Lab Objectives - Exam 1
1/104
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
105 Terms
Know common devices used to measure PROM
Goniometers
Tape
Inclinometers
Bubble
Digital
CROM & BROM
Athrodial protractors
Goniometers
Plastic, steel, gravity dependent, cheap
They use weighted pointer
MOST COMMONLY USED
Measures almost any joint
Alignment is key
Stationary arm, moveable arm, fulcrum
Read the beginning and end ROM (represents angle created by proximal and distal bones of joint)
May lack good criterion-related validity but excellent reliability
Intra-rater
Peripherial joints
No difference in small vs large
Tape
C7 to S1
Schober technique
Lumbrosacral junction
10 cm above
.90 Correlation coefficient with roentgenograms
Modified Schober Technique
Lumbrosacral junction
10 cm above
5 cm below
.90 Correlation coefficient with roentgenograms
Inclinometer
Accurately measures ROM
Bubble and digital
Fast & small
Repeatable, measuring all joints including composite movement of multiple joints
Active and passive measurements made by one person
More expensive
CROM (cervical)/BROM (back)
Intra-rater .75 to .91
Inter-rater .41 to .88
Measures forward head/ back ROM
Arthodial protractors
Uncommon
Measures device for joint flexibility
Enables quick and accurate testing of ROM in all major joints
Transparent heavy gauge aircraft plexiglass
Large easy to read red and blue degree markings
Accurately measure PROM
Align fulcrum with joint
Stationary arm parallel to proximal segment
Movable arm along distal segment
Stabilize and move passively (outside force, no voluntary muscle contraction, quantity of the motion, quality of endfeel)
Manually
Mechanical (CPM)
Identify procedures to improve reliability
Use preferred position and stabilize proximal joint component
Explain and demonstrate the desired motion to your patient
Move joint passively to complete ROM
Determine end-feel and make a clinical estimate on ROM
Palpate appropriate bony landmarks
Align goniometer’s SA and MA with landmarks
Determine axis of motion
Read and record measurement
Compare to opposite side
Re-measure at the same time of day when your patient returns for their follow-up visit
Successive measurements should be taken by same examiner (same force for end-feel)
Inexperienced examiners should take several measurements
Know how to document goniometric measurements
Be specific and objective
Conicise
Be familar with what is acceptable at clinic
Open-minded for differing opinions
DO NOT USE WITHIN NORMAL LIMITS (age appropriate norms)
Relate to well-known test
Record beginning and ending position using 0-180 degree notation method (use table)
Do not use total joint ROM
Accurately perform isolated MMT of UE/LE/trunk
Follow standard positions, stabilize proximal, apply resistance in line with muscle action
Accurately assign a strength grade using the Lynch/Modified Lovett scale
Grade 0–1: No contraction/trace
Grade 2: Movement in gravity-eliminated
Grade 3: Movement against gravity
Grade 4–5: Movement against gravity + resistance
Identify/eliminate substitutions
Example: During sit-ups, moving arms changes moment arms (shorter → easier, longer → harder). Substitutions change torque demand.
Apply alternate grading scales (calf, hand, trunk)
Trunk: Lawn Chair sit-up progression grading
Calf: Heel raise reps (noted as functional testing in lab discussions)
Hand: Grip/pinch dynamometer (noted in muscle testing alternatives)
Explain basic concepts of osteokinematics
Planes of motion→ axis of rotation→ movements
Sagittal plane→ mediolateral axis → flex/ext
Frontal plane→ anteroposterior axis→ abd/add
Horizontal plane→ vertical axis→ int/ext rotation
Glenohumeral joint
Number of axis = 3
Orientation of axis = mediolateral, vertical, anteroposterior
Location passing through = humeral head
Plane of motion = sagittal, horizontal, sagittal
Movement = flex/ext
Humeroulnar joint
Number of axis = 1
Orientation of axis = mediolateral
Location passing through = medial and lateral epicondyles of humerus
Plane of motion = sagittal
Movement = flex/ext
Radiocarpal joint
Number of axis = 2
Orientation of axis = mediolateral, anteroposterior
Location passing through = head of capitate (may be scaphoid)
Plane of motion = sagittal, frontal
Movement = flex/ext, ulnar/radial deviation
Hip joint
Number of axis = 3
Orientation of axis = mediolateral, vertical, anteroposterior
Location passing through = femoral head
Plane of motion = sagittal, horizontal, frontal
Movement = flex/ext, int/ext rotation, abd/add
Tibiofemoral joint
Number of axis = 2
Orientation of axis = mediolateral (slight deviation), vertical
Location passing through = lateral and medial epicondyles of femur, along the tibia
Plane of motion = sagittal, horizontal
Movement = flex/ext, int/ext rotation
Talocrual joint
Number of axis = 1
Orientation of axis = mediolateral (slight deviation)
Location passing through = talus, or medial and lateral malleoli
Plane of motion = sagittal
Movement = dorsiflexion/plantarflexion (pronation/supination of subtalar joint)
Analyze open vs closed chain
Standing from seated position & straighten the leg while sitting = knee extension
Open chain = straighten leg while sititng
Close chain = stand up from a seated position
Explain arthrokinematics and convex-concave rule
Convex on concave = roll & glide opposite
Concave on convex = roll & glide same
Examples: shoulder (convex humeral head on concave glenoid) vs knee (concave tibia on convex femur).
