Men’s Health Pharmacology
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
72 Terms
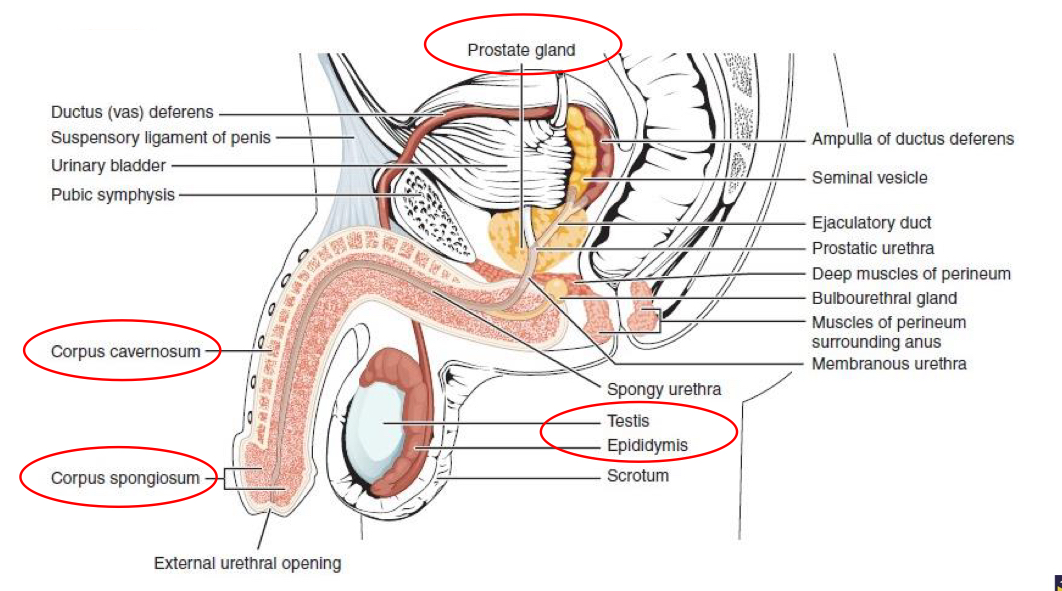
What is a diagram showing anatomy of the male reproduction system?
What are Leydig cells?
Adjacent to tubules
What are Leydig cells responsible for?
Androgen secretion, LH also targets cells and stimulates testosterone secretion
Where does testosterone go after secreted from Leydig cells?
Moves into tubule lumen
What are Sertoli cells?
Form part of the tubules, tight junctions between cells in blood testis barrier
What is the role of Sertoli cells?
Developing spermatocytes, FSH targets Sertoli cells and spermatogonia
What can happen if the blood testis barrier is damaged?
Autoimmune attack can occur directed at the sperm, infertility can be the result
What is a diagram showing Leydig cells and Sertoli cells?

What are the main testosterone targets?
Developing gametes
Muscle
Primary and secondary sexual characters
The brain
What is a diagram showing the pituitary testis axis?
Hypothalamus releases GnRH
Acts on gonadotrophs in anterior pituitary
Negative feedback initiates from Sertoli cells where they release inhibin - inhibits FSH secretion by AP
Testosterone inhibits GnRH secretion by hypothalamus and decreases pituitary sensitivity to GnRH
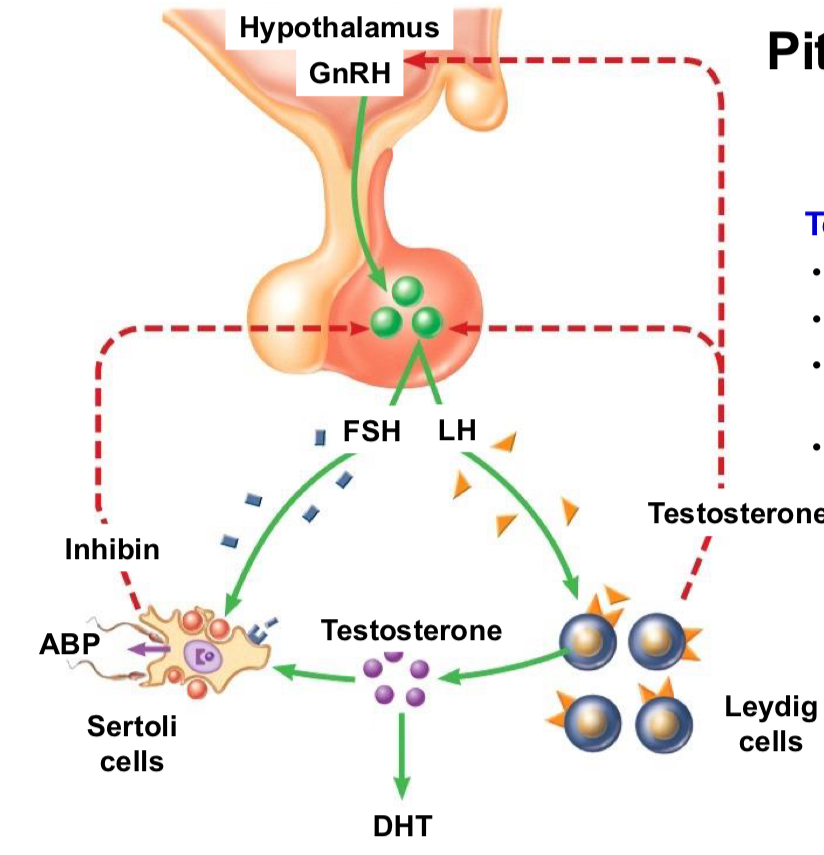
What does FSH produce when acting on Sertoli cells?
