Pain Management of the Laboring Woman
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
PAIN NEUROLOGY
Visceral pain
Dull and aching
Results from the activation of nociceptors of the thoracic, pelvic, or abdominal viscera (organs)
Visceral structures are highly sensitive to distension (stretch), ischemia and inflammation
Referred pain
Somatic pain
Sharp, burning, prickling
Referred to as skin, tissue, or muscle pain
The nerves that detect somatic pain are located in the skin and deep tissues
PAIN DURING LABOR AND BIRTH
HOW LABOR PAIN IS DIFFERENT FROM OTHER TYPES OF PAIN
Labor pain:
Is not a symptom of injury or illness
Only lasts a certain amount of time
Is predicable
Intensifies gradually over time
Labor pain differs from other kinds of pain in ways that make coping easier. Labor pain:
Is not a symptom of injury or illness: Many times we associate pain with something being wrong which can increase a laboring woman’s anxiety. It will be necessary to remind her that the labor pain she is feeling is normal and is a sign that her body is working hard and well.
Only lasts a certain amount of time: Once active labor begins the process rarely takes more than 24 hours.
Labor pain is predictable: Contractions can last up to 90 secs and come in a regular pattern, followed by a few pain-free minutes in between them. This means a laboring woman can predict and prepare for each contraction and rest between them.
Intensifies gradually over time: Contractions almost always start off mild and gradually grow longer, stronger and closer together. This gives the laboring woman time to adapt.
PAIN PERCEPTION AND EXPRESSION
Highly personal and subjective
Affected by gender, culture, ethnicity, and past experiences
Physiological/affective expression
Increased catecholamines
Increased blood pressure, heart rate, and temperature
