Psychopathology
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
45 Terms
Psychopathology
field of stuy that deals with mental, emotional and behavioural problems
involves research into classification, diagnosis, causation, prevention and treatment of psychological disorders
Statistical Infrequency
satistical norms = any commonly seen behaviours
defines behaviour according to how it's observed
deviation = any unusual behaviour or characteristic that is raely seen is abnormal, behaviour doesn’t fit within the ‘normal distribution
EXAMPLE: intellectual disability disorder, average IQ = 100,
Evaluation of Statistical Infrequency
usual characteristics can be positive
many abnormal characteristics are desirable
e.g. high IQ is statistically abnormal but doesn’t require treatment to return to normal
and some undesirable behaviors are common, like depression
therefore unable to distinguish between desirable and undesirable behaviours using statistical infrequency
issues with labelling
some people may not benefit from being labelled as abnormal
although labelling usually leads to treatment it can have nagtive side effects
e.g. someone with low IQ who is not distressed wouldn’t need a diagnosis of intellectual disability
therefore labelling them as such may damage their self-view and others’ view of them
real life application
in some situations it is appropriate to use a statistical criterion to define abnormality
e.g. it can form a useful part of clinical assessment in diagnosing intellectual disability disorder for those with an IQ two SDs below the mean
helps determine severity of symptoms, but should be used alongside another method (e.g. failure to function adequately)
suggests statistical infrequency is only one of a number of tools to diagnose mental disorders
cut off point is subjective
limitation is cut off points are subjectively determined
if abnormally is defined in terms of statistical infrequency, then we need to decide where to separate normal from abnormal
means that such disagreements are difficult to define abnormality in terms of statistical infrequency
cultural relativism
an issue is that behaviours that are statistically infrequent in one culture may be statistically more frequent in another
e.g. hearing voices in UK is likely to lead to diagnosis of schizophrenia, compared to African countries where this is a common experience
this means that there are no universal standards or rules for labelling a behaviour as normal
Deviation from Social Norms
social norms: ways in which most people behave, established by social groups, varies depending on cultural and historical context
deviation: a behavior different from how society expects people to behave, so behaviour that goes against the unwritten rules of society, antisocial or undesirable behaviour that goes against social norms
Deviation from Social Norms Evaluation
human rights abuses
limitation is in the past some diagnoses were to maintain control over minority ethnic groups and women
e.g. drapetomania was previously listed in the DSM as mental illnesses affecting black slaves who ran away, nymphomania described women attracted to working-class men
nowadays this classification seems ridiculous as our social norms have changed which suggests that perhaps some modern classifications of mental disorders are abuses of people’s rights to be different
desirable vs undesirable disorders
this definition distinguishes between desirable and undesirable behaviour
social deviance definition takes into account the effect the behaviour has on others
definition offers a practical way of identifying undesirable/damaging behaviour which may trigger help from others
context and degree of behaviour
a limitation is that judgements of deviance are often related to the context of the behaviour
e.g. wearing a bikini at the beach vs at school
deviant behaviour is only considered so when it is out of context and behaviour that deviates from social norms isn’t always a sign of mental illness
social deviance on its own cannot offer a complete definition of abnormality as it is related to context and degree
cultural relativism
defining abnormality by social norms is bound by culture as social norms are defined by our culture
cultural norms change between cultures and over time so we must update our ideas of abnormality to fit with them
the DSM-V has been updated to include reference to cultural context in many areas of diagnosis
shows that it is possible to address this issue by including different diagnostic systems
Failure to Function Adequately
failure = unable to cope with everyday life
not contributing to society adequately
criteria for diagnosis:
obsever discomfort
unpredictability
irrationality
dysfunctional behavior
personal distress
maladaptive behaviours
FTFA - Rosenhan & Seligman’s Features of Personal Dysfunction
irrationality = behaviours that cannot be explained in a rational way
violation of moral standards = behaviours that go against society’s moral standards
unpredictability = unexpected behaviours, characterised by loss of control, like committing suicide after failing a test
unconventionality = displaying unconventional behaviours
personal distress = key feature of abnormality includes depression and anxiety disorders
observer discomfort = displaying behaviours which makes others uncomfortable, e.g. hoarding
maladaptive behaviour = behaviours stopping individuals from attaining life goals socially and occupationally
Failure to Function Adequately Evaluation
strengths
recognises the subjective experience of the patient, allowing us to view mental disorder from the perspective of the person experiencing it
easy to judge objectively because we can list behaviours (e.g. dress self, prepare meals)
has practicality and sensitivity as a definition
behaviour may be functional
dysfunctional behaviour can be adaptive and functional for the individual
definiton is incomplete as it fails to distinguish between functional and dysfunctional behaviours
who judges?