Inhibin and ABP (androgen binding protein)
Why are ABPs needed?
Allows androgens to bind as they are not soluble enough to cross membranes
What can testosterone be converted to?
DHT
Why is DHT preferred over testosterone?
10x higher efficacy than testosterone
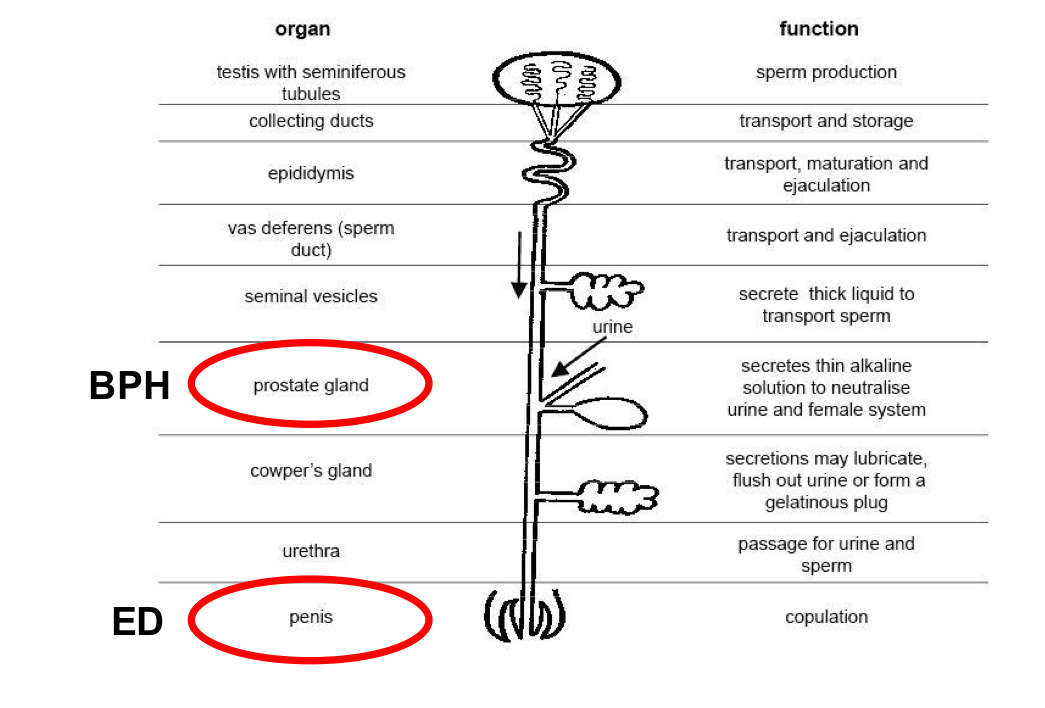
What is a diagram showing anatomy of the male reproduction system highlighting ED and BPH?
How do the haemodynamics of an erection work?
