gut metabolism hormones mcq
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
glands
Epithelial tissue derivatives specialised for secreting
epithelial tissue
Functional grouping of cells specialised in the exchange of material between the cell and
it’s environment, lines and covers various body surfaces and cavities and forms secretory glands
Secretion
release from a cell in response to appropriate stimulation of specific products that have been
produced by the cell.
what are the 2 major communication systems
nervous and endocrine systems
name the four chemical messengers
1) Autocrine/Paracrine
• local chemical messengers
• exert effect on neighbouring cells (paracrine)
or on same cell (autocrine)
2) Neurotransmitter
• short-range chemical messengers
• diffuse across narrow space (synapse) to act
on adjoining target cell (another neuron, a
muscle, or a gland)
3) Neurohormones
• hormones released into blood by
neurosecretory neurons
• distributed through blood to distant target cells
4) Hormones
• long-range messengers
• secreted into blood by endocrine glands in
response to appropriate signal and act on
distant target cells
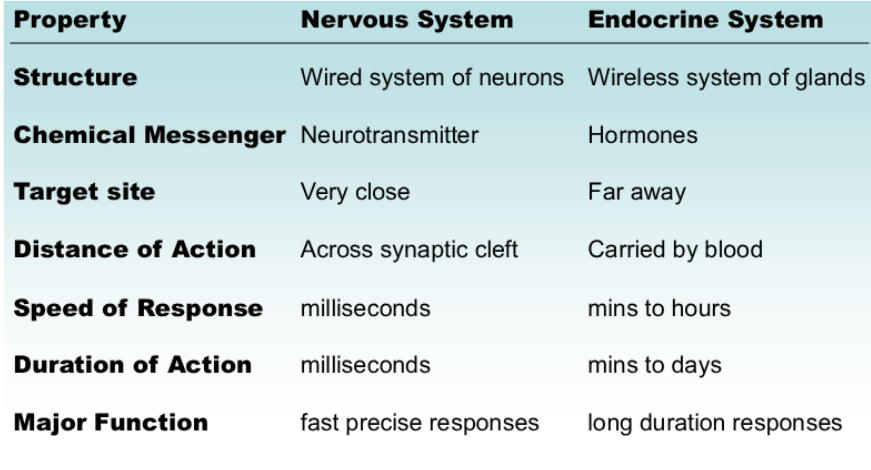
nervous versus endocrine
Neural messages can only travel along existing nerve tracts;
hormonal messages can travel in the circulatory system; thus any cell receiving blood is potentially able to receive a message.
• Neural messages are digital, all-or-none events that have rapid onset and offset; neural signals can take place in milliseconds; plus, electrical signal can travel along myelinated axons at speeds up to 100 meters per sec!
Hormonal messages are analog, graded events that can take
seconds, minutes or hours to occur.
effects of hormones
Hormones rarely change the function of a cell; rather, they alter the rate of
normal cellular function.
– Thus, hormones affect cell morphology and size (including development of muscle and neuronal
cells), and affect cell death (apoptosis) throughout the nervous system.
• Although hormones obviously affect behavior, it is also true that behavior can
influence hormonal levels and hormonal effects.
