Cardio Exam 2- Madras
1/103
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
104 Terms
When do you do a lipid panel
Fasting
Low-density lipoprotein (LDL)
major atherogenic lipoprotein (carries 60-70% of blood CHO)
main target for lipid-lowering medications
high-density lipoprotein (HDL)
happy cholesterol
anti-atherogenic effect
Causes of reduced HDL
smoking, obesity, sedentary lifestyle, beta-blockers
causes of increased HDL
smoking cessation, moderate alcohol ingestion, physical exercise, weight loss, oral contraceptives, phenytoin
Apolipoproteins
structure to lipoprotein
receptor binding
activate enzyme system
chylomicrons made of
triglycerides
Resulting Medical Conditions
MI, angina, arrhythmias, stroke, peripheral arterial disease, abdominal aortic aneurysm, sudden death
High TG puts you at risk for
pancreatitis
what causes hypercholesterolemia
thiazides, cyclosporine, glucocorticoids, protease inhibitors, isotretinoin, beta-blockers, progestins, mirtazapine, sirolimus
Non-pharm
diet, regular exercise, decrease body weight (10% body weight), stay away from saturated fats, smoking cessation, lower BP
Plant Sterols/Stanols
Benecol and Take Charge
lower LDL
GI side effects
Bile Acid Sequestrants Ex
Colestipol, cholestyramine, colesevelam
Main effects of bile acid sequestrants
bind bile acids, send signal to liver (need more), drop liver supply of cholesterol = lower LDL BUT they can raise TG (bad)
Colesevelam different indication
help with glycemic control in type 2 DM; contraindicated in bowel obstruction and TG >500
Colestipol dose
start 5gm QD or BID or 2gm QD or BID
max 30gm/day granules or 16gm/day tablet
cholestyramine dose
take with meals
start 4gm QD or BID
max 24gm/day
colesevelam
take with meals
3.75gm/day in 1-2 divided doses
colestipol and colesevelam granules for oral suspension counseling point
do NOT take in dry form
cholestyramine suspension counseling point
do NOT sip or keep in mouth for long time —> may cause tooth discoloration and enamel decay
bile acid sequetrants interactions
take 1-4 hours before or 4-6 hours after bile acid sequestrant
colesevelam: decrease binding affinity for other drugs
when to take IR lovastatin
evening meal
when to take ER lovastatin
take in evening at bedtime
max effect seen in statins
in about 6 weeks
stations MOA
inhibit HMG CoA reductase —> increase synthesis of cell surface LDL receptor —> increase LDL blood clearance
what are the two high intensity statins
atorvastatin and rosuvastatin
when to take simvastatin
in the evening
Rosuvastatin is preferred in which patients
asian
statins can cause
myopathy or increased muscle injury at 80mg
80mg should only be used in pts who have been taking this dose ≥12months with no muscle toxicity
which statin needs adj in renal impairment
lovastatin, pravastatin, simvastatin, rosuvastatin (40mg), pitavastatin (not indicated to reduce CV morbidity & mortality)
rosuvastatin indication
primary prevention of CVD
secondary prevention
already had a CV event
Statin Adverse effects
increase HBA1c and fasting glucose levels reported with statin
ADA Guidelines: may elevated type 2 DM risk if at elevated risk of developing type 2 DM —> monitor glucose status regularly and DM prevention reinforced —> not recommended statins be D/C
