pmcol 200 final
1/162
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
163 Terms
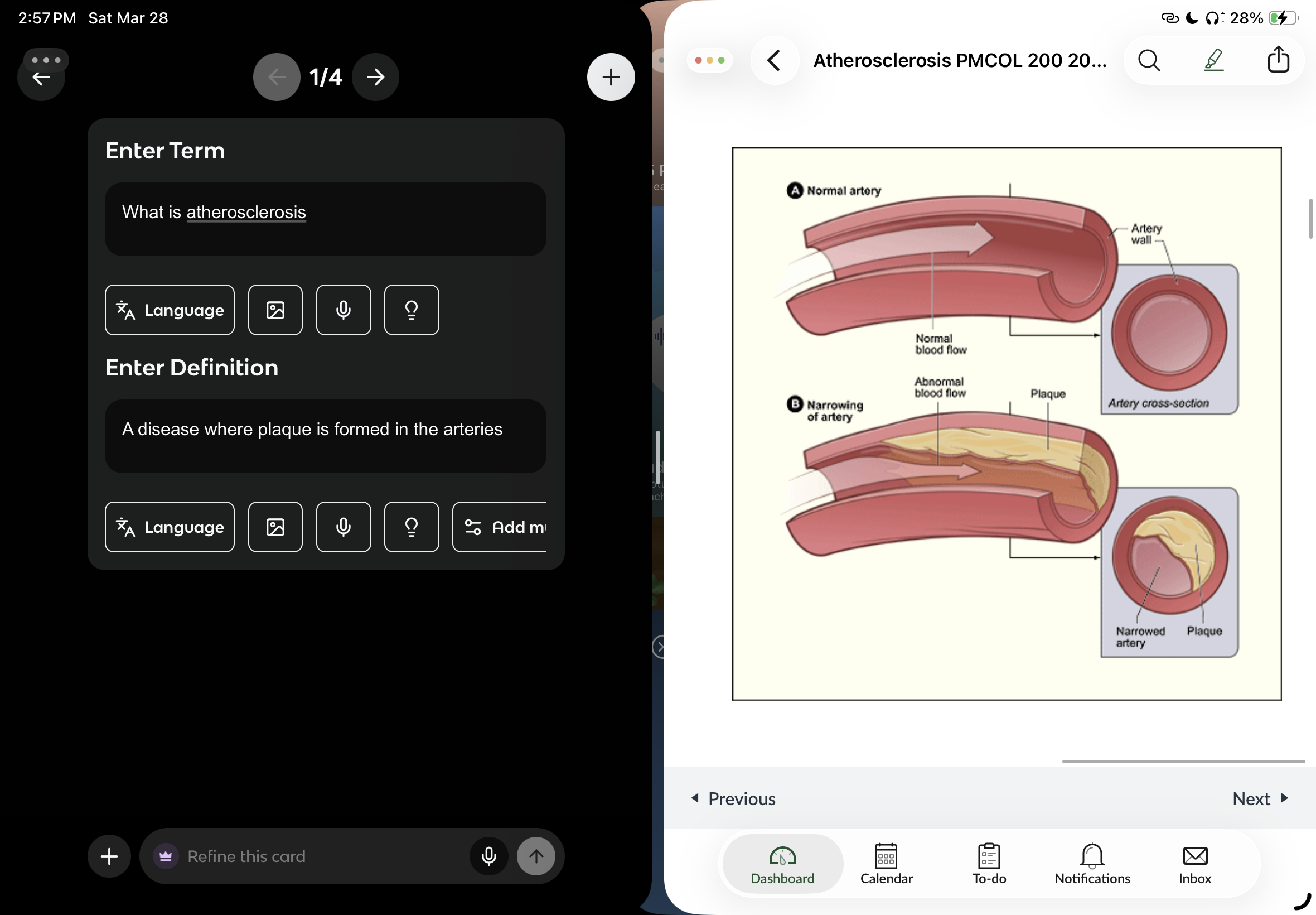
What is atherosclerosis
A disease where plaque is formed in the arteries (reduced blood flow to organs) + plaque dislodgement and flow to other locations
Why atherosclerosis only in arteries and not veins
Because they experience higher pressure
Clinical manifestations of atherosclerosis (5)
Coronary artery disease (heart attacks)
Carotid artery disease (stoke) brain
Peripheral artery disease (intermittent claudication)
Renal artery stenosis (chronic kidney disease)
Mesenteric artery ischemia (abdominal pain)
What are the risk factors of atherosclerosis
Metabolic: modifiable + non-modifiable
Lifestyle + environmental: modifiable
What causes plaque development
Lipids (LDL-C MAJORRR, cholesterol, triglycerides)
Blood clots after plaque formation
Inflammation
What is the main approach to reducing atheroscelrotic cardiovascular disease
Lowering LDL-C
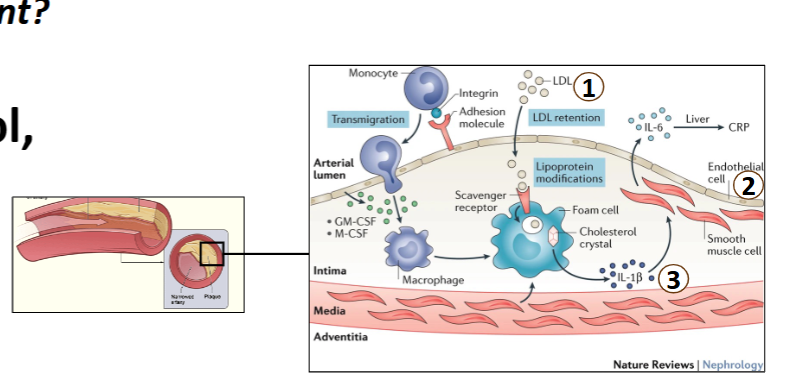
How does atherosclerosis start
Damage to the endothelium in the arteries (lipids can pass through intima) → inflammation + macrophage activation of LDL → turn into foam cells → accumulation > plaque stabilization by smooth muscle —> clot dislodge = further damage = blood clot
Embolus
Made of the clot that is formed in response to plaque
Cholesterol + triglycerides are ______ in the blood and need ____ to carry them
Insoluble; lipoprotein transporters
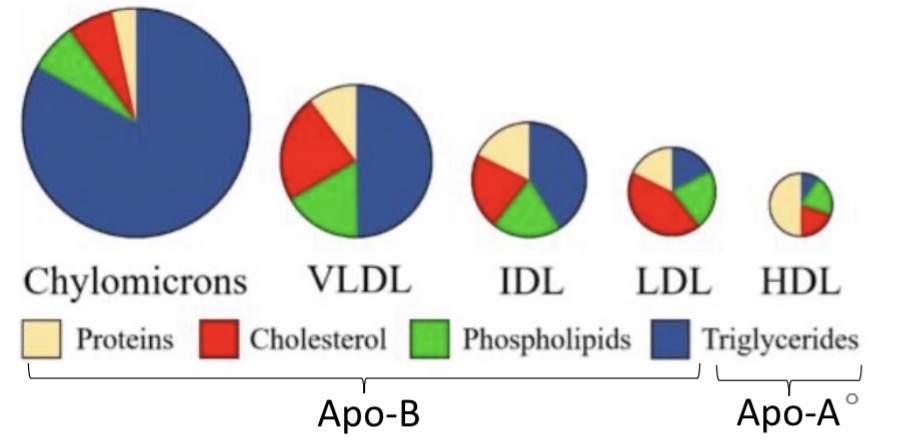
What are the types of lipoproteins transporters (4)
Chylomicrons
Very low-density lipoproteins
Low-density lipoproteins
High-density lipoproteins.
