EHR Final Exam Preparation Guide
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
61 Terms
ECW Screenshots
Questions include screenshots from the ECW program.
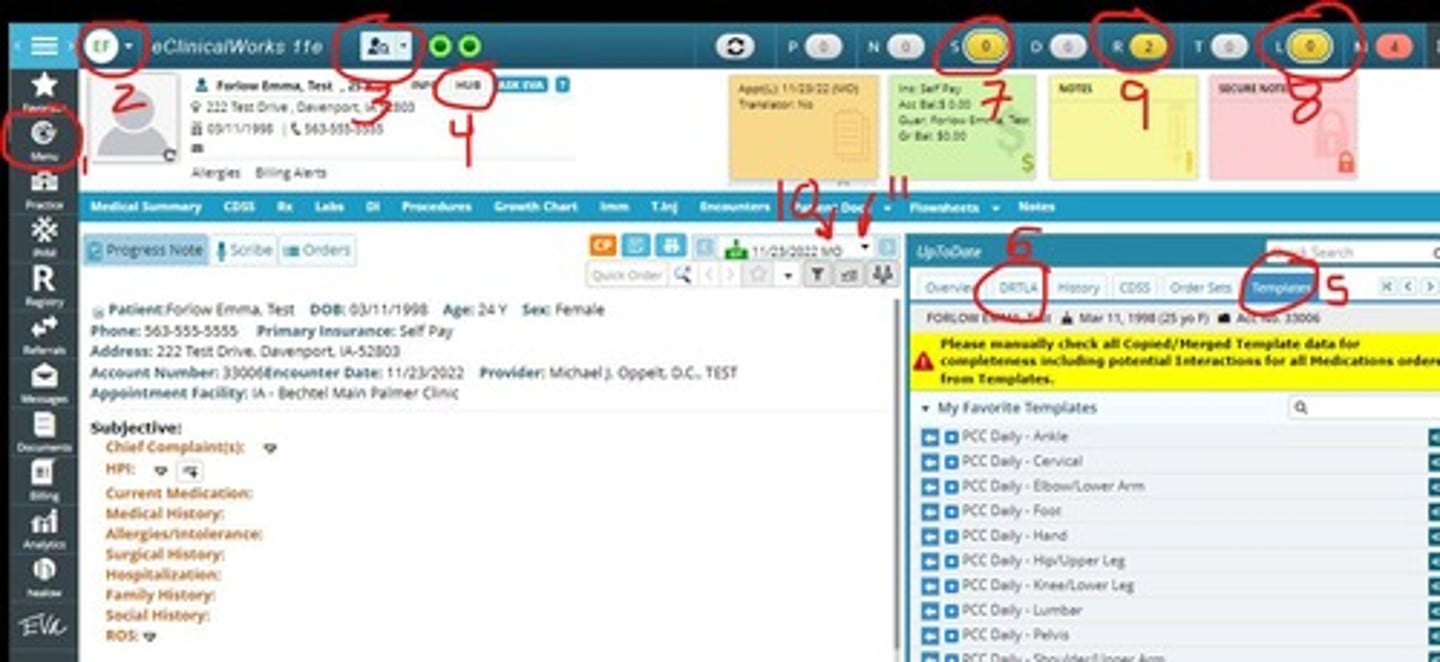
Documentation Focus
Know where to place information in notes.
