Lecture 15 - Evaluating BEVs and Skin Renderings
1/55
Earn XP
Description and Tags
ONCOL 306 - Imaging. University of Alberta
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
Treatment to the breast can be targeted towards which two regions?
whole breast (after lumpectomy)
chest wall (after mastectomy)
What are the potential 4 beams that are used in breast treatment
two tangent beams which run across the breast tangentially
± AP/PA to treat supraclavicular nodes
How does the dose differ based on if whole breast or chest wall is being treated
lumpectomy = 4250 cGy
chest wall = 4500-5000 cGy
how is the treatment set-up for breast different than other treatment sites?
breast treatments are clinical set-ups, meaning the RTTs need to visually verify the position of the target before imaging
what are the three steps of the clinical set-up done before imaging?
compare the light field on the patient to skin renderings
verify clearange of the light field over breast anteriorly
confirm chin and arm positions (not in the light field)
what treatment technique is often added to the tangent fields to boost certain parts of the field while keeping other parts of the initial field colder?
field-in-field technique

why is the lung typically within the treatment field for breast tangential treatments?
lung is needed within the treatment field to ensure we are able to cover all of the desired breast tissue
what 4 borders on the light field need to be compared to the skin renderings?
medial border of medial tangent field
posterior border of lateral tangent field
superior and inferior borders of both tangent fields
where should the medial, superior and inferior borders lie on with the medial tangent field?
medial = pretty much mid sternum
superior = above where breast tissue is falling and just below clavicular head
inferior = 1.5-2 cm below breast tissue
where should the posterior border lie on with the lateral tangent field?
visualize the breast tissue isn’t falling laterally below mid clavicular line
the lumpectomy scar will also be used as a landmark if needs to be in the light field or not
what two pieces of information do skin renderings provide about the patient and treatment plan?
information about the patient’s breast position
does the breast fall laterally when she is lying down (could present set-up challenge)
information about field borders
where they lie, if IM nodes are being treated, if post. borders include all of scar, how tight superior border is (may require extra attention to ensure breast doesn’t fall too sup)
what is the purpose of field localization
localization means we are looking to make sure the isocenter is placed at the right location
can be confirmed with BEVs before tx to ensure field falls right into treatment field (talked about later)
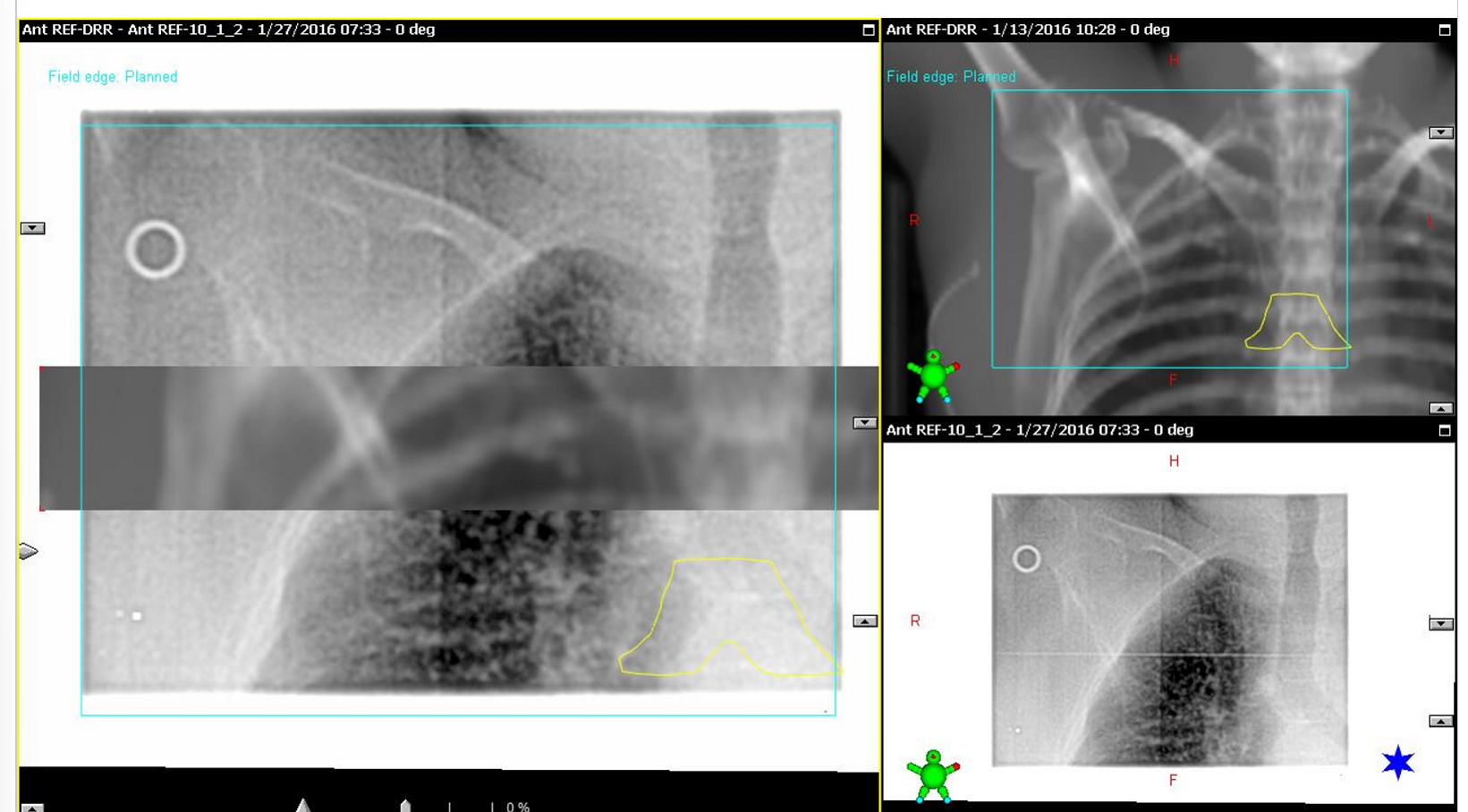
what set of images are done for field localization in breast treatments?
orthogonal reference images: often ANT and LAT images
taken at vertical and horizontal planes
after taking your othogs, what are always the first two steps when looking at the image
assess image quality, anatomy, and positioning
perform image match using primary and secondary structures

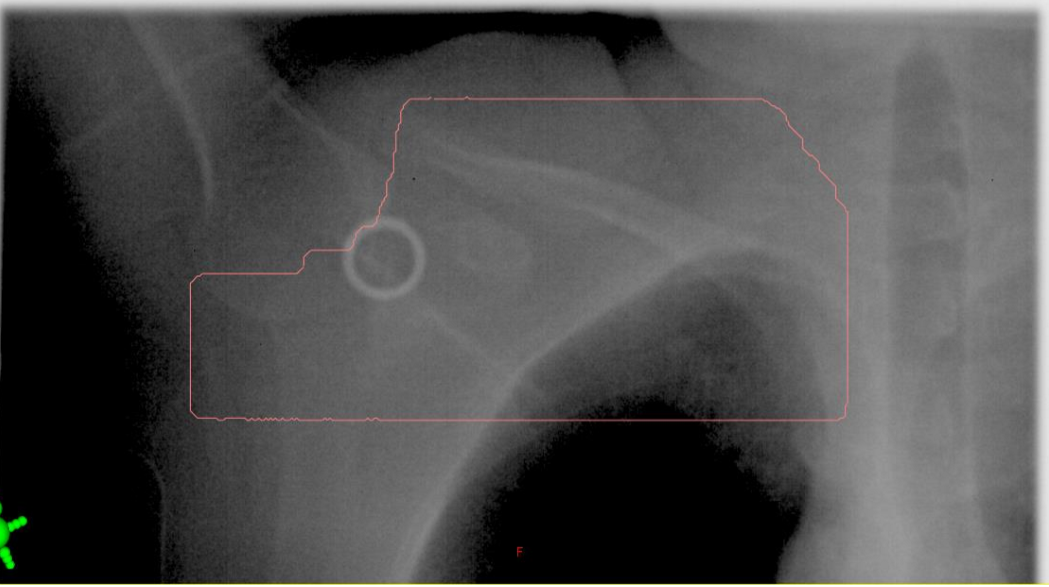
what does the wire define on the x-ray imaging?
