Looks like no one added any tags here yet for you.
Pain
Subjective & Multidimensional, unpleasant sensory and emotional experience associated with actual or potential tissue damage
purpose of pain
signals ongoing or potential tissue damage, protective measure to prevent further injury.
Types of pain
acute and chronic
acute pain
immediately felt, happens when experiencing injury
chronic pain
Pain lasting longer than 3 months
categories of pain
Somatic
Visceral
Psychological
somatic pain
originates from skin or muscoskeletal system (ligaments, tendons, muscle, joints), usually localized pain, can usually pinpoint point in time in which pain is felt (Ex.ankle sprain pain)
visceral pain
pain originating from visceral organs, diffused pain (not pinpointed) or deferred pain (causes pain elsewhere in body), usually have other symptoms like nausea
Psychological pain
sensation of pain but no apparent physical cause of pain ( damage). Psycological/emotional pain, feel pain when anticipate something will hurt
Pain is felt when there is a stimulation of
Afferent nerve endings called nociceptors
types of nociceptors
Mechanosensitive, thermosensitive, chemosesnsitive
Mechanosensitive nociceptors
respond to touch and pressure or stretch
thermosensitive nociceptors
respond to extremes of heat and cold
chemosensitive nociceptors
respond to different chemicals (serotonin- during inflammatory process)
referred pain
pain that is felt in a location other than where the pain originates
What causes referred pain?
mix up of messages where too many afferent nerve signals try to get through at same time and brain confuses areas of spinal cord sending up signals
radiating pain
pain felt at the site of tissue damage and in nearby areas
throbbing pain
vascular circulation
shooting pain
Nerve pain
deep pain
Bone pain
Stiff/achy pain
Chronic inflammation
Question to ask athletes about pain during initial assessment
Subjective assessment with open ended questions (pain scales)
Ex. Can you describe the pain, how long does pain last? Where does it hurt
OPQRST
A mnemonic used in evaluating a patient's pain:
Onset
Provoke/palliative (what makes better/worse)
Quality (describe pain)
radiate/reffered
Severity
Timing.
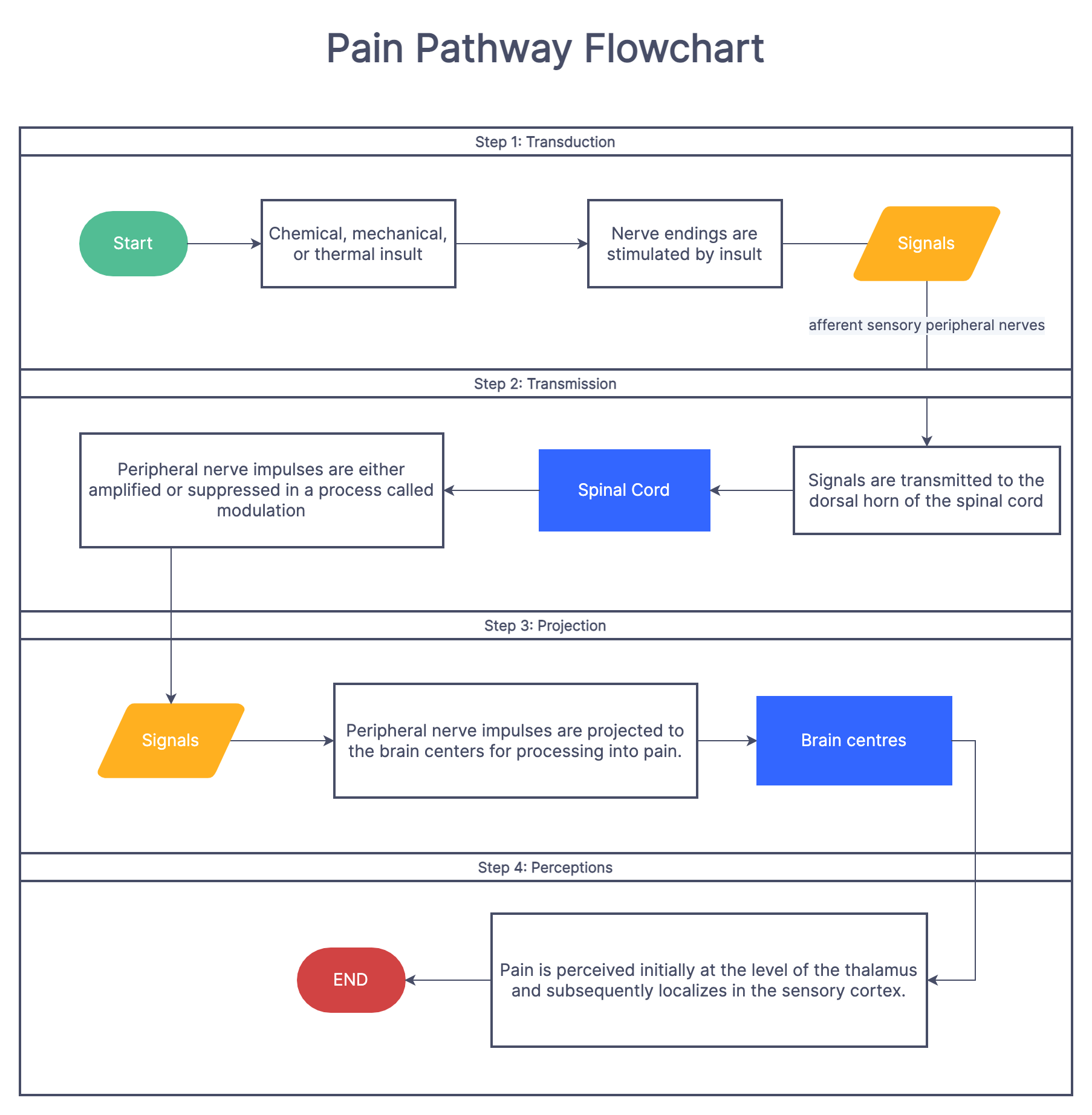
Pathway of pain
1. Noxious stimulus in peripheral
2. Nociceptors
3. Primary (first-order neurons) to spinal cord synapses and release substance P on dorsal horn