proteins makes things denser
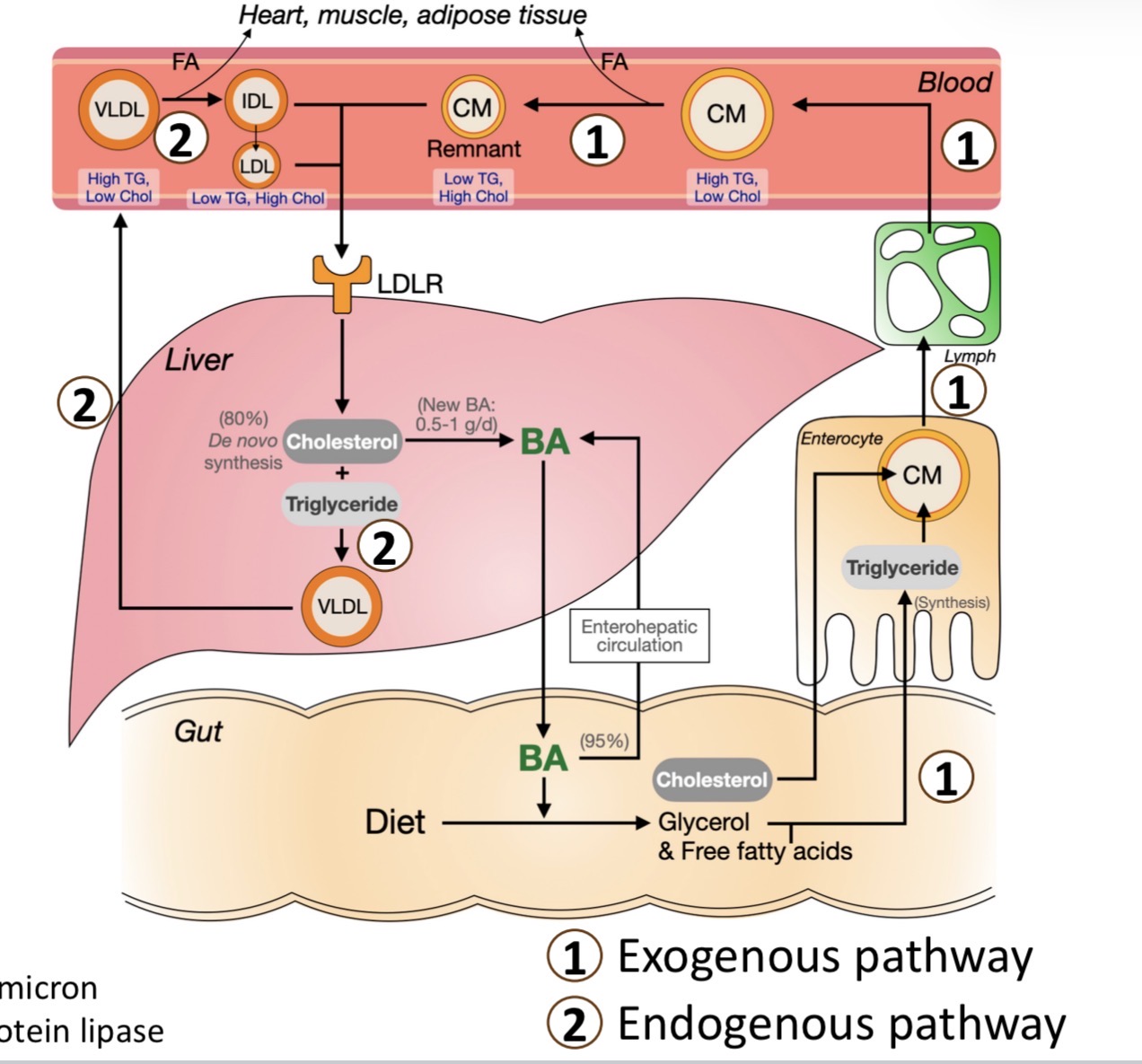
Exogenous pathway of lipid metabolism
dietary triglycerides broken down → (glycerol + FA) by (bile acids + pancreatic lipase)
enters enterocyte by simple diffusion assembled into chylomicron
chylomicron → lymphatic → jugular vein
any steps not work = atherosclerosis
what treatments of other 3 disease that can reduce the risk of atheroscleorsis
hypertension
chronic kidney disease
diabetes
systolic blood pressure
pressure in arteries during heart contraction
diastolic bp
pressure in arteries during heart relaxation
formula for blood pressure
bp = cardiac output (CO) * total peripheral resistance
cardiac output
volume of blood pumped out by the heart in one minute
CO= Stroke volume (mL/ beat) * heart rate (beats/min)
total peripheral distance
total resistance in blood in systemic circulation in peripherals
what are the short term regulation of BP
baroreceptors in carotid artery and aorta by regulating SNS and PSNS
baroreceptors when bp low
activate sympathetic, inhibit PSNS
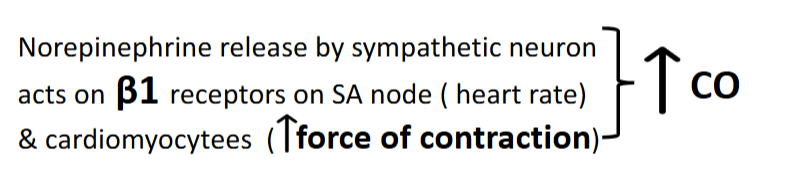
baroreceptors on cardiac output of SNS
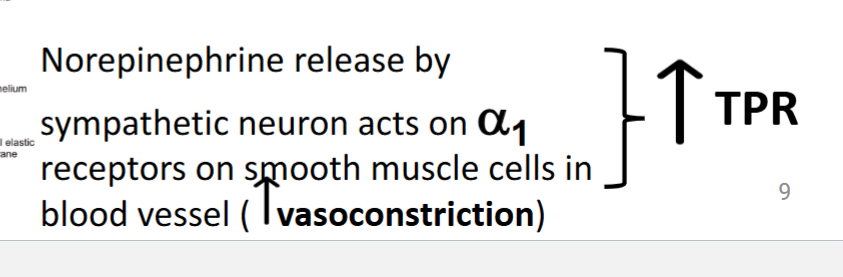
baroreceptors on total peripheral distance of SNS
baroreceptors when BP is high
activate PSNS inhibit SNS
decrease norepinephrine release to decrease force of contraction on beta1 receptors on SA node + cardiomyocytees
decrease NR on alpha1 receptors on smooth muscle to decrease vasoconstriction
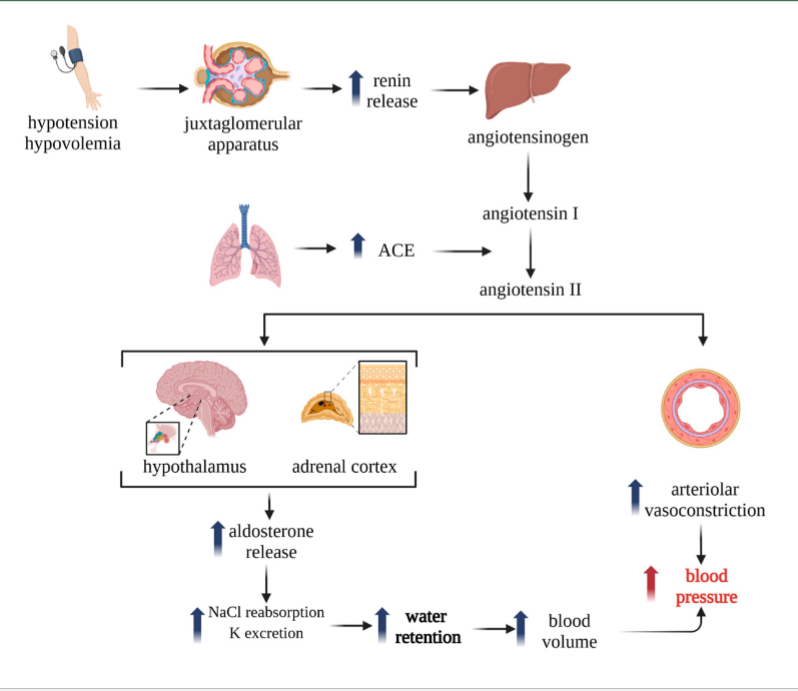
short term regulation of low blood pressure RAS
