Cranial Nerves
1/248
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
249 Terms
Eye motions are controlled by
CN III, CN IV, CN VI
medial rectus muscle
adduction, nasal direction, towards middle
lateral rectus muscle
abduction, moves eye laterally
superior rectus muscle
elevates eye
inferior rectus
depressor down
superior oblique
depression and intorsion
intorsion of the eye
upper pole of the eye is rotated towards the nose (superior muscles)
extorsion of the eye
upper pole of the eye is rotated away from the nose (inferior muscles)
CN III eye movements use what muscles
superior rectus
inferior rectus
medial rectus
inferior oblique
CN IV eye movements use what muscles
superior oblique
CN VI eye movements use what muscles
lateral rectus
superior and inferior oblique are most efficient when eye is?
Adducted
Parasympathetic nucleus of cranial nerve III
Edinger-Westphal Nucleus
Three clinical tests of eye movement are commonly used in diagnosis of eye movement disorders. The three most common tests evaluate
• the position of the eyes at rest
• the ability to move the eyes up, down, in and out on command
• the ability to follow an object with the eyes when the object is moved in each of the four directions (tracking).
Three clinical tests of eye movement are commonly used in diagnosis of eye movement disorders. The three most common tests evaluate:
• the position of the eyes at rest
• the ability to move the eyes up, down, in and out on command
• the ability to follow an object with the eyes when the object is moved in each of the four directions (tracking)
Using these three tests, what deficits would result from damage to CN III?
At rest, The eye would be down and out
Difficulties when CN III is damaged
Adduction of the eye (medial)
Elevation of the eye
Depression of the eye
If CN III signs are seen on the right side but not the left, would the lesion more likely involve the nuclei of CN III or the third nerve?
Involve the nerve because the nuclei of the two sides are so close together that they both are likely to be damaged by a CNS lesion
After loss of the parasympathetic functions of CN III, resulting from damage to the Edinger-Westphal nucleus, identify three expected findings (symptoms) that would be observed?
-The pupil would be dilated because of loss of tone in the constrictor muscles
-There would be a loss of the pupillary light reflex because light causes pupillary constriction by parasympathetic activation via CN III
-The lens would remain elliptical and there would be loss of accommodation (ability to focus on near objects).
Ptosis
dropping of eyelid (CN III)
Levator Palpebrae
Muscle that elevates eyelid (VN III)
Accommodation of lens
Describes the changes in shape of the lens to allow for near and far vision
Extorsion
Rotation the eye so the top moves laterally
Ciliary Muscles
Muscles that relax tension on the lens and cause the lens to be more spherical (see closer up)
Strabismus
Deviation of eye from normal position
Diplopia
Double vision (mismatching images from left and right eye)
Mydriasis
Dilated Pupil
CN IV is the only nerve to
exit dorsally and contralaterally from the brainstem and exclusively innervate a contralateral structure (superior oblique)
True or false: The right nucleus of CN IV supplies the left IO.
FALSE (SO)
True or False: The left CN IV supplies the right SO.
FALSE
True or False: The left CN IV supplies the right SO.
TRUE
True or False: The right CN IV supplies the right IO.
FALSE
True or False: Damage to the R. nucleus of IV produces intorsion of the left eye
FALSE, extorsion
True or false: Damage to the L. CN IV produces down and out deviation on the left.
FALSE
True or False: Damage to the L. nucleus of IV produces upward deviation of the R. eye.
