Lesson 71 Hormones and hormonal disorders
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
hormonal changes in estrus cycle
high estrus in follicular phase. estrogen decreases in luteal phase
high progesteron in luteal phase→ peaks near the end
uterus releases PGF2a if no pregnancy detected peaks near end of luteal phase. PGF2a causes decrease in progesterone
FSH sharp increase and LH surge causes by estrogen prior to ovulation
what hormones control the length of estrus cycle
prostaglandin
Other clinical application of prostaglandin
estrus synchronization in cattle and horses by terminating cycle earlier→ induces heat sooner
how long is estrus cycle in horses and cows
21 days
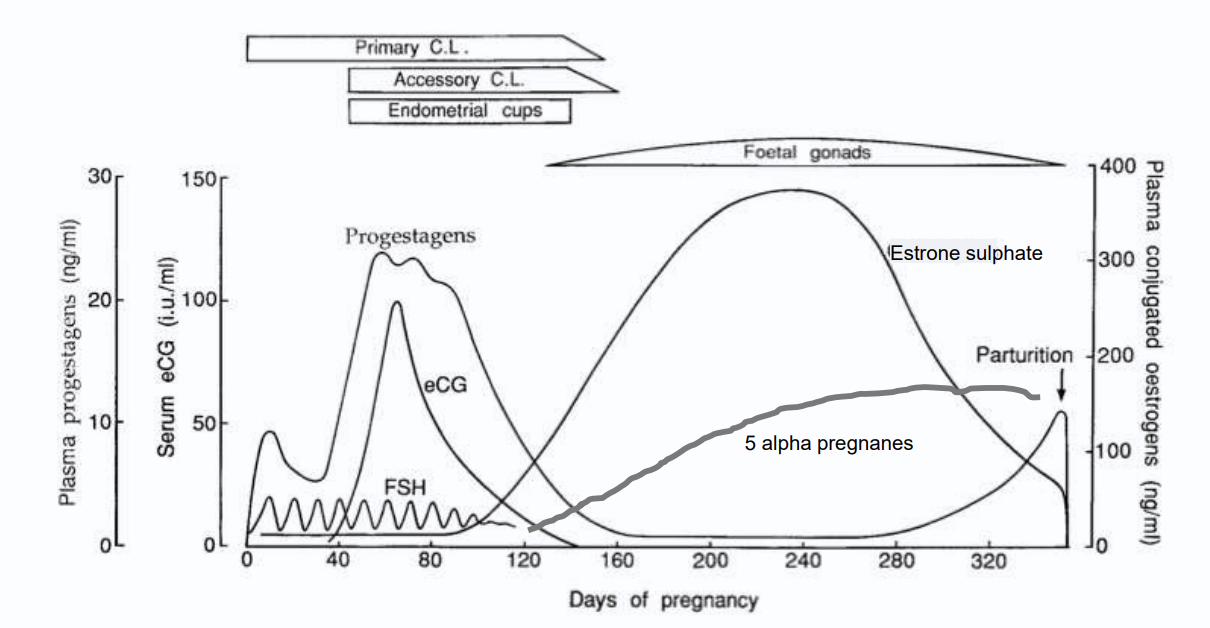
primary and accessory CL produces progesterone
Endometrial cups form day 35 of pregnancy and produces ECG
ECG mimics FSH and works like LH in mares
foetal gonads produce estrogen sulphate (pregnancy specific)
How long is canine diestrus
2 months
how long is canine heat phase?
9 days
how long is canine gestation
63 days
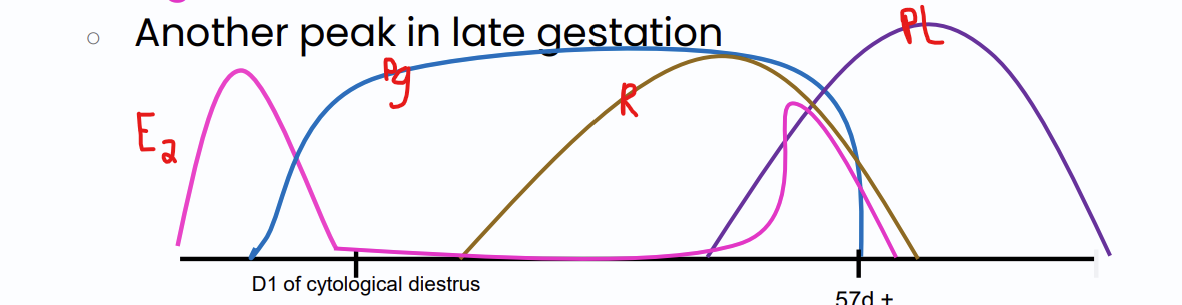
relaxin
produced by placenta in dogs and detected day 20 of pregnancy
function: maintenance of pregnancy and during parturition it loosens the muscle for easier passage of fetus
Prolactin
increases in late gestation.
