Bilevel Positive Airway Pressure
Pressure-supported, noninvasive ventilation that provides positive inspiratory and end-expiratory pressure
May be used to avoid intubation and mechanical ventilation
Often used in the hospital or home setting for the management of obstructive sleep apnea
Fio2 - 21 to 100%
Non-Invasive Medical Monitoring - Telemetry
Continuous monitoring of heart rate and rhythm and respiratory rate (ECG)
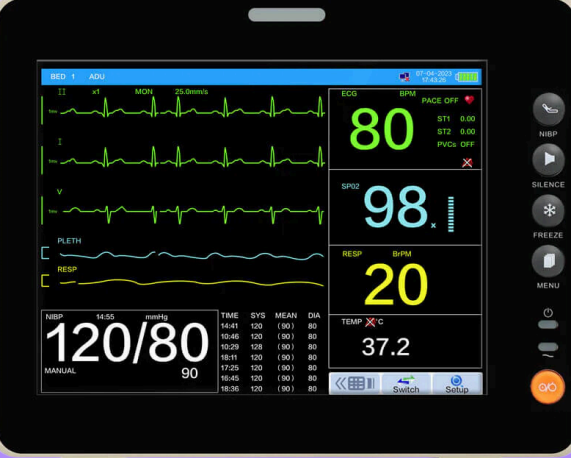
Non-Invasive Medical Monitoring - Pulse Oximeter
A noninvasive, transcutaneous method of monitoring the percentage of hemoglobin saturated with O2 in arterial blood
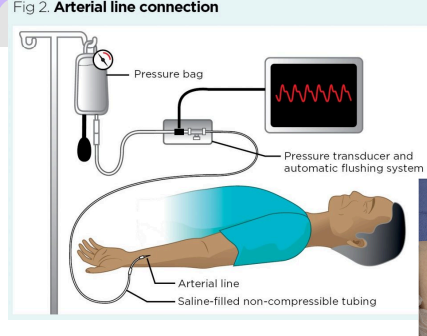
Invasive Medical Monitoring - Arterial Line
Direct and continuous monitoring of systolic, diastolic, and MAP; source for repeated arterial blood gas
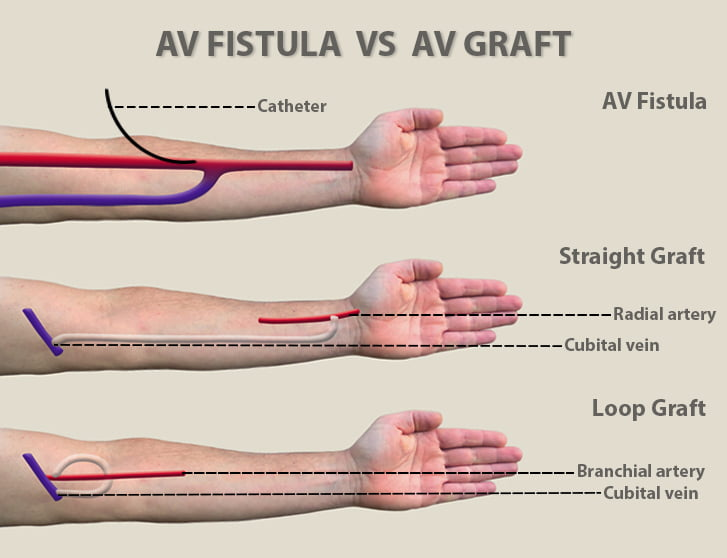
Medical surgical management devices - AV fistula / graft
Provides access for long term hemodialysis
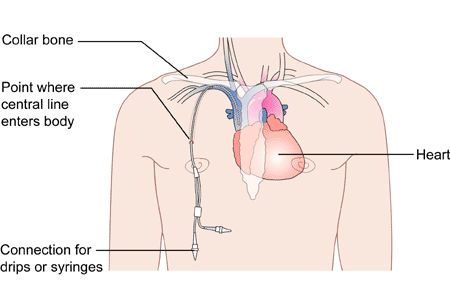
Invasive Medical Monitoring - Central Venous Catheter