TRUE
CN IV damage produces extorsion on the ______ side
same
The left Nucleus of CN IV produces upward deviation of the _____ side
opposite
True or false: Damage to the right CN IX produces extorsion of the right eye
True
Superior Oblique (intorsion vs extorsion)
In group: Intorsion
Inferior Oblique (intorsion vs extorsion)
Out group: Extorsion
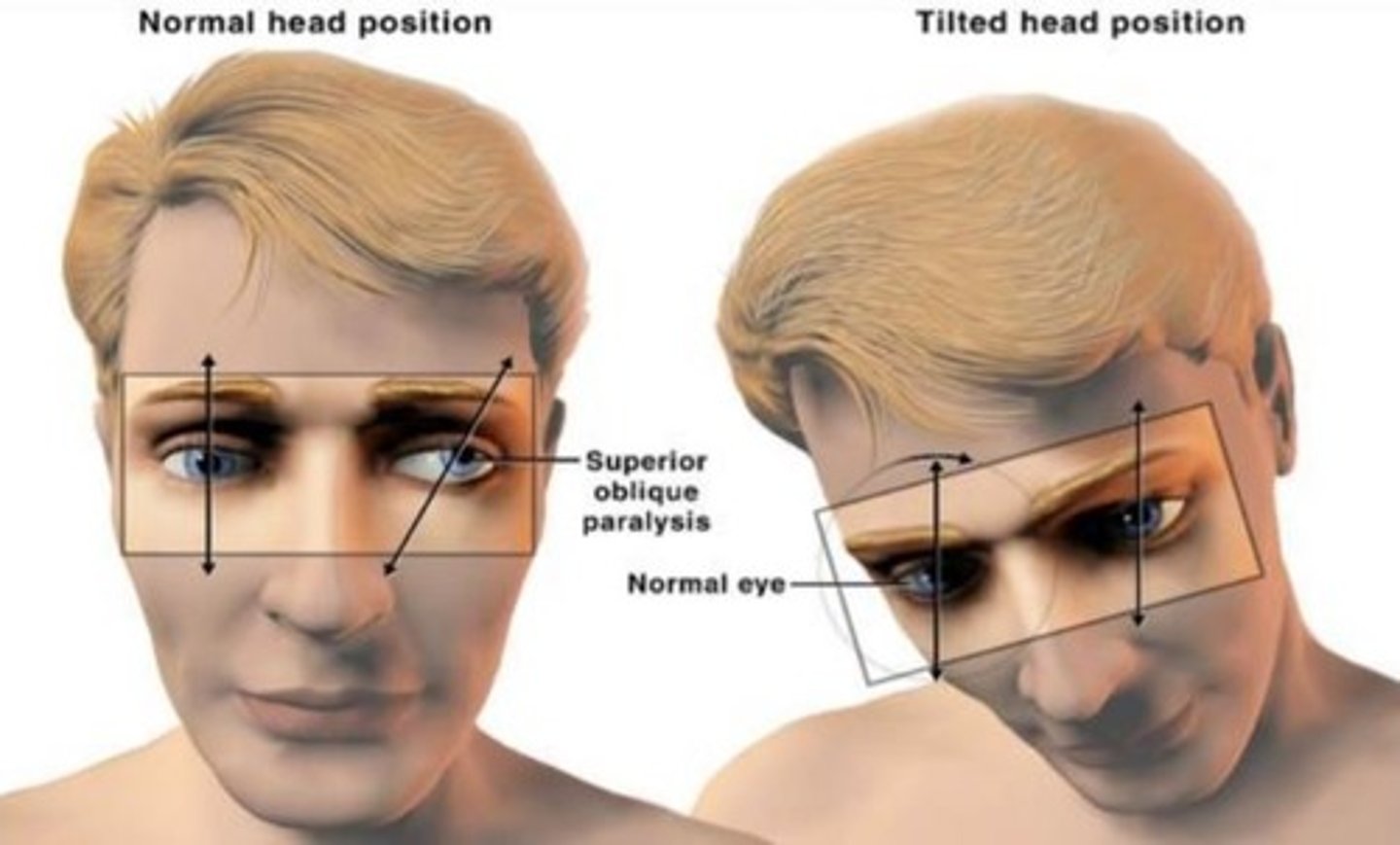
A patient presents with symptoms that you immediately recognize as indicative of left CN IV damage. You are cued by the way the patient carries her head. In order to get rid of diplopia resulting from the left SO paralysis, the head is tilted to align the two eyes. This is a difficult question, but see if you can figure it out. The diagram above (Figure 15) holds a few clues.
