Chest X-Rays
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
Aspergilloma
Pulmonary fibrosis
Radiation fibrosis
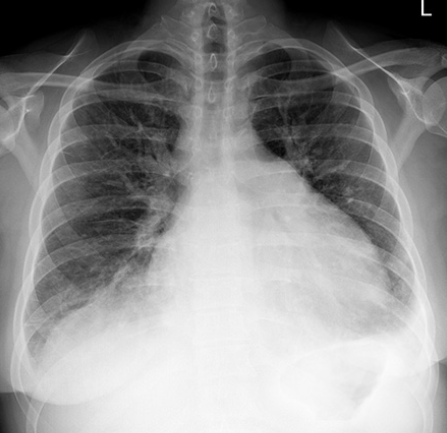
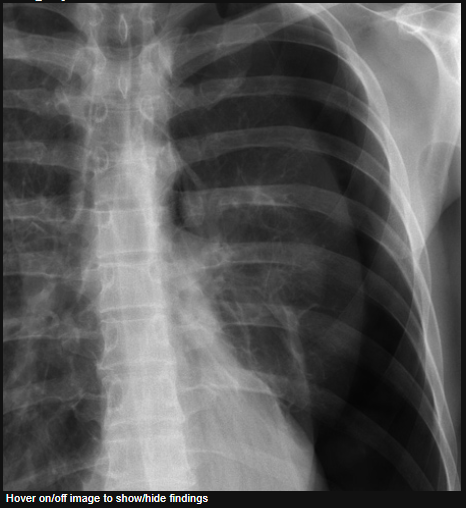
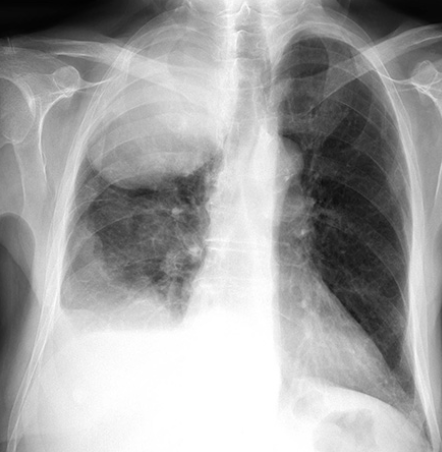
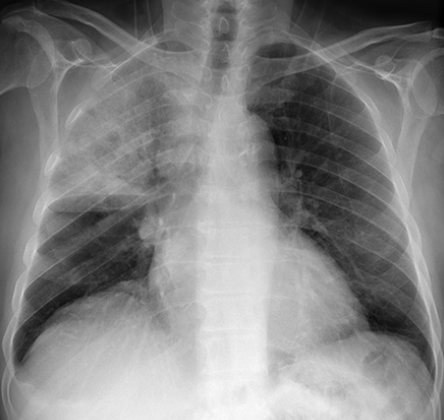
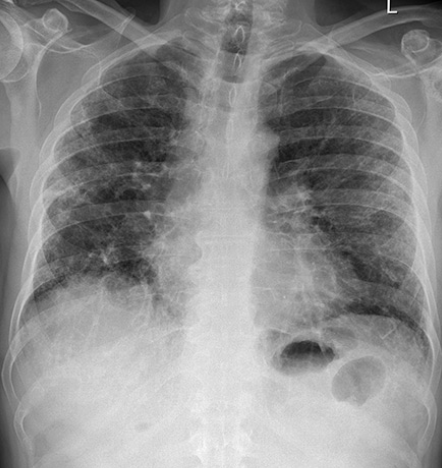
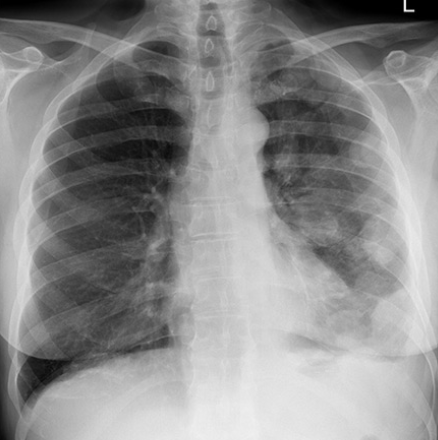
The trachea is deviated to the left. It is possible to say this with confidence because the patient is not rotated - the spinous processes lie midway between the medial ends of the clavicles. Any deviation of the trachea from the midline is therefore genuine.