Convex-on-concave movement
Relatively fixed = concave
Relatively mobile = convex
Movement (roll & glide) = opposite
Concave-on-convex movement
Relatively fixed = convex
Relatively mobile = concave
Movement (roll & glide) = same
Glenohumeral joint in open chain movement
Fixed concave = glenoid fossa
Mobile convex = humeral head
Convex-on-concave
Humeroulnar joint in open chain movement
Fixed convex = trochlea on humerus
Mobile concave = trochlea notch
Concave-on-convex
Wrist radiocarpal joint in open chain movement
Fixed concave = radius distal end
Mobile convex = carpal bones
Convex-on-cave
Hip in open chain movement
Fixed concave = acetabular fossa
Mobile convex = head of the femur
Convex-on-concave
Tibiofemoral joint in open chain movement
Fixed convex = femoral condyles
Mobile concave = tibial condyles
Concave-on-convex
Talocrural joint in open chain movement
Fixed concave = distal end of the tibia and both malleoli
Mobile convex = trochlea and sides of the talus
Convex-on-concave
Glenohumeral flexion
Roll = superior
Slide = inferior (or spin)
Glenohumeral extension
Roll = inferior
Slide = superior (spin)
Glenohumeral internal rotation
Roll = anterior
Slide = posterior
Glenohumeral external rotation
Roll = posterior
Slide = anterior
Glenohumeral abduction
Roll = superior
Slide = inferior
Glenohumeral adduction
Roll = inferior
Slide = superior
Humeroulnar flexion
Roll = anterior
Slide = anterior
Humeroulnar extension
Roll = posterior
Slide = posterior
Radiocarpal flexion
Roll = anterior
Slide = posterior
Radiocarpal extension
Roll = posterior
Slide = anterior
Radiocarpal radial deviation
Roll = lateral
Slide = medial
Radiocarpal ulnar deviation
Roll = medial
Slide = lateral
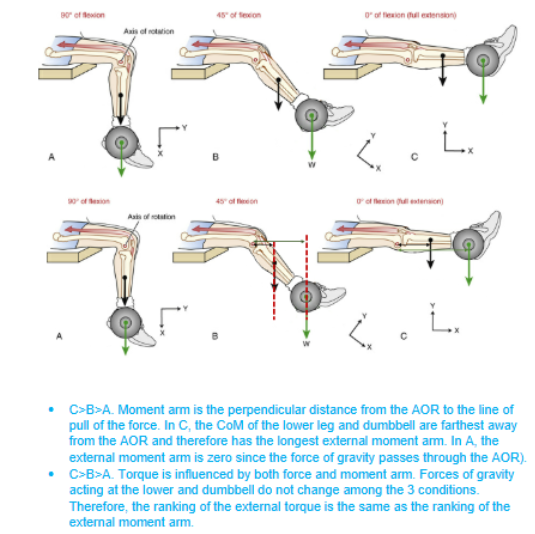
External torque with load (external force & moment arm)
Torque = Force × Moment Arm; gravity acts as external force, perpendicular distance as moment arm
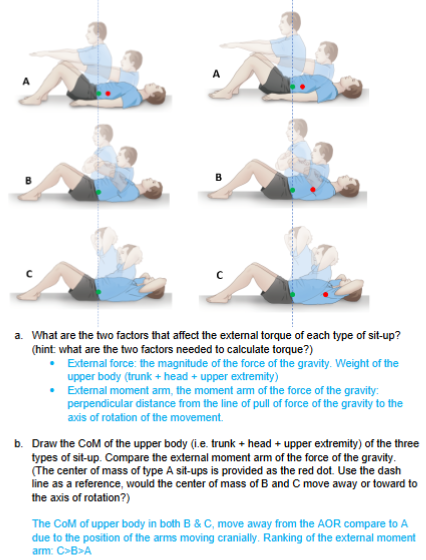
External torque with effort (internal forces & moment arms)
Internal torque = muscle force × internal moment arm; must balance external torque.