wire defines the surgical scar
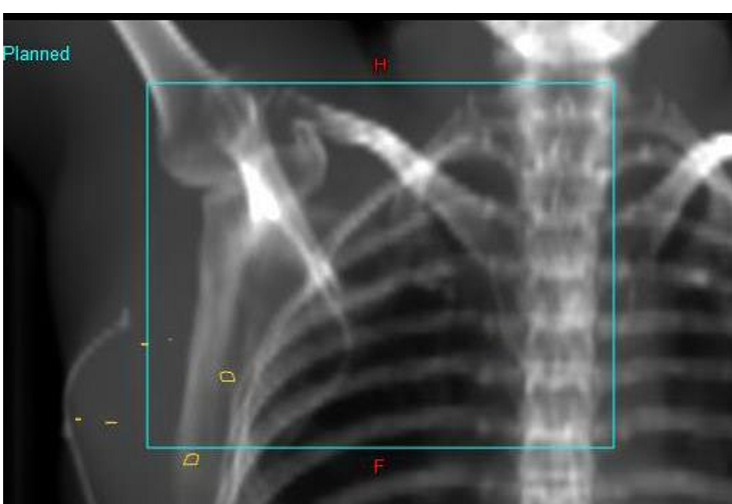
what are the yellow contours on the image?
contours placed by dosimetry to mark the site of surgical clips
What are the primary and secondary match structures for Sup/Inf for breast treatments
primary = clavicle head - sternoclavicular joint region
secondary = intervertebral spaces, apex of lung, ribs, carina
what may be used in conjunction with the clavicle head to get match exact?
the intervertebral spaces
what are the lateral primary and secondary match structures for breast treatments
primary = thoracic vertebrae (lateral edge or spinous processes)
secondary = rib cage / heart shadow
how much of the thoracic vertebrae should be used when doing lateral match and why?
use as much of thoracic spine as possible as the target volume is quite long
what are the Ant / Post primary and secondary match structures for breast treatments
primary = sternum (especially for DIBH techniques): manubrium / sternal body or anterior edge of thoracic vertebrae
seconday = anterior edge of thoracic vertebrae or sternum (whatever you didn’t use as primary, use as secondary)
why is the contoured carina added on to the DRR
because the carina is not well visualized without it
what is used for field confirmation after the kV-kV image match?
BEV - treatment field images
typically MV image quality
are BEVs used for field localization?
no, they do not provide orthogonal information so they cannot be used for field localization
at what angle and MLC set-up are BEVs taken at?
taken at the treatment angle wit the MLC in place
important: what 4 things are we evaluating with the BEV image assessment
MLC shielding (in relation to the patient)
lung volume
treatment field clearance (sup, inf and ant) around the breast
bolus if applicable
BEVs are not used for field localization, but they are used to verify / confirm …
verify and confirm position of the treatment beam
what imager is used to take the BEV image
MV EPID imager
this is done to ensure field borders and MLC are within the image

what are the two ways to evaluate the lung inclusion within the MLC?
use moving window and make lung match
don’t use moving window and just look at where the apex of the lung hits the posterior border of the contour
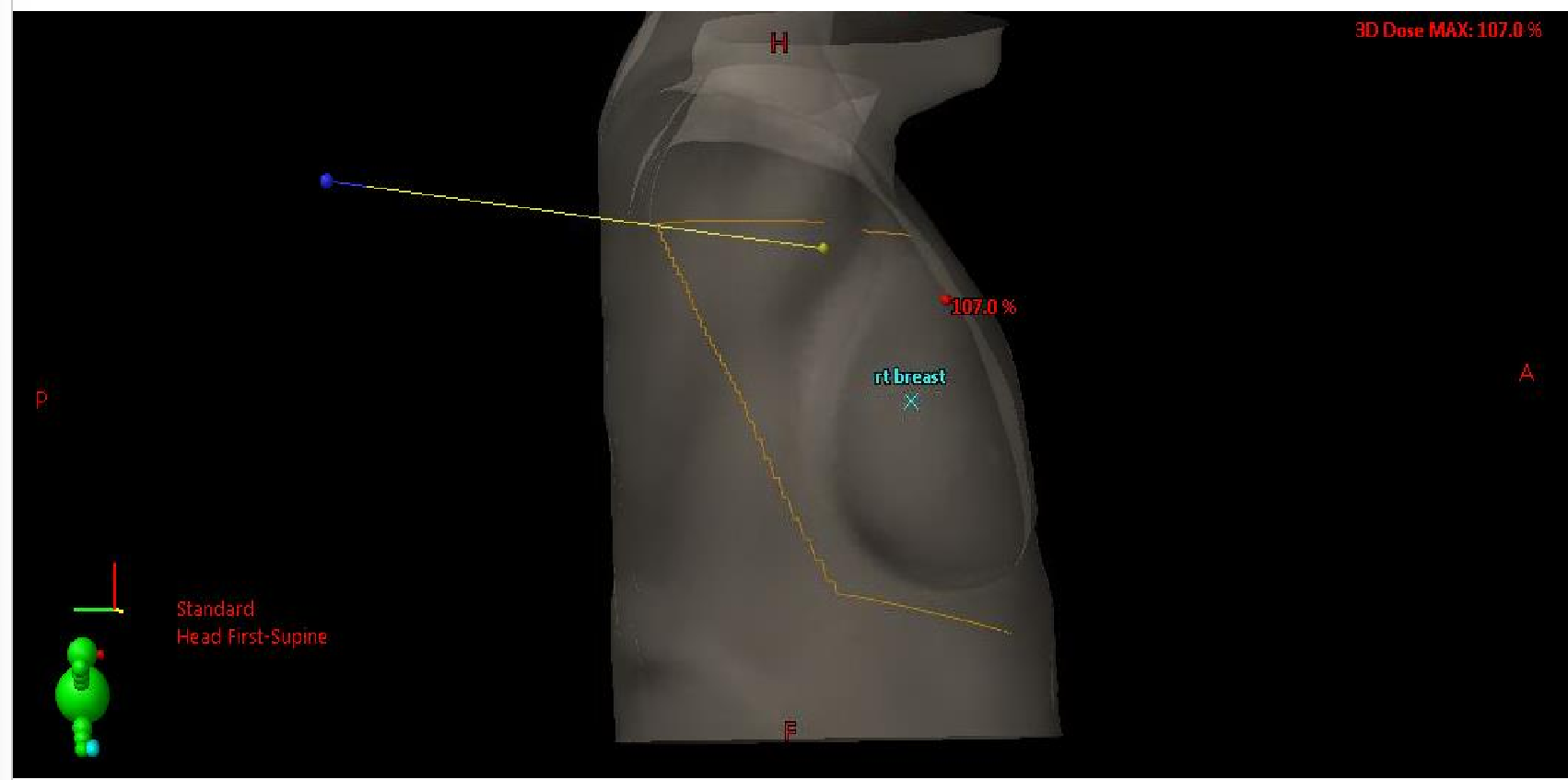
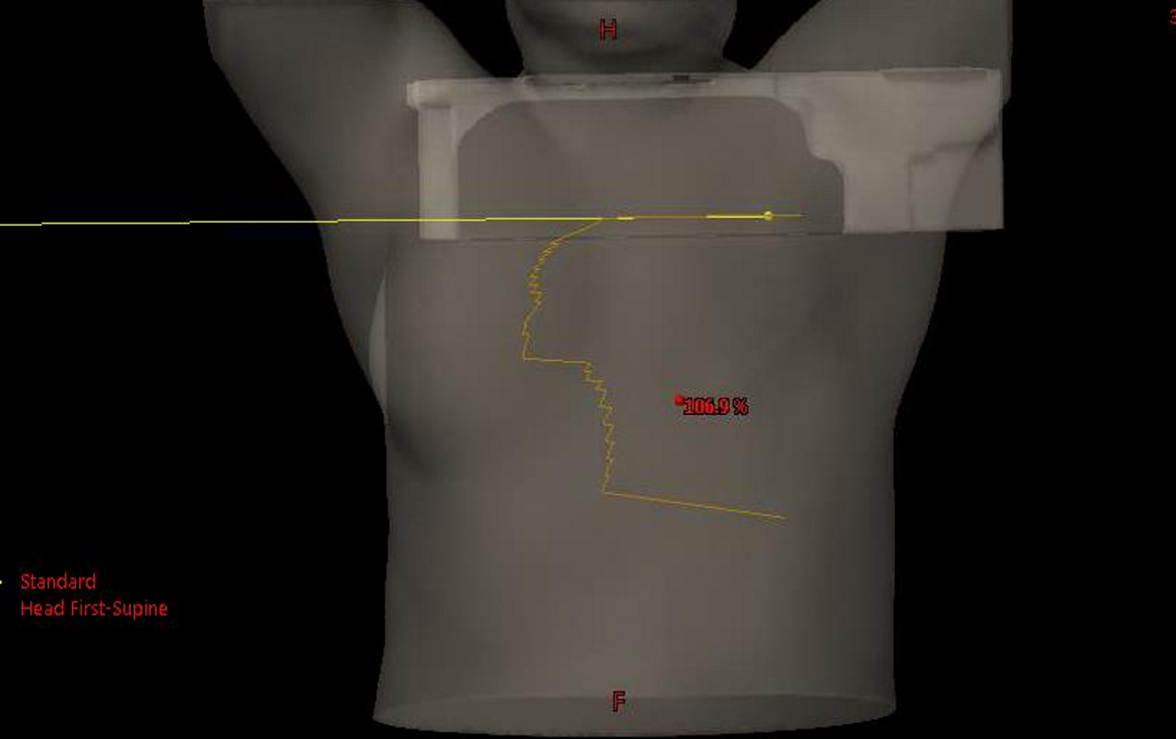
What are skin renderings used for?