function: produce milk
estrogen during pregnancy
peaks again in late stage of gestation
hormones used to diagnose pregnancy in mares
EcG-produced by endometrial cups but will still be present until end of pregnancy regardless of termination
hormones used to diagnose pregnancy in dogs
relaxin since its specifically from the placenta
5 alpha pregnanes
metabolite of progesterone. increases in late gestation
function:progesterone like functions
What is the average size of a normal preovulatory follicle in cows?
1-2 cm
cystic ovarian disease in cattle
1 or more cystic structure on ovary that stay longer than 7-10 days and prevent normal cyclic activity
why is cystic ovarian disease common in dairy cows
bc producing lots of milk causes stress and they are also in a negative energy balance.
follicular cysts
thin walled, less than 3 mm thick
several large cyst or multiple small cysts
produces estrogen
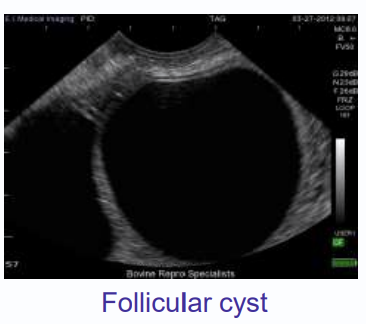
clinical presentation for follicular cysts
anaestrus, nyphomania (estrus like behavior), virilism (male characteristics)
luteal cysts
thick walled, more than 3 mm thick
single cysts
produces mainly progesterone
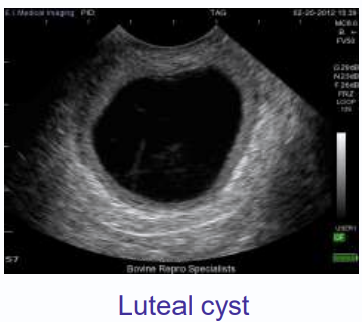
clinical presentation luteal cyst
anestrus
why does a cow with luteal cyst commonly present with anestrus
negative feedback from increased progesterone
difference between progesterone secreting vs estrogen secreting ovarian cyst
progesterone: signs of estrus
estrogen: signs of estrus, attraction to male dogs, swelling of vulva, discharge, hyperestrogenism if prolonged (alopecia, hyperpigmentation)
hyperestrogenism signs
bilateral alopecia, hyperpigmentation, bone marrow suppression, nonregenerative anemia, luekopenia, thrombocytopenia
how to treat follicular cyst on large animal
LH supplement or GnRH analog
-both acts as the missing LH surge to turn the follicle into a CL
follicular cysts form
when dominant follicle fails to ovulate due to lack of LH surge
how to treat follicular cysts in small animals
spay/ ovariohysterectomy
types of vaginal epithelial cells
anuclear, superficial, iintermediate and parabasal
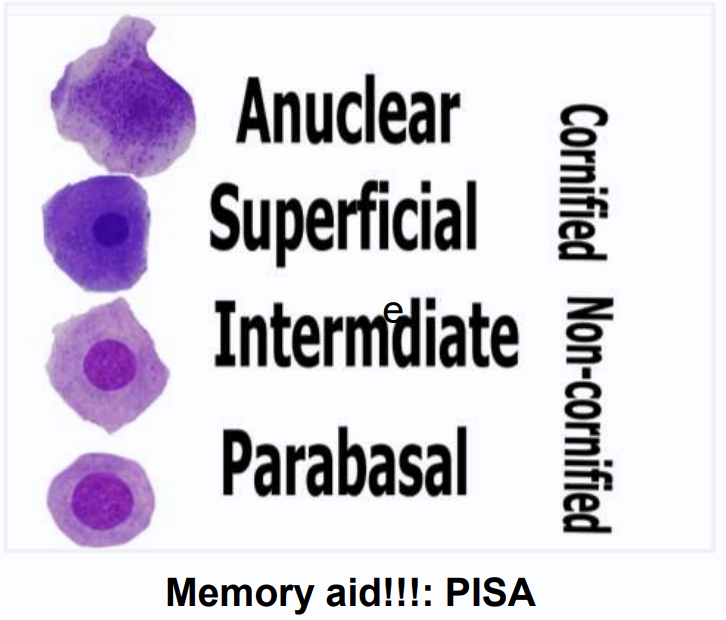
which vaginal cell types are cornified
anuclear and superficial
which vaginal cell types are noncornified
intermediate and parabasal
which cell types are under estrogen influence (shows animal is in heat)
cornified cells (anuclear and superficial)
pyometra
accumulation of pus in the uterus in presence of functional CL
Why does CL advance pyometra
secretes progesterone, closed cervix, lowered uterine defense, and increased gladnular secretion