Altered respiratory pattern
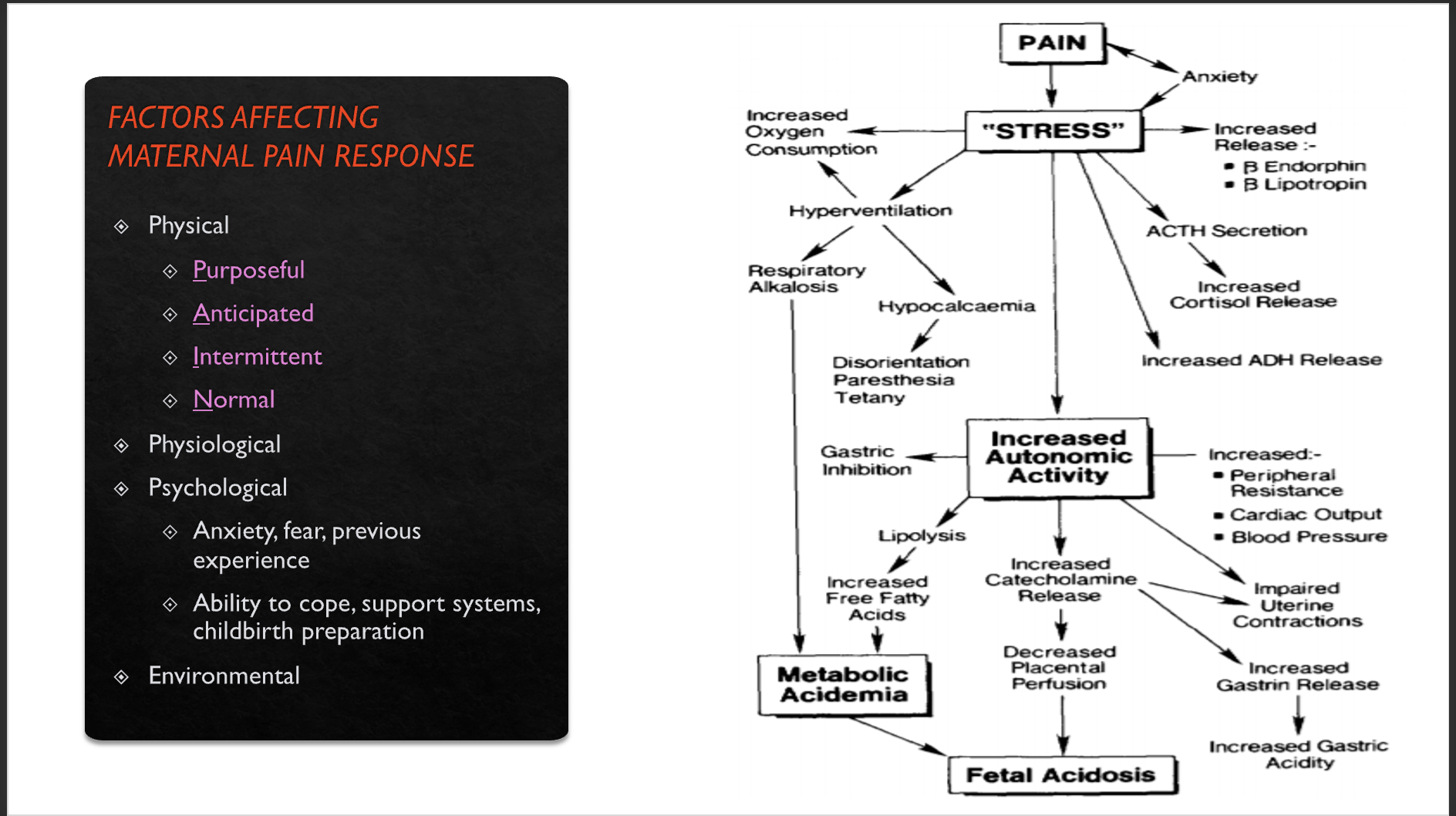
FACTORS AFFECTING MATERNAL PAIN RESPONSE
Labor pain is different for each woman, and it can be different for each labor. However, women often experience:
(Physical)
Lower abdominal pain during contractions.
Low back pain, either with contractions or, less often, continuously.
Pain throughout the belly, in the hips, buttocks or thighs, or in some combination of these locations.
Pain that moves from front to back, back to front or down the thighs.
Pain that is felt in several areas at once, or just in one specific place.
Words women use to describe their pain include cramping, sharp, aching, throbbing, pressing and shooting.
(Physiological)
During labor, there is an increase in endorphins that act as the body’s natural pain relief. Recent research has shown that massage may facilitate and stimulate the brain’s ability to produce endorphins.
The gate-control theory proposes that there is a gating mechanism involved in the transmission of pain impulses to the cerebral cortex area of the brain or in other words it affect a woman’s level of pain awareness. With the use of massage, focal point, and relaxation, pattern breathing, for example, a gate closes to prevent other impulses from being interpreted as the primary message, allowing for a degree of pain relief.
(Environment)
Loud noises
On-going interruptions
Bright lights
Restricted movement AND
Limited privacy
Can intensify a woman’s pain during labor
PAIN PATHWAYS AND CHILDBIRTH, cont.
Gate Control Theory
This theory suggests that the spinal cord contains a neurological "gate" that either blocks pain signals or allows them to continue to the brain.
In times of anxiety or stress, descending messages from the brain may amplify the pain signal at the nerve gate as it moves up the spinal cord, which will intensify pain.