for initial field and set-up confirmation BEFORE imaging
what are orthogonal kV/kV used for?
for field localization (isocenter placement)
what are MV EPID BEVs used for?
for field confirmation
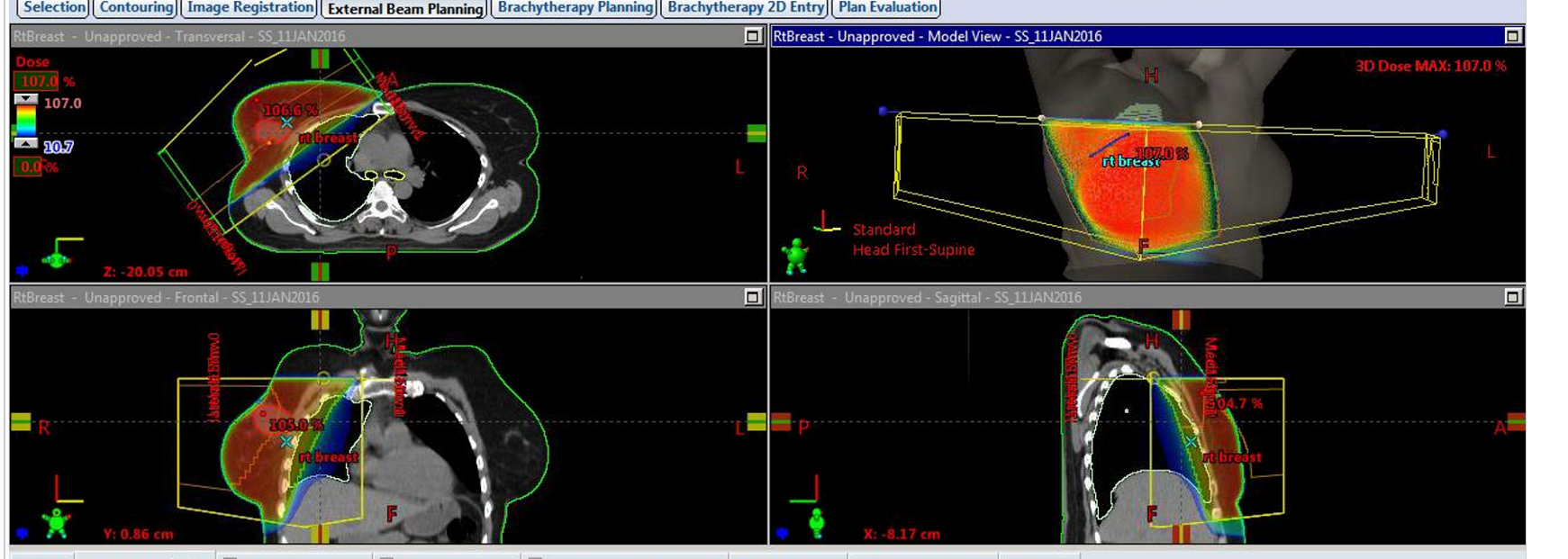
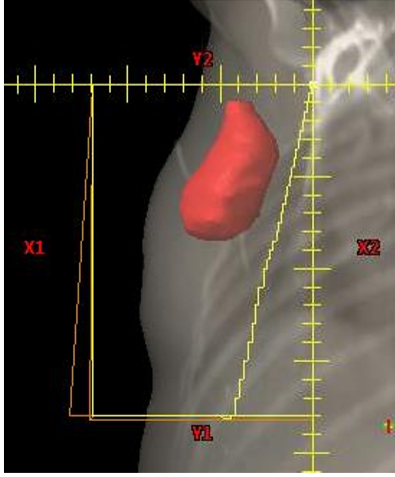
what is one thing that may be an issue with this patient’s two field tangential treatment
patient has larger breast, so we must check the lateral skin rendering to ensure that the breast is following accurately
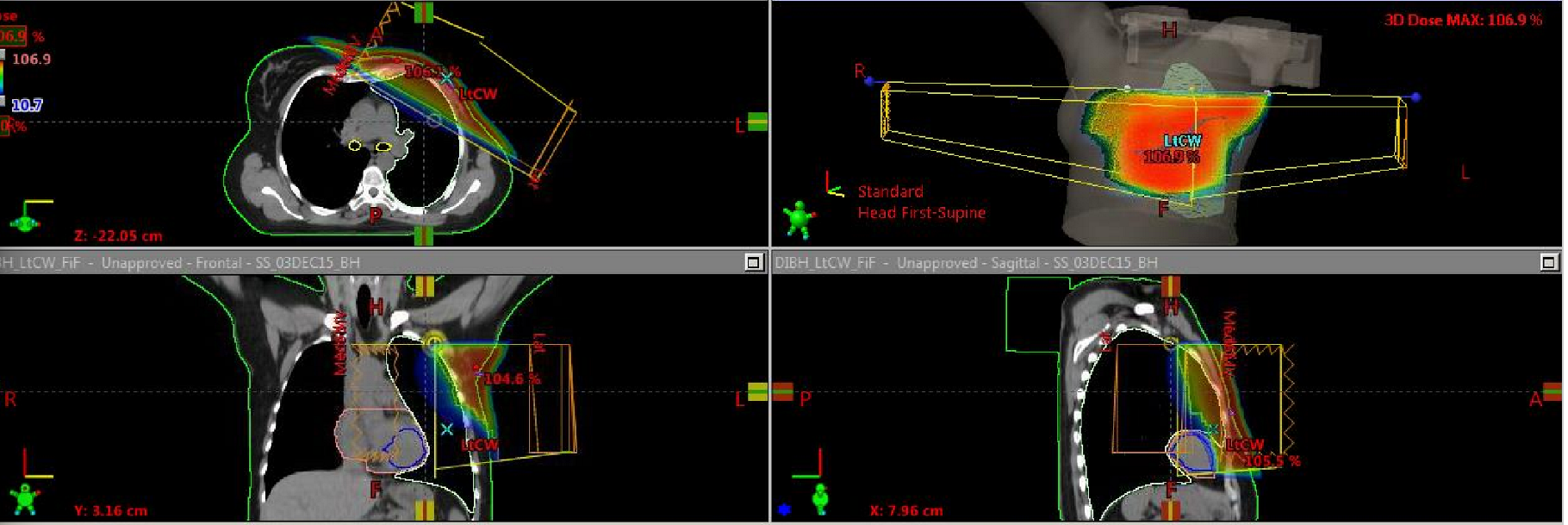
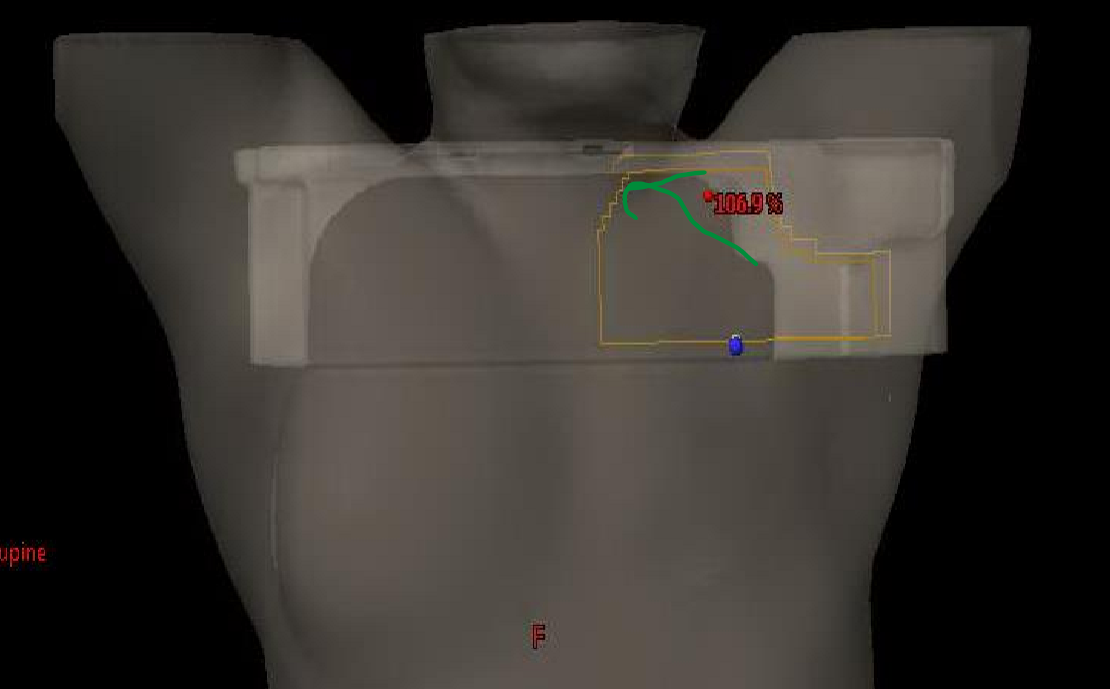
What type of surgery has this patient had? Would we expect bolus?
patient has had a mastectomy so the breast has been removed
we are treating the chest wall so we would expect there would be bolus present

are the AP/PA supraclav fields exactly ant and post? if not what are they?