Largest external torque, due to longest external moment arm
Internal moment arm does not change among sit-ups
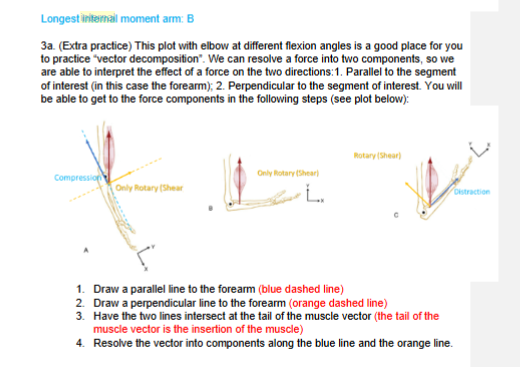
The component vector acting along the parallel line will result in a distraction/compression force (blue vector). How to differentiate whether this component vector will be distraction or compression force?
a. When the arrow head is pointing toward the hand, this component vector is pulling the forearm “away” from the joint center (i.e. AOR) distraction (example: C)
b. When the arrow head is pointing toward the joint center, this
component vector is pulling the forearm “toward” the joint center (i.e. AOR) compression (example: A)
The component vector acting along the perpendicular line will result in a rotary/shear force. (orange vector)
Calculate muscle force using torque equilibrium
Equation: Muscle Force = (External Force × External MA) ÷ Internal MA
Torque = force x moment arm
Internal torque = muscle forces
External torques = body weight or other external forces
Clockwise torque = counter-clockwise torque
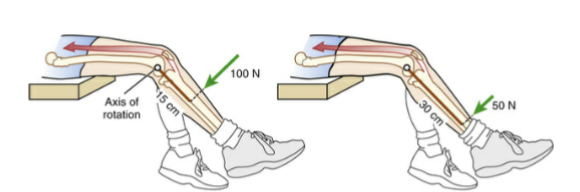
How do you determine the external moment arm & what is moment arm? With 15 Newton-meter, how much force is required from therapist to resist maximal torque production?
Perpendicular distances between the line of pull of force and AOR
EMA = solid brown line (cm)
15 Nm/.15 m (15 cm) =100 N
15Nm/.3 m (30 cm) = 50 N (smaller force)
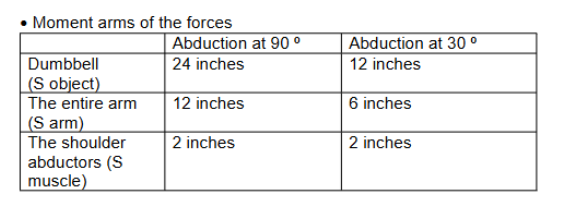
Calculate the muscle forces required by shoulder abductors to hold 4 lb dumbell at 90 degree shoulder abduction.
Weight of arm = 10 lb
Weight of dumbell = 4 lb
Internal torque = external torque
IF x IMA = EF x EMA
IFmuscle x IMAmuscle = EFarm x EMA arm + EFobject x EMAobject
IF x 2 in = 10lbs x 12in + 4lbs x 25 in
IF x 2 in = 216 in/lbs → 108 lbs
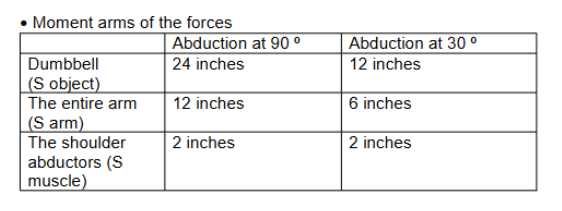
Calculate the muscle forces required by shoulder abductors to hold 4 lb dumbell at 90 degree shoulder abduction.