name the four types of hormones
Two hormone categories based on solubility
– Hydrophilic (lipophobic, water soluble)
• 1. Peptide hormones
• 2. Catecholamines
– Lipophilic (hydrophobic, water insoluble)
• 3. Thyroid hormone
• 4. Steroid hormones
Classification
steroid hormones
steroid hormones derived from cholesterol
- are small lipid-soluble molecules
- diffuse through cell membrane
- receptor is intracellular
2 types of receptors
surface receptors
– bind peptides & catecholamines
– at cell membrane
activation alters
– channel function
– second-messenger
system
• nuclear receptors
– bind thyroid & steroid hormones
– inside the cell
steroid receptors bind
steroid hormone
• hormone-receptor complex
becomes a transcription
factor (alters gene
transcription)
• each steroid receptor binds
a unique DNA sequence
(response element within
an enhancer region)
• this alters the rate of
transcription
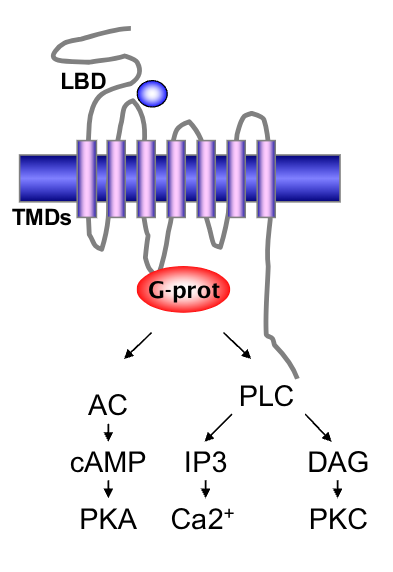
surface receptor structure
receptor domains
• ligand binding domain (LBD)
• 7 transmembrane domains (TMDs)
• G-protein coupled
• mechanism
• peptide hormone binds to receptors
on the surface of the cell
• activates G-protein
• induces intracellular signals
Neuropeptide Examples: Prolactin,
Adrenocorticotrophic hormone (ACTH),
Antidiuretic hormone (vasopressin),
Oxytocin, Insulin, Somatostatin
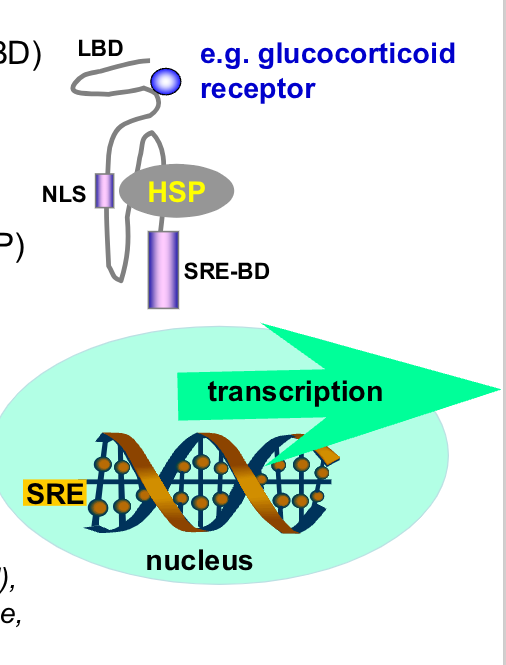
nuclear receptor structure
receptor domains
• Hormone/Ligand binding domain (LBD)
• DNA binding domain binds steroid
response element (SRE).
• Nuclear Localization Signal (NLS)
covered by heat shock proteins (HSP)
• mechanism
• binding of hormone induces
detachment of HSP; uncovers NLS
• receptor+hormone enters nucleus
• acts as a transcription factor
Estrogen, Glucocorticoid (Cortisol),
Mineralocorticoid (Aldosterone), Progesterone,
Androgen (Testosterone)
permissiveness versus antagonism versus synergism
target cell may be unresponsive due to lack of
receptors (physiological, genetic, disease)
• one hormone can influence activity of another hormone
by regulation of its receptor:
Permissiveness
– one hormone is required for another hormone to work
Synergism
– actions of several hormones are complimentary
– combined effect is greater than sum of separate effects
Antagonism
– one hormone inhibits another hormone’s receptors
– reduces effectiveness of second hormone
properties of endocrine glands
-derived from epithelial tissue
– composed of clumps of
secretory cells
– surrounded by capillaries
(fenestrated)
– exocrine glands have ducts
– endocrine glands have no
duct system
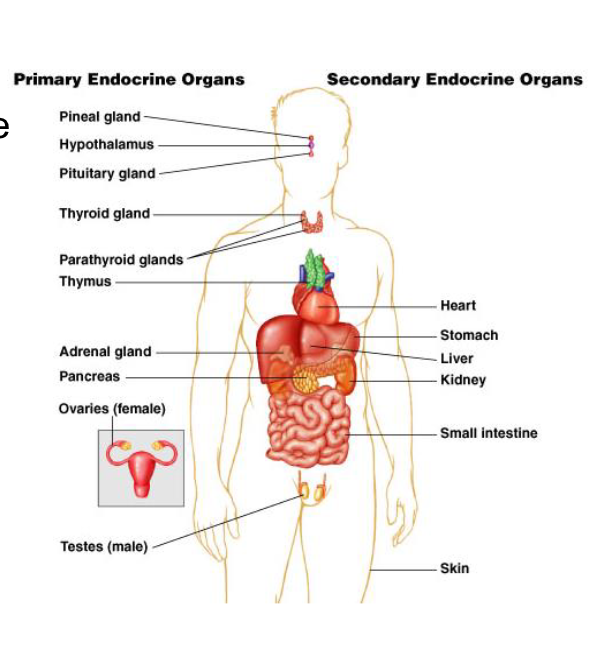
primary versus secondary endocrine organs
Primary Endocrine Organs
– discrete organs
– main function is endocrine hormone release
– pituitary, thyroid, parathyroid, adrenal and
pineal glands
Secondary Endocrine Organs
– dispersed in organs
– have other major functions
– heart, kidney, liver, etc.