AP field is angled 10 degrees to ensure the radiation does not diverge into the esophagus
the PA field is placed at 170 degrees to match the divergence of the AP field to minimize dose into spinal cord, esophagus, etc

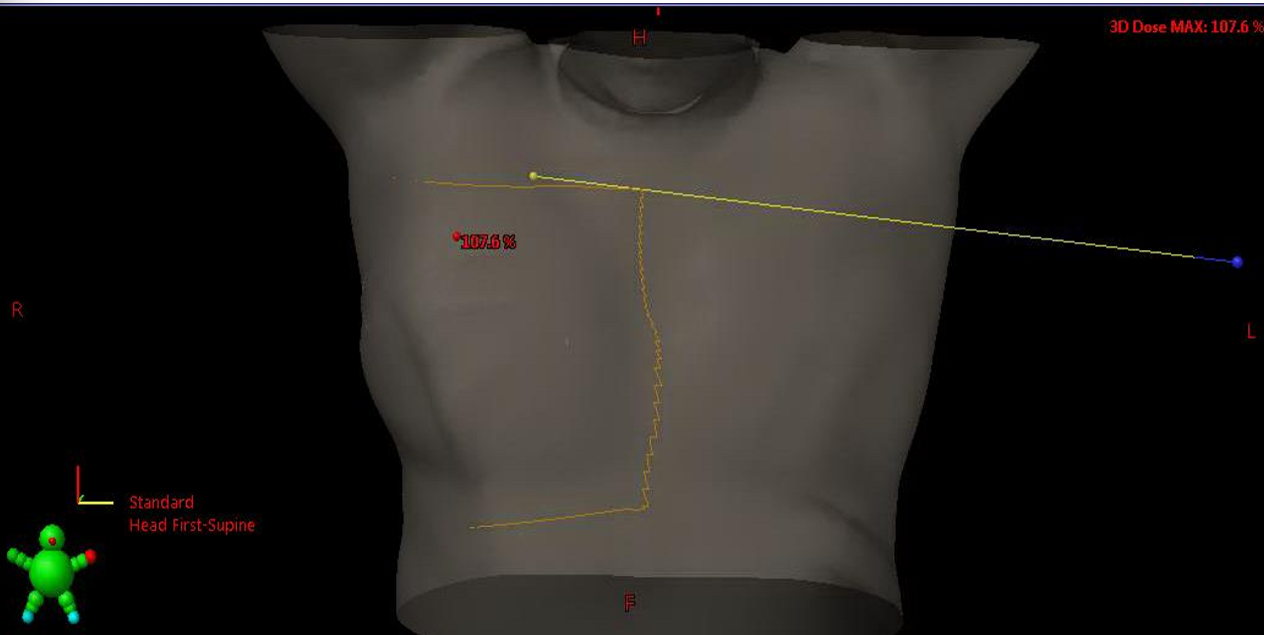
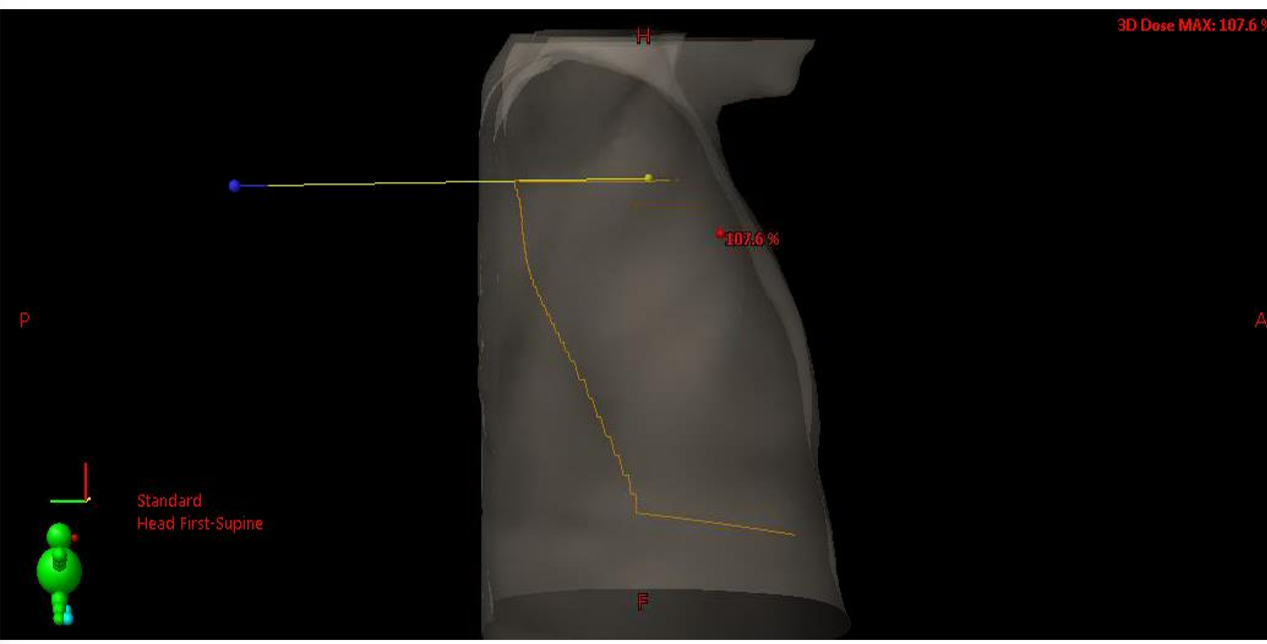
What does the FLASH extending to the contralateral breast tell us about what we are treating?
FLASH is clearing the opposite breast because we are treating the IMC nodes
within intercostal spaces 1-3
when doing our medial BEV check for a chest wall patient? what are two things we are looking for
we want to check the posterior MLC, making sure there is same amount of lung in each
also we want to do a bolus assessment to see it is conforming nicely
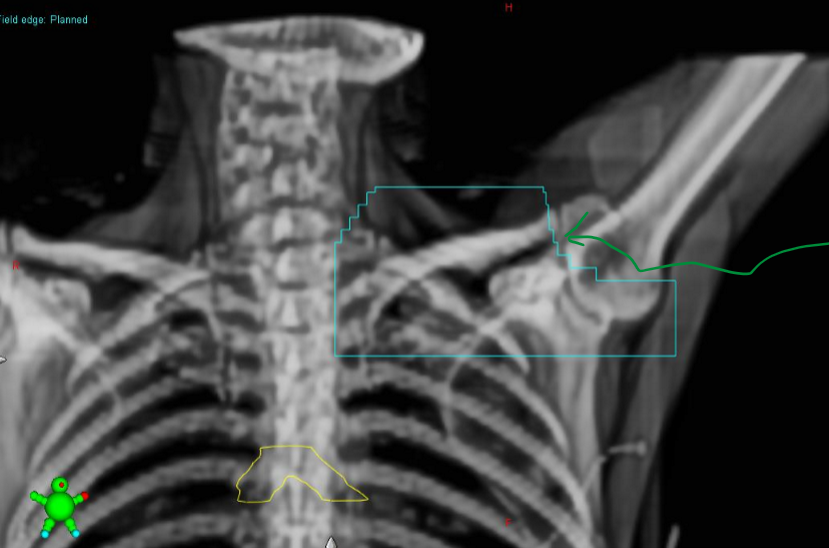
what are the MLCs the arrow is pointing to shielding?
