Systems Phys Exam 2 Study guide
1/108
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
109 Terms
What are the functions of blood? Transport, Regulation, Protection
Transport
O2 and nutrients to body cells
Metabolic wastes to lungs and kidneys
Regulation
Maintaining body temperature by absorbing and distributing heat
Maintaining normal pH
Maintaining adequate fluid volume in circulatory system
Protection
Preventing blood loss - Platelets initiate clot formation
Preventing infection
Antibodies
white blood cells
What is the composition of Blood?
45% RBC, 55% Plasma
What are the 3 types of blood
(formed elements)
Erythrocytes (RBCs), leukocytes (WBCs), thrombocytes (platelets)
Plasma contains
90% water, Nutrient, gases, hormones, wastes, proteins, dissolved solutes
Erythrocytes contain the protein____ to which O2 and CO2 reversibly combine
Hemoglobin
Types of Blood Vessels
arteries, arterioles, capillaries, venules, and veins
Arteries carry____ away from heart
Oxygenated blood
Veins carry___ to the heart
Deoxygenated blood
2 types of circulation
Pulmonary & systemic
Pulmonary circulation
carries oxygen poor blood and then returns oxygen rich blood
(think of lungs and its output)
System circulation
Caries oxygen rich blood and then returns oxygen poor blood
(Thing of blood flood after leaving heart)
Pressure in blood flow
force exerted by the blood; measured in mmHg
blood flows from higher to lower pressure
Flow in blood
Volume of blood moved per unit time; mL/min
Resistance in blood
difficulty for blood to flow between two points
measure of friction that impedes flow
Resistance Factors
Blood viscosity
Blood vessel length
Blood vessel radius
Blood Viscosity
Friction between molecules of a flowing fluid; affected by water volume and the number of erythrocytes
Blood Vessel radius’ effects
Dilated vessels decrease resistance, while constricted vessels increase resistance
Radii of blood vessels do not stay constant
Most important determinant of changes in resistance
Hematopoiesis
formation of all blood cells; in Red Bone Marrow
too few rbcs lead to hypoxia
Hematopoietic stem cells
(HematoCytoblasts)
Stem cell that gives rise to all formed elements
Erythropoietin (EPO)
Stimulates formation of RBCs; Released by kidneys in response to hypoxia
Hypoxia causes
Decreased RBC numbers
(due to hemorrhage or destruction)Insufficient hemoglobin per RBC (ex: iron deficiency)
Reduced O2 availability
(eg. altitudes, pneumonia,
lung problem)
RBC Composition
Heme, iron, globin
RBC component information
Iron bind to ferritin or hemosiderin; stored for reuse
Heme, degraded to yellow pigment bilirubin
Globin metabolized into amino acid, released into circulation
Bilirubin
Liver secretes Bilirubin into intestines; degraded to urobilinogen
Anemia
Low oxygen
O2 carrying capacity too low to support normal metabolism
not disease
Symptoms: fatigue, pallor, dyspnea, and chills
Polycythemia
Excess RBCS
increased blood viscosity
Polycythemia vera: Bone marrow cancer
Secondary polycythemia
low oxygen or increased EPO production
Leukocytes/WBCs
<1% total blood volume
defend against disease
Originate from hemocytoblast stem cells
Leukocytosis
WBC count higher than usual, → response to infection
Leukocytes grouped into two categories
Granulocytes
Agranulocytes
Granulocytes
Contain cytoplasmic granules
Neutrophils, eosinophils, Basophiles
Agranulocytes
No cytoplasmic granules
Lymphocytes
monocytes
Lymphoid stem cells
produce lymphocytes
Leukopenia
Low WBC count
Leukemias
Bad WBCs
Cancerous condition involving overproduction of immature, nonfunctional, & abnormal WBC
Cancer cells fill red bone marrow, leading to anemia & bleeding
Treatments: irradiation, antileukemic drugs; stem cell transplants
Thrombocytopenia
Deficient number of circulating platelets
treatment: transfusion of concentrated platelets
Thrombocytopenia: Impaired liver function
Inability to synthesize clotting factors
caused by: vitamin K deficiency, hepatitis
What is a thrombus
Clot
May block circulation, leading to tissue death
Embolus
ex: pulmonary or cerebral emboli
risk factors: atherosclerosis, slowly flowing blood or blood stasis from immobility.