Indicated for a patient with significant fluid volume deficit and is used as a guide to overall fluid balance
Measurement of CVP is a direct reflection of right heart function
Also provides vascular access for parenteral nutrition, large fluid volumes, or noxious medication
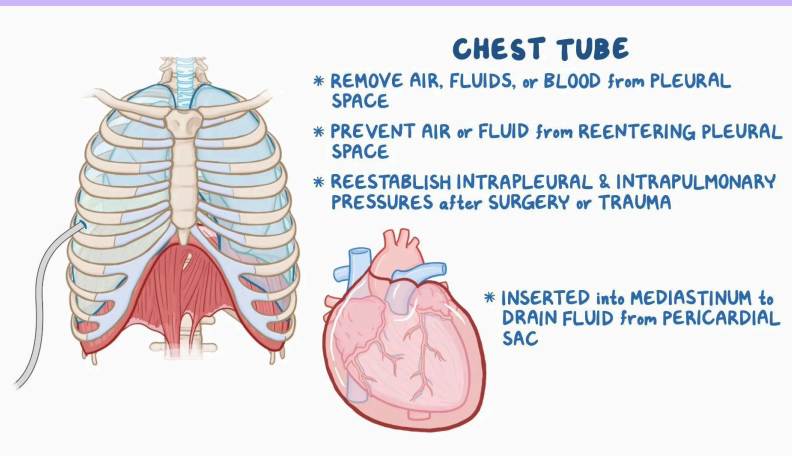
Medical surgical management devices - Chest tube
Removes and prevents the reentry of air or fluid from the pleural or mediastinal space and provides negative intrapleural pressure
Used to treat pneumothorax, hemothorax, pleural effusion
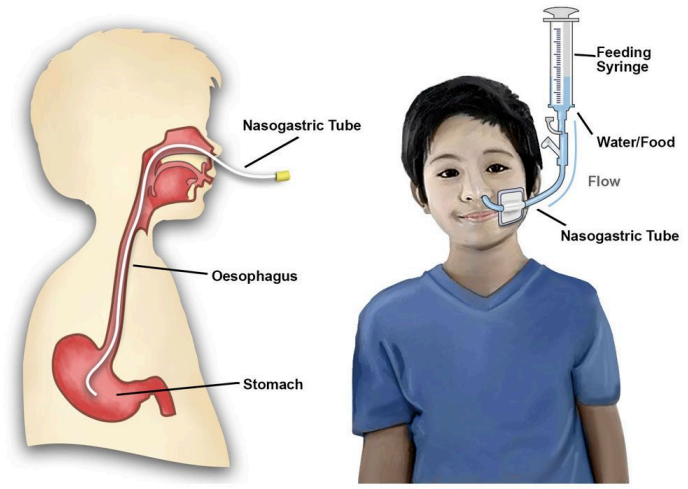
Medical surgical management devices - Nasogastric Tube
For feeding, gastric decompression and keeping the stomach empty after surgery
Medical surgical management devices - Nebulizer
Delivers aerosolized water or medications to the respiratory tract, lungs, throat, or nose

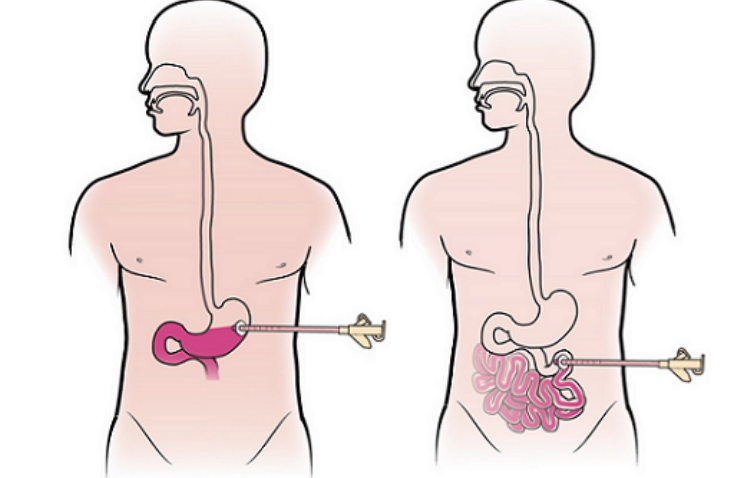
Medical surgical management devices - Percutaneous endoscopic gastronomy / jejunostomy
Provides long-term access for nourishment to patients who are
unable to tolerate food by mouth