we are shielding the thyroid
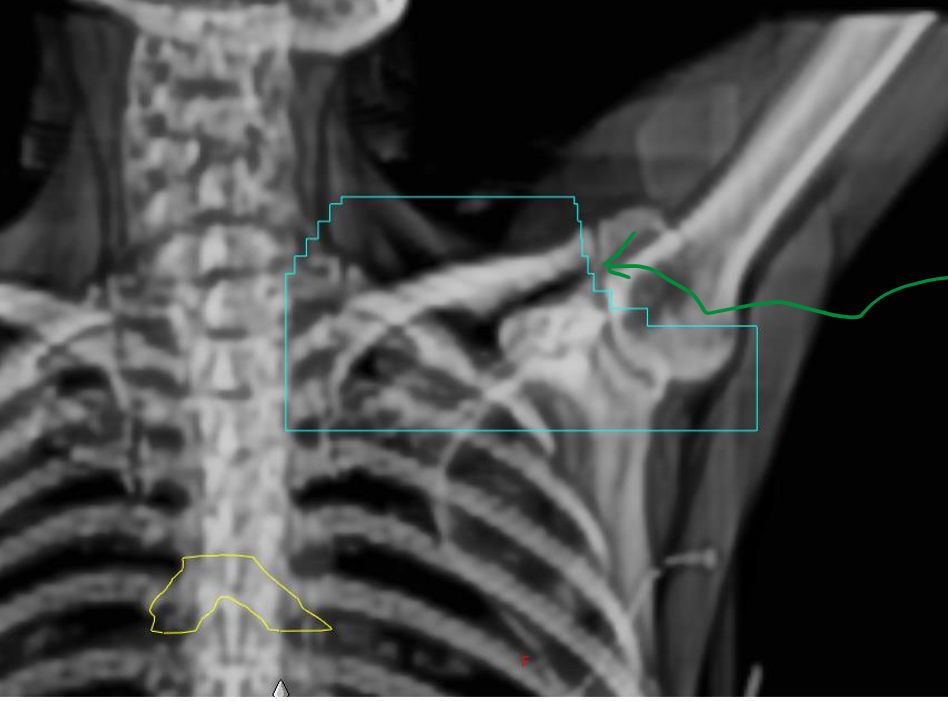
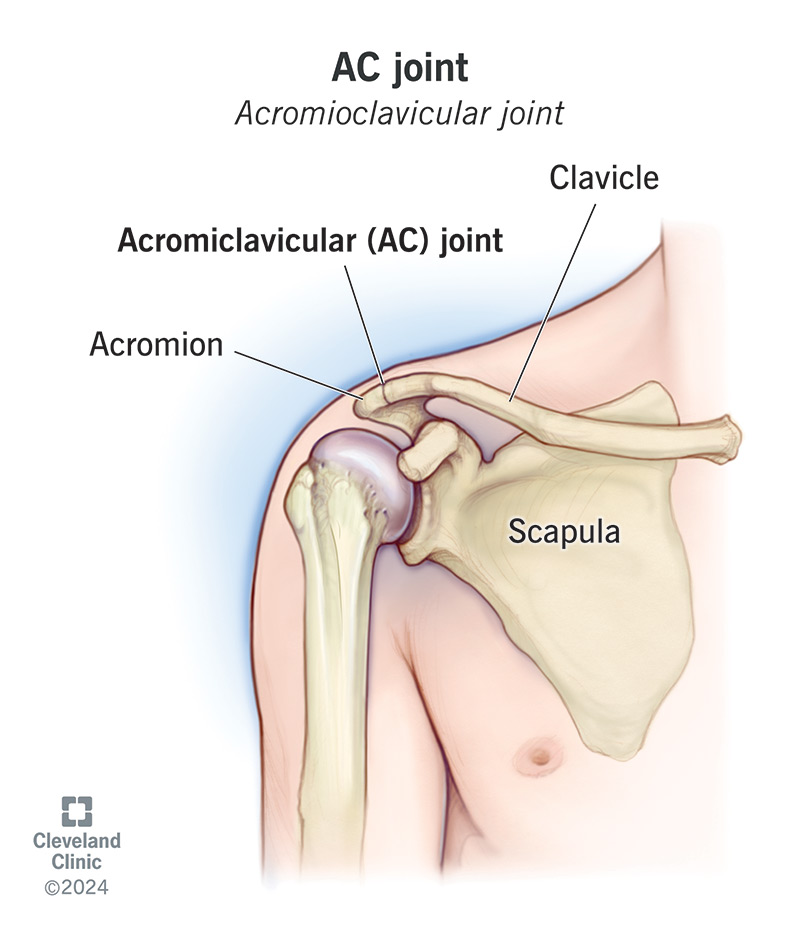
what are the MLCs the arrow is pointing to shielding?
what two lymphatic nodes are being included in the BEV?
we are shielding the acromioclavicular joint
two nodes: supraclavicular and axillary nodes
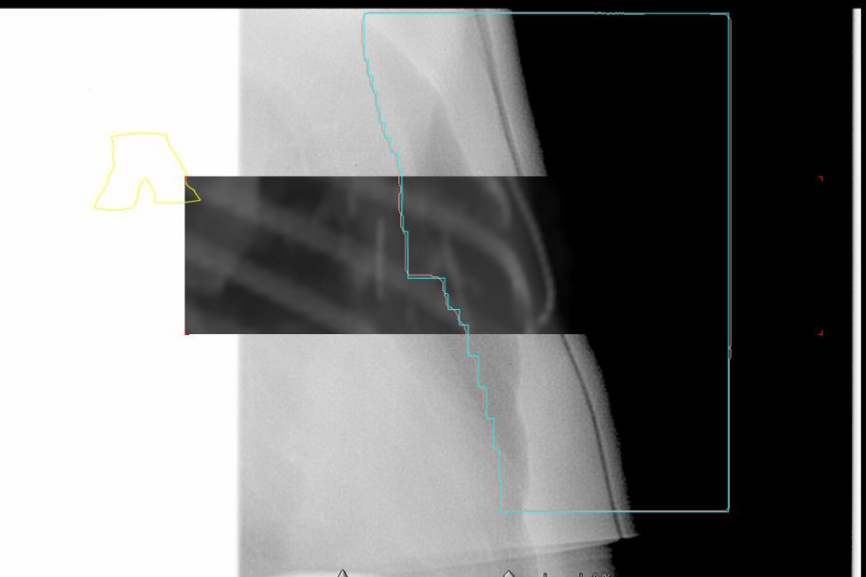
on a supraclav BEV, what three thing are we assessing?
arm position (see clavicle and humoral head)
field borders relative to patient anatomy (sup, inf, medial, lateral)
MLCs relative to the patient’s anatomy
when looking at a supraclav BEV, do we assess lung volume?
NO, it is irrelevant on this field, just assess the field borders
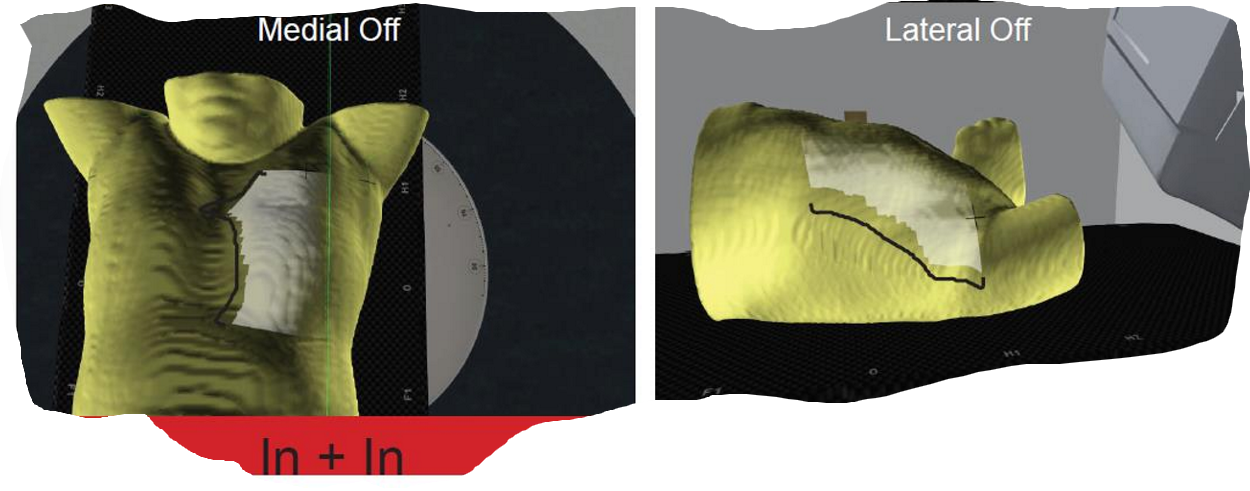
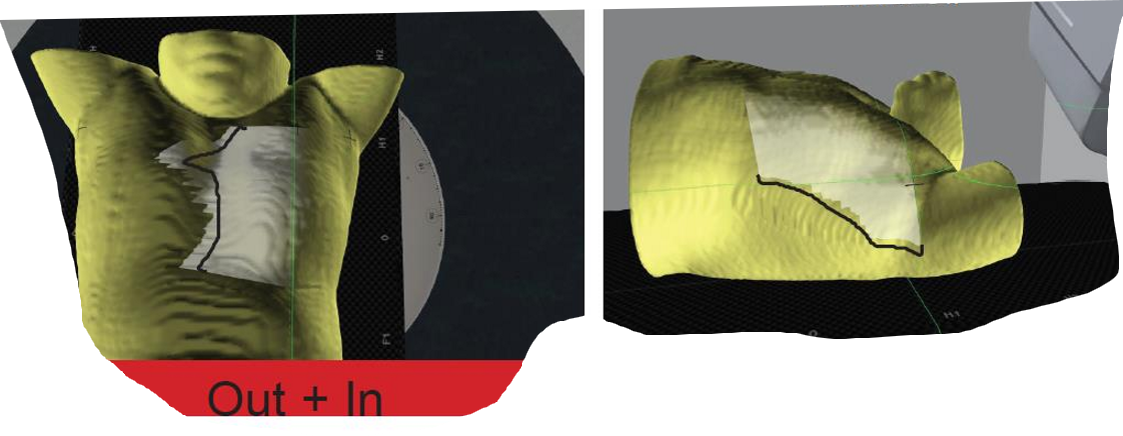
if our field light is ‘in + in”, what two things is that telling us about our isocenter?