What test(s) do you do before initiating statin and as clinically indicated thereafter
ALT, AST (liver enzyme tests), total bilirubin, and alkaline phosphatase (liver panel) if experiencing heptatoxicity symptoms
ACC/AHA/ADA Guidelines: obtain ALT and AST at baseline (fasting ideal)
Do NOT measure routinely if taking statin >3times ULN increase in transaminases with no symptoms does not occur frequently, does not impact occurrence, improves when decrease dose or give alternative statin
Statin Adverse effects/ interactions
dyspepsia, increase blood glucose, myopathy/rhabdomyolysis (increased risk with gemfibrozil), CYP3A4 inhibitors (interaction)
what you draw when you have myalgia (myopathy/rhambdomyolysis)
CK (creatine kinase), CPK
Gemfibrozil myotoxicity
inhibits glucuronidation or preventing renal clearance of statins and increases statin levels, fenofibrate less potential to interfere with statin metabolism
hallmark of rhabdomyolysis
brown-tinged colored urine
risk factors for myotoxicity
older age, kidney/liver disease, excessive alcohol intake, heavy exercise
Not severe statin symtoms
rechallenge with modify dosing regimen, use another statin or in combo with nonstatin to obtain max lowering of LDL
True/False You measure CK levels routinely if taking statin
false— only take CK levels if severe statin-associated muscle symptoms
ACC/AHA/ADA 2018 Lipid Guidelines lipid panel
4-12 weeks after starting or adjusting statin dose then every 3-12 months
Foods to avoid with lovastatin, atorvastatin, simvastatin
grapefruit juice
If we double dose of statin does it double efficacy
No
Bempedoic Acid (Nexletol)
adenosine triphosphate-citrate lyase (ACL) inhibitor
decrease LDL-C by up regulating LDL receptors
main effect: decrease LDL
Nexletol (Bempedoic Acid) indications
decrease MI and coronary revascularization risk in adults who are not able to take recommended statin and have CVD, or high risk for CVD event by do NOT have CVD
adverse effects Nexletol (Bempedoic Acid)
hyperuricemia, increased LFTs, tendon rupture
when to check lipid panel for Bempedoic Acid (Nexletol)
8-12 weeks after stating medication
Fibrates examples
gemfibrozil, fenofibrate
Fibrates MOA
stimulate PPAR-a receptors
increase HDL, decrease TG, increase apo A1 and A2
Class of Nexletol
ACL inhibitor
Adverse effects of Fibrates
gallstones- main,
Monitoring in Fibrates
CBC, LFTs
contraindications with Fibrates
gallbladder disease, hepatic disease, renal disease, primary biliary cirrhosis
Ezetimibe (Zetia)
decrease LDL
dose 10mg QD
adverse effects Ezetimibe (Zetia)
increase LFTs, GI, back pain, chest pain, angioedema, gallstones, pancreatitis, ect.
AVOID use with gemfibrozil
Main effect of Zetia
lower LDL
pathway Zetia works on
exogenous pathway
Nicotinic Acid- Niaspan
decrease LDL and TG, decrease hepatic TG production
DO NOT recommend dietary supplement SR products
DO NOT recommend IR products
NOT SUBSTITUTED FOR EQUIVALENT DOSES
OTC fish oil: NOT FDA
Niaspan: extended release—> safer profile, less hepatoxicity
Niaspan lipid effects
lower LDL, lower TG, increase HDL
Nicotinic Acid Adverse effects
itching: prostaglandin mediated
hyperuricemia
hyperglycemia
myopathy
hepatoxicity (most with SR): max dose niaspan 2gm/day
FLUSHING: prostaglandin mediated—> reduce with aspirin, Tylenol, take with food or bedtime, avoid hot shower