The head is titled to the ____ because ____
The head is tilted the side opposite of the affected eye because the normal head compensates for the head tilt
Function of CN VI (abducens)
Movement of the eye laterally by contraction of the ipsilateral LR muscles
What are the three nuclei of CN VII
Motor Nucleus
Salivatory Nucleus
Nucleus Solitarius
Innervation pattern of eye muscles mnemonic
LR6-SO4-ALO3
Lateral rectus CN 6, Superior Oblique CN 4, All others CN 3
Saccades
abruptly changing fixation point of eye
Volitional Saccades
Under conscious control from the frontal lobe
Reflexive Saccades
Unconscious superior colliculi
Smooth Pursuit
slow tracking allowing an object to be in central vision
paramedian pontine reticular formation
CN VI sends axons to the same side then crosses in the contralateral medial longitudinal fasciculus to synapse on cells of CN III to move the contralateral eye
Both eyes will rotate right
Internuclear opthalmoplegia
damage to the MLF, cannot tract inward however because cranial nerve 6 remains in tact they can move the eye nasally to focus on a near object
multiple sclerosis
Deviation of the eye at rest: down and out
CN III (means that the eyes cannot go in and up if this is injured)
Deviation of the eye at rest: up
CN IV
Deviation of the eye at rest: in
CN VI
Inability to move the eyes: Down when adducted
CN IV
Inability to move the eyes: Up or In
CN III
Inability to move the eyes: out
CN VI
Identify the eye muscle that produces movement in each of the following directions: Down when adducted
SO
Identify the eye muscle that produces movement in each of the following directions: up when abducted
SR
Identify the eye muscle that produces movement in each of the following directions: in
MR
Identify the eye muscle that produces movement in each of the following directions: up when adducted
IO
Identify the eye muscle that produces movement in each of the following directions: down when abducted
IR
Identify the eye muscle that produces movement in each of the following directions: out
LR
Two patients have paralysis of the right LR muscle. In patient A the right CN VI has been severed; the damage to patient B is at the nucleus of CN VI, including the paramedian pontine reticular formation. How would you tell the difference between these two patients with a simple clinical test?
a. Both patients will show deviation of the right eye nasally at rest (strabismus). And, when asked to converge the eyes to focus on a point near the nose, the left eye of both patients will look in towards the nose.
b. If patient A is asked to look to the right, the left eye will move nasally, but the right eye will not move temporally.
c. If patient B is asked to look to the right, neither eye will move. This is because the involvement of the PPRF nucleus interrupts the circuit for conjugate lateral deviation
d. If the lesion has spared the nuclei of CN VI but involved the MLFs between CNs III and VI, neither eye would deviate at rest, but neither eye would move nasally when the patient is asked to make conjugate lateral eye movements to the right and left side. However, the eyes would move nasally to focus on an object near the nose (like when reading). This is called internuclear ophthalmoplegia (INO). Remember that eye movement problems will often be bilateral because of the close proximity to the midline of the nuclei of CNs III, IV and VI, and the MLF. If all the eye muscles are involved, the lesion is probably peripheral, where CNs III, IV and VI run together (e.g., the cavernous sinus or superior orbital fissure).
The pretectal area of the midbrain receives visual afferents that originate
in the retina and pass through the optic nerve
sphincter muscle controls
pupil size
ciliary muscle
allows the lens to round and focus the eye for near vision
the LGN (is / isn't) a necessary relay for the retinotectal system
ISN'T
Parasympathetic pupil constriction
AFFERENT (Towards to brain from the eye)
signal comes down optic nerve, through optic chiasma, along optic tract, and to the pretectal nucleus
then sent to edinger-westphal nucleus
Parasympathetic pupil constriction EFFERENT (from the brain to the eye)
Signal from EWN travels along oculomotor nerve, through ciliary ganglion, to the iris sphincter and ciliary muscle causing the pupil to constrict
Which of the following characterize input to the pretectal nuclei?
a. involves both eyes
b. both direct from retinae and relayed from contralateral pretectal nucleus c. travels in part through posterior commissure
d. travels in part through anterior commissure
e. relays through lateral geniculate body
f. directly synapses onto CN III neurons
involves both eyes
both direct from retinae and relayed from contralateral pretectal nucleus
travels in part through posterior commissure
Which of the following characterize output to the pretectal nuclei?