Weight of arm = 10 lb
Weight of dumbell = 4 lb
Internal torque = external torque
IF x IMA = EF x EMA
IFmuscle x IMAmuscle = EFarm x EMA arm + EFobject x EMAobject
IFmuscle x 2 in = 10 lbs x 6 in + 4lbs x 12 in
IFmuscle x 2 in = 108 in/lbs → 54 lbs
Compared 90 to 30 degrees, which has larger muscle force from the shoulder abductors?
90 degrees
Longer moment arm increases the external torque, which must counteract by generating a greater internal torque
Understand concepts of stability including center of mass and base of support
COM low and in BOS = most stable as force of gravity acts directly through BOS
COM higher and closer to edge of BOS = most mbile as force of gravity is nearly outside the BOS
Whole body COM = S2
Limb loss = COM will move away from loss of limb, superiorly and laterally from S2
Compensate when weight is added or taken away
Apply concepts of stability to assit a patient with stair climbing
Stay below patient (ascending behind, descending in front)
Always have patient where gait belt tightly around smallest part of waist
One hand on belt, other on shoulder to prevent leaning forward
Move one foot at a time to ensure larger BOS and so COM is distributed
Patient moves, then you move
Can ask to hold rail for extra BOS
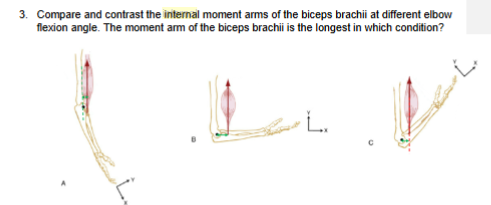
Analyze moment arms at different forearm positions
Biceps brachii has longest MA in supination, reduced in pronation.
Pronation = closer to AOR (short perpendicular distance)
Supination = flexion (bias) maximize MA
Brachialis: constant MA.
Pronation/suppination don’t affect the MA
Pronation (bias) minimize MA
Bony land marks to identify AOR for elbow flexion and extension?
Passes through trochlea and capitulum of humerus
Medial and lateral epicondyle is used to identify
Biceps brachii
O: supraglenoid tubercle (long) & coracoid process (short)
I: radial tuberosity
A: flex elbow, supinate radio-ulnar, flex glenohumeral
Brachialis
O: distal anterior humerus
I: Ulnar tuberosity
A: flex elbow
Brachioradialis
O: lateral supracondylar ridge of humerus
I: styloid process radius
A: flex elbow, pronate/supinate radio-ulnar depends on forearm position
Supinated forearm
Bias biceps brachii
Maximize MA on biceps
20-25% greater elbow flexor torque (increased MA)
Pronated forearm
Bias brachialis
Minimize MA on biceps
No effect on MA of brachialis
Neutral forearm
Bias brachioradialis
Maximize MA of brachioradialis
Analyze torque generation at different elbow positions
Peak torque at ~90° flexion (largest MA + optimal length-tension relationship)
Weaker at full extension/flexion due to smaller MAs
Supinator action
Supinate forearm
Rotates radius to turn palm anteriorly or superiorly if elbow is flexed
Extensor indicis action
Extends 2nd digit
Helps extend hand at wrist
Extensor pollicis longus action
Extends DIP at thumb
Extends MCP
Extends carpometacarpal joints
Pronator quadratus action
Pronates forearm
Deep fibers bind ulna and radius together
Brachioradialis action
Weak flexion of forearm
Maximal flexion when forearm is midpronated
Pronator teres action
Pronate forearm
Flex forearm
Flexor carpi radialis action
Flexes hand
Abducts hand
Palmaris longus action
Flexes hand
Tenses palmar aponeurosis
Biceps brachii action
Both = supinate forearm (most powerful) when supine & flex forearm
Long = weak arm flexor
Short = resists dislocation of shoulder
Review muscle actions
Pronators: pronator teres, pronator quadratus
Supinators: supinator, biceps brachii
Role of triceps brachii when turning a screw
Cancels biceps’ elbow flexion torque during supination, providing stability.