what does endocrinologist study
Neuro-Endocrinology studies how the brain
regulates Pituitary hormone secretion
Control of Endocrine System
Endocrine System
long versus short hormonal feedback loop
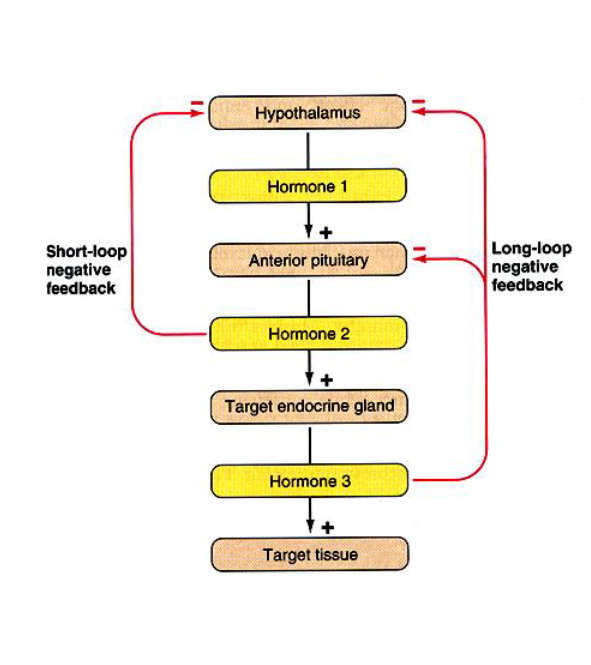
trophic hormones
regulate secretion
other hormones (either releasing or
inhibitory)
• example
– thyroid-stimulating hormone (TSH)
– secreted from anterior pituitary
– stimulates thyroid hormone secretion from
thyroid gland
– maintains structural integrity of thyroid
gland
Anterior pituitary
Thyroid
stimulating
hormone (TSH)
Thyroid gland
Thyroid Hormone
(T3.T4)
functions of the endocrine system
1. regulates organic metabolism and H2O and electrolyte balance
• 2. Induces adaptive changes to help cope with stressful situations
• 3. Promotes smooth, sequential growth and development
• 4. Controlling reproduction
• 5. Regulating red blood cell production
• 6. Along with the autonomic nervous system, controlling and integrating
activities of both the circulatory and digestive systems.
describe why the endocrine system is complex
A single endocrine gland can produce multiple hormones, eg
Anterior pituitary secretes 6 different hormones, each with distinct
functions.
• A single hormone may be secreted by more than one endocrine
gland, eg Pancreas and hypothalamus both secrete somatostatin.
• Frequently a single hormone may have more than one target cell
and hence produce more than one type of response, eg vasopressin
promotes H2O reabsorption by binding V2 receptors and cause
vasoconstriction of arterioles throughout the body by binding with V1
receptors on arteriolar smooth muscle.
• Rate of secretion of some hormones varies considerably over time
in a cyclic pattern eg the menstrual cycle.
A single target cell may be influenced by more than one hormone
eg, in liver cell: insulin promotes conversion of glucose into glycogen
by stimulating one particular hepatic enzyme, while glucagon,
stimulates another hepatic enzyme to enhance the degradation of
glycogen to glucose.