or have a nasoenteral obstruction,
or for a patient with confusion/ agitation at risk for nasoenteral tube dislodgement
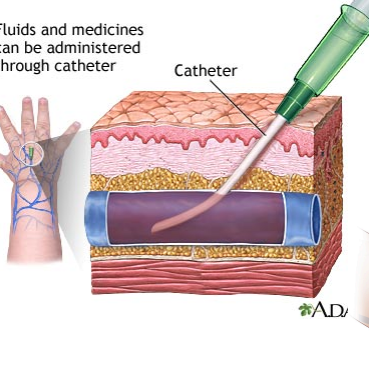
Medical surgical management devices - Peripheral IV Line
Provides temporary access for delivery of medications, fluids, electrolytes, nutrients, or blood product transfusions
It cannot be used to draw blood
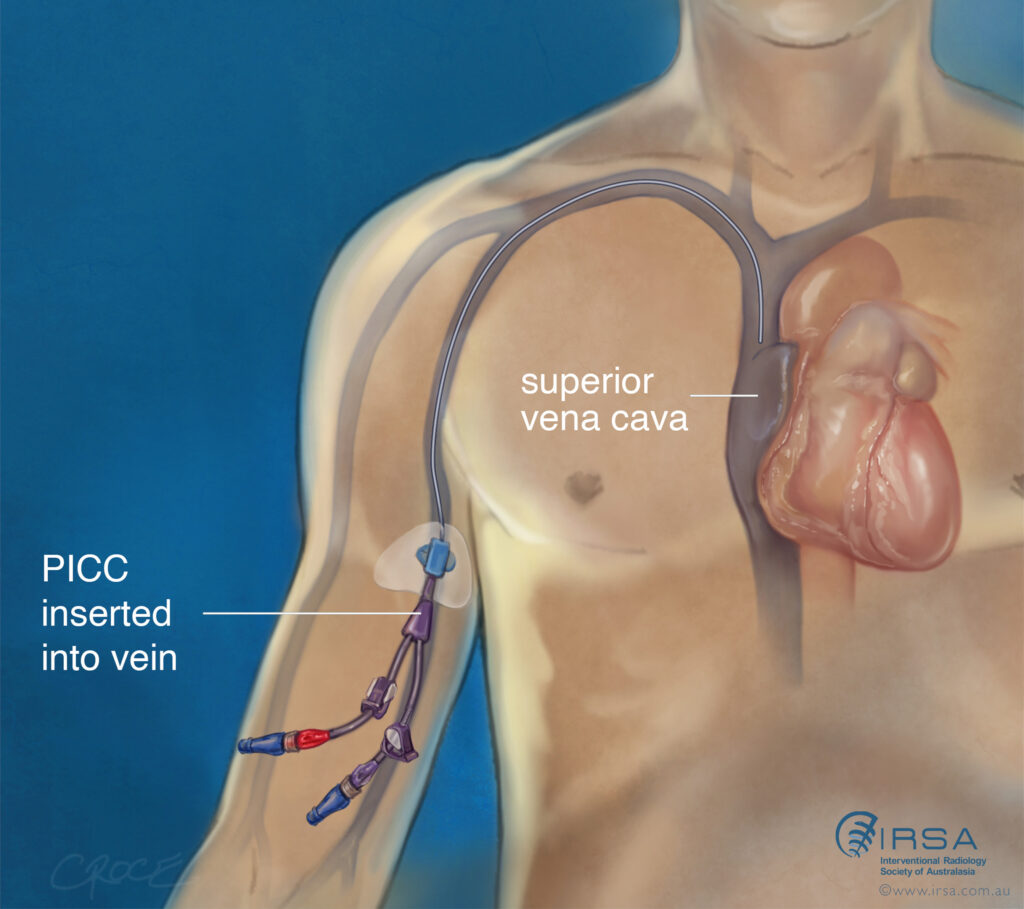
Medical surgical management devices - Peripherally inserted central catheter
Provides IV access for administration of total parenteral nutrition (TPN), medications, fluid, blood products, or chemotherapy.
Generally placed for midterm access (weeks to months)
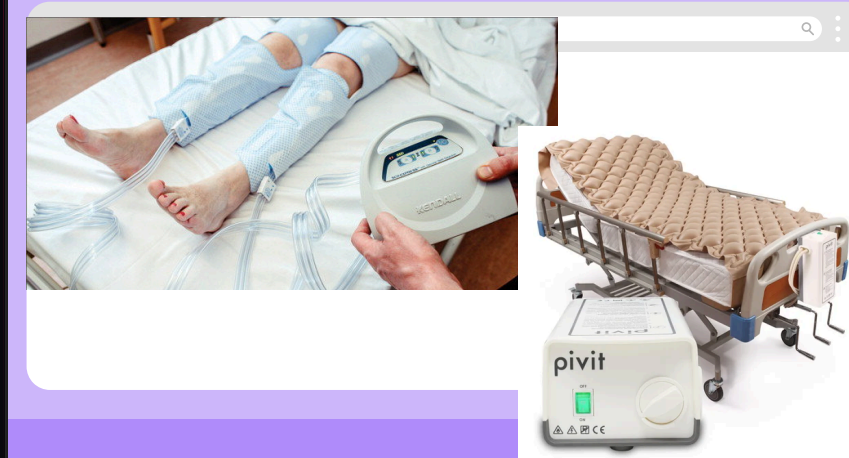
Medical surgical management devices - Sequential compression devices
Provides intermittent pressure to the lower extremities via gradual and sequential inflation and deflation of the air-filled sleeves
Promotes venous return and prevents deep vein thrombosis (DVT) and venous thromboembolism (VTE) secondary to prolonged or postoperative bed rest or inactivity