Plaque in blood stream
Pathway of blood
Vena Cava → Right A → Tricuspid → Right V → Pulmonary Valve → Pulmonary trunk → R/L Pulmonary artery → Lungs → R/L Pulmonary veins → Left A → Bicuspid valve → Left V → Aorta → Body
Types of Cardiac Muscle cells
Contractile & Pacemaker cells
Contractile cells
responsible for contraction
Pacemaker cells
noncontractile cells that depolarize; Do not need nervous system stimulation
All cardiomyocytes contract as unit, or none contract
contraction of all cardiac myocytes ensures effective pumping action
Coordinated heartbeat is a function of
the presence of gap junctions
Intrinsic cardiac conduction system
Network of noncontractile (autorhythmic) cells
initiate &distribute impulses to coordinate depolarization and contraction of heart
Sequence of Excitation
Cardiac pacemaker cells pass impulses, in order
SA node → AV node → AV bundle → R & L bundle branches → Purkinje fibers
SA node (Pacemaker)
Generates impulses about 75x / min (Sinus Rhythm)
Av node
If defective, may cause a heart block: Too slow to maintain adequate circulation
Treatment: Artificial pacemaker (recouples atria and ventricles)
Benefit of longer AP and contraction
Sustained contraction ensures efficient ejection of blood
Contractile muscle fibers
make up bulk of heart muscle and are responsible for pumping action
Steps in AP of contractile cardiac muscle cells
Depolarization: Na+ influx, opens Na+ channels
Plateau phase: Ca2+ influx, K+ channels closed
Repolarization: Ca2+ inactivate, K+ channels opening
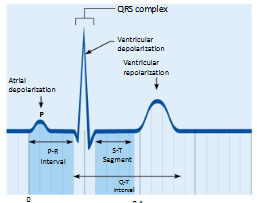
Waves of EKG
P wave
QRS Complex wave
T Wave
P-R interval of EKG
Beginning of atrial excitation to beginning of ventricular excitation
S-T Segment of EKG
Entire ventricular myocardium depolarized
Q-T interval of EKG
Beginning of ventricular depolarization through ventricular repolarization
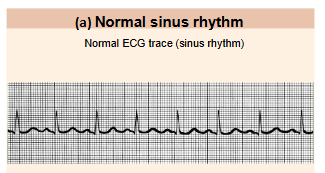
EKG of heart
remember both, this bottom one is related to top one
Electrocardiogram(ECG or EKG)
Composite of all action potentials at given time
EKG detects
Enlarged R waves - indicate enlarged ventricles
Elevated or depressed S-T segment - indicates cardiac ischemia
Prolonged Q-T interval reveals - repolarization abnormality that increases risk of ventricular arrhythmias
Systole
Period of heart contraction
Diastole
Period of heart relaxation
Cardiac cycle
Blood flow through heart during one complete heartbeat
Atrial systole & diastole; followed by ventricular systole & diastole
Ventricular Ejection Fraction
Ejection Fraction = (Stroke volume / End-Diastolic Volume) x 100%
ventricular contraction
when blood is forced out of ventricles
Isovolumetric contraction Steps
Atria relax; ventricles contract
Rising ventricular pressure; AV valves close
Split second period: Ventricles close, volume remains constant, ventricles continue contracting
Valves open when ventricular pressure exceeds large artery pressure
Isovolumetric Ventricular Relaxation Early Diastole
Ventricular repolarization (T wave); Ventricles relax
End-Systolic Volume
Ventricular pressure drops causing backflow of blood
Ventricles completely closed
Isovolumetric Ventricular Relaxation Mid
Ventricles relax, no blood is entering or leaving ventricles
AV Valves are closed, no change in volume
Ventricular Filling
AV valves open, blood flows from atria into ventricles
Atria contracts at end of diastole; 80% of filling occurs passively before atrial contraction
Heart Sounds
Lub-Dup: closing of heart valves
Lub (1st sound): Closing of AV valves at beginning of ventricular systole
Dup (2nd sound): Closing of SL valves at beginning of ventricular disatole
Extra Heart sounds
Heart murmurs
S3 (volume problem
S4 (pressure problem)
Cardiac Output
Amount of blood pumped out by each ventricle in 1 minutes (Liters/min)
Cardiac output equation
CO = Heart Rate x Stroke Volume
What is Stroke Volume
The amount of blood ejected by each ventricle during a single heartbeat.