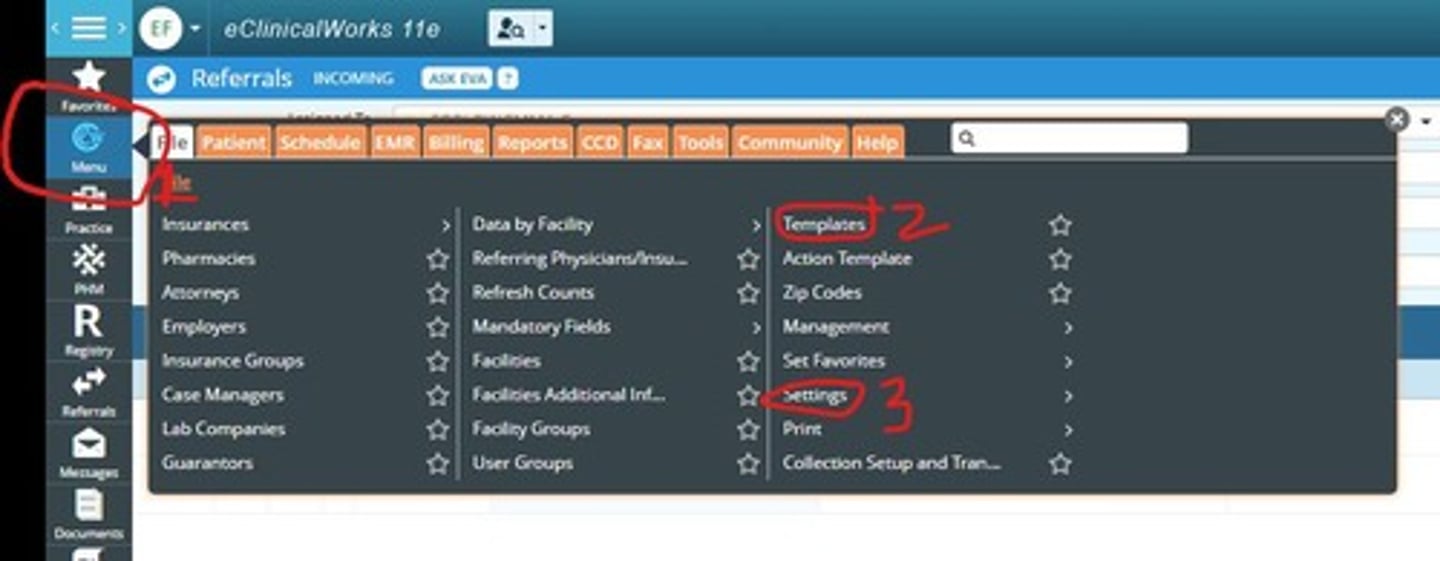
Menu Button
Used to access settings and templates.
Patient Search
Search patients by last name, first name, or number.
Patient Hub
Access patient information and demographics.
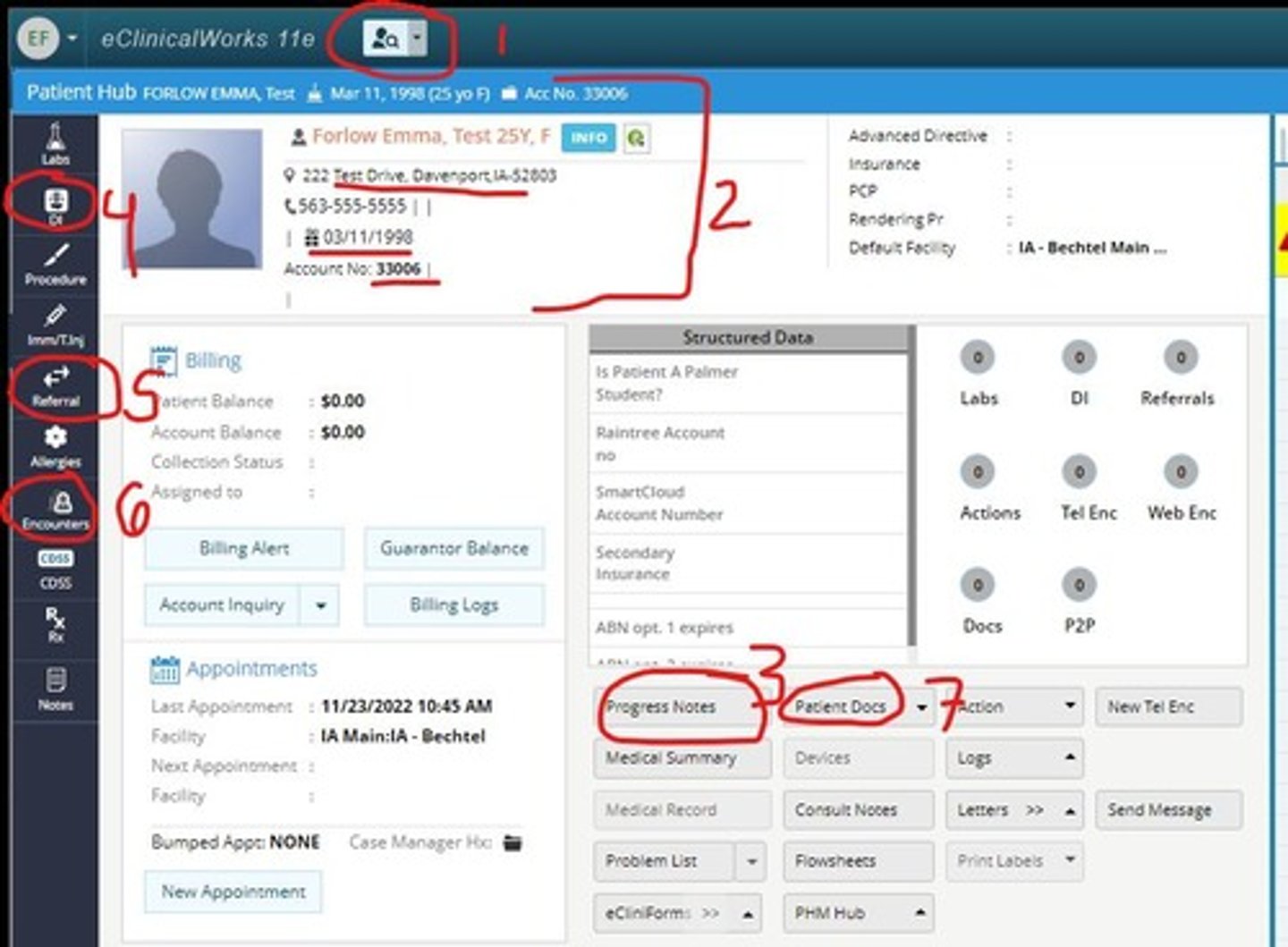
Progress Note
Document patient assessments and treatment plans.
Subjective Info
Add patient history and symptoms in HPI section.
Objective Findings
Document examination results like ROM and inspection.
Assessment Codes
Use ICD10 codes for diagnoses.
Treatment Plan
Outline treatment and ordering procedures.
Log Out Procedure
Click initials to log out properly.
Template Usage
Pull templates into notes for efficiency.
DRTLA Panel
Access historical patient information in right chart.
Referral Management
Manage referrals to rehabilitation departments.
Lab Orders
Use the R jelly bean for lab tests.
Patient Documentation
Includes insurances and scanned records.
Initials in Progress Note
Ensure correct provider is noted in documentation.
Weekly Review
Review one week at a time for better understanding.
HPI
History of Present Illness, patient symptom details.
Subjective
Patient-reported information about their condition.
Objective