Synergist for vigorus supination and pronation
Attaching to ulna neutralize flexion tendency of biceps with supination task
Biceps and triceps are
Synergists for supination
Antagonists for elbow flexion and extension
Role of anterior deltoid when pushing a door
Synergist
Produces flexion torque that drives the limb forward and neutralizes the shoulder extension of long head of triceps
Review arthrokinematics of pronation & supination
Radius rotates around ulna
Pronation
Proximal RU = radial head rolls anteriorly, slides posteriorly against radial notch of ulna (internal rotation)
Distal RU = distal radius rolls anteriorly and glide anteriorly against the head of ulnar
HR = spin of fovea of radial head against capitulum of humerus
Supination
Proximal RU = radial head rolls posteriorly and glide anteriorly against the radial notch of ulna (external rotation)
Distal RU = distal radius rolls posteriorly and glide posteriorly of the ulnar
HR = spin of fovea of radial head against capitulum of the humerus
Compare the effect of muscle forces of the deltoid at the GH joint
Vector resolved into:
Parallel to humerus: superior shear force → pulls humeral head upward (risk of impingement).
Perpendicular to humerus: abduction torque → initiates and drives GH abduction.
If acting alone: inefficient abduction, superior migration of humeral head, impingement of subacromial structures, poor stability.
Compare the effect of muscle forces of the rotator cuff at the GH joint
Provide compression force → centers humeral head in glenoid.
Provide inferior-directed shear force (especially infra/teres minor/subscapularis) → offsets deltoid’s superior translation.
Assist with fine-tuning rotation (external rotation to clear tubercle under acromion).
Complementary role: Deltoid drives motion; rotator cuff stabilizes and controls arthrokinematics.
Explain scapulohumeral rhythm by describing the osteo- and arthro- kinematics at the glenohumeral joint during arm elevation
First half of elevation (0-90) & second half of elevation (90-180)
Osteo: 60 degrees abduction
Arthro: humeral head rolls superiorly and glides inferiorly
Explain scapulohumeral rhythm by describing the osteo- and arthro- kinematics at the scapulothoracic joint during arm elevation
First half of elevation (0-90) & second half of elevation (90-180)
Osteo: 30 degrees upward rotation (contributed by SC and AC joint)
Arthro: N/A
Explain scapulohumeral rhythm by describing the osteo- and arthro- kinematics at the sternoclavicular joint during arm elevation
First half of elevation (0-90)
Osteo: 20-25 degrees elevation
Arthro: Clavicle rolls superiorly and glides inferiorly
Second half of elevation (90-180)
Osteo: 25 degree posterior rotation (limited elevation)
Arthro: Clavicle spinning on sternum
Explain scapulohumeral rhythm by describing the osteo- and arthro- kinematics at the acromioclavicular joint during arm elevation
First half of elevation (0-90)
Osteo: 5-10 degrees upward rotation
Arthro: N/A
Second half of elevation (90-180)
Osteo: 25-30 degrees upward rotation
Arthro: N/A
What’s the effect of the deltoid muscle force on the joint surface of the GH joint during arm elevation?
a) How do you decide the two axes to resolve your vector into?
One axis will be along (parallel to) the moving segment (humerus in this case)
Other axis will be perpendicular to the humerus.
The two axes will intersect at the insertion of the deltoid (the tail of the vector)
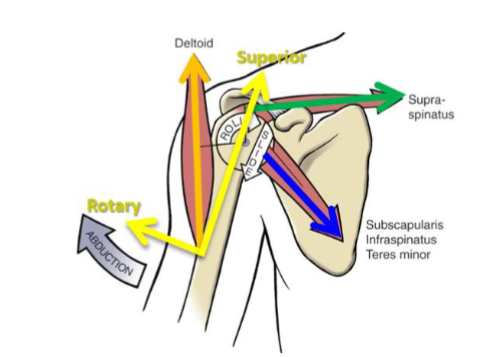
What are the effects of the deltoid muscle force acting at the GH joint on each of the axes you identified in a)?
Parallel to the humerus: pulling the humeral head superiorly (superior shear force)
Perpendicular to the humerus: abduction of the GH joint
What are the consequences if the deltoid is the only muscle activated during shoulder abduction?
If the deltoid is the only muscle activated during shoulder abduction
the movement may be inefficient and potentially harmful.
The deltoid initiates abduction, but without support from other muscles—especially the rotator cuff muscles, the humeral head may migrate superiorly
Leading to impingement of the subacromial structures
Lack of stabilization from the rotator cuff can compromise joint integrity, increasing the risk of shoulder instability or injury
What’s the effect of the supraspinatus (single muscle) and infraspinatus, teres minor and subscapularis (the three combined) acting at the glenohumeral joint during arm elevation (frontal plane only)?