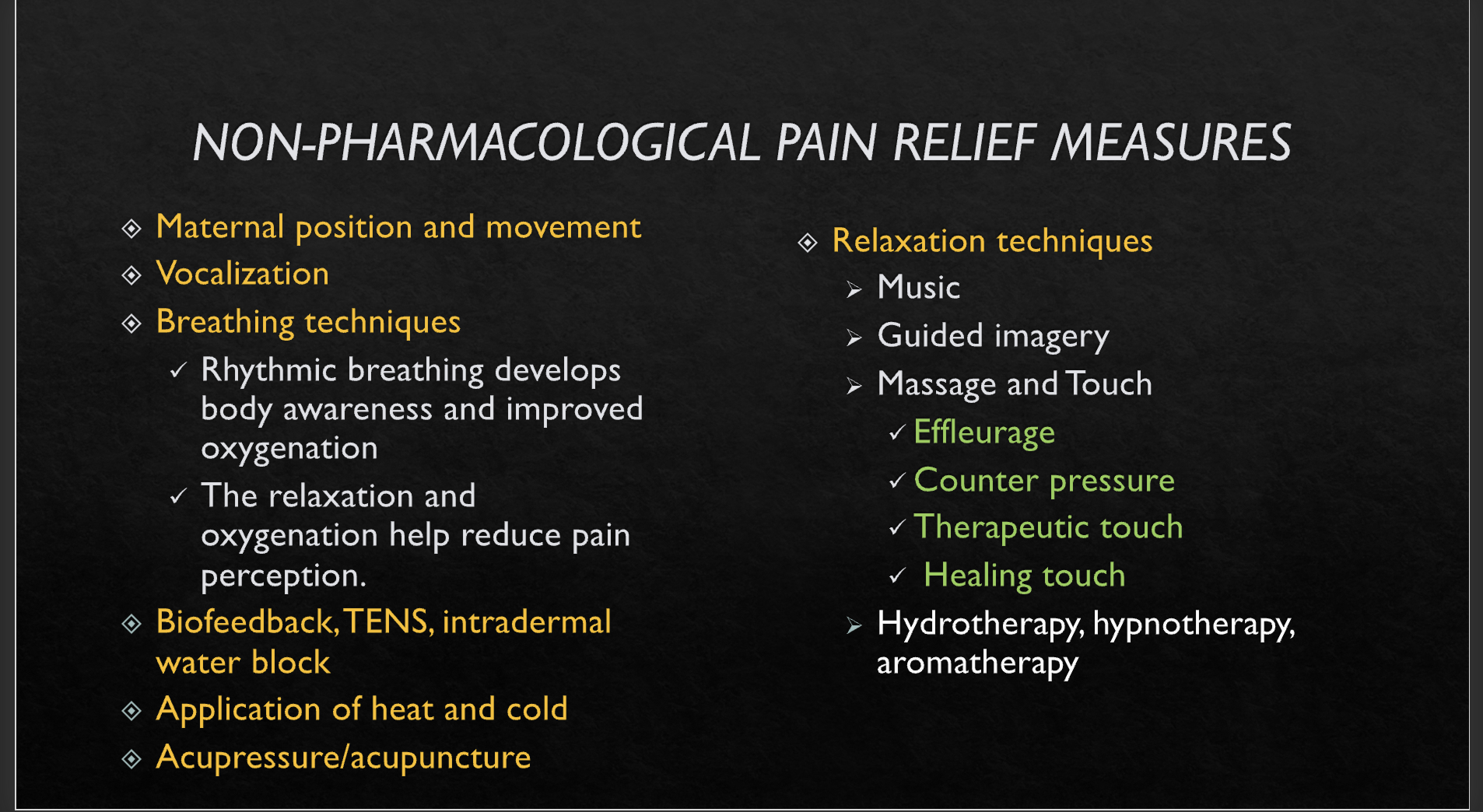
NON-PHARMACOLOGICAL PAIN RELIEF MEASURES
PHARMACOLOGICAL CHOICES FOR PAIN RELIEF
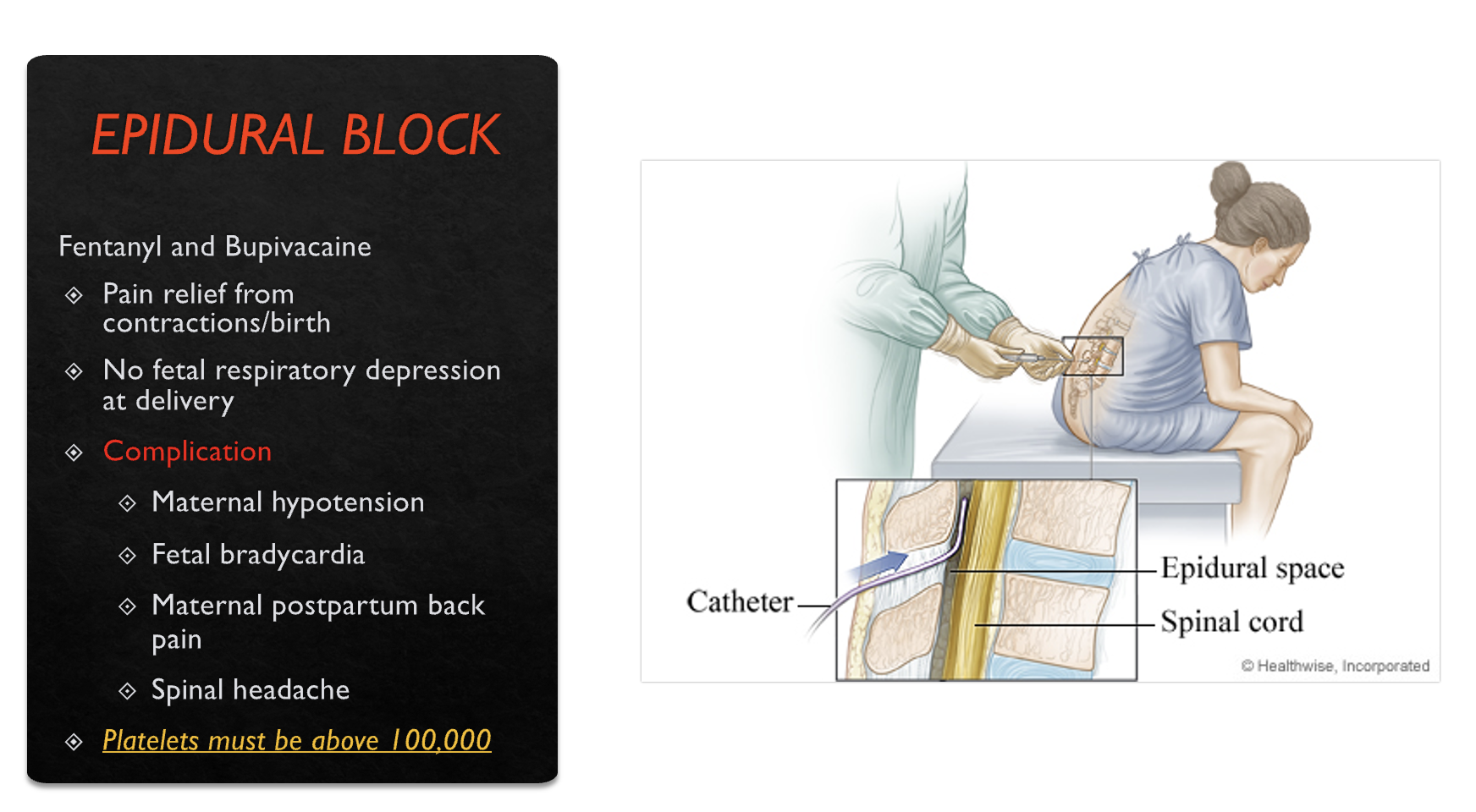
EPIDURAL BLOCK
Limited mobility
Sympathetic blockage
Common side effects
Positional effects (one-sided numbness)
Maternal hypotension
Fetal bradycardia
Accidental injection into blood vessel
Urinary retention, bladder distention
MANAGEMENT OF MATERNAL HYPOTENSION