BP low → intrarenal receptors in renal artery sense low pressure OR low NaCl filtrate in macula densa —> release renin → activate RAS
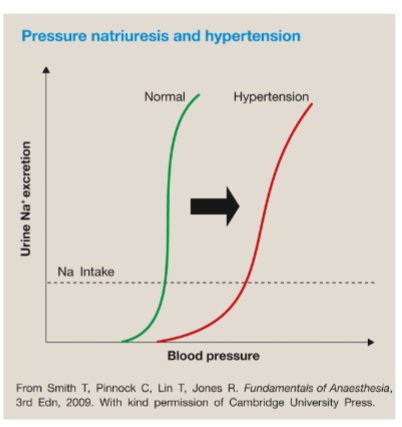
long-term regulation of blood pressure
pressure natruiresis (Na secretion in response to pressure
long term high blood pressure
renal artery pressure increase + Na reabsorption decrease (excreted in urine) → draws water out → low BP due to low water in blood
long term low blood pressure pressure natruiresis
renal pressure decreases, Na reabsorption increases (less excretion in urine —> draw water in → high BP
what are the lifestyle changes to reduce risk of atherosclerosis
healthy diet, exercise, limit alcohol/ no smoking
only for those who are at risk, those who have it need meds
orthostatic hypotension
reudced bp when standing because gravity decrease amount of venous return to heart
why do we drugs to treat hypertension if we have our own defense mechanisms
baroreceptors reset to higher BP (they would only bring it back to the HTN “normal” BP)
RAAS is overactivated due to artery thickness and stiffness (due to low pressure in kidney renin thinks person has low BP)
pressure natruiresis (kidney) shifts right
thiazides what and what
diuretic hypertension drugs
includes hydrocholorthiazide, chlorthalidone, indapamide
what is the mechanisms of thiazide
blocks Na/Cl TP in distal tubule → dec. Na+ reabsorption → dec. blood volume → decrease cardiac output /BP
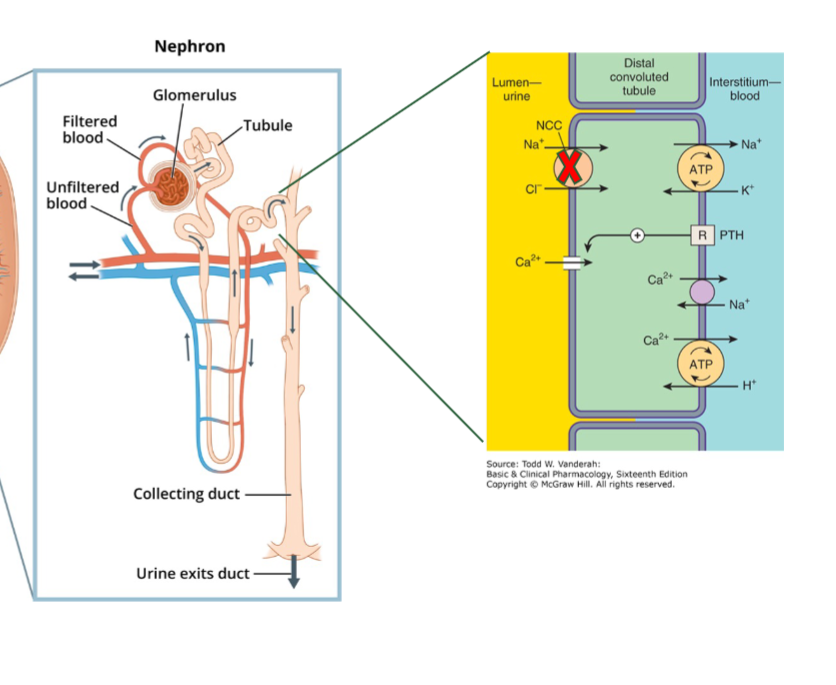
what are the side effects of thiazides
hyponatremia and hypokalemia
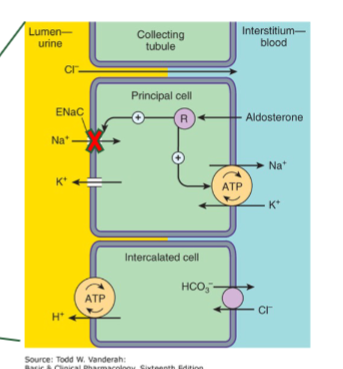
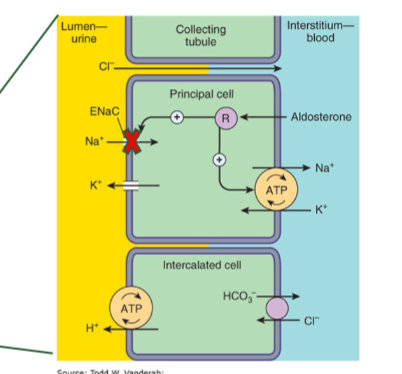