someone may be unaware they are not coping or may feel distressed and seek help
or others may judge the behaviour as abnormal
unemployment may due to other circumstances rather than failure to function adequately
limitation of the approach is that judgement is highly subjective
cultural relativism
limited by being culturally relative
defining abnormality according o adequate functioning is related to cultural ideas of how we should live our ives
failue to function adequaltely defintion likely to vary for different cultures as the standard of one culture is being used to measure another
important as it may explain why lower class and non-white patients are more often diagnosed with mental disorders as their lifestyles are different from dominant culture
Deviation from Ideal Mental Health
good mental health = a set of criteria including lack of symptoms, independence, realistic view of the world and good self esteem
deviation = failing to have one of Jahoda’s criteria for good mental health
DIMH - Jahoda’s Criteria for Ideal Mental Health
resisting stress = having self-respect and a positive self concept (coping)
accurate perception of reality = perceiving the world in a non-distorted fway with an objective and realistic view of the world
self-actualisation = experiencing personal growth and development (fulfilment)
environmental mastery = being competent in all aspects of life and able to meet the demands of any situation, having the ability to adapt to life hanging circumstances (interpersonal relationships)
autonomy = being independent, self-reliant and able to make personal decisions (independence)
positive attitude towards oneself = having self-respect and positive self-concept (high self esteem)
Deviation from Ideal Mental Health - Evaluation
positive approach
adopts more positive approach in defining abnormality
focuses on ‘ideal’/desirable behaviours rather than undesirable which has influenced the positive psychology movement
therefore this definitio ahs played an important role in the development of the humanistic approach in psychology
unrealistic criteria
difficult to fill all criteria
some criteria, like environmental mastery is difficult to measure
interesting concept but not very usable when defining abnormality
cultural reltivism
Jahoda’s mental health criteria are culture bound
e.g. self actualisation more relevant to members of individualistic cultures than collectivist cultures
so, if we apply Jahoda’s criteria to those from collectivist cultures, there is likely to be a high incidence of abnormality \
limits generalisability to certain groups
Depresion
DSM-5 Classification
low mood and energy levels
major depressive disorder: severe but often short-term depression
persistent depressive disorder: long-term depression
disruptive mood dysregulation disorder: childhood temper tantrums
premenstrual dysphoric disorder: disruption to mood prior to and/or during menstruation
Characteristics of Depression
Behavioural (actions)
changes to usual activity levels = sufferers have reduced energy levels, causes them to feel lethargic and withdraw from work, education and social life
changes sleep and eating patterns = increase or decrease in appetite and eating, increased or deceased sleep (insomnia or hypersomnia)
possibly aggression or self-harm
Emotional (feelings)
lowered mood
anger
decline in self-esteem
Cognitive (thoughts)
poor concentration
persistent concern: thoughts are biased towards seeing the negative
Physical Symptoms