Whenever you see deviation of the trachea, ask yourself if it has been PUSHED or PULLED. Here the trachea has been PULLED to the left by the volume loss in the left upper lobe caused by localised lung fibrosis. In this case this was due to previous radiation treatment.

PCP

Tension pneumothorax
Signs of tension
The left lung is completely compressed (arrowheads).
The trachea is pushed to the right (arrow)
The heart is shifted to the contralateral side - note right heart border is pushed to the right (red line)
The left hemidiaphragm is depressed (orange line)
Pleural effusion
Here the trachea and mediastinum are deviated to the right.
Are they PUSHED or PULLED?
There is opacification of the left lower hemithorax due to a pleural effusion (fluid gathering in the pleural space). This has PUSHED the whole mediastinum to the right.
In this case the patient was found to have mesothelioma, a malignancy of the pleura related to asbestos exposure.
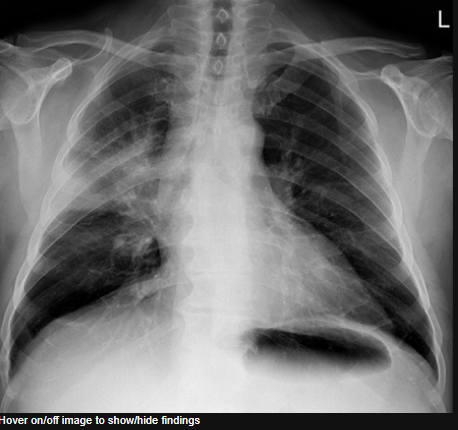
Pneumothorax: Large pneumothorax
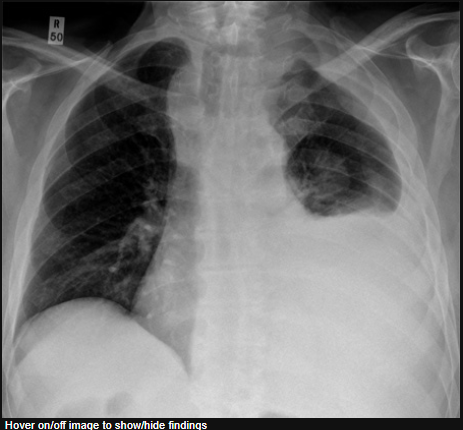
Along with symptoms such as breathlessness, establishing the size of a pneumothorax helps to determine management.
Pneumothoraces are managed in accordance with British Thoracic Society guidelines which define a large pneumothorax as being of greater than 2 cm width at the level of the hilum.
This chest X-ray shows a large pneumothorax (P) which is >2 cm depth at the level of the hilum.
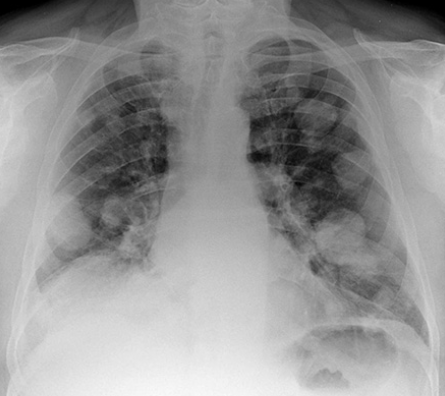