SV = EDV (120mL) - ESV (50 mL) = 70 mL/beat
3 Main factors affecting Stroke Volume
Preload
Changes in the EDV
Contractility
changes in the magnitude of sympathetic nervous system input to the ventricles
Afterload
Changes in afterload, the arterial pressures against which the ventricles pump
Venous Return
rate of blood flow back to the heart’s right atrium
Contractility
Increased contractility lowers ESV which is caused by
Epinephrine release stimulates increased Ca2+ influx, leading to more cross bridge formations
Afterload
Back pressure from arterial blood pushing on SL valves
Aortic pressure is ~80 mmHg
Pulmonary trunk pressure ~10 mmHg
Hypertension increases afterload, resulting in increased ESV and reduced SV
Hypertension ______ afterload, resulting in increased ESV and reduced SV
increases
Tachycardia
HR >100 beats/min
Bradycardia
HR slower than 60 beats/min
Congestive heart failure (CHF)
CO is so low that blood circulation is inadequate to meet tissue needs
Coronary atherosclerosis
Heart becomes hypoxic, contracts inefficiently
Persistent high BP
Causes myocardium to exert more force (weakens myocardium)
Chronic increased ESV causes myocardium hypertrophy and weakness
Dilated cardiomyopathy
Ventricles stretch, become flabby, myocardium deteriorates
Cardiac Output Imbalance of Heart
Left side failure = Pulmonary congestion
Right side failure = Peripheral congestion
Known as Edema
Failure of either side weakens the other side
Treatment: removal of fluid, drugs to reduce afterload and increase contractility
Pulmonary congestion
Blood backs up into lungs
Only left side heart failure
Peripheral congestion
Blood pools in body organs
Called edema, only on right side of heart
Arteries
Oxygenated blood away from heart except when it comes to the pulmonary artery, which carries deoxygenated blood
Veins
Deoxygenated blood to heart except for the pulmonary veins
Capillaries
Exchange of gases, nutrients, wastes, hormones, etc
Flow of blood
Arteries → Arterioles → Capillaries → Venules → Veins
Blood Pressure from aorta to vena cava
Blood pressure decreases from Aorta to Vena Cava
Diastolic and Systolic pressure come together at the arterioles
Mean arterial pressure
Pressure that propels blood to tissues
MAP calculated by DP + PP
Diastolic + Pulse pressure
Pulse Pressure formula
PP = SP - DP
Systolic pressure - Diastolic pressure
Tunica Intima
Intimate contact with blood
Tunica Media
Of smooth muscle and elastin
Sympathetic vasomotor nerve fibers innervate this layer, controlling
Vasoconstriction
Vasodilation
Bulkiest layer responsible for maintaining blood flow and blood pressure
Tunica externa
Outermost layer of wall
Loose collagen fibers that protect and reinforce wall and anchor it to surround structures
Compliance
Volume/Pressure
Higher compliance means it is easily stretched