sick and run down
difficulty sleeping
poor appetite
muscle pains
weight loss
tired
Types of Phobias
specific phobia = fear of an object or situation
social anxiety (social phobia) = fear of social situations
agoraphobia = fear of public places (being trapped)
Phobia Classification
DSM-5 Classification: Specific Phobia
unreasonable, excessive fear triggered by a specific object or situation
immediate anxiety response which is out of proportion to the danger presented
recognition the fear is irrational not required
avoidance or extreme distress
phobia is life limiting as it severely impacts the sufferers personal life
six months or more duration
not caused by another disorder
Phobia Characteristics
Behavioural (actions)
crying
screaming
running away/avoidance
failure to function
endurance
Emotional (feelings)
fear
anxiety
panic
Cognitive (thoughts)
selective attention/reduced cognitive capacity
irrational beliefs
awareness of unreasonable behaviour
cognitive distortions
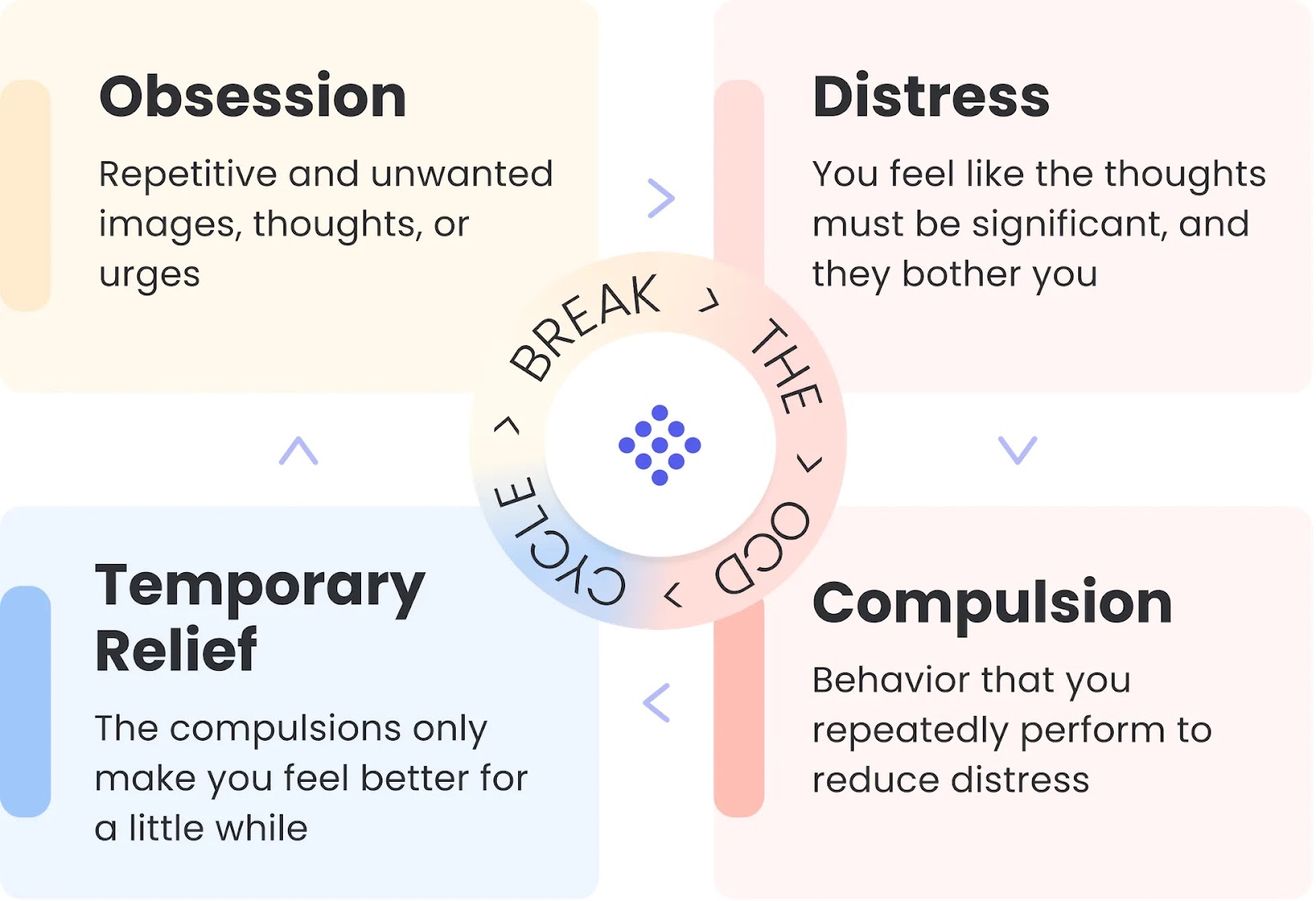
Obsessive-Compulsive Disorder (OCD)
DSM-5 Classification
repetitive behaviour accompanied by obsessive thinking
OCD: obsessions (reoccurring thoughts) and compulsions (repetitive behaviours)
Types of OCD
trichotillomania = compulsive hair pulling
hoarding disorder = compulsive gathering of possessions and the inability to part with anything regardless of its value
excoriation disorder = compulsive skin picking
OCD Characteristics
Behavioural (actions)
compulsions to repeat behaviours usually to reduce anxiety
Emotional (feelings)
anxiety
depression
guilt
Cognitive (thoughts)
recurrent obsessive thoughts accompanied by rituals to cope with the obsession
sufferers understand the irrationality of their perceived unlikely worst case scenario but still unable to control
Explaining Phobias: Behavioural Approach
According to behavioural approach abnormal behaviours caused by:
classical conditioning
operant conditioning
social learning theory
These theories have been applied to a range of psychological disorders, most notably phobias.
Two-Process Model (Mowrer, 1947): explained how phobias are learned through classical conditioning and maintained through operant conditioning
Classical Conditioning
first part of two process model
a phobia is acquired through association
association between a neutral stimulus and unconditioned stimulus will trigger an unconditioned response
e.g.
neutral stimulus = dog = no response
unconditioned stimulus = pain (being bitten)
unconditioned response = fear
dog + pain (being bitten) = fear
conditioned response = fear of dogs
Little Albert
Watson & Raynor (1920) conducted a laboratory experiment to examine whether a fear response could be learned through classical conditioning in humans
participant was an 11 month old child called Little Albert
Watson & Raynor noted he showed no response to various objects, like a white rat
in order to test if they could create a fear response W&R struck a metal bar with a hammer to create a loud noise every time he went to reach for the rat
they did this three times
thereafter when Albert was show the rat he cried
experiment demonstrated a fear response could be induced with classical conditioning in humans
Little Albert also developed fear of similar objects like a Santa Claus beard which showed how he had generalised his fear to other objects
Operant Conditioning
although classical conditioning explains why we develop our phobias it doesn’t explain why they don’t just decay over time and how they are maintained