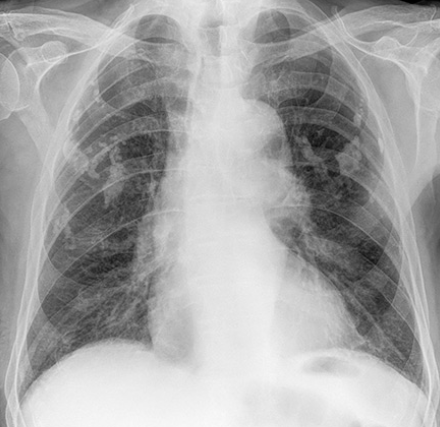
Sarcoidosis
Bilateral hilar enlargement - Sarcoidosis
In this image both the hila are enlarged and of increased density
Bilateral hilar enlargement is the classic chest X-ray appearance of sarcoidosis – as was found to be the case in this patient following lymph node biopsy

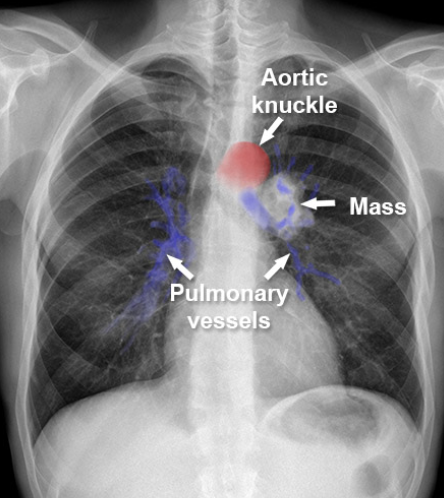
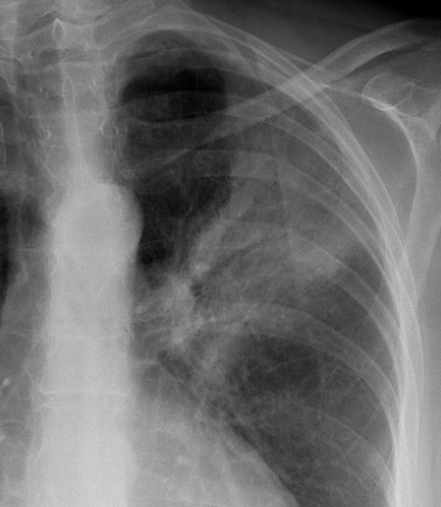
Unilateral hilar enlargement - Lung cancer
Learning to assess the hilar structures is difficult
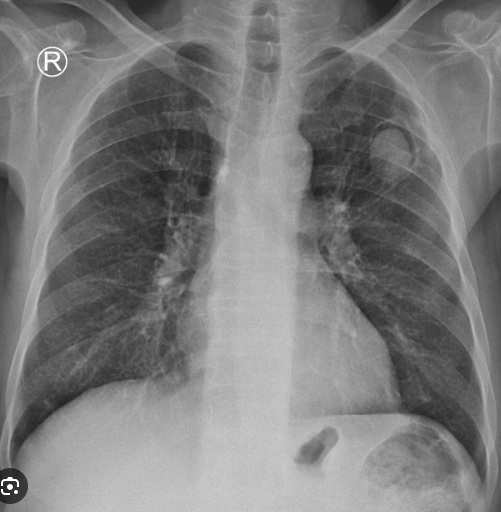
Normal hilar structures are asymmetric in shape but are usually similar in size and density
Discrepancy in size or density of the left and right hila may indicate a pathological process
In this image the left hilum is too big and too dense (white) and the normal pulmonary vessels are difficult to delineate
Following bronchoscopy and tissue biopsy this mass was found to be a primary bronchogenic cancer
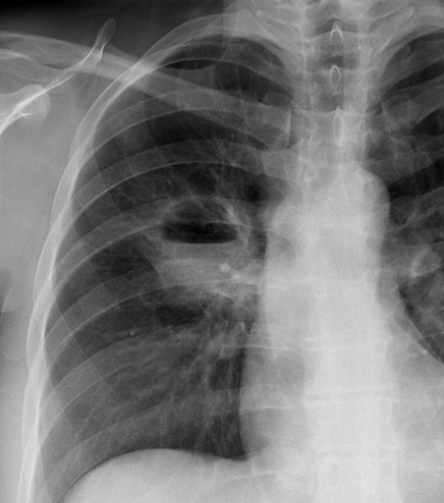
Right upper lobe collapse
There is volume loss of the right upper lobe. The right upper zone has become dense due to lobar collapse. The volume loss has displaced the trachea which is PULLED to the right, and the horizontal fissure (arrow) has been PULLED upwards.
Right upper lobe collapse is hardly ever caused by plugging of mucous or foreign bodies. The presence of right upper lobe collapse in an adult should therefore immediately raise the suspicion of an underlying malignant process occluding the right main bronchus.