amiloride
potassium sparing duretic that bloacks ENaC in distal tubule + collecting ducts → decrease cardiac output → decrease BP
K+ wont leave blood because lumen is not negative from Na being reabsorbed
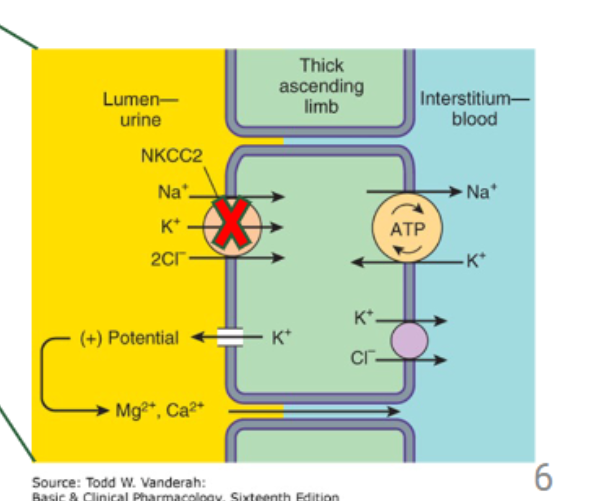
furosemide
loop diuretic that blocks NKCC in thick ascending limb
ONLY IN PATIENTS WITH HEART FAILURE OR CHRONIC KIDNEY DISEASE
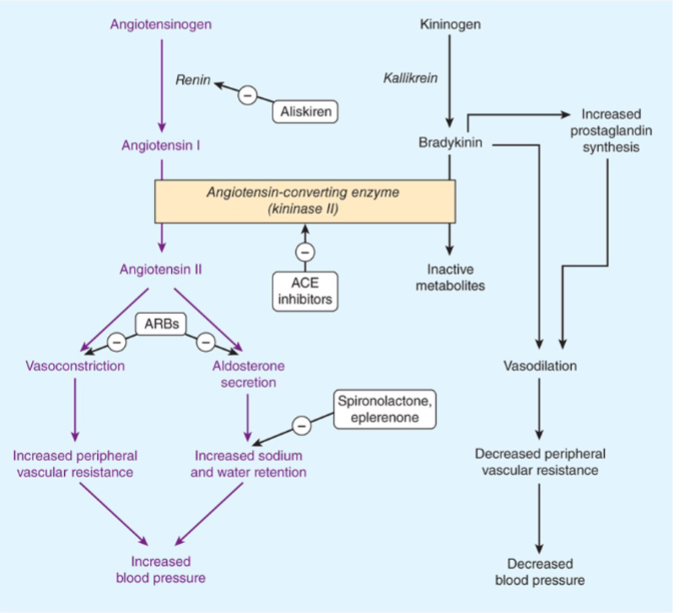
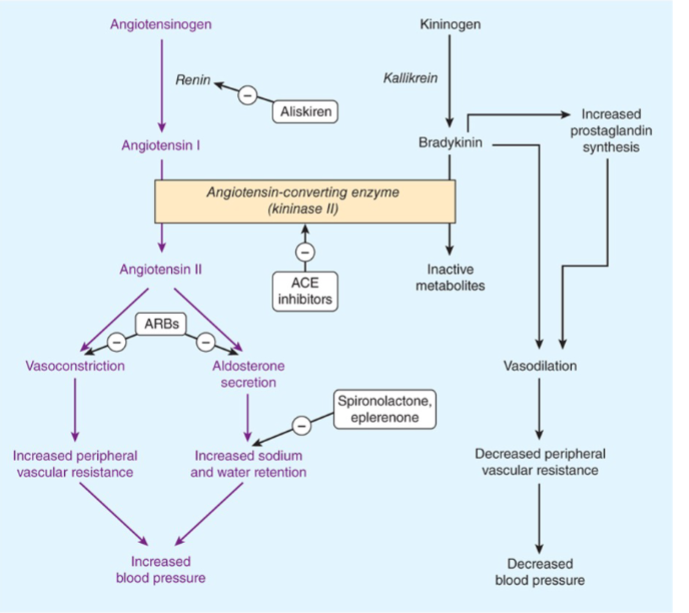
ACE inhibitors
a group of RAAS inhibitors that include (captopril, enalapril, lisinopril, ramipril)
what is the mechanims of RAAS inhibitors
inhibit angiotensin II and aldosterone production → decrease BP
increase bradykinin (vasodilator) → decrease BP
why do we need to inhibit RAAS pathway
because it secretes aldosterone and is overactive in hypertensive patients
what are the adverse effects of RAAS inhibitors
dry cough and angiodema from bradykinin effects (sensitize neurons)
ARBs
angiotensin receptor blockers that inhibit RAAS (includes: losartan, valsartan, telmisartan)
what is the mechanism or ARBs
they block the AT1 receptor of Ang II
indication of ARBs
first line class for hypertension meds when ACE inhibitors are not tolerated
what are the adverse effects of ARBs
hyperkalemia (aldoesterone effects, inhibit sodium will increase potassium in blood)+ acute kidney injurt
what is the indication of ACE inhibitors
first line class for HTM (great benefit if pateint has heart failure or chronic kidney disease)
ACE inhibitors and ARBs (should/should not)be combined together
SHOULD NEVER it will completely abolish RAAS (mega hyperkalemia), kidney problems