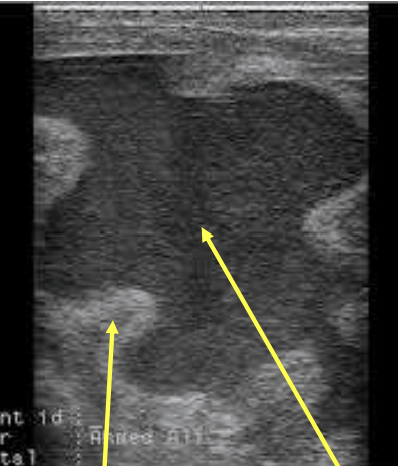
How does pyometra appear on ultrasound
thick uterine wall and hypoechoic fluid in the uterine lumen
What causes pyometra?
reoccuring infection, active CL, fetal death in closed uterus, bacterial organisms
clinical signs of pyometra in cattle
no systemic illness, closed cervix= no discharge, anestrus, non cyclic
rectal exam: enlarged uturus, fluid filled, thick walled atonic, and CL
pyometra in mares
similar to chronic closed abscess
-caused by inability of cervix to open(fibrosis)
endometrium becomes too damaged and fertility is impacted
-does not show signs of systemic illness
What hormones downregulates the uterine defense mechanism and results in closure of the cervix
progesterone
cystic endometrial hyperplasia (CEH)
progressive hyperplasia and cystic degeneration of endometrial glands with each nonpregnant cycle
-predisposes bitches to infertility and bacterial infection
-exogenous progesterone or estrogen can predispose to CEH
how does CEH look on the uterine horn
cobblestone appearance
E.coli
gram negative rod that causes 98% of the canine pyometras
clinical signs of pyometra in bitches
systemically ill, endotoxemic shock from endotoxins released form bacteria
renal dysfunction- prerenal azotemia (dehydration/shock), glomerular disease, decreased GFR, decreased ability to concentrate urine from endotoxemia
closed vs open cervix pyometra
closed- less sick
open- more sick
How does pyometra look on ultrasound in dogs
uterine lumen is more anechoic because pus is more watery in dogs than other species
which hormone more closely associated with development of pyometra in dogs
progesterone→ decreaes uterine defense, promotes CEH, closure of cervix
hypoluteidism
low plasma progesterone→ pregnancy loss
benign prostatic hyperplasia
most comonly diagnosed prostatic disease in dogs. mostly seen in 6+ yr old intact dogs
what causes prostatic hyperplasia
since prostate in androgen dependent
more testosterone which are reduced to dihydrotestosterone (DHT) which are biologically active and promotes prostatic hyperplasia
how many accessory sex gland in horses and bulls
4
how many accessory sex gland in pigs
3
how many accessory sex gland in cats
2
how many accessory sex gland in dogs
1
clinical presentation prostatic hyperplasia
can be aymptomatic, serosanguinous prepuital discharge (bloody discharge from penis), reddish semen,
straining to defecate
hematuria (NO dysuria or stranguria)
caudal abdominal pain
infertility
prostatic metaplasia
secondary to estrogen stimulation, low grade inflammation
dx: squamous epithelial cells on cytology
prone to cyst, prostatitis/abscess