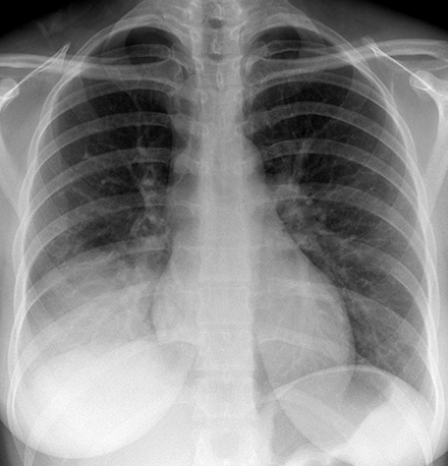
Small pneumothorax
This chest X-ray shows an apical pneumothorax (P) which does not reach down to the level of the hilum.
Although size is an important factor in the management of a pneumothorax the clinical features are also considered. If a patient with a pneumothorax is breathless or has known lung disease then interventional measures can be implemented even if the pneumothorax is small.
Lung cancer - Mass
This image shows a very large rounded mass filling the upper zone of the right lung
Whenever there is an abnormal area of shadowing (increased density/whiteness) in the lungs, the diagnosis of infection or cancer should be considered likely causes
It is frequently the clinical information which determines the diagnosis rather than the X-ray
The presence of a pleural effusion does not help to determine if an area of abnormal shadowing is due to infection or cancer as both can cause effusions
Lung cancer - consolidation
This X-ray shows an area of air-space shadowing (consolidation)
This appearance can be due to either infection or cancer - an X-ray cannot determine the difference
Further investigation with CT and bronchoscopy found a primary lung malignancy in this case
Note: Remember that the term ‘consolidation’ does not only refer to infection. The term ‘air-space shadowing’ or other similar descriptive terms are often used in radiology reports.
Read more on consolidation
Hilar mass and effusion
The right hilum is grossly abnormal in this image - compare with the left side where the normal vascular structures of the hilum are clearly defined
The mediastinum is widened due to enlargement of lymph nodes immediately to the right of the trachea - the right paratracheal stripe is no longer visible
Blunting of the right costophrenic angle and formation of a ‘meniscus’ are typical features of a pleural effusion
Lung cancer was confirmed following bronchoscopy and biops

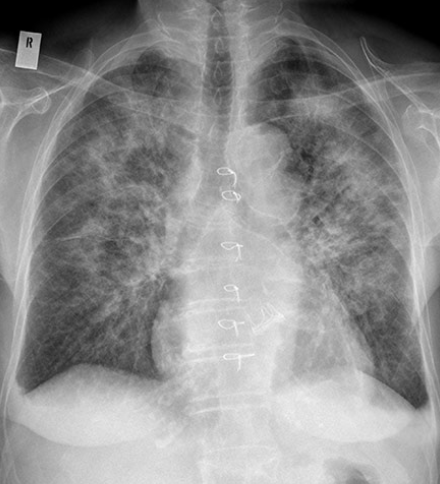
Cavitated lung mass
Lung cancers may initially form a solid mass and then cavitate internally due to cell necrosis
Squamous cell lung cancer is the cell type most likely to cavitate - as was confirmed in this patient following biopsy
Lung cavities can be caused by diseases other than cancer - such as infection or vasculitis
Read more about lung cavities here
This patient had a previous history of coronary artery bypass graft (CABG) surgery - note the sternal wires and clips

Metastases (to lung) - Cholangiocarcinoma
The lungs are a common site of metastatic disease from other parts of the body
The appearances of metastases are highly varied
This image shows numerous small lung nodules scattered throughout both lungs
This patient had a metastatic cholangiocarcinoma
Metastases from other cancers - such as breast or thyroid cancer - can have similar appearances

Metastases (to lung) - Renal cell carcinoma
This image shows numerous lung nodules of varied sizes scattered throughout both lungs
This patient had renal cell carcinoma which is often said to give rise to ‘canon-ball’ metastases in the lungs - a descriptive term referring to their appearance - big and round