• The same chemical messenger may be a hormone or a
neurotransmitter eg, Norepinephrine. This is secreted as a hormone
by the adrenal medulla and as a neurotransmitter from sympathetic
postganglionic nerve fibers.
• Some organs are exclusively endocrine in function (specialise in
hormone secretion alone, eg anterior pituitary) while others perform
nonendocrine functions as well as hormone secretions eg testes
produce sperm and also secrete the male hormone testosterone.
relationship between pituitary and hypothalamus
hypothalamus-pituitary: major unit of endocrine system
• integrates nervous and endocrine systems
• pituitary function depends on hypothalamus
• pituitary (1 cm) lies at base of brain below hypothalamus
• it is connected by nerve fibers and blood vessels
• regulates function of
– thyroid
– adrenal
– reproductive glands
– somatic growth
– lactation
– water metabolism
structural description of hypothalamus and pituitary gland
hypothalamus lies at base of
brain
➢ pituitary connects to base of
brain by infundibular stalk
➢ anterior pituitary: epithelial
structure develops from
Rathke’s pouch
➢ posterior pituitary: neural
structure develops from floor of
midbrain, consists of nerve fibers
that run from hypothalamus to
anterior pituitary
posterior pituitary
along with hypothalamus
forms neuroendocrine
system
• composed of neural tissue
• stores two peptide
hormones in axonal ends
• release Oxytocin and
Vasopressin (Antidiuretic
hormone, ADH)
production of vasopressin and oxytocin
nerve cell bodies in of
hypothalamus
• peptides are packaged into
vesicular granules
• granules transported down
axons into posterior lobe
• peptide is released from
terminal (similar to
neurotransmitter release)
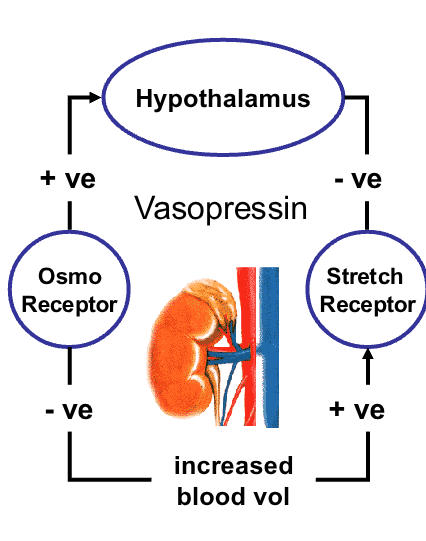
vasopressin/antidiruietic hormone purpose
controls blood volume
• acts on kidney to increase water
reabsorption in distal tubule
• increased blood volume
– sensed by stretch receptors in heart
atrium
– signal to hypothalamus
– decreased vasopressin production
• decreased blood osmolarity
– reduced activity of hypothalamic
osmoreceptors
– reduces vasospressin secretion
diabetes and vasopressin
in Diabetes - failure of ADH secretion or reduced sensitivity
of kidney to ADH (antidiuretic hormone) may occur
• Analogues for clinical use
– Vasopressin; desmopressin (enuresis); terlipressin
(control of bleeding); felypressin (adjunct to local
anaesthetic)
oxytocin
during birth, estrogen rises
• uterus produces oxytocin
receptors
• oxytocin contracts uterus
• synthetic oxytocin induces
labour
• oxytocin also helps in smooth
muscle contractions which
cause release of milk
• Influence maternal behaviour,
facilitates bonding or
attachment
• oxytocin may regulate brain
function…
posterior pituitary hormones

anterior pituitary
epithelia-derived upgrowth
from roof of oral cavity
• secretes tropic and direct
hormones
• anterior pituitary hormones
are regulated by
hypothalamic hormones
cell types of anterior pituitary
Unlike the posterior pituitary the anterior pituitary itself synthesises
the hormones it releases into the blood.
• Five different cell populations secrete 6 major peptide hormones.
• Generally each cell type produces mainly one hormone
• cells named according to hormone they produce
1. Somatotrophs make growth hormone (somatotrophin) – primary
hormone that regulates overall body growth.
2. Thyrotropes secrete thyroid stimulating hormone (TSH, tyrotropin)
– stimulate secretion of thyroid hormone and growth of the thyroid
gland.