aldoesterone antagonists
RAAS inhibitors that include spironolactone and elprenolone block aldoesteron receptor
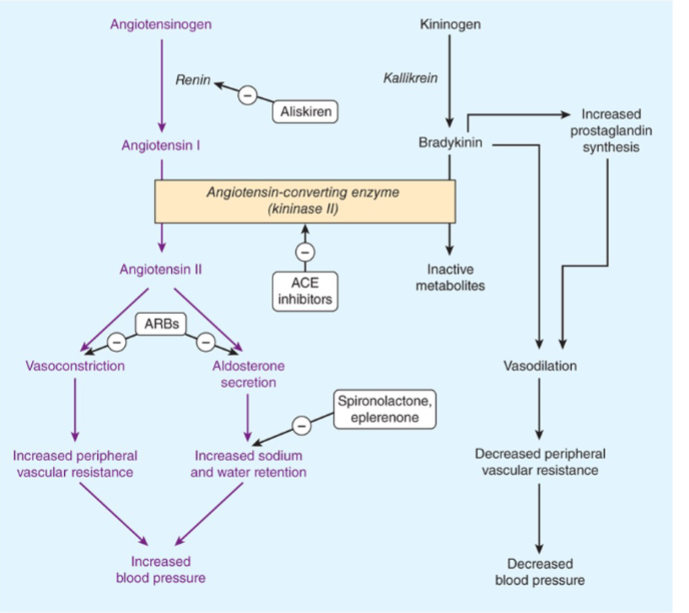
mechanissm of aldoesterone antagonists
block aldoesterone receptor to inhibit synthesis of ENaC chanenels→ dec. Na+ reabs
indication of aldosterone antagonists
best add on for resistant HTN (especially good for patients with primary aldosteronism)
adverse effects of spironolactone
gynecomastia (similar to sex hormone)
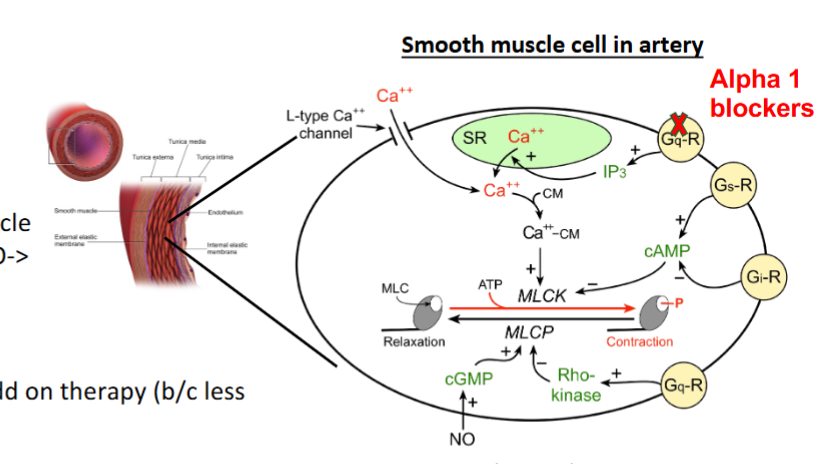
dihydropyridines
calcium channel blockers that include (nifedipine, amlodipine, felodipine)
mechanism of dihydropyridines
block L-type calcium channels in smooth muscle of arteries → increase vasodilation → decrease BP
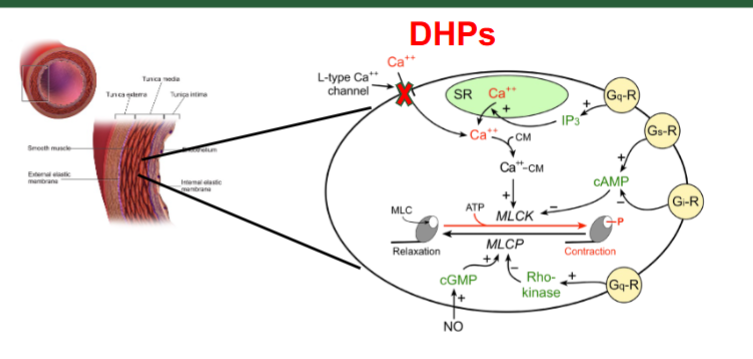
what is the indication for DHP + adverse effect
first line class for HTN
edema (increased pressure in capillaries only not venules → hydrostatic pressure difference)
non-dihydropyridines (nonDHP)
calcium channel blockers that include diltiazem and verapamil
mechanisms of calcium channle blockers
block L type Ca channels in SA node in heart → decrease heart rate
block L type Ca channels in cardiomyocytes in heart → decrease contraction
indication + adverse effects of non DHP
HTN pateints with arrythmia
adverse: bradycardia
betablockers
metoprolol, esmolol, bisoprolol
mechanisms of beta blockers
block beta 1 receptors in SA node in heart → decrease heart rate
block beta 1 receptors in cardiomyocytes in heart → decrease heart rate
Gs coupled
indication of betablockers