Flaccid penis - smooth muscle is contracted of arteriolar and arterial walls an allows a small amount of blood flow
When stimulated - smooth muscles of cavernous arteries relax and causes dilation - corporal tissues become engorged with blood
Engorgement causes corporal tissues to swell and erects the penis - pressure 90-100mmHg
Engorged corporal tissue compressses veins and venules and prevents blood outflow
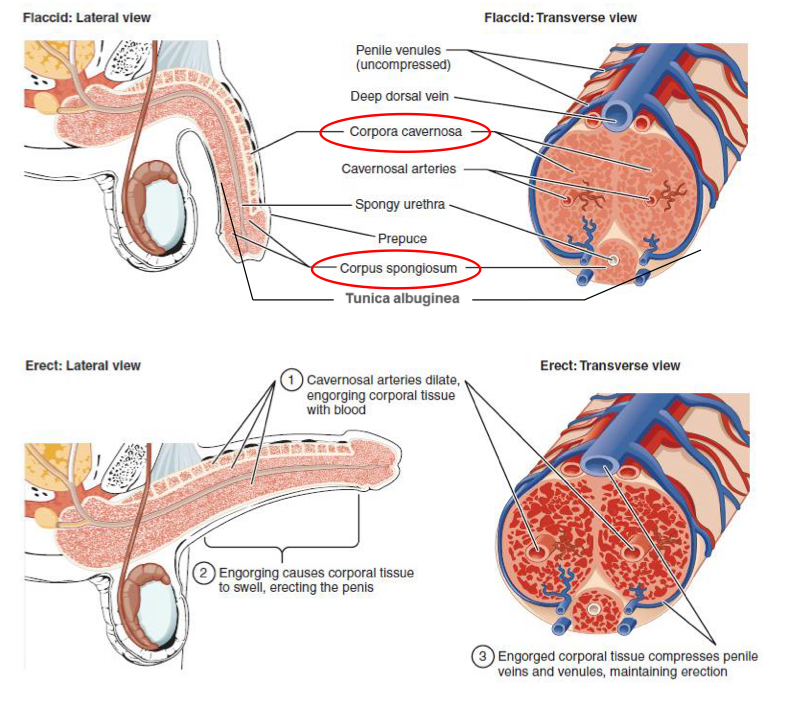
What is the result of the engorged corporal tissue from an erection on pressure?
Increased cavemosal pressure, increased pressure in corpus spongiosum and maintains erection
How does stimulation lead to erection in central neural activation?
Perceptual/cognitive = stimulus arousing, emotional/motivation - appropriate time for arousal? Physiological leafdds to switch on machinery/autonomic outflow
What nerves innervate the penis?
Sympathetic, parasympathetic - somatic and sensory innervation
How do receptors activate the penis from stimulation?
Penile mechanoreceptors activated, initiates erection via a spinal reflex but not usually sustained and instead balanced between contractant and relaxant transmitters
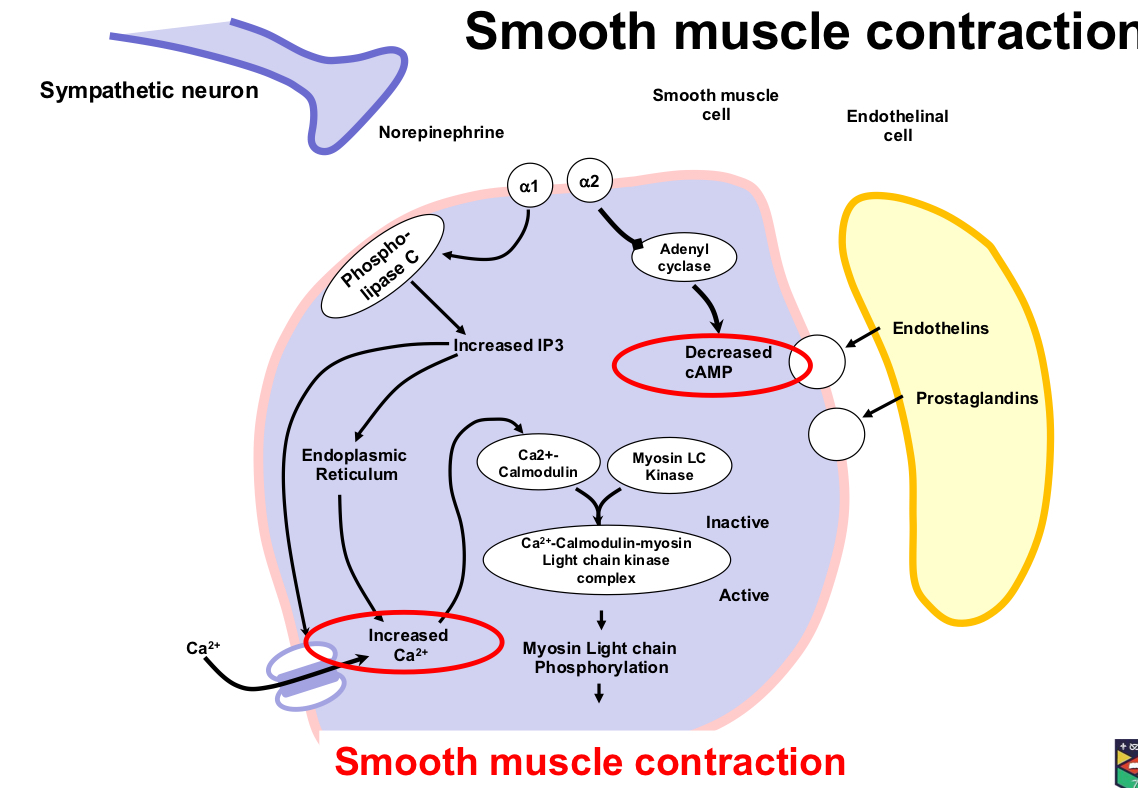
How does smooth muscle contraction work before an erection?