our isocenter is either too lateral OR too anterior
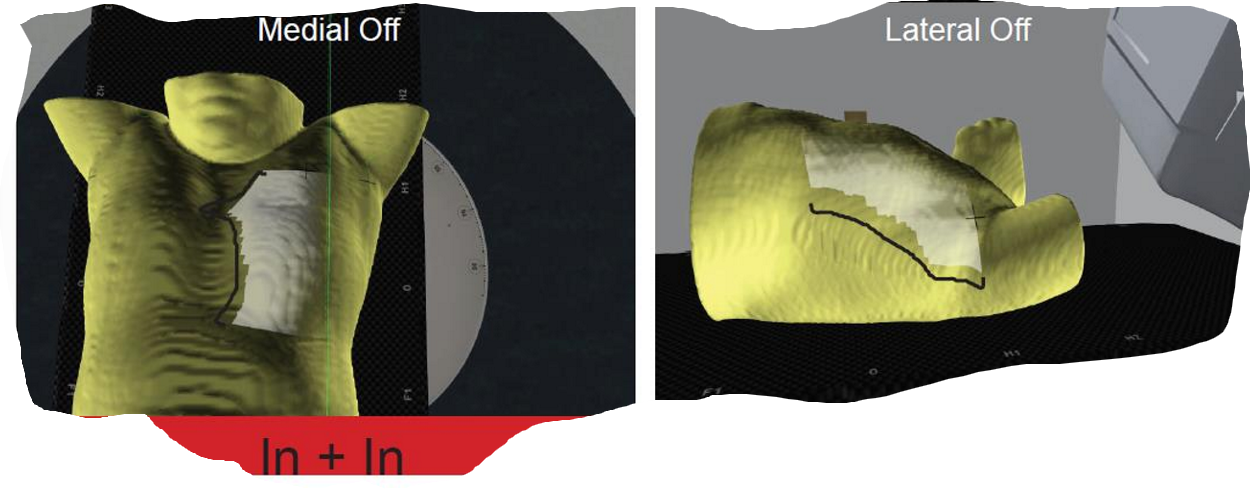
what two ways could we correct our isocenter being too lateral or too anterior
move the patient laterally
move the patient anterior to make the isocenter fall more posterior
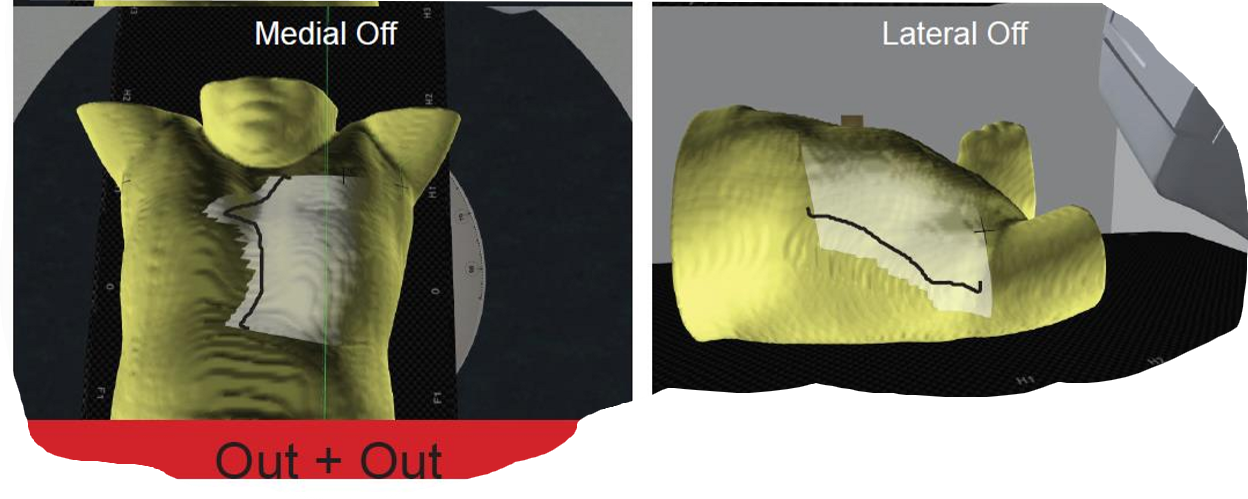
if our field light is “out + out”, what two things is it telling us about our isocenter
our isocenter is either too medial OR too posterior
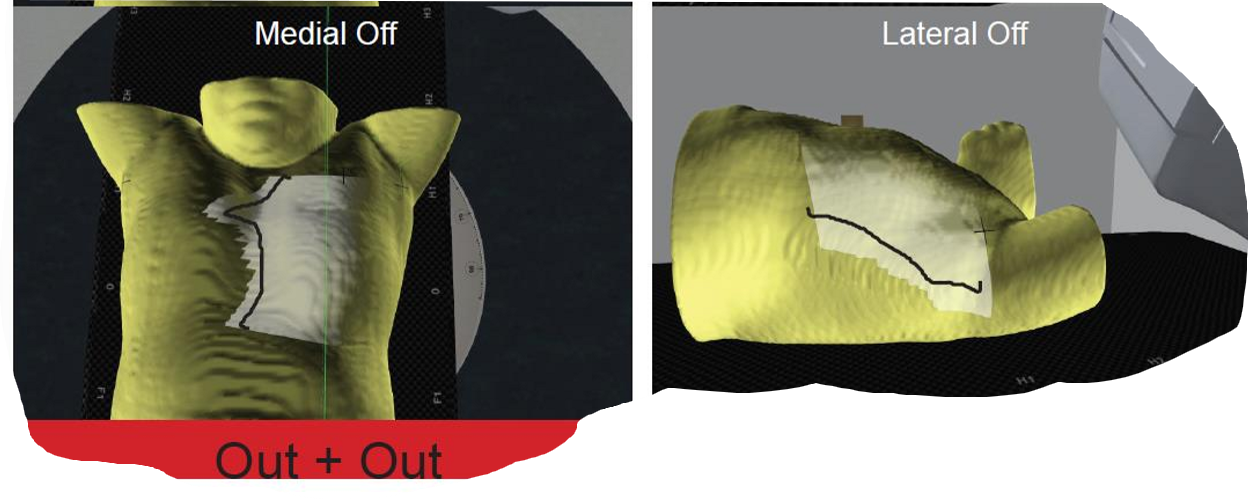
what two ways could we correct our isocenter being too medial or too posterior
move the patient medially
move the patient posteriorly to move the isocenter more anteriorly
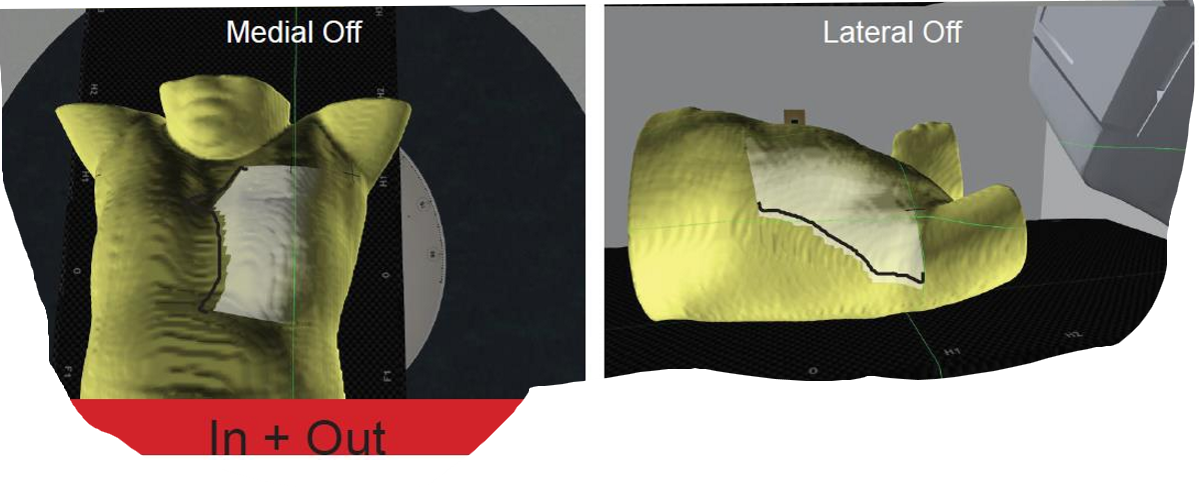
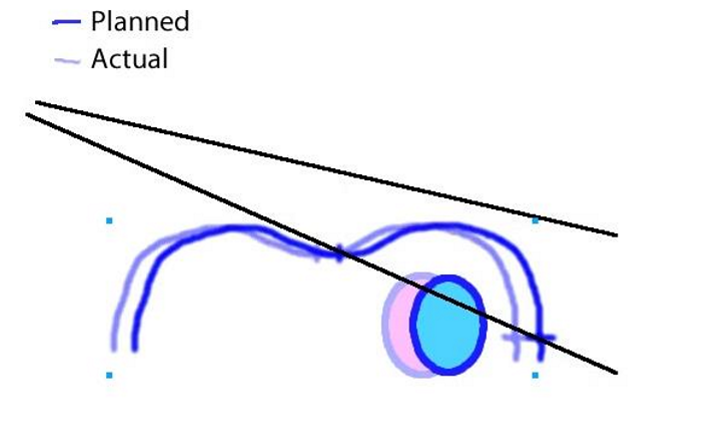
If our field light is in medially and out laterally, what does that tell us about our patient positioning?