not first line for HTN pateints but effective in HTN pateints with heart failure (HFrEF)
adverse effects of betablockers
bradycardia, heart block
what should beta blockers not be combined with
nonDHP both are reducing heart rate and contraction SEVERE BRADYCARDIA (heart shut down)
alpha 1 receptors
prazosin, terazosin, doxazosin
mechanism of alpha 1 blockers
block alpha 1 receptors in smooth muscle arteries and venules → vasodilate → decrease cardiact out put → decrease blood pressure
both decrease cardiac out put
indication of alpha 1 blockers
not first line for HTN pateints only an add on therapy due to less faviorable ourcomes (HTN has benign prostatic hyperplasia + urination problem)
adverse effects of alpha 1
orthostatic hypotension
it vasodilates arteries and veins (decreasing the blood flow back to heart)
alpha 2 agonists
clonidine + methyldopa
mechanism of alpha 2 agonists
inihibit sympathetic outflow (ddecrease norepinephrine) → decreaes BPi
indication of alpha 2 agonists
not first line, only in resistant HTN
pregnancy (preeclampsia)- methyldopa (good for pregnancy)
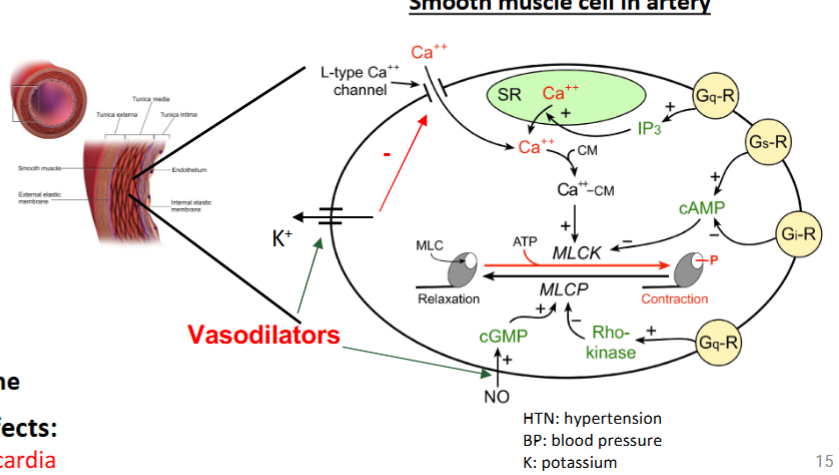
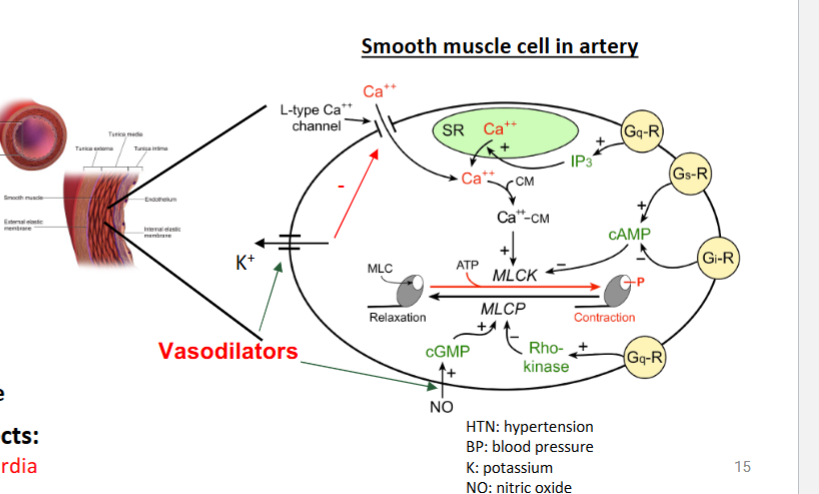
hydralazine + mioxidil
direct vasodilators
what are the mechanisms of hydralazine
increase NO → increase vasodilation → decrease BP
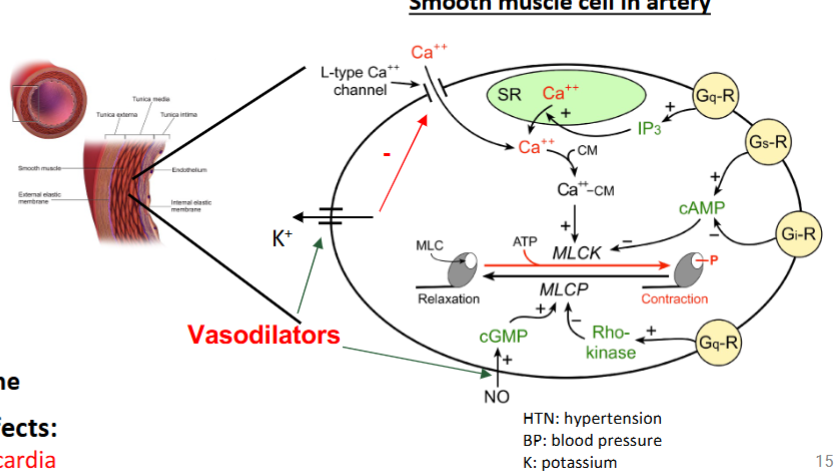
what is the mechansism of minoxidil
open K channels → hyperpolarization of smooth muscle → vasodilation → decrease BP
indication of direct vasodilators
not first line, only in resistant HTN (last resort)
pregnancy preeclampsia- hydralazine
adverse effects of direct vasodilators
