Clinical ex. Phys CH. 25
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
what is osteoporosis
Skeletal disorder characterized by compromised bone strength, predisposing individuals to an increased risk of fracture
Osteoporosis mean bone mineral density (BMD) is..
2.5 standard deviations below the mean (T-score -2.5)
Osteopenia
less severe form of disease
in osteopenia, BMD score is
BMD T-score is between -1 and -2.5
Fracture risk assessment (FRAX) does not just look at ___. They also look at
BMD.
Age, gender, use of oral glucocorticoids (GCOP), history of fracture
what are utilized and calculated in a fracture risk assessment (FRAX)
Risk factors are utilized in an algorithm (with or without BMD) and a 10 year probability of fracture is calculated
FRAX is not validated for use under the age of
40
FRAX does not show to be a better predictor of fracture over, only...
give an example
BMD classifications of osteoporosis vs. osteopenia alone
ex. many with osteopenia will experience a fracture where not all with osteoporosis will
onset for osteoporosis is typically...
rate increases during..
after the age of 40 (.5-1% of loss per year after age 40)
rate increases during a 3-5 year period after menopause
Most often a results of age-related bone loss..
postmenopausal bone loss, or other secondary factors (immobility, medication side effects, RA, Chrons disease, etc.) - or a combo of any of these
since _/_ of every women will experience osteoporosis at some point in their life, it is thought of...
1/2, it is thought of as a "women's disease" - but prevalence in males is at least 15%
When do you reach peak bone mass
25-30 yrs
peak bone mass
highest amount of bone mass attained during life
influencers of peak bone mass
genetics, physical activity, diet, and hormonal balance
what will determine osteoporosis development throughout life
Amount of peak bone mass and extent of bone loss that occurs throughout life
first line of defense for prevention of osteoporosis
maximizing peak bone mass during childhood and adolescence
bone modeling
bone formation without prior bone resorption
bone remodeling
old bone is broken down and new bone is produced in its place to maintain bone strength repair and fatigue damage
bone remodeling involves
bone resorption (break down of bone by osteoclasts) followed by bone formation (production of bone by osteoblasts)
bone remodeling takes
several months
If resorption and formation are balanced then bone mass is..
maintained
if resorption is greater than formation, then bone loss occurs
hormonal influencers in pre puberty
primarily influenced by estrogen, growth hormone, and insulin-like growth factors
bone growth in length occurs
occurs at the growth plate and influenced by Indian hedgehog, parathyroid hormone related protein, estrogen, and thyroid hormone
during/after puberty and into adulthood:
bone mass changes are mostly influenced by estrogen
estrogen deficiency =
bone loss
estrogen deficiency occurs after menopause and is why osteoporosis
becomes extremely more common in women with age
Young amenorrheic women experience bone loss due to...
hormone disruption
(damage can be intense enough that they are unable to regain sufficient bone mass even with resumption of regular menstrual periods)
what can create estrogen deficiency and affect bone mass
surgical removal of ovaries
what in men can result in bone loss
testosterone deficiency
other factors affecting bone mass: energy deficiency
energy deficiency in men and women of all ages increases bone loss
calcium or vitamin D deficiencies:
hinder bone mass
If calcium intake is insufficient during childhood when bone modeling is still occurring, then the body will sacrifice increases in bone length to maintain bone strength!
other factors affecting bone mass: mechanical loading
looks to increase bone mass and strength depending on frequency and magnitude of load
vice versa will also occur with decreased loading (bone loss and reduced strength)
most common sites for osteoporotic fractures are
the wrist, spine, humerus, hip (femoral neck), rib, pelvis
Most common sites are typically due to load on osteoporotic load, but can be influenced by..
torsional or compressive loads as well (especially the spine)
symptoms of osteoporosis
typically none during periods of accelerated bone loss or unbalanced bone remodeling
what is typically the first sign of osteoporosis and why is that unfortunate?
Fracture, this is unfortunate because that means the damage has already occurred
diagnostic testing for osteoporosis
dual energy absoprtiometry (DEXA/DXA) is the most common technology to assess BMD
DEXA is not used for overall BMD but typically more specific of the
hip, spine, and less often the forearm
what is used for diagnosis and most often the determination of 10 year risk?
femoral hip BMD
T score compares your bone density to a..
young adult at peak bone strength. It is not used if a person is younger than 50 years old.