according to operant conditioning phobias can be negatively reinforced, this is where a behaviour is strengthened, because an unpleasant consequence is removed
negative reinforcement = avoiding phobic stimulus reduces fear and results in desirable consequences
Social Learning Theory
not part of the two process model but is a neo-behaviourist explanation
phobias may also be acquired through the modelling of the behaviour from others
e.g. seeing a parent respond to a dog with extremem fear may lead a child to acquire a similar behaviour because the behaviour appears rewarding (i.e. fearful person gets attention)
Evaluation Explaining Phobias Behaviourist Approach
Research Support
Watson & Raynor (1920) demonstrated the process of classical conditioning in the formation of phobias in Little Albert, who was conditioned to fear white rats
supports the idea that classical conditioning is involved in acquiring phobias
Application
behaviourist approach can be applied to therapy
behaviourist ideas been used to develop effective treatments including systematic desensitisation and flooding
systematic desensitisation helps people unlearn their fears using the principles of classical conditioning
flooding prevents people from avoiding their phobias and stops the negative reinforcement from taking place
Importance of Classical Conditioning
two-process model supported by people recalling when their phobia appeared
however, not everyone with a phobia can recall such traumatic incidents
Sue et al. suggests different phobias may be the result of different processes
demonstrates the role of classical conditioning in developing phobias, but other processes may be involved in their maintenance (e.g. agoraphobics a specific incident, arachnophobes learned through modelling)
Incomplete Explanation for Phobias
although operant and classical conditoing are involved in the development an maintenance of phobias, there are some aspects of phobic behaviour that require further explaining
we have biologial preparedness to easily acquire phobias of things hat were a danger to our evoloutionary past (e.g. snakes, heights)
shows that the two-process model cannot account for biological preparedness which explains why we develop phobias of some stimuli and not others as there is more to acquiring phobias than simple conditioning
doesn’t take into account other factors
Alternative Explanations for Avoidance
in more complex behaviour like agoraphobia avoidance behaviour may be motivated by positive feelings of safety
this explains why some agoraphobics can leave their house with a friend with relatively little anxiety
problem as the two process model suggests avoidance is motivated by anxiety reduction rather than seeking safety
Ignores Cognitive Factors
behaviourist explanation been criticised for being too simple and reductionist
behaviourist approach ignores role of cognition in the formation of phobias and cognitive psychologists suggests that phobias develop as a result of irrational thinking not just learning
e.g. claustrophobics may think I am going to get trapped in this space and die which is an irrational thought
cognition approach also led to the development of congitive behavioural therapy (CBT), a treatment which is said to be more successful than the behaviourist treatments
Systematic Desensitisation
behavioural therapy combining relaxation and gradual exposure to the phobic stimulus