vasodilation of carotid arteries → baroreceptor activation → reflex tachycardia (inc. sympathetic innervation to heart)
alpha 1 vs alpha 2 receptors
alpha 1 = Gq vs alpha 2 =Gi
what are the first line drugs of HTN`
thiazide, ACE inhib, ARBs, DHPs
either alone or in combo (never ACE with ARB)
gram negative vs gram pos cell memb
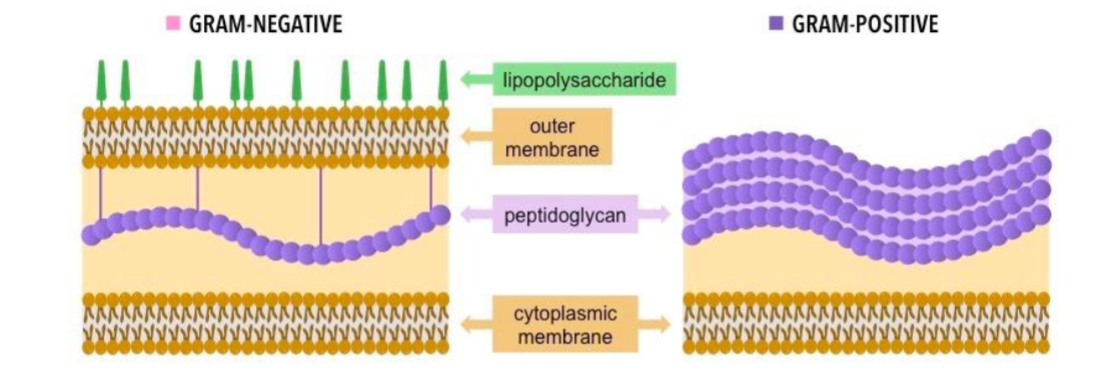
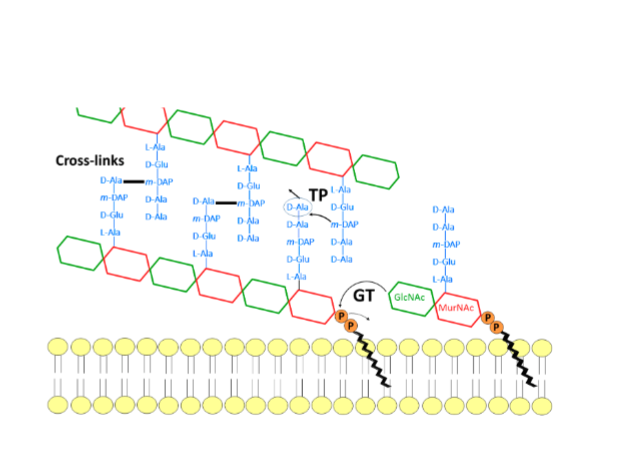
what is the peptidoglycan structure made of
glycan or N-acetylglucosamine and N-acetylmuramic acid (GlcNAc and MurNAc)
glycosyltransferase
(GT) an enzyme that polymerizes indivudal glycan strands together
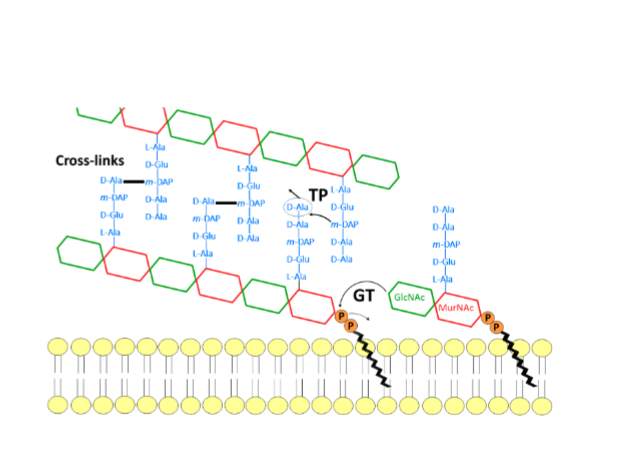
transpeptidase
TP cross linking strads (main target of antibioticss)
what are the 4 types of bacterial illnesses
food borne illnesses
sexually transmitted diseases
skin infections
highly infectious disease
what bacteria was cephalosporins derived from
the fungus Acremonium
how do beta lactams work
interrupt cell wall synthesis by inhibitng DD-transpeptidase (penicillin binding protein) enzyme that is responsible for cross linking cell wall → holes → bactericidal
effectiveness of different beta lactams on gram bacteri
only gram-positive at first but now has increased activity to negative
vancomycin
inhibits peptidoglycan cross inking produced by Actinobacteria
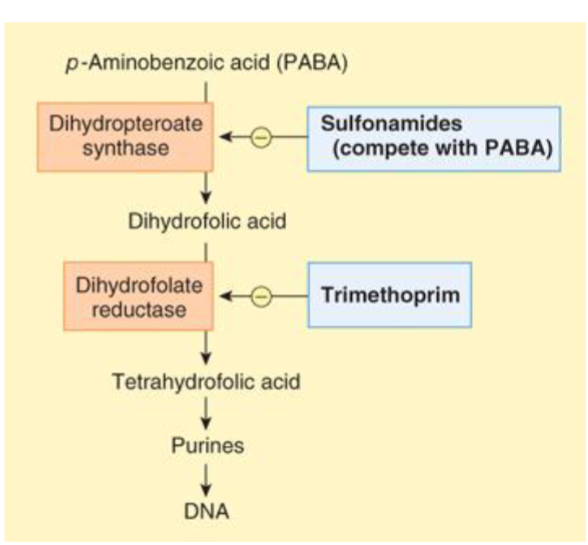
what do bacteria use to synthesize nucleic acids
folic acids
PABA
para-aminobenzoic acid is a nutrient obtained from the environment that is a folate precursor
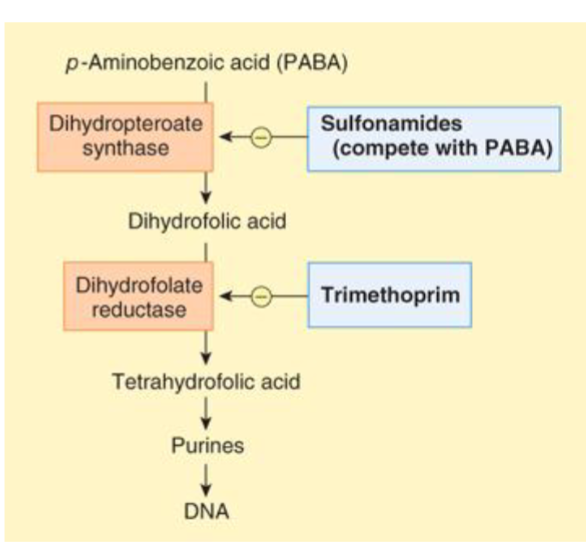
sulfonamides and trimethoprim