4. 2nd order neuron through ascending spinal tracts to brain
5. Thalamus — sensory relay station
6. Third order neuron
7. Cortex - registered as pain
8. descending spinal tracts
Types of afferent fibers
A beta & A delta or C
Aβ fibers
group 2 - signals travel quickly 35-75m/sec - low threshold for stimulation (doesn't take much to trigger impulse) - large diameter - TOUCH & PRESSURE & TEMPERATURE acute pain
Aδ Fibers (A Delta)
group 3 - medium/large diameter - thinly myelinated 5-30m/sec - pain messages sharp localized pain
C fibers
group 4 - no myelin 0.5-2m/sec - chronic aching pain - smallest diameter
Coping definition
ability to identify, manage and overcome issues that stress one in any capacity
With coping what are we looking to reduce?
reduce threat value of any stimulus and the associated emotions or tissue that may change it with
Can you enhance ability to cope with pain
through education and understand threat
How is perception related to coping with pain?
- painful experience will hurt less not at all if brain thinks you're not in danger / threatened
- perception can dictate outcome response (low threat perception = less pain response)
- kids have dramatic reaction right away to pain as they fear pain overall - quick to settle emotions as we'll
Pain control theories
Gate control theory, descending pain control (central braising) theory, β-Endorphin theory
gate control theory of pain
non painful stimulus blocks painful stimulus spinal cord level
• stimulation of Aβ fibers that blocks c and Aδ carrying fibers
• Substantia geletiosa acts as gatekeeper and determines pain response or afferent sensation through Aβ fibers to be transported through 2nd order neurons
• Gate = substantia geletnosa , is first come first served bases,
Ex When we grab our toe after hitting it we stimulate mechanosensitive receptors along Aβ fibers the fastest, which get to gate first, and therefore brain first. So brain feels touch and blocks pain signals
Descending pain (central braising) theory
???
β-Endorphin theory
noxious stimulus of nociceptors resulting in transmission of pain information along Aδ and C afferent can stimulate release of endogenous opiate like chemical called β-endorphin
• these are our body's natural painkillers
• Not clear why β-endorphins produce analgesic effects
• Can stimulate with exercise and acupuncture
• can help Chronic pain - prescribe exercise!!!!