a. involves both eyes
b. both direct from retinae and relayed from contralateral pretectal nucleus c. travels in part through posterior commissure
d. travels in part through anterior commissure
e. relays through lateral geniculate body
f. directly synapses onto CN III neurons
involves both eyes
travels in part through posterior commissure
directly synapses onto CN III Neurons
Direct light reflex
effects on eye illuminated
Consensual Light Reflex
Affects other eye
Describe the near Triad ( what must happen for you to accomplish near vision)
convergence of the eyes
contraction of ciliary muscle produces tension on lens allowing focusing on closer objects ( makes lens rounder) - accommodation
constriction of pupil bilaterally
Argyll Robertson Pupil
Small bilateral pupils, constrict very poorly to light
will not react but will accommodate to near stimuli
Associated with CNS syphilis
damage to pretectal nuclei will impair
the consensual light reflex induced to either eye
Horner's Syndrome
Mitosis (pupil constriction)
Ptosis (eye drop)
Anihidrosis (loss of sweating on that side)
Stimulating the edge of the cornea with saline/cotton will produce
ipsi and contralateral corneal reflex in intact trigerminal sensation
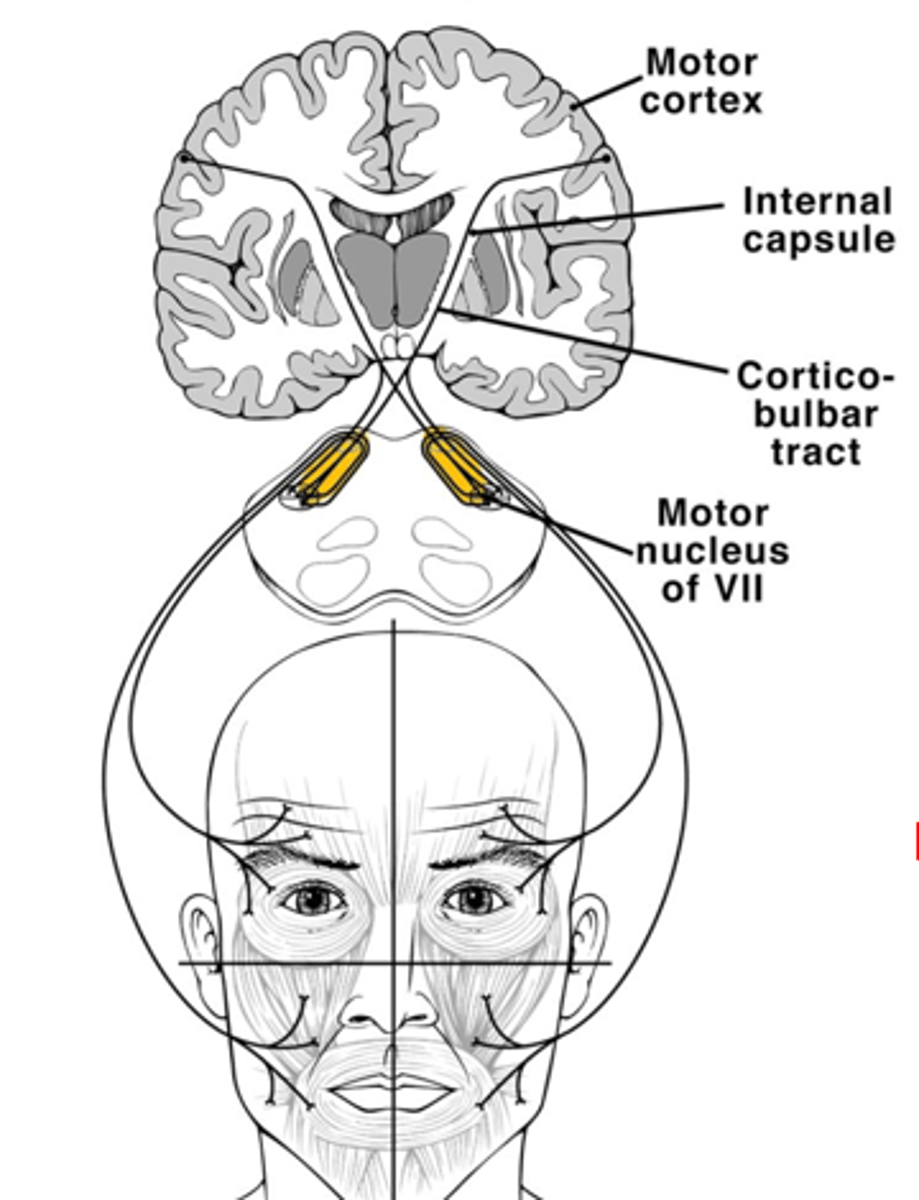
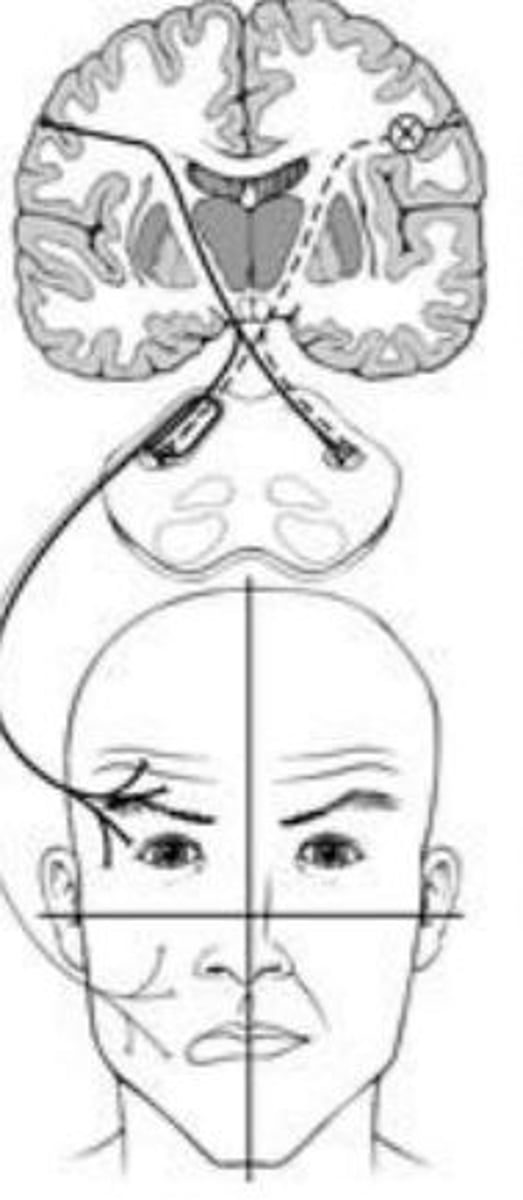
Upper motor lesion CN VII (facial) causes what
Spare the eyebrow but cause contralateral smile droop (impacts lower part of face on opposite side)
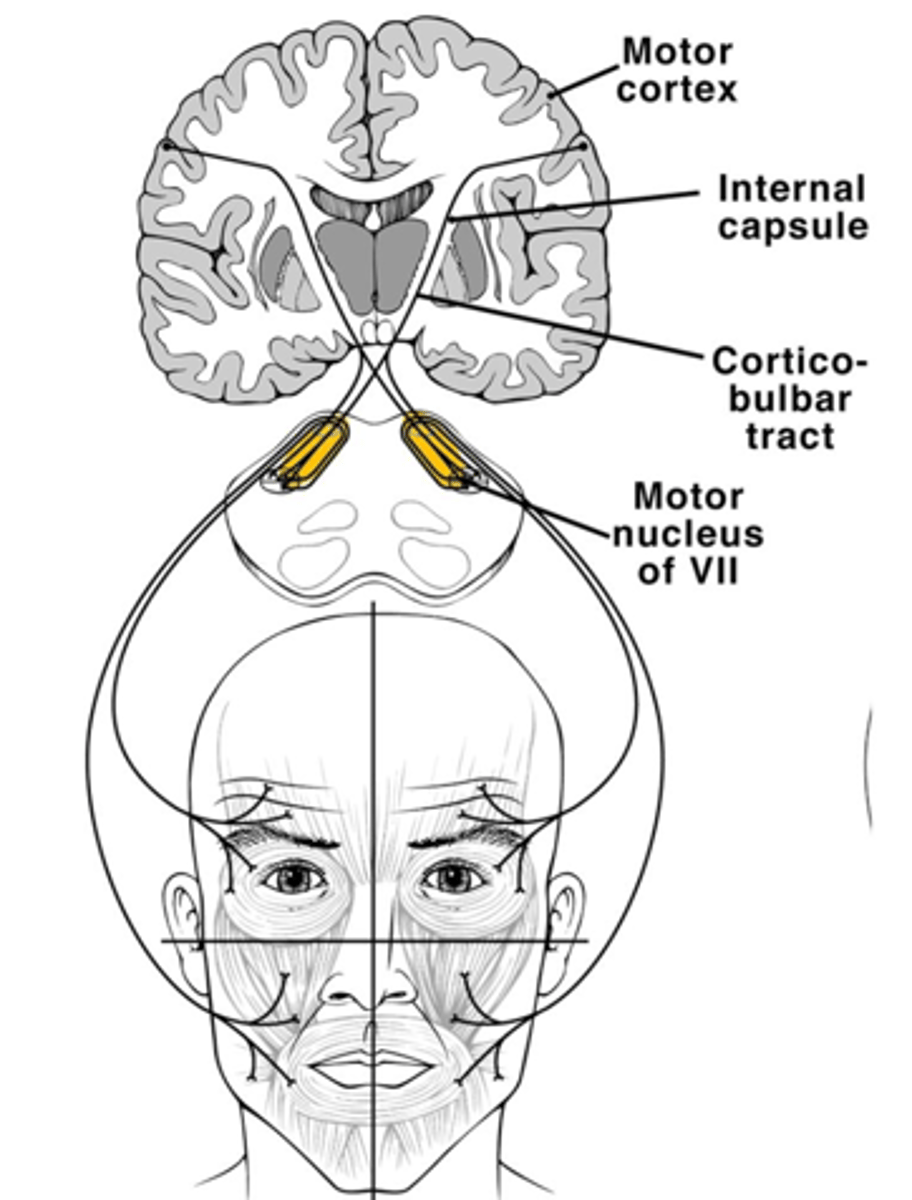
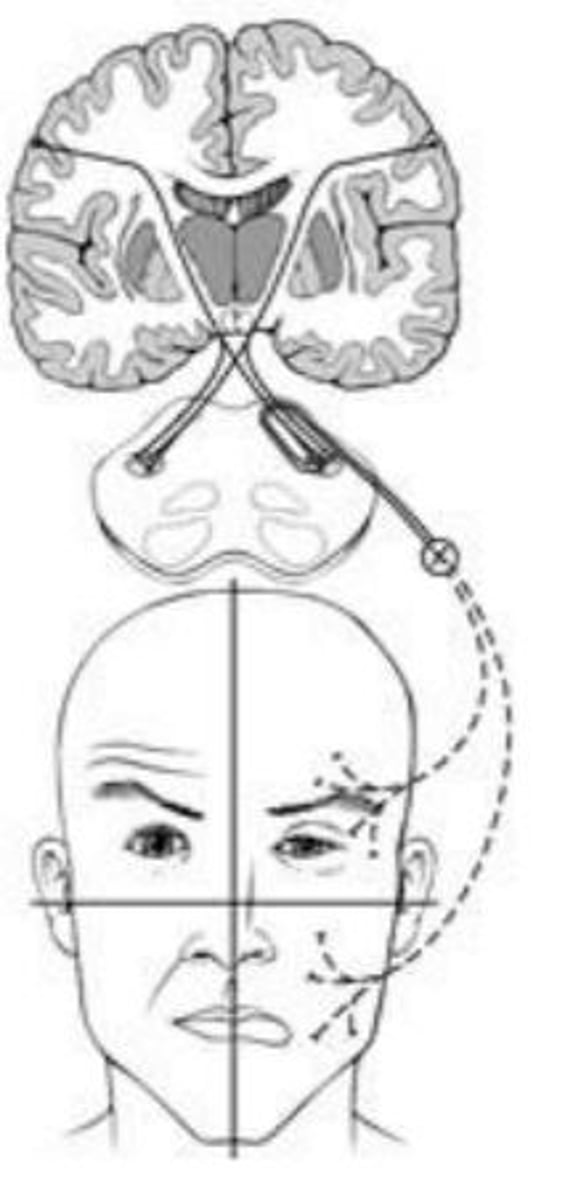
Lower motor lesion CN VII (facial) causes what
weakness of eyebrow and smile on the same side
If a patient who has left facial weakness had a cortical stroke which vessel is likely the cause?
right middle cerebral artery
If a patient has left facial weakness what cranial nerve and location is it at?