our patient has a roll, and their contalateral breast is more anterior than the treatment side

how would we fix our patient if the field light was in medially and out laterally?
we would rotate the treatment side down: the therapist would rotate roll from the patient’s contralateral side
if our field light was out medially and in laterally, what does that tell us about our patient’s positioning
our patient has a roll, and their treatment breast is more anterior than the contralateral side

how would we fix our patient if the field light was out medially and in laterally
we would rotate the treatment side up: the therapist would rotate roll from the patient’s treatment side

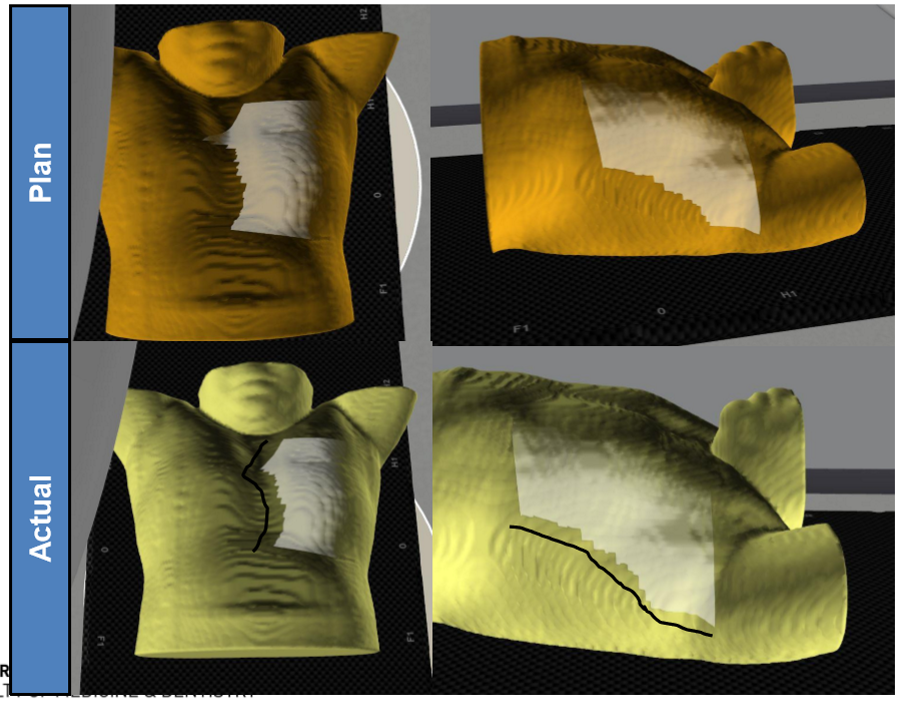
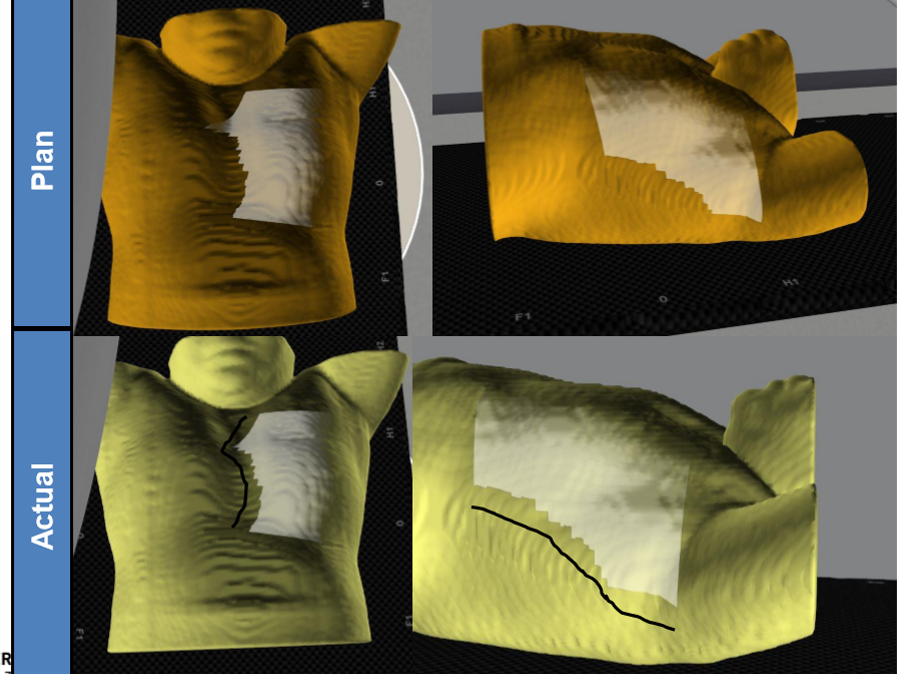
what is the positioning error? what impact does it have on the lung volume treated?
the patient was set up with a roll: the patient’s treatment side was elevated
the volume of lung receiving radiation has increased
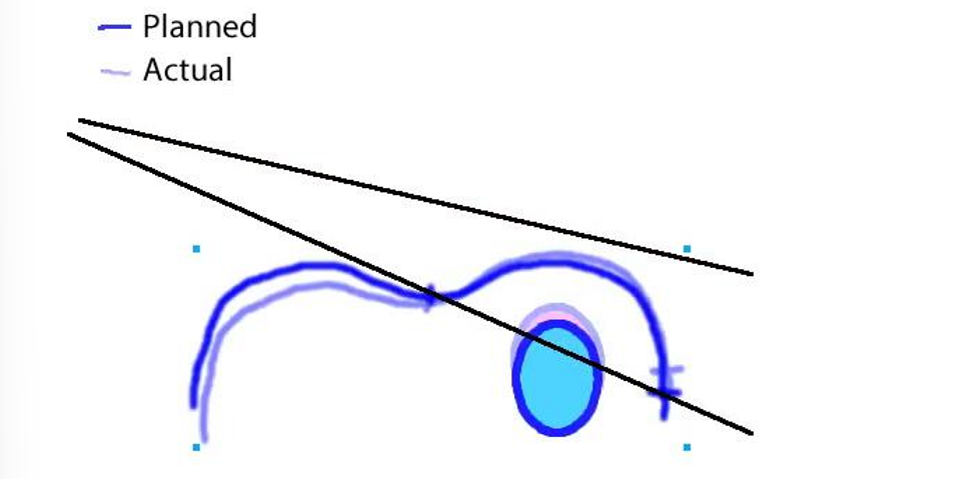
on a BEV, how would a patient roll error (as seen on previous flashcard) look?