SPINAL NERVE BLOCK

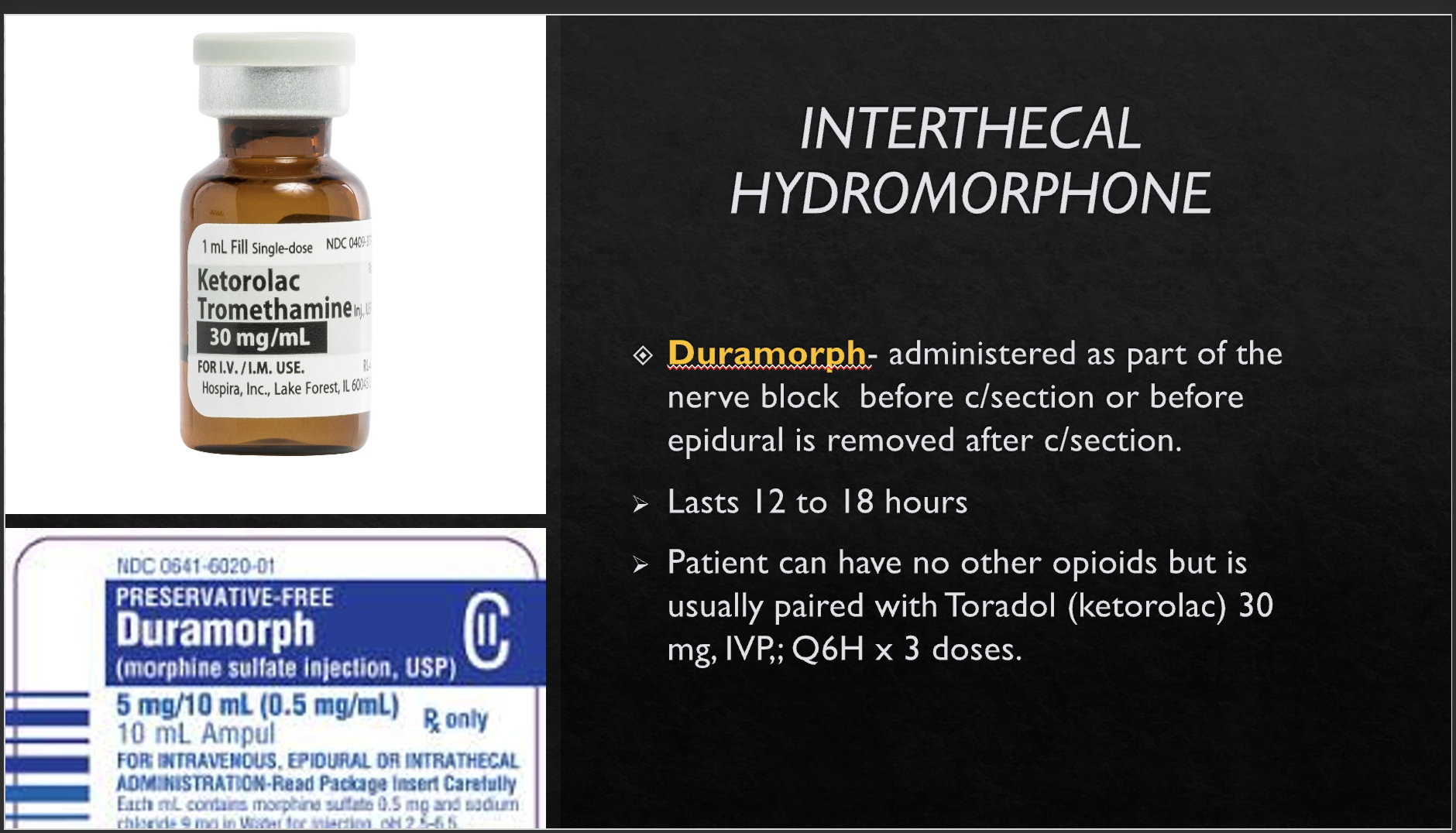
INTERTHECAL HYDROMORPHONE
GENERAL ANESTHESIA
Major risks for woman and fetus
Preoperative preparation
Intubation is required
PACU nursing care
Cardiac monitoring
Continuous vital signs
PCA pump set up and administration
Pre-op prep
Patient interview and consent
IV administration
Assessment of mouth/teeth and airway
Major risks include
Maternal hyperoxia (too much oxygen can be toxic to the CNS; seizures/coma)
Maternal hypercapnia which can lead to fetal acidosis (excessive carbon dioxide in the bloodstream-inadequate respiration)
Maternal uterine vasoconstriction and reduced uterine blood flow which could lead to decreased perfusion to the fetus
NURSING CARE RELATED TO COMFORT MEASURES
Consider the expected outcomes for each comfort measure that is implemented