Air bronchogram - Example 1
‘Air bronchogram’ is a characteristic sign of consolidation – here is an example in a patient with pneumonia
The black lines represent patent airways within consolidated lung (highlighted area)
Consolidation - Right upper lobe
Consolidation may be limited to a particular lobe of the lung
This image shows consolidation of the right upper lobe which is confined inferiorly by the horizontal fissure
If the consolidation is due to infection, then the term ‘lobar pneumonia’ is correctly used
Lobar pneumonia is usually caused by typical organisms – such as Streptococcus pneumoniae
Consolidation - Right middle lobe
The right middle lobe is located below the horizontal fissure which confines the area of consolidation in this image
The right middle lobe is also next to the right heart border which is obscured in this image
Consolidation - Right lower lobe
Both this image and the image above could correctly be described as showing consolidation of the right lower zone
It is possible to determine that the consolidation in this image is in the right lower lobe rather than the middle lobe
The right lower lobe is located adjacent to the right hemidiaphragm which is not clearly visible in this image
The right heart border is still visible which indicates that the consolidation is not in the middle lobe
These images demonstrate examples of the silhouette sign
Read more about the silhouette sign
Primary TB
There are no radiological features which are in themselves diagnostic of primary mycobacterium tuberculosis infection (TB) but a chest X-ray may provide some clues to the diagnosis
This image shows consolidation of the upper zone with ipsilateral hilar enlargement due to lymphadenopathy
These are typical features of primary TB
Note: The chest X-ray may be normal in primary TB, in fact most patients infected are never unwell enough to require a chest X-ray
Miliary TB
Miliary TB is due to disseminated spread of mycobacterial infection
It can occur either at the time of primary infection or on disease reactivation – prognosis is poor
Very fine nodules are typically seen scattered throughout the lungs

Lung abscess with gas/fluid level
This patient had a history of breast cancer – (it would be unusual for a metastatic breast lesion to cavitate)
The cavity was an abscess which arose due to the patient being immunocompromised by chemotherapy drugs
A fluid level represents a collection of pus in the abscess
Bronchiectasis
Bronchiectasis may be present even if the X-ray is normal – most patients suspected of having bronchiectasis will need a high resolution CT to confirm the diagnosis
Severe bronchiectasis causes coarsening of the lung markings – very extensive in this case
COPD – Hyperexpansion
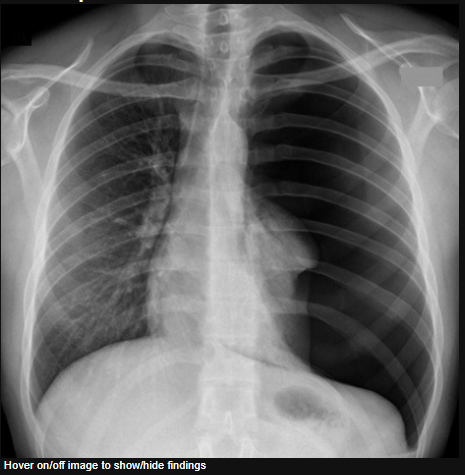
In normal subjects the diaphragm is intersected by the 5th to 7th anterior ribs in the mid-clavicular line
It is often difficult to see the ribs in patients with COPD as they are osteopenic due to long term steroid use - as in this patient
In this image, the 7th ribs, which are only just visible, intersect the diaphragm (red lines) level with the mid-clavicular line – so are the lungs hyperexpanded?