norepinephrine acts on the smooth muscle cell
Adenyl cyclase is activated which decreases cAMP level
Phospholipase C increases IP3 and increases calcium release which leads to myosin chain phosphorylation and smooth muscle contraction
How does smooth muscle relaxation work to cause an erection?
Acetylcholine decreases sympathetic activation
AcH works on eNOS, which sends nitric oxide to the cell
This activates guanyl cyclase which works to decrease Calcium
Prostaglandin e1, at the same time, acts on adenylyl cyclase to increase cAMP
What can the causes of male erectile dysfunction be?
Psychogenic - exaggerated inhibitory responses or excessive sympathetic outflow
Neurogenic - nerve damage in brain, spinal cord or nerves innervating penis e.g., spinal cord injury, Parkinson’s, iatrogenic damage
Arteriogenic causes
Venogenic changes
What subcategory of ED are psychogenic and neurogenic?
Failure to initiate
What subcategory of ED causes are arteriogenic and venogenic?
Failure to fill and store
What are the 2 classes for reasons for ED?
Failure to initiate
Failure to fill and store
What are the risk factors for ED and also atherosclerosis?
Hypertension, hyperlipidemia, smoking, diabetes are all risk factors for atherosclerosis and ED
What are arteriogenic causes of ED?
Atherosclerotic processes reduce arterial flow and perfusion pressure in cavernous sinusoids - insufficient penile engorgement to reach full-erection phase and therefore to initiate rigid-erection phase
What is the mechanism for how arteriogenic causes cause ED?
Reduced elasticity of vessel walls in sinusoids, increased vasoconstriction, impaired endothelial NO
What are venogenic causes for ED?
Failure of adequate venous occlusion following cavernosal engorgement - prevents transition to rigid-erection phase and reduces maintenance of erection
What hormone targets Leydig cells?
LH
What hormone targets Sertoli cells?
FSH
Where do PDE5 inhibitors work?
PDE5
Where does alprostadil work?
Prostaglandin PGE1
How is alprostadil administered?
Intracarvenosal injection or urethral suppository - local application to minimise side effects
What are the ADRs of alprostadil?
Priapism (prolonged erection), penis deformation
What counselling should be provided for alprostadil?
Condoms should only be used when taking this drug if the partner is pregnant if using the suppository formulation
What are the side effects of alprostadil?
Hypotension, anticoagulant effects, penile and other localised pain
What are the interactions of alprostadil?
Can potentially enhance hypotensive effects with antihypertensive drugs
What are some examples of phosphodiesterase 5 inhibitors?
Sildenafil, vardenafil and tadalafil
How do PDE5 inhibitors work?
Maintains high levels of cGMP and decreases calcium ion levels
What is the PK of PDE5 inhibitors?
Metabolised by Cyp3A4 - tadalafil has a longer half life, once daily rather than PRN
What are the CI of PDE5 inhibitors?
Patients taking nitrates or history of non-arteritic anterior ischaemic optic neuropathy or those where vasodilation is inadvisable
What are the cautions for PDE5 inhibitors?
CVS disease, those taking alpha-blockers and antiarrhythmics
What are the interactions for PDE5 inhibitors?
Potent CYP3A4 inhibitors, can cause 5x+ increase in AUC and can cause large increase in exposure e.g., grapefruit
What are the 2 approaches to dealing with ED?
Pharmacological - pathways that are penis specific e.g., NO-cGMP pathway or pharmaceutical - means to limit exposure of other organs e.g., PGE1
What is the aetiology of BPH?
Increases as age increases
What does pharmacotherapy for BPH focus on?
Stopping disease progression and symptom relief
What is BPH?