rhabdomyolysis when dose ≥1gm/day and given with statin
Niaspan can activate
peptic ulcers
Contraindications with Nicotinic Acid
Active liver disease, active peptide ulcer disease, arterial bleeding
Precautions(risk vs benefit)
Hx of liver disease
gout —> baseline uric acid levels repeat stabilized dose
DM (alternative to statins or vibrates) check baseline glucose level repeat when stabilized dose
Lomitapide (Juxtapid) main effect
Lower LDL
Lomitapide (Juxtapid)
approved for homozygous familial hypercholesterolemia
Boxed warning Lomitapide
Increased liver transaminases (measure ALT,AST, alkaline phosphatase, total bilirubin at baseline; then at least ALT and AST before every dose increase or every month) for 1st year then at least ALT and AST at least every 3 months and before each dose increase
increases hepatic fat
how is Juxtapid taken
orally
Where is Praluent stored
in fridge
Alirocumab (Praluent)
PCSK9 inhibitor—binds to low-density lipoprotein receptors on hepatocyte surface to promote LDLR degradation within liver
reduce risk of MI, stroke, and unstable angina requiring hospitalization in adults with CVD
Alirocumab (Praluent) dose
start at 75mg SubQ
Evolocumab (Repatha)
PCSK9 inhibitor
reduce risk of MI, stroke, and coronary revascularization in adults with CVD
SubQ
How is Leqvio used
SubQ
Fish Oil
Increases LDL (5-10%), increases HDL (1-3%), DECREASE TG(30%)
Vascepa- Fish Oil
EPA (omega 3 fatty acid)
Dose- BID orally with good
Hepatic impairment: monitoring LFTs
REDUCE-IT Trial
Patients had CVD or had DM and other CV risk factors: taking statin and fasting TG 135-499mg/dL and LDL 41-100mg/dL
Lovaza Fish Oil
contains DHA and EPA
oral administration
GI upset effect
ACC AHA Guidelines
Need to draw lipid profile within 24hours
LDL accurate if TG are <400 (cannot calculate if TG >400)
LDL<70 mg/dL (calculation not reliable)
may measure direct LDL or modified LDL estimate to increase accuracy compared to calculation
High Intensity Statin (Lowering LDL by ≥50%)
Atorvastatin 40 or 80
Rosuvastatin 20 or 40
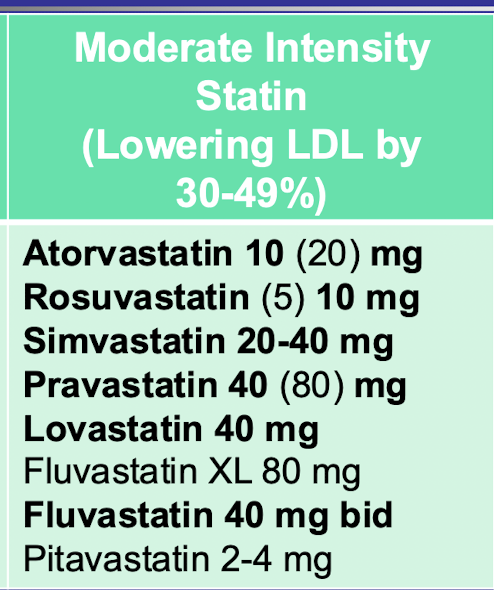
Moderate intensity statin (lowering LDL by 30-49%)
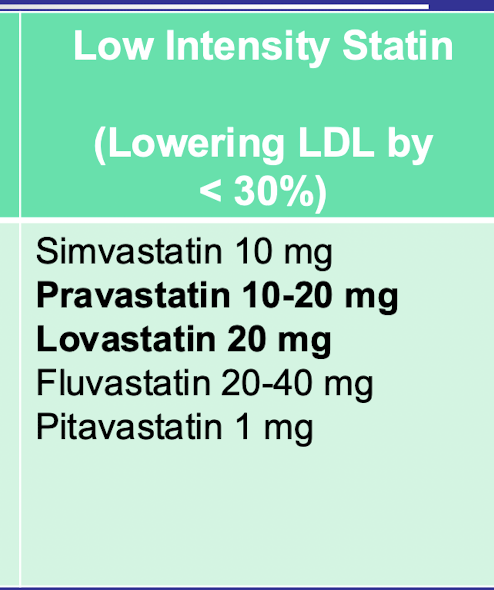
Low intensity statin (lowering LDL by <30%)
1st statin group
Secondary ASCVD prevention
Already high risk DONT need ASCVD score
2nd statin group
Severe hypercholesterolemia (LDL ≥ 190mg/dL)
Age 20-75
No risk score
3rd statin group
Primary prevention: adults 40-75 with DM and NO ASCVD and LDL ≥70mg/dL
4th statin group
Primary prevention: adults 40-75 and LDL 70-189 AND NO DM AND NO ASCVD AND ≥7.5% 10yr ASCVD risk
*NEED RISK SCORE
Clinical ASCVD defined
ACS, MI, stable or unstable angina or coronary or other arterial revascularization, stroke, TIA, PAD including aortic aneurysm
Very high-risk defined
multiple major ASCVD events OR 1 major ASCVD event and multiple high-risk conditions
≤75 YO with Clinical ASCVD
high intensity statin
Very high risk clinical ASCVD and on max tolerated statin dose and LDL ≥70mg/dL
adding ezetimibe
Clinical ASCVD and ≥75 YO
moderate or high-intensity statin
Primary Prevention: Severe Hypercholesterolemia
20-75 YO and LDL≥190mg/dL
high intensity statin/max tolerated statin (no risk assessment is needed, first goal: ≥50% LDL reduction)