Doctor's findings during patient examination.
Inspection
Visual examination of the patient.
Assessment
Evaluation of patient's condition and diagnosis.
ICD-10 Codes
International Classification of Diseases coding system.
CPT Codes
Current Procedural Terminology for billing procedures.
Plan
Treatment strategy based on assessment findings.
Radiology Order
Request for imaging studies under treatment plan.
Procedure
Specific actions taken during patient care.
Care Plan
Document outlining follow-up and treatment goals.
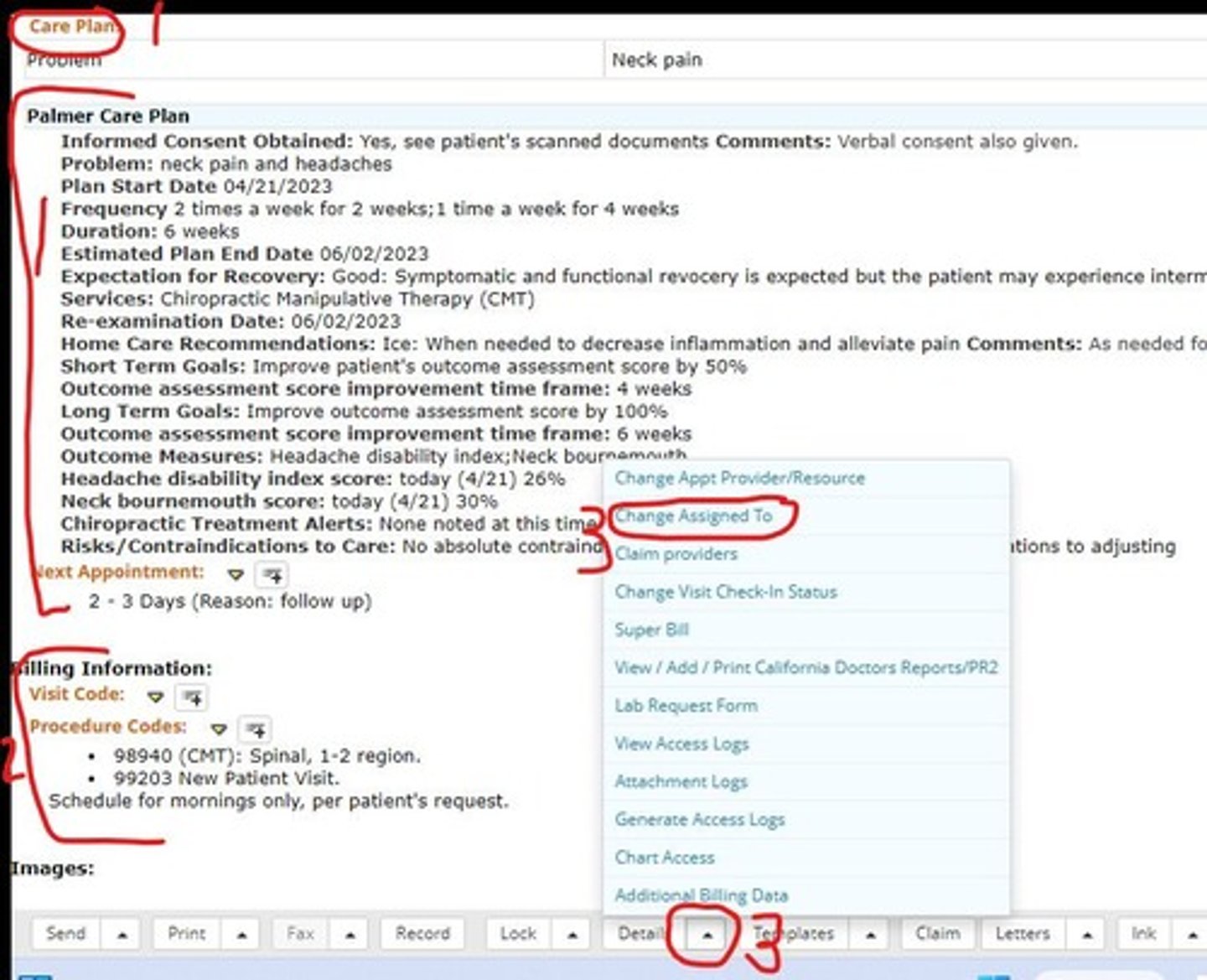
Visit Code
Code used for billing patient visits.
Examination
Detailed assessment of specific body regions.
PART Findings
Documentation supporting adjustments in treatment.
Re-evaluation
Assessment for previously established patients.
Referral
Request for specialist consultation or treatment.
Contraindications
Factors that prevent certain treatments or procedures.
Active Range of Motion
Patient's ability to move joints voluntarily.
Passive Range of Motion
Movement of joints by an examiner.
Neurological Testing
Assessment of nerve function and reflexes.
Orthopedic Testing
Evaluation of musculoskeletal system for injuries.
Billing Information
Details required for processing patient charges.
Diagnosis Code
Code used to identify a patient's diagnosis.
Pin Template
Template for entering personal identification number.
Assigned To
Designates who is responsible for the note.
Lock Button
Finalizes note; only providers can use.
Tracking Board
Monitors patient and doctor locations in clinic.
PEN
Indicates patient scheduled but not arrived.
ARR
Patient arrived; timer for visit starts.
STUD
Patient is currently in room with student.
READY
Indicates student is prepared for doctor visit.
PROV
Identifies doctor's current working room.
CHK
Indicates patient has been checked out.
CANC
Patient has cancelled their appointment.
N/S
Patient did not show up for appointment.
R/S
Patient has rescheduled their appointment.
RAD/LAB/REF
Patient is in another department for services.
Daily Visit
Routine patient evaluation and treatment process.
ROS
Review of Systems; history questions for regions.
PFSH
Past Family and Social History relevant to patient.
Level of Service
Determines complexity of examination and billing.
New Patient Codes
Codes for billing new patient evaluations.
Established Patient Codes
Codes for billing returning patient evaluations.