3. Corticotropes, produce and release adrenocorticotropic hormone (ACTH)
– stimulates cortisol secretion by the adrenal gland and promotes growth of
the adrenal gland.
4. Gonadotropes – secrete 2 hormones that act on the gonads: Follicle
stimulating hormone (FSH) helps regulate gamete production in both sexes.
In females stimulates growth of ovarian follicles, within which ova develop
and also promotes secretion of oestrogen by the ovaries. In males required
for sperm production.
5. Luteinizing hormone (LH) – helps control sex hormone secretion in both
sexes. In females LH responsible for ovulation, and controls secretion of
oestrogen and progesterone. In males LH causes secretion of testesterone
from the testes.
6. Lactotrophs secrete prolactin. Enhances breast development and milk
production in females. Function in males is less certain
what regulates anterior pituitary hormone seceretion
The 2 most important factors that regulate anterior pituitary hormone
secretion are:
1) hypothalamic hormones
2) feedback by target gland hormones.
There are 7 hypophysiotropic hormones:
1. Tyrotropin releasing hormone (TRH).
2. Corticotropin releasing hormone (CRH)
3. Gonadotropin releasing hormone (GnRH)
4. Growth hormone releasing hormone (GHRH)
5. Somatostatin (Growth hormone inhibiting hormone; GHIH)
6. Prolactin releasing hormone (PRH)
7. Dopamine (Prolactin-Inhibiting hormone; PIH)
factors other than growth hormone affecting growth
Genetic determination: of an individuals growth capacity
An adequate diet, including enough protein and ample amino acids to
accomplish protein synthesis necessary for growth.
Freedom from chronic disease and stressful environment: Stunted
growth from stress induced secretion of cortisol –over a prolonged
period of time.
- Cortisol can promote protein breakdown, inhibiting growth of long
bones and block the secretion of GH.
Normal levels of growth-influencing hormones: In addition to GH,
other hormones including thyroid hormone, insulin and the sex
hormones play secondary roles in promoting growth.
Major Regulators of Growth
• Growth hormone
• Somatomedins (IGFs; insulin growth
factors)
Others – growth influencing hormones.
• Oestrogens/Testosterone
• Insulin
• Thyroid hormones
• Calcitonin, PTH and Vitamin D
growth hormone circulation
─ also called somatotropin
─ peptide hormone 191
amino acid
─ mol wt approx. 20 kDa
─ 500μg made per day
(circulating 0-30 ng/ml,
t1/2 ~20min)
─ GH is encoded on
chromosome 17
growth rate
Release of GH
• not continuous
• different factors responsible for
growth at different periods
Fetal growth
• promoted by placenta hormones
• GH plays no role in fetal growth
Postnatal growth spurt
• first two years of life
Puberty growth spurt
• Male: Androgens (testes) promote
growth
• Female: Androgens (adrenal glands,
less potent) promote growt
growth in children
Children display 2 periods of rapid growth – a postnatal growth spurt
up to the age of 2 and a pubertal growth spurt during adolescence
• Before puberty little sex differences in height or weight. Puberty
begins at age 11 in girls and age 13 in boys
• GH and androgen secretion is elevated – promote protein synthesis
and bone growth
- Testosterone – promotes sharp increase in height in boys
- In females androgens from the adrenal cortex most likely involved in
female growth spurt. There is a rise in oestrogen secretion during
puberty but the role this female sex hormone may play is unclear.
• testosterone and oestrogen both act on bone to halt its further
growth so that full height is attained at the end of adolescence
release of growth hormone
ulsed release
─ released from anterior pituitary in several bursts
─ high morning before awakening, low in day
─ secretion stimulated during deep sleep
─ rhythm linked to sleep-wake not light/dark
─ surges in first 2 hr sleep at night
Number/magnitude pulses depend on age
─ high in puberty
─ low in adults
─ absent at 50yr+
Age-related decrease in GH release
─ change in muscle:fat ratio
─ decreased bone density
─ GH sold as “anti-ageing” therapy? (but may
actually speed ageing)……..