Left pons
what side does the uvula go for glossopharyngeal (CN IX)
goes to the side that still has an intact lower motor pathway, goes to unaffected side of lower motor lesion
nucleus solitarius
pain temperature and touch from pharynx and posterior tongue
back 1/3 of tongue
Blood pressure
9th cranial nerve
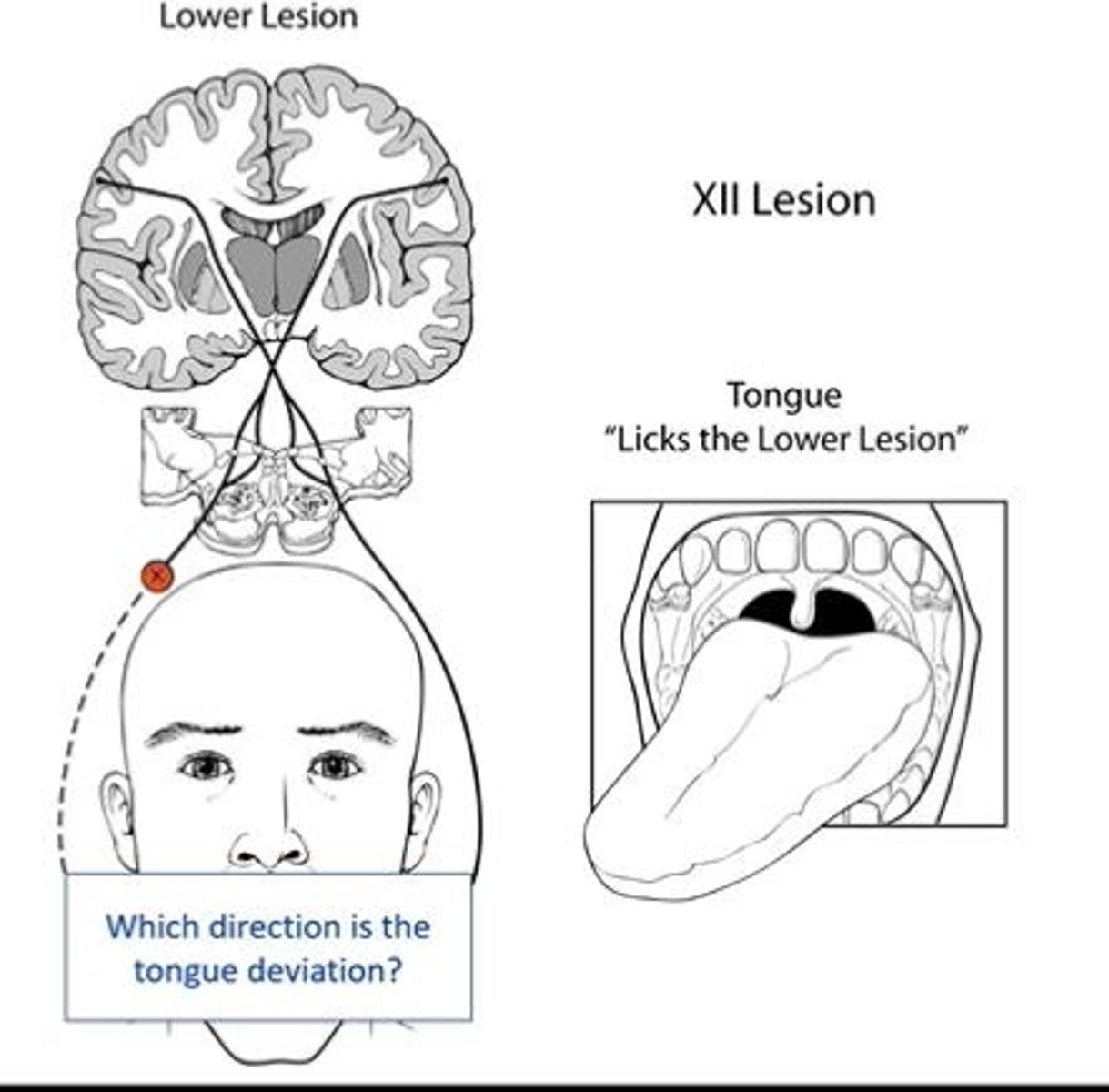
CNXII Lower motor lesion
lick the lower lesion, goes to weak side
CN XII Upper lesion
Will go to the opposite side of the lesion (will not lick the lower)
What side will the tongue go for CN XII upper lesion?