Patient positioning and use of accessory muscles of respiration can influence the anatomical positioning of the ribs on a chest X-ray
Flattening of the diaphragm (red lines) is often a more reliable feature of lung hyperexpansion
The green dotted lines indicate the predicted normal diaphragm shape and position

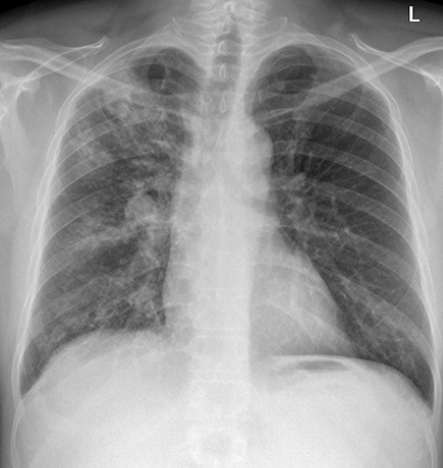
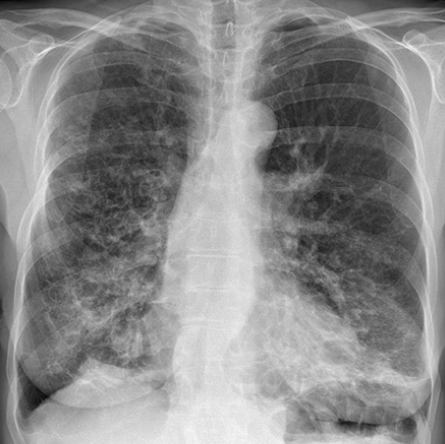
Reticular shadowing - Fibrosis
Pulmonary fibrosis causes reticular (net-like) shadowing of the lung peripheries which is typically more prominent towards the lung bases
It may cause the contours of the heart to be less distinct or ‘shaggy’
Chest X-rays can be helpful in monitoring the progression of pulmonary fibrosis
Asbestos plaques
Calcified plaques are associated with previous exposure to asbestos and are almost invariably asymptomatic
They appear as irregularly-shaped areas of calcific density (as white as bone) and should not be mistaken for areas of consolidation
Pleural plaques are a benign entity (do not lead to cancer or mesothelioma) and their presence does NOT equate to the diagnosis of ‘asbestosis’
Note: Asbestosis is fibrosis of the lung caused by the presence of asbestos fibres in the lungs themselves – it may have similar appearances to the fibrosis seen on the previous page
Mesothelioma
(Same patient as image above)
The effusion in the image above was drained
Lobulated thickening of the pleura became visible
The left lung is reduced in volume
These are the typical features of mesothelioma
Note: Pleural metastases (usually from an adenocarcinoma) may have similar appearances to mesothelioma
Cardiomegaly
History of hypertension and angina
This patient has an enlarged heart
CTR = 68%

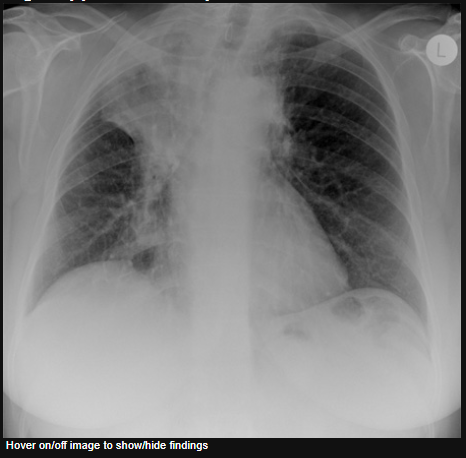
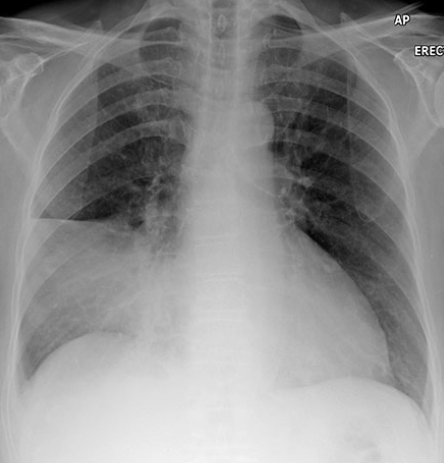
Upper zone vascular prominence
Enlarged heart (CTR = 55%)
The upper zone vessels are prominent – an indicator of increased pulmonary venous pressure
Signs of pulmonary oedema have also developed – septal lines (Kerley B lines) due to interstitial oedema, and airspace shadowing due to alveolar oedema
The costophrenic angles are blunt due to bilateral pleural effusions

Alveolar oedema - Bat's wing pattern
Alveolar oedema is caused by fluid leaking from the interstitial tissues into the alveoli and small airways, and manifests as airspace shadowing (consolidation)
In the context of acute pulmonary oedema, alveolar oedema radiates symmetrically from the hilar regions in a ‘bat's wing’ distribution of airspace shadowing
Note the enlarged heart (CTR 60%) and the cardiac surgery artifact – sternal wires and metallic heart valve
Blunting of the costophrenic angles is due to pleural effusions – interstitial fluid has leaked into the pleural cavity
Pericardial effusion
This image shows some of the features of heart failure
1 - Upper zone vascular prominence
2 - Airspace shadowing (alveolar oedema)
3 - Septal lines (interstitial oedema)
4 - Pleural effusion
The heart is also enlarged and has a globular (rounded) appearance due to a pericardial effusion (fluid accumulation within the pericardial sac)