GHRH control of GH
GHRH (growth hormone
releasing hormone) and
somatostatin produced by
hypothalamic neurons
─ GHRH receptor is a 7
transmembrane domain
G-protein coupled receptor
─ GHRH stimulates GH
synthesis and secretion
─ GH bursts initiated by bursting
secretion of GHRH
─ terminated by somatostatin
what does injection of growth hormone into animals cause
─ increases glucose levels in blood
─ promotes protein synthesis
─ promotes lipolysis in adipocytes
─ promotes bone growth
─ results in erythropoesis
─ has anti-insulin activity
long term metabolic effects of growth hormone
Carbohydrates
─ increases glucose levels in blood
Proteins Synthesis
─ increases tissue amino acid uptake
Lipids (Lipolysis)
─ increases free fatty acids in blood
Stimulates Growth
─ stimulates IGF production
what does GH stimulate
– Liver production of
somatomedins (insulin-like
growth factor; IGF-1)
– Acts on bone & soft tissues to
promote growth
– Stimulates protein synthesis, cell
division (of chondrocytes),
lengthening, thickening of bones
• metabolic effects
– increases fatty acid levels in blood
(by breakdown of fat)
– increases blood glucose levels
(by decrease of glucose uptake
by muscles)
GH releases IGF-1
Growth Hormone
how does growth hormone mediate its actions
GH mediates actions via IGFs
─ GH stimulates liver to produce IGFs
─ IGFs (insulin-like growth factors) structurally related
to insulin
─ IGF stimulates
─ bone and soft tissue growth
─ Hyperplasia: cell proliferation
─ Hypertrophy: increasing the size of cells
─ Prevents apoptosis
─ Examples of disease
─ Mice genetically lacking GH are dwarfed
─ IGF can overcome GH defects
alton giant
─ GH excess caused by
tumour cells of anterior
pituitary
─ in children gigantism
─ in adults acromegaly
Pituitary Gigantism
Growth Hormone
Robert Wadlow the
“Alton Giant”
He was 8 feet, 11
inches tall and
weighed 475 pounds
at the age of 22
acromegaly
GH hypersecretion after adolescence
causes acromegaly
• benign tumors (adenomas) in pituitary
gland produces excess GH
• Features
– thickening of bones
– coarsened facial features
– soft tissue swelling (hands and feet)
– heart failure
– vision loss (compressed optic chiasm)
• Medication reduce GH secretion/tumor
– Bromocriptine (DA receptor agonist)
– somatostatin, to stop GH production
– GH receptor antagonists are emerging
Acromegaly
Growth Hormone
Progression of acromegaly
A - Age 9 (normal)
B - Age 16 (coarsening features)
C - Age 33 (established acromegaly)
D - Age 52 (severe acromegaly)
dwarfism
GH deficiency
• (1) low GH
• treated by replacing with GH
Hereditary
• (2) low GHRH
Laron dwarf
• (3) defective GH receptor
African Pygmy
• (4) defective IGF1 receptor
overall metabolic effect of growth hormone
Increases fatty acid levels in the blood by enhancing breakdown of
triglyceride fat stored in adipose tissue.
Increases blood glucose by decreasing glucose uptake by muscles and
increasing glucose output by the liver– muscle use mobilised fatty
acids as fuel instead of glucose.
Overall metabolic effect of GH = mobilise fat stores as a major
energy substrate while conserving glucose for glucose dependent
tissues such as brain.
Note: Brain can only use glucose as its metabolic fuel, yet the brain
cannot store glycogen (stored glucose) to any extent.
This pattern is useful during prolonged fasting or other situations where
the body’s energy needs exceed available glucose stores.
other hormones related to growth
Thyroid hormone – essential for growth BUT not directly responsible for
promoting growth.
Plays a permissive role in skeletal growth; the actions of GH only manifest
when sufficient TH is present.
Hypothyroid children: Growth severely stunted.
Hypersecretion: does not affect growth.
Insulin – growth promoter.
Promotes protein synthesis.
Insulin deficiency – blocks growth
Hyperinsulinism – spurs excessive growth.
Androgens – pubertal growth spurt, stimulate protein synthesis in many
organs.
Stimulate linear growth
Promote weight gain
Increase muscle mass
Testosterone - Most potent androgen, promotes a sharp increase in height in
adolescent boys.