important that patient remains relaxed a all times through relaxation techniques like deep muscle or progressive relaxation
anxiety hierarchy constructed from least to most. frightening
counterconditioning replaces anxiety with relaxation for the phobic stimulus
reciprocal inhibition impossible to be afraid and relaxed at the same time
Evaluation of Systematic Desensitisation
Effective Treatment
a strength of SD is that it is effective in treating specific phobias
Gilroy et al 2003 found successful treatment of spider phobia using SD compared to control group treated by relaxation without exposure up to 33 months following treatment
shows SD is helpful in reducing the anxiety in spider phobia and that effects are long lasting
Suitable for Diverse Range of Patients
compared to alternative treatments SD is suitable for diverse range of patients
e.g. flooding not suitable for children and those with learning difficulties as they may not fully understand what is happening (can’t give informed consent) during flooding or engage in the reflective aspects of CBT
Preferred Over Flooding
patients often choose SD over flooding as it causes less trauma
patients may also find talking with therapist during SD to be pleasant
reflected in the low drop out rates (attrition) for SD compared to flooding
Not Appropriate for all Phobias
may not be effective in treating all phobias
Ohman (1975) suggests SD may be less effective in treating ‘ancient phobias’ with an evolutionary element and or effective in treating those acquired through personal experience
suggests SD can only b used effectively in tackling some phobias, not all
may only work in therapy situation and not useful in real world
relies on participant’s ability to create a vivid mental image which some are not able to do so, ineffective for those who can’t
Flooding
immediately exposing the patient to their phobic stimulus
longer sessions required, but only one may be needed
eliminates avoidance behaviour and extinguishes the phobic response untilt hey are calm and fear is reduced
traumatic experience so patient needs to be well prepared
uses principles of operant conditioning
Evaluation Flooding
Cost Effective
can be an effective treatment fro those who stick with it and relatively quick compared to SD
Choy at al 2007 found both SD and flooding to be effective, but flooding was more effective in treating phobias
Traumatic Experience
highly traumatic experience so not suitable for every patient
although patients fully consent to the therapy there is a high drop out rate which ultimately reduces its effectiviness
individual differences in responding to looding limit the effectiveness of the therapy in the treatment of phobias
Limited Effectiveness
although flooding is highly effective in treating simple phobias it. is less effective for complex phobias like social phobia
may be due to the cognitive aspect of social phobias
this type of phobia may benefit from more cognitive therapies like CBT that tackle irrational thinking
Depression
DSM recognises these categories of depression:
major depressive disorder = short term but severe periods of low mood
persistent depressive disorder = long term or recurring depression
disruptive mood regulation disorder = childhood temper tantrums
premenstrual dysphoric disorder = disruption to mood before and/or during
bipolar depression = extreme mood swings, including periods of mania (high energy and elevated mood) and periods of depression (low energy and sadness).