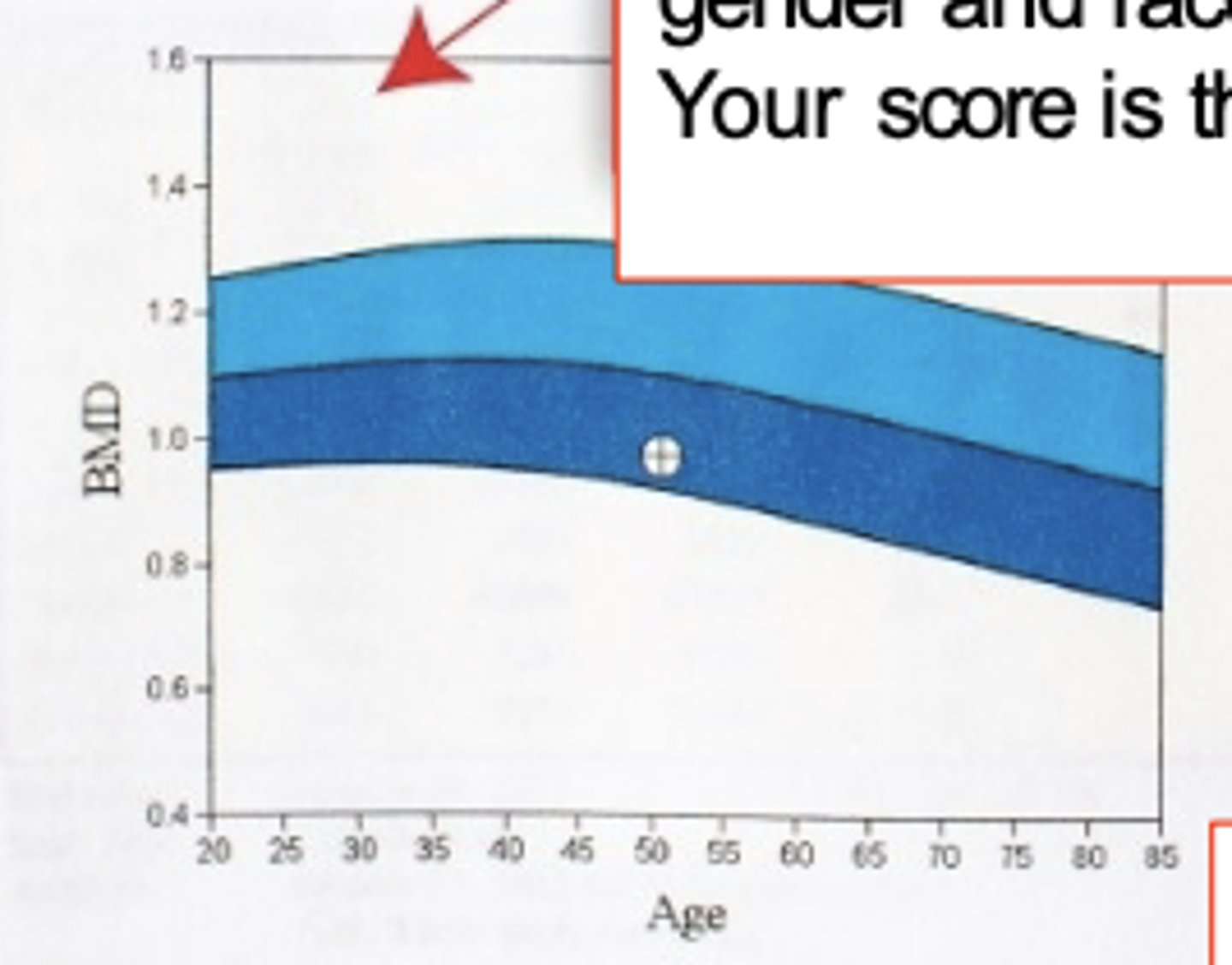
The reference graph compares your bone density to the...
young normal population (light blue) and a population of the same age, gender and race (dark blue). Your score is the circle.
Z score compares your bone density to
people of the same age.
A score of less than ___ implies less than average. If your T- score is less than __ or your Z score is less than __, you should contact your physician and have a comprehensive bone density DXA scan performed
-1, -1, -2
ACSM does not view osteoporosis as
an absolute or relative contraindication
For osteoporosis and osteopenia, best practice to avoid...
high-impact skeletal load testing such jumping/stepping
alternatives for exercise testing
cycling protocol, treadmill protocol (walking only)
consider fall risk and increased risk of fracture with a fall
treatment for osteoporosis
exercise, calcium supplementation, vitamin D supplementation, assessment of energy efficiency considerations
exercise alone for osteoporosis is...
not sufficient to prevent all bone loss, but is vital to bone health and reducing loss
Therapeutic goals include reducing fractures/risk of fractures with:
- Fall prevention protocols
- Promotion of spine-sparing strategies
Osteogenic exercise regimens that are currently supported (always with patient
specificity in mind - considering current risk of fracture with stress):
- Load-bearing activities at high magnitude with few reps
- Variable strain distributions throughout the bone structure
- Loading in a site-specific manner (hips, wrist, low back)
- Long-term and progressive exercise
- Dispersing loading activities throughout the day rather than all at one time
aerobic physical activity for osteoporosis
- 30-60 min of moderate activity each day
- 150-300 cumulative min/week
more exercise prescription for osteoporosis
- balance training (improves fall prevention)
- flexibility
- postural correction
what should all be considered when designing a program
Fall and fracture risk, medical history, physical function, goals, and
preferences
benefits of exercise needs to..
outweigh risk of fractures
what else should be prioritized in exercise program for patient with osteoporosis
balance, functional, and strength training