resemble PABA and dihydrofolic acid and interfere with PABA pathways
blocking only = bacteriostatic
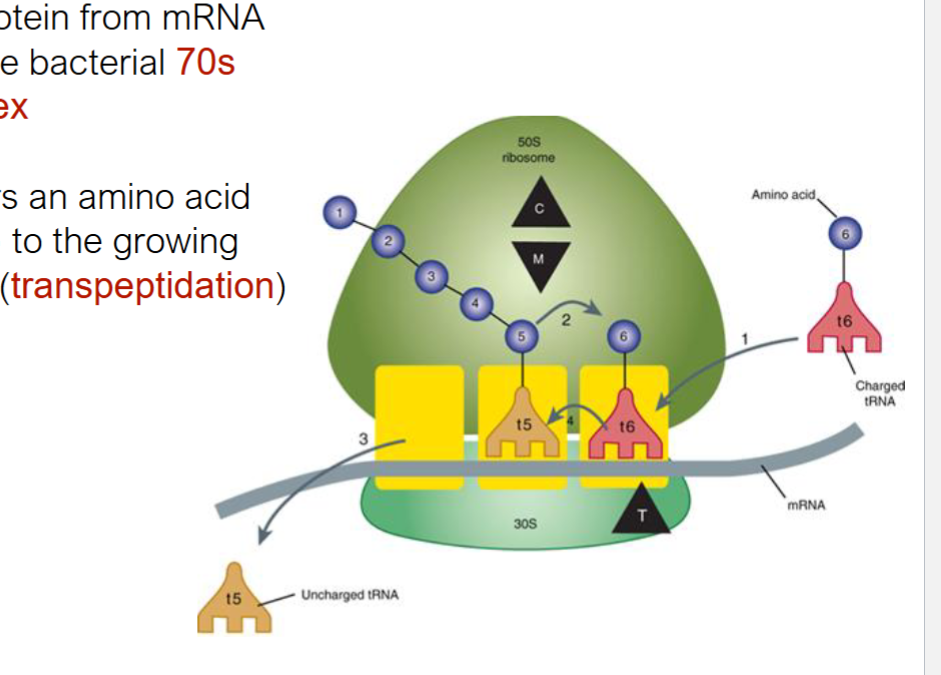
transpeptidation
tRNA t6 transfers aa to growing aa chain on 70s ribosome
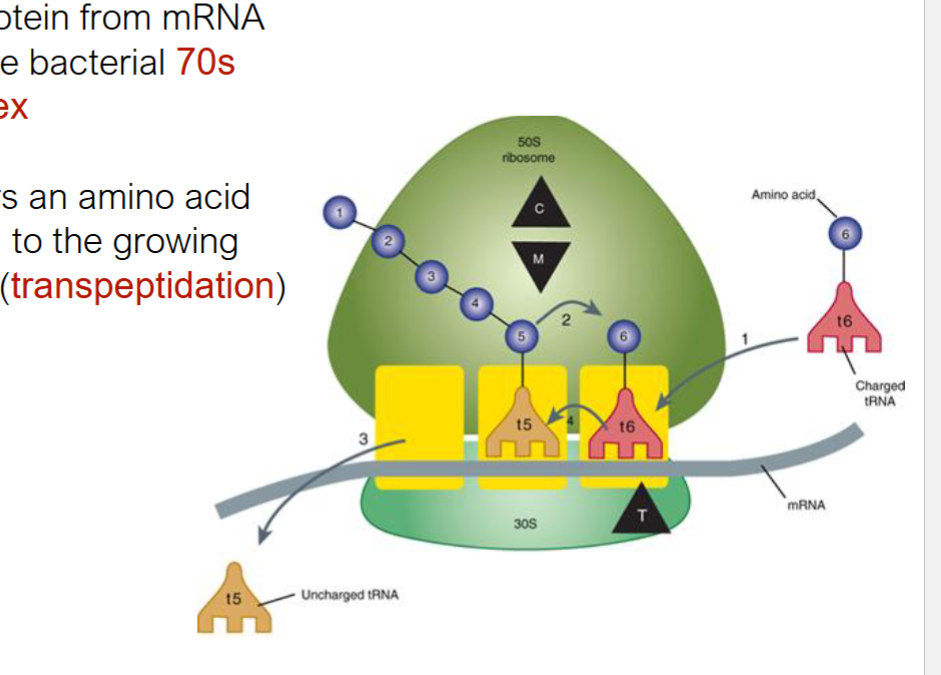
chloramphenicol and macrolides
bind to 50s subunit and block transpeptidation
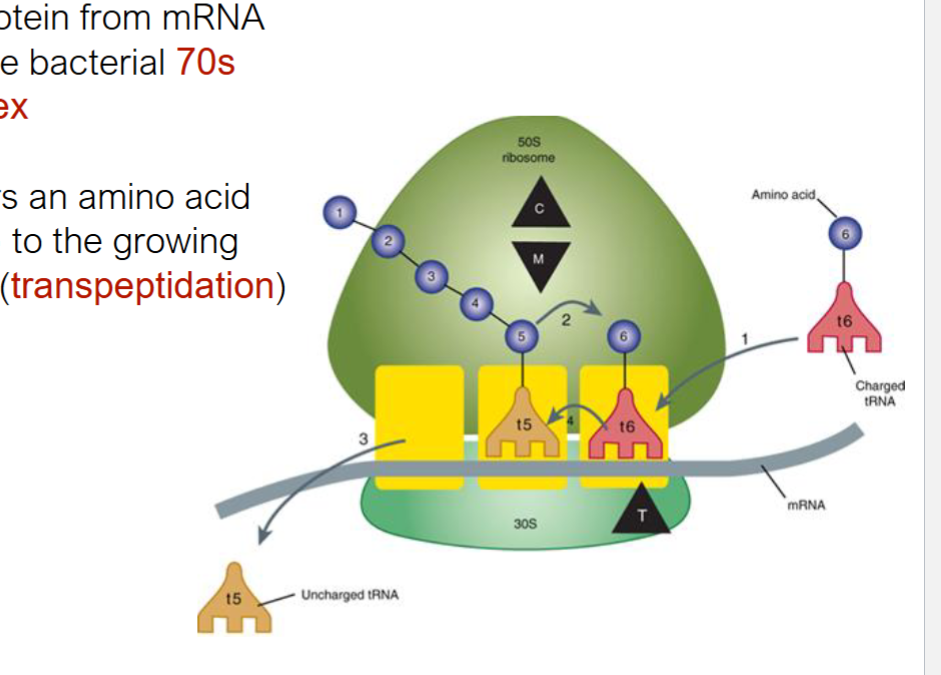
tetracyclines
bind 30s ribosomal subunit and prevent tRNA binding
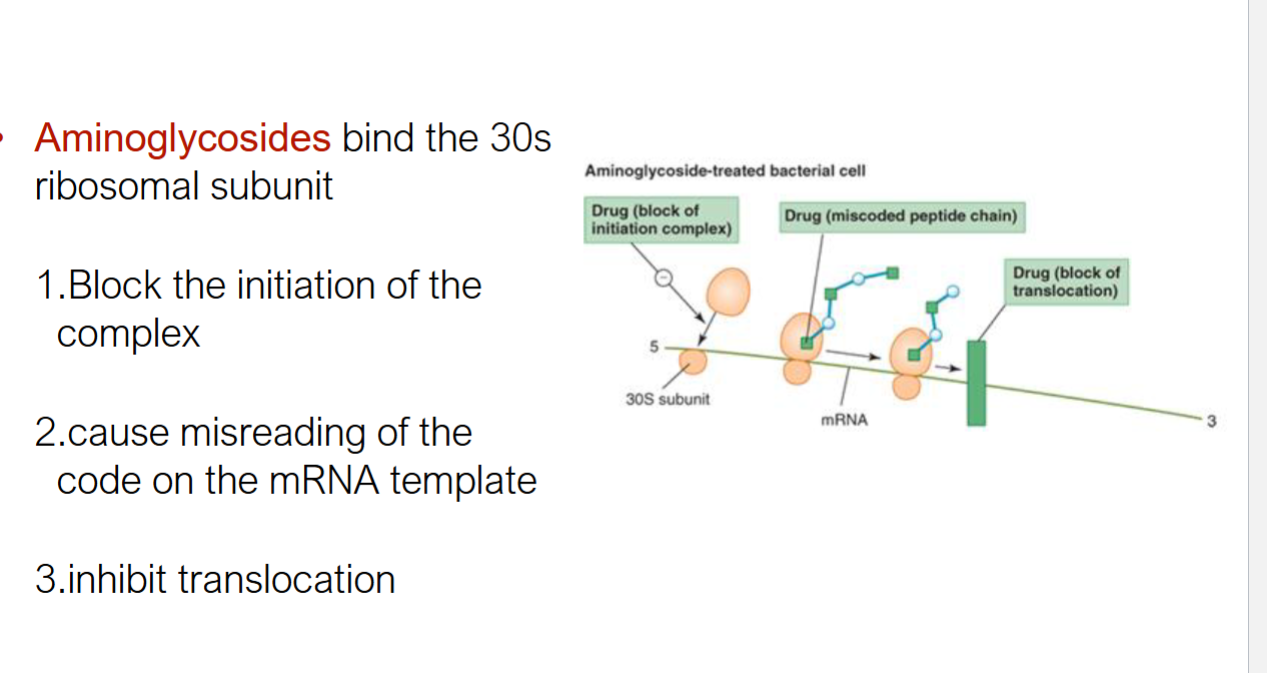
aminoglycosides
bind 30s ribosomal subunit that has 3 methods of function
block initiation
cause misreading of mRNA code
block translocation
stevens-johnson syndrome and toxic epidermal necrolysis
rare conditions that skin becomes detached from underlying tissues and sloughs off body
what are some methods of antibiotic resistance 4
drug inactivation or modificaiton
alteration of binding site
alteration of metabolic pathways
reduced drug accumulation (efflux) (elimination + distribution)
what are antibiotics
soluble compounds that are produced and released by microorgnanisms and that inhibit the growth or kill other microorganisms
what are viruses
obligate itracellular parasites
virions
viruses when they are not inside an infected cell, an independent particle
bacteriophage
a virus that only infects bacteria
viral range
a group of cell types or species that a virus can infect
most animal viruses ____ cros phyla
do not (some infect only closely related species)
pathogenicity
ability of viruses to causes disease
virulence
degree of pathogenicity
latency
ability of virus to remain formant in organisms