unipolar depression = persistent and intense feeling of sadness or a lack of interest in external activities
Explaining Depression: Cognitive Approach
teaches that individuals who suffer from mental disorders have distorted and irrational thinking - which may cause maladaptive behaviour
it is the way you think about the problem rather than the problem itself which causes the mental disorder
individuals can overcome mental disorders by learning to use more appropriate cognitions, if people think in more positive ways they can be helped to feel better
focues on an individual’s negative thoughts, irrational beliefs and misinterpretations of events as being the cause of depression
2 main theories as to how faulty cognitions cause depression:
Beck’s Negative Triad
Ellis’ ABC Model
Beck’s Theory
Explains vulnerability to depression in cognitive terms
faulty information processing = selective attention to the negative aspects of situations, black and white thinking
negative self schemas = affects how we interpret any new information
negative tried = 3 kinds of automatic negative thinking world, self, future
Beck’s Negative Triad

Beck’s Negative Triad
Cognitive Biases/Faulty Information Processing
Beck believed that people who are depressed make fundamental errors in logic
Beck proposed that depressed people tend to selectively attend to the negative aspects of a situation and ignore the positive aspects
tendency to blow small prob;ems out of proportion with thinking in terms of black and white and ignoring the middle ground
they are prone to distorting and misinterpreting information, a process known as cognitive bias
two types of cognitive bias include:
over-generalisation = make a sweeping conclusion based on a single incident
catastrophising = exaggerating a minor setback and believing it’s a complete disaster
Negative Self Schemas
a schema is a building block of knowledge, a ‘package of ideas and information that has developed with experience
self-schema is a package o ideas that we have about outre;ves
people who have become depressed have developed negative-self schemas and therefore they interpret all information about themselves in a negative way, which may lead to cognitive bias
these schemas may come from negative experiences, like criticism
Weissman and Beck (1978)
AIM: to investigate the thought process of depressed people to establish if they use negative schemas
PROCEDURE: thought processes were measured using dysfunctional attitude scale (DAS). participants were asked to fill in a questionnaire by ticking whether they agreed or disagreed with a set of statements.
FINDINGS: depressed particiapants amde more negative assesmentsthan non-depressed people. when given some therapy to challenge and change their negative schemas there was an improvement in their self-ratings
CONCLUSION: depression involves the use of negative schemas
Negative Triad
Beck built on the idea of maladaptive responses and suggested that people with depression become trapped in a cycle of negative thoughts
they have a tendency to view themselves, the world and the future in pessimistic ways - the triad of impairments
cognitive biases and negative self schemas maintain the negative triad, a negative and irrational view ourselves, our future an the world.
for sufferers of depression, these thoughts occur automatically and are symptomatic of depressed people
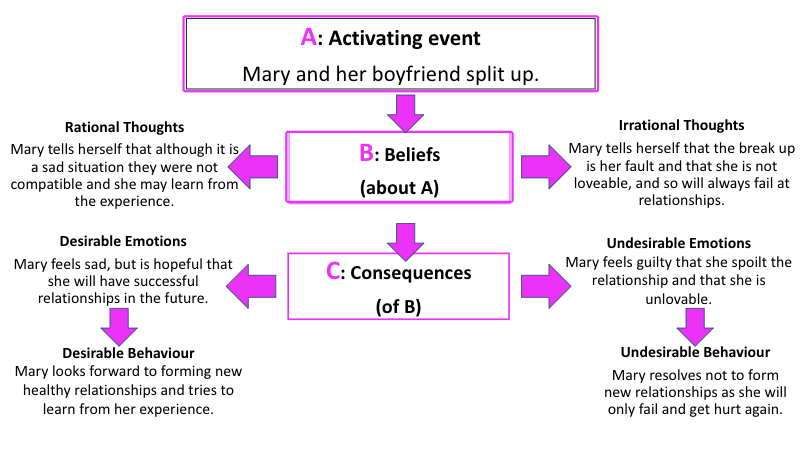
Ellis’ Theory
the ABC model = irrational beliefs make us overreact to events and get depressed
A-Activating Event = a negative life event
B-Beliefs = irrational interpretations of A make us overreact to the life event
C-Consequences = emotional and behavioural outcome is depression
Ellis’ ABC Model
ellis proposed that good mental health is a result of rational thinking
ellis argued that there are common irrational beliefs that underlie much depression and sufferers have based their lives on these beliefs
ellis argued that the source of irrational beliefs lies in musturbatory thinking = certain ideas or assumptions must be true in order for an individual to be happy, ellis identified the three most important irrational beliefs
i must be approved of or accepted by people i find important
i must do well or very well, or i am worthless
the world must give me happiness, or i will die
Evaluation Ellis’ Theory
Partial Explanation
ellis’ model only describes reactive depression triggered by life events