Benign prostatic hyperplasia
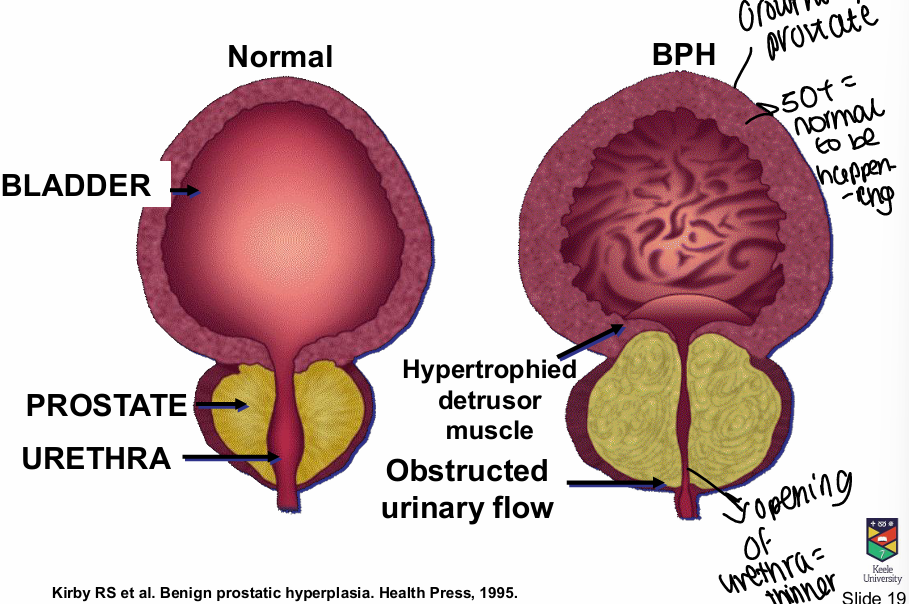
What is the pathophysiology of the bladder/prostate in BPH?
Growth of prostate/bladder thicken, hypertrophied detrusor muscle, urethra opening is thinner
What is the histology of BPH?
Stromoglandular hyperplasia
What can BPH be associated with?
Presence of lower urinary tract symptoms (LUTS), anatomical - enlargement of gland (BPE), pathophysiologic compression or urethra and compromises urinary flow (BOO) - but all separate conditions also
What is BOO?
Bladder outlet obstruction - urethra compression and urinary flow compromised
Are BPH and LUTS the same?
No - both can occur simultaneously
What is BPE?
Benign prostatic enlargement - subset of BPH
How is BPH treatment success measured?
Less symptoms, less bother and increased QOL, decrease prostate size/growth stopped, increase in peak flow rate/relieve obstruction, prevent long term outcomes, acceptable adverse events profile
How do a1 adrenergic blockers work?
Relax smooth muscle in the prostate producing an increase in urinary flow rate - no effect on prostate size
What are some examples of a1 adrenergic blockers?
Tamsulosin, alfuzosin, doxazosin, indoramin, pazosin, terazosin
What is the PK of a1 adrenergic blockers?
Well absorbed after oral admin and work quickly
What are the CI of a1 adrenergic blockers?
Pts with history of postural hypotension and micturition syncope
What are the cautions of a1 adrenergic blockers?
Drowsiness, hypotension and syncope/fainting
How do 5a reductase inhibitors work?
Prevent conversion of circulating testosterone to more potent DHT
What are examples of 5a-reductase inhibitors?
Finasteride and dutasteride
What is the onset of benefits from 5a reductase inhibitors?
Slow - months to reduce prostate size and symptom relief
What are the safety warnings around handling 5a reductase inhibitors?
Women of childbearing potential should avoid handling, men taking should use condoms if partner is likely to become pregnant due to potential birth defects
What are some side effects of 5a reductase inhibitors?
Reduced libido, impotence and breast tenderness
What typical therapy is used for BPH?
Combination therapy of 5a reductase inhibitors to stop disease progression and alpha blockers to relieve symptoms rapidly
What type of disease is prostate cancer?
Androgen dependant disease in initial phase
How does an GnRH antagonist work?
Competes for receptor binding with endogenous GnRH and shuts whole pathway down
How do GnRH agonists work?
Initial increase in gondatropin secretion, followed 2-3 weeks later by marked inhibition due to desensitised GnRH receptor - suppresses LH and FSH
What are examples of available GnRH agonists?
Leuprolide, goserelin, triptorelin
What are examples of GnRH antagonists?
Abarelix, degarelix