Opposite side as upper lesion
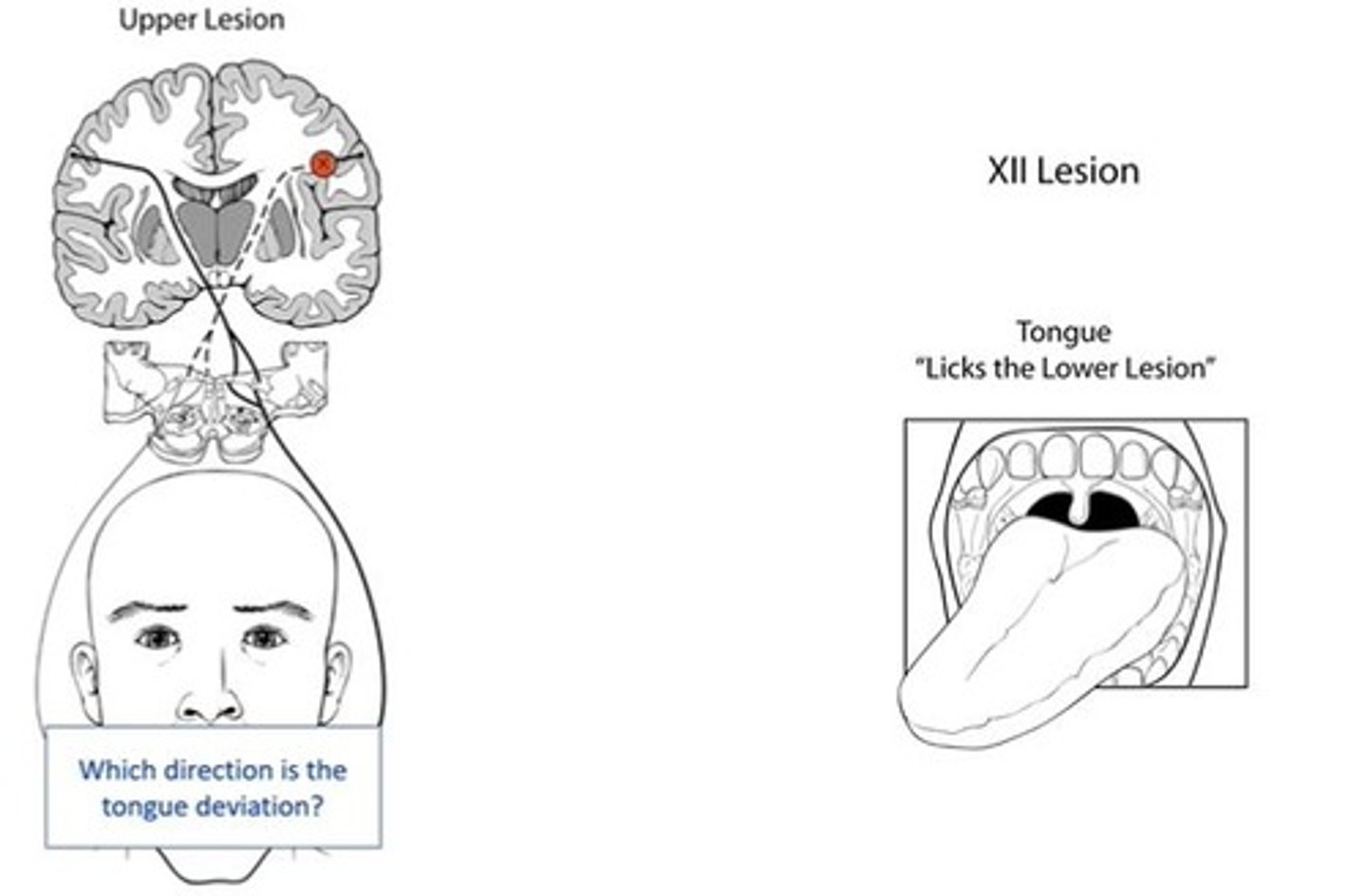
What side will the tongue go for CN XII lower lesion?
To the side of the lesion ("licks lower lesion")
The patient with a lesion distal to the lateral pons will most likely exhibit?
Ipsilateral smile droop and ipsilateral upper facial weakness
(eyebrow is supplied by both right and left so that is why cortex supplies both left and right
What do they usually test in neuro for different functions?
pupillary light, corneal, cough, and gag
afferent and efferent for midbrain pons and medulla
Upper motor lesion for CN VII (PONS, facial nerve)
opposite side smile droop
Lower motor lesion CN VII (PONS, facial nerve)
Ipsilateral smile AND facial weakness IMPACTS THE EYEBROW
remember: cortex
contralateral
your patient has difficulty maintaining a patent airway and is unable to lift their head off the bead; which is the most likely cause
Medullary infarct involving CN X and XI causing bulbar weakness
Which of the following structures participate in both the direct and consensual light reflex
Optic Nerve
Optic Chiasm
Optic Tract
Pretectal Area
Edinger-Westphal nucleus
CN III
Pupillary Sphincter
What nerves monitors the consensual reflex to the eye?
CN V (Trigeminal) sensing touch on the cornea
CN VII (Facial) motor response inducing the eyelid to close
What are the symptoms for a CN VII (facial) lower motor lesion?
eye and mouth are dropping
What are the symptoms for a CN VII (facial) uppermotor lesion?
only the mouth is dropping, since it is from the top the eyebrows are controlled
ipsilateral means
same side
contralateral
opposite side
Name the nucleus of CN VII: Submandibular Gland
Salivatory Nucleus