not all depression has an ‘activating event’ and can arise without an obvious cause
Practical Application
led to succesful therapy (REBT)
challenging irrational negative beliefs reduces depression and supports the model
Lipskey et al (1980) found a correlation between difference in beliefs and changes in emotional distress
Doesn’t Explain all Aspects of Depression
doesn’t explain anger, hallucinations and delusions that some patients experience
Evaluation Beck’s Model
Supporting Evidence
view that depression is linked to irrational thinking is supported by research, Hammen and Krantz 1976 found that depressed participants made more errors in logic when asked to interpret written material than non-depressed participants
Grazioli & Terry (2000) found pregnant women high in cognitive vulnerability were more likely to suffer PND
Clark & Beck (1999) found evidence of cognitive vulnerabilities before depression developed
Practical Application
explanation forms the basis of CBT (cognitive behavioural therapy) - a successful therapy
all cognitive elements (negative triad) of depression are identified and challenged by the therapist
Incomplete Explanation
doesn’t explain all elements of depression which is complex and has other symptoms e.g. anger, hallucinations, bizarra beliefs
Overall Evaluation
Narrow Explanation
doesn’t take into account biological or genetic factors and so is reductionist
Blames the Patient
overlooks situational factors which could be key, like major life events
Cause and Effects is Unclear
unlcear which comes first, develop negative way of thinking due to depression or depression due to negative thinking
Not all Irrational Beliefs are Irrational
Alloy and Abrahamson (1979) found that depressed people gave more accurate estimates of likelihood of disaster than normal control participants
A + A proposed that depressed people are actually realists and see things how they really are
Alternative Explanations
the biological approach to understanding mental disorders suggests that genes and neurotransmitters may cause depression
the success of drug therapies for treating depression suggest that neurotransmitters do play an important role; the medication alters the levels of specific neurotransmitters and reduces the symptoms
diathesis-stress approach suggests that people with genetic vulnerability for depression are more prone to the effects of living in a negative environment which then leads to negative irrational thinking
Treating Depression - CBT
CBT most common psychological treatment for depression
method for treating mental disorders based on both cognitive and behavioural techniques
therapist aims to make the client aware of the relationship between thought, emotion and action
it is a way of talking (psychotherapy) about:
thoughts on self and other people
how actions effect your thoughts and feelings
from cognitive view therapy aims to change the way someone thinks, challenging negative thoughts
therapy also includes behavioural techniques like behavioural activation with encourages patients to engage in activities they were avoiding, and coping mechanisms which therapists use role play to imagine acting out in real life
when these parts of the sequence are clearly outlined and understood they can be changes so CBT helps break the cycle of maladaptive thinking, feelings and behaviour
Cognitive Approach to Treating Depression
Cognitive-Behaviour Therapy (CBT)
most commonly used treatment for depression
combines. cognitive and behavioural techniques
cognitive element:
assessment - client and therapist identify problems and set goals
plan is put in place
identify negative and irrational thoughts
behavioural element:
work to change unhelpful thought patterns and put more effective behaviours in place
other key elements
homework: clients are asked to complete assignments between therapy sessions
behavioural activation: encourage patient to be more active and engage in enjoyable activities
unconditional positive read: non-judgemental relationship between client and therapist, therapist provides respect and appreciation regardless of what the client says and does
Beck’s CBT:
identifies the negative triad
challenges negative thoughts
homework set to record positive experiences to use in therapy to demonstrate reality
client assessed to discover the severity of their condition