2 ways to cope with pain
Passive and active coping
Active coping
want to learn about problem, want to explore new ways to move, will explore edges of pain, usually positive person and looks to make further plans
Pasive coping
people who avoid activity, would rather lie there well someone else fixes the
Pin perception psychological factors
- previous pain experience
• pain expectations
• pain tolerance level
• effect of modalities -
• body part / what injury looks like
• situation/ time of seasons/winning/ losing
• status of player
Handeling acute pain situations & techniques
establish control, Establish helping /collaborative relationship , Alter the concentration, Provide information
sense of humour, Patient / pain education, Distraction/ attention, Visualization (pain modalities), Goal setting (reduce swelling to reduce pain), Relaxation skills
Poole it's chronic pain are Lilly to also be dealing with _______
depression as well
• can have dependency on pain medication
• Depression can result from long term use of pain medication
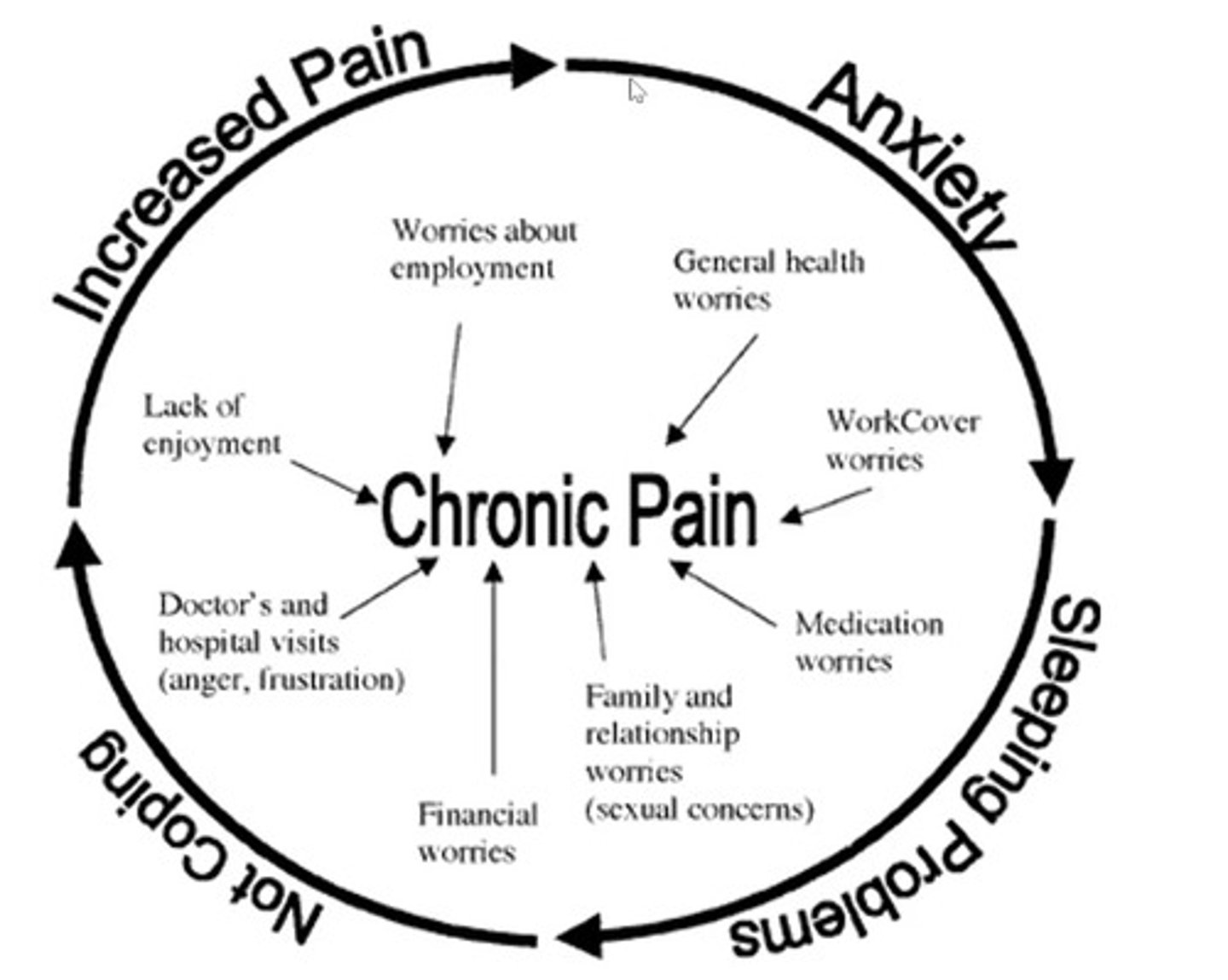
Chronic pain cycle
Increased pain - anxiety - sleeping problems - not coping
(Lack of employment, medication worries, general health worries, work cover worries, relationship worries)