Supraspinatus: Superior roll (abduction) & compression
Subscapularis, infraspinatus, and terest minor: Compression
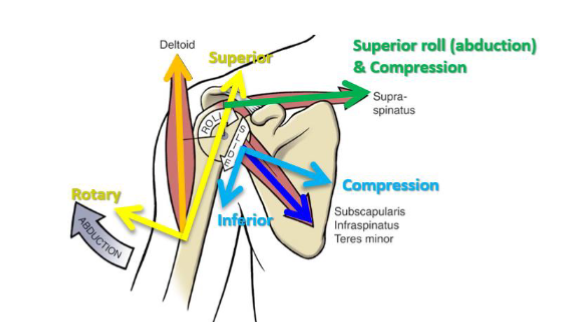
Supraspinatus
Drives the abduction with superior roll of the humeral head
Compresses the humeral head
There is a small superior translation force which is negligible.
In addition, supraspinatus creates a semi-rigid spacer above the humeral head, restricting excessive superior translation of the humerus
Advantage: the superior roll contributes to the abduction of the GH joint, the compression force contributes to joint stability
Infraspinatus, teres minor, and subscapularis
Inferior glide of the humeral head
Compresses the humeral head
Advantage: the Inferior directed force is needed to neutralize the strong superior translation force from deltoid, the compression force contributes to joint stability
Infraspinatus and teres minor
Externally rotate the humerus
Advangtage: the external rotation increases the clearance between the greater tubercle and acromion

Using a TheraBand to represent the muscle force of the anterior deltoid on a skeleton model, are you able to “see” the change of the moment arm when you elevate the arm of the skeleton?
The muscle fiber of the anterior deltoid almost passes through the anterior-posterior axis of rotation
Arm is < 30 degrees of abduction.
As we elevate the arm of the skeleton model, the distal end of the theraband moves superior
The perpendicular distance between the line of pull and AOR increase
How does the changes in the moment arm of the deltoid compare to the supraspinatus?
The moment arm of the deltoid increase from 0-120 degrees of arm abduction.
The moment arm of the suprapinatus stays consistent from 0-120 degrees of arm abduction.
Compare the mechanical advantages between the suprapinatus and the deltoid muscle
Supraspinatus has a greater mechanical advantage at the initial (<30º abduction) or later range (>60º) of abduction
Deltoids has a greater mechanical advantage at the initial (<30º abduction) or later range (>60º) of abduction
What are other movements that occur throughout 0-180 degrees?
Clavicle retracts at SC joint (≈ 15°)
Upwardly rotating scapula posteriorly tiles (≈ 20°)
Less consistently, externally rotates (≈ 10°)
GH joint externally rotates about (≈ 45°)
Locate key anatomical features of the shoulder girdle via palpation and outlining the structures.
Sternum: jugular notch, xiphoid process, sternoclavicular joint.
Clavicle: outline entire clavicle, mark SC and AC joints.
Scapula: outline entire scapula; spine, acromion, AC joint, supraspinous fossa, infraspinous fossa, medial & lateral borders, superior & inferior angles, coracoid process.
Humerus: greater tubercle, lesser tubercle, intertubercular groove.
Postural assessment (partner): look for scapular deviations: elevated/depressed, upward/downward rotation, adducted/abducted (protracted/retracted), tipped/tilted, or winged scapula.
Analyze collective muscle actions at the scapulothoracic joint based on the knowledge of the origins, insertions and line of pull of the muscles
Muscles | Scapular Action |
|---|
a | Upper trapezius + Lower trapezius + Serratus anterior | Upward rotation |
b | Upper trapezius + Middle trapezius + Rhomboids | Retraction + elevation |
c | Rhomboids + Levator scapulae | Downward rotation + elevation + retraction |
d | Lower trapezius + Pectoralis minor | Depression |
Upper trapezius
O: Occipital bone & upper cervical spinous process
I: Lateral clavicle, acromion
A: Upward rotation & elevation of scapula
Middle trapezius
O: Upper thoracic SP
I: Scapular spine
A: Retract scapula
Lower trapezius
O: Lower thoracic SP
I: Medial scapular spine
A: Upward rotate, depress, retract scapula
Serratus anterior
O: Lateral surface of the ribs
I: Medial border scapula
A: protract and upward rotate scapula
Rhomboids
O: Lower cervical SP (minor) & upper thoracic SP (major)
I: Medial border scapula below scapular spine
A: Retract, elevate, downward rotate scapula
Levator scapulae
O: Transverse process of upper cervical
I: Superior angle scapula
A: Elevate & downward rotate scapula