therapist will establish a baseline prior to treatment to help monitor improvement
identify the negative triad and make client aware of the relationship between thought and emotion
challenging negative thoughts by making clients aware of them, then replacing them with more optimistic and rational beliefs through process of reality testing
Ellis’ CBT Rational Emotive Behaviour Therapy (REBT):
talking therapy that extends the ABC model
identifies and disputes irrational thoughts (rational confrontation)
replaces them with more effective ones
results in new feelings being produced
REBT is based on the premise that whenever we become upset it is not the events taking place in our ,ives that upset us; it is the beliefs that we hold that cause us to become depressed
Ellis believed that irrational beliefs make impossible demands of the individual, leading to anxiety
central technique of REBT is to identify amd dispute patient’s irrational negative thoughts. Ellis identified 3 different types of disputing:
logical disputing: “does this thinking make sense?” client’s self defeating beliefs don’t logically follow the information available
empirical disputing: “is there proof to support this belief? client’s self defeating beliefs are not consistent with reality
pragmatic disputing: “how useful is this belief?” self defeating beliefs are not useful
Newark et al 1973
AIM: to discover if people with psychological problems had irrational attitudes
METHOD: two groups of participants were asked if they agreed with the following statements identified by Ellis as irrational:
a) it is essential that one be loved or approved by virtually everyone in the community
b) one must be perfectly competent, adequate and achieving in order to consider oneself worthwhile
one group consisted of people with diagnosed anxiety. the other group has no psychological problems, defined as normal
RESULT: total of 65% of the anxious participants agreed with statement a) compared to 2% of non-anxious participants. b) 80% of anxious participants agreed, compared to 25% of non-anxious participants
CONCLUSION: people with emotional prolems think in irrational ways
CBT Evaluation
STRENGTHS
effective in reducing symptoms and in preventing relapse
John March et al (2007) found CBT to be as effective as drugs in treating depression
compared CBT and drugs alone then together
327 adolescents, after 36 weeks 80% CBT, 80% drugs and 85% for both significantly improved
showed CBT to be as effective as drugs and more so when use alongside
CBT first choice for treatment for depression in NHS
clients learn to understand themselves and use skills learned in new situations
patient can take active role in their recovery
WEAKNESSES
CBT may not work in severe cases as patient may be unmotivated and unfocused during sessions to deal with cognitive demand of CBT, may need drugs first to keep them focused and alert, limitation of CBT as cannot be sole treatment for depression in all cases
over emphasis on cognition, minimises importance of individual’s real life circumstances
CBT focuses on here and now but some patients may have issues in their past they want to discuss, therefore find the present-focused approach frustrating and unhelpful
doesn’t take into account social circumstances, not all depression stems from irrational beliefs or one specific activating event, but rather prolonged poor environment e.g. domestic abuse, CBT ineffective at treating these patients
Rosenzweig (1936) suggested small differences between therapies mean success isn’t determined by technique but rather quality of relationship with therapist
CBT takes longer than drugs and is more expensive, higher attrition rates
Economic Implications of CBT
when people g to work more is contributed to the economy through taxes but when people don’t. go to work less tax is paid
less time of work due to illness means less sick pay paid by employer
absence from work costs the economy roughly £15 billion a year, most of this due to mild struggles with mental illness
improvements in psychological health/treatment programmes mean people manage their health better, less likely to relapse and take less time off work which reduces cost to the economy
influential scientific research findings may increase investment from overseas companies into the UK, boosting the economy
individuals who are happier are more productive
providing effective treatments could be a financial burden to the NHS