more lung is visable within the BEV

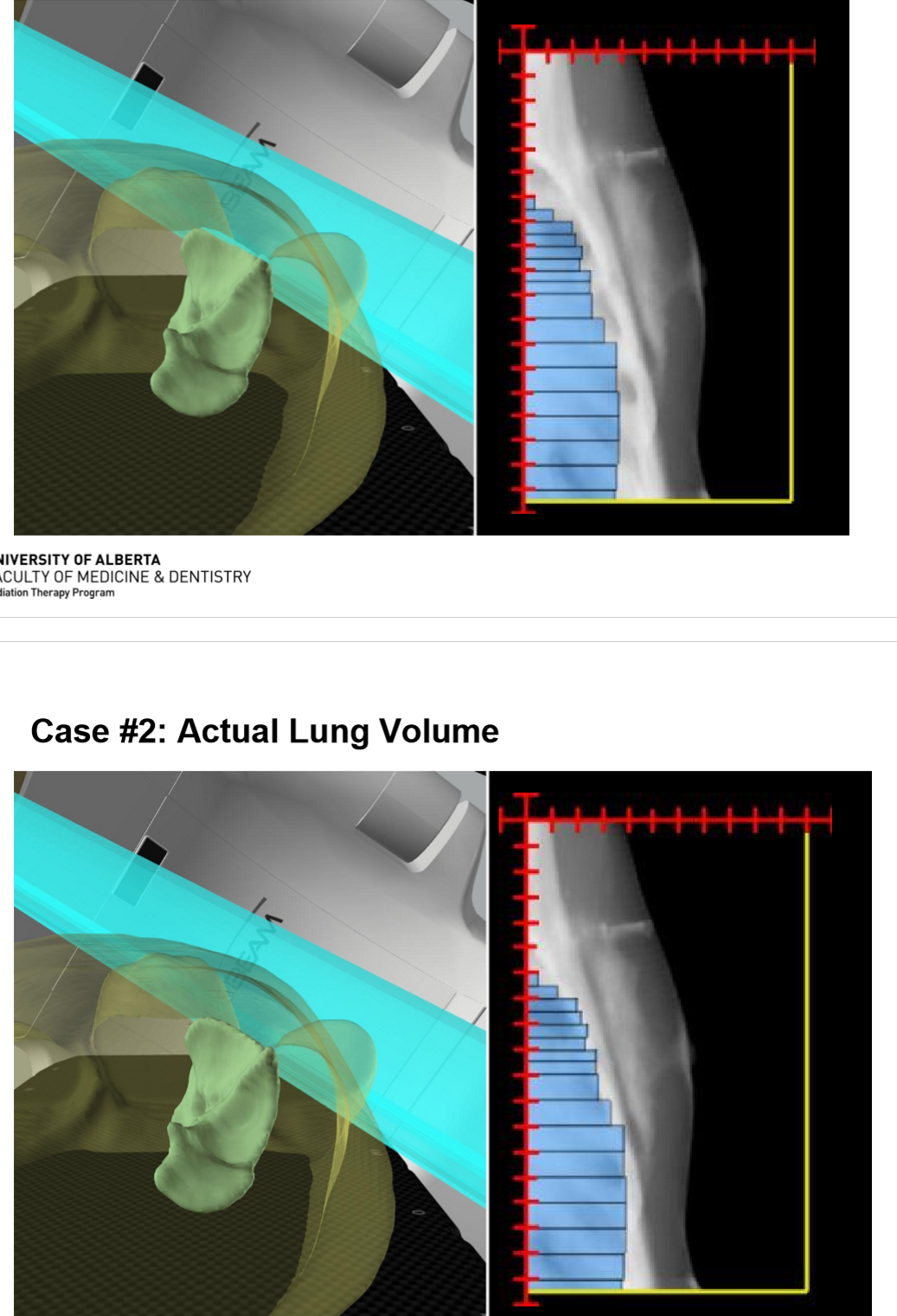
assume the patient’s lateral is correct, what is the positioning error? what impact does it have on the lung volume treated?
the isocenter is too anterior (so the patient is too posterior)
the lung is actually receiving less dose than it should be (because there is not enough CW coverage)
on a BEV, how would an anterior isocenter (patient posterior) error look?
in the actual lung volume, there is less lung emerging anterior to the MLCs then what was orignally planned
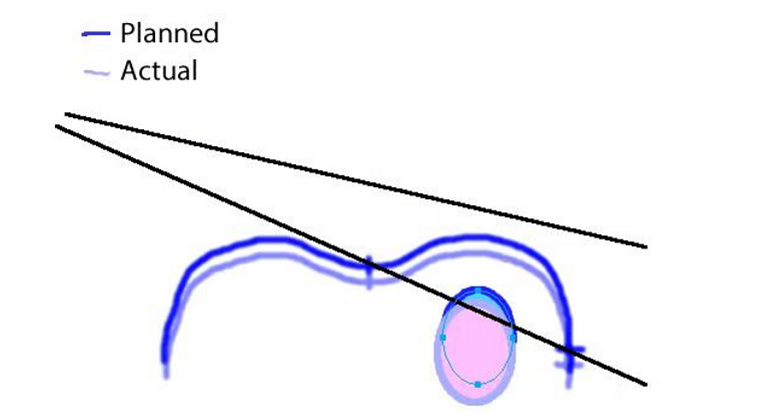
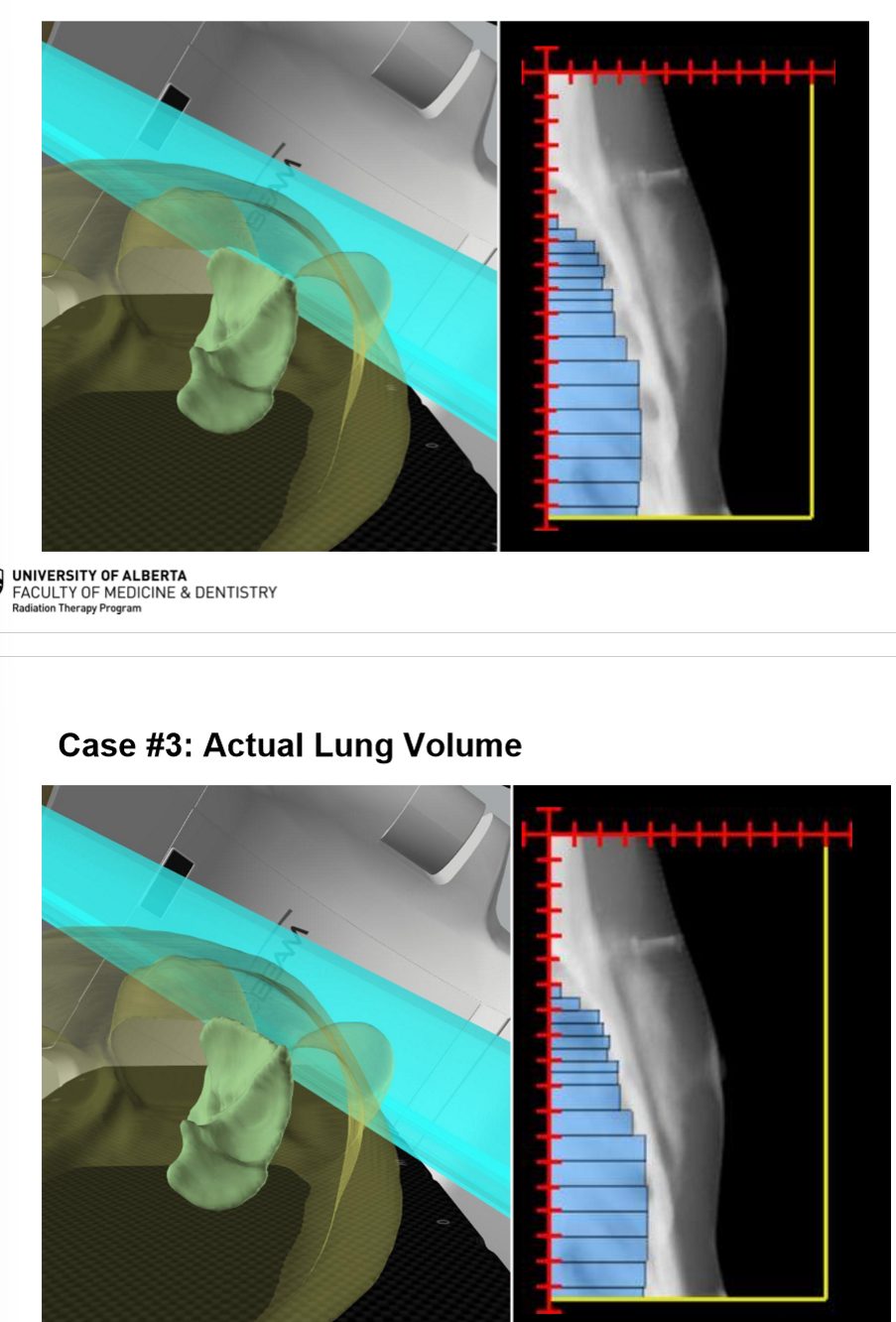
assume the patients A/P is set properly, what is the positioning error? what impact does it have on the lung volume treated?
the isocenter is too lateral and the patient is too medial and the lung is actually getting less dose then what is planned
On a BEV, how would a lateral isocenter (medial patient) look?
less lung irradiated than what was planned
what are the 5 general steps of doing a breast image match?
assess image quality - make adjustments as needed (AP/Lat)
Assess anatomy and identify any foreign structures / objects
determine the best primary and secondary match structures
perform image match
evaluate the BEVs