Androgens have virtually no effect on body growth in the absence of GH.
Oestrogens - thought to contribute to the pubertal growth spurt in females but
its exact role is uncertain.
thyroid gland
Located on the front of upper part of trachea
• develops from epithelial outgrowth of tongue
Major secretory cells – follicular cells, arranged in
hollow spheres – functional unit is a follicle
Follicles appear as rings consisting of a single layer of
follicular cells enclosing an inner lumen filled with
colloid – a substance that serves as an extracellular
storage site for TH.
thyroid hormones functions
Major constituent of colloid is a large glycoprotein
molecule known as thyroglobulin (Tg) –
incorporated into TH during their synthesis.
Types of thyroid hormones
• T3 (Triiodotyronine) (t1/2 ~1.5 days) in follicles
• T4 (Thyroxine) (t1/2 ~7 days) in follicles
• Calcitonin by C cells – role in Calcium
metabolism not related to T3/T4
Function of T3 and T4
• accelerate metabolism
• increase carbohydrate, fat and protein turnover
T3 and T4
Structure of T3 and T4
• tyrosine-based hormones
• T3 has 3 iodine atoms, T4 contains 4
• T3 more effective, but T4 more abundant
Levels of T3 and T4
• controlled by anterior pituitary TSH
• transported in blood, bound to thyroxine-
binding globulin (TBG)
• made by follicular cells when iodide available
• iodide absorbed from blood to thyroid follicles
effects of thyroid hormone
Effects of thyroid hormone
- Main determinant of basal metabolic rate
- Influences synthesis and degradation of
carbohydrate, fat and protein
- Increases target cell responsiveness to
catecholamines
- Increases heart rate and force of contraction
- Essential for normal growth
- Plays crucial role in normal development of the
nervous system
goiter and hashimotos
Goiter - low iodine uptake
─ normal: thyroid gland takes up 30% of
ingested iodide
─ disease: dietary iodide insufficiency
─ no T3/T4 made
─ thyroid cell proliferation
─ iodide uptake increases
─ normal human thyroid gland of 25 g may
grow to 250 g during goiter
Hashimoto’s - autoimmune disease
─ autoimmune (autoantibodies destroy
thyroid follicular cells)
hypothyroidism
- Primary failure of the thyroid gland itself
Secondary to a deficit of TRH, TSH or both
- Inadequate dietary supply of iodide
cretinism hypothyroidism versus myxedema
Cretinism
Hypothyrodism - Infants
• stunted growth
• lack of bone formation
• skeletal abnormalities
• severe mental retardation
• Protruding tongue
myxedema Hypothyroidism developing in older child or in adult
Clinical features
• Generalised fatigue
• Mental slugglishness
• Slow speech
• Cold intolerance
• Overweight
• Shortness of breath
• Constipation
• Decreased sweating
• Cool and pale skin
• Generalized edema
• Enlargement of tongue
• Deepened voice
hyperthyroidism
ymptoms
• high metabolic rate
• protruding eyes
• hyperactivity, insomnia
• heat sensitivity, weight loss, always hot
Grave’s disease
• autoimmune (TSH mimicked by
autoantibodies – also known as thyroid
stimulating immunoglobulin (TSI))
• Treatments
– Beta blockers help some symptoms
– Anti-thyroid medications
– Radioactive iodine treatment
destroys overactive thyroid cells
– Surgery thyroidectomy
adrenal glands
adrenal glands embedded above each kidney in a capsule of fat
adrenals have two divisions: cortex and medulla
adrenal medulla
composed of chromaffin cells
• originate from sympathetic nervous system
• Catecholamines
– epinephrine (adrenaline)
– norepinephrine (noradrenaline)
INNER
adrenal cortex
OUTER
similar origin to gonads
• make steroids hormones
• Mineralocorticoids (outer gland)
– aldosterone
• Glucocorticoids (middle gland)
– cortisol (corticosterone)
• Androgen sex steroids (inner gland)
– DHEA (dehydroepiandrosterone)
layers of adrenal cortex
Consists of three layers or zones
• Zona glomerulosa – outermost layer
• Zona fasciculata – middle and largest portion
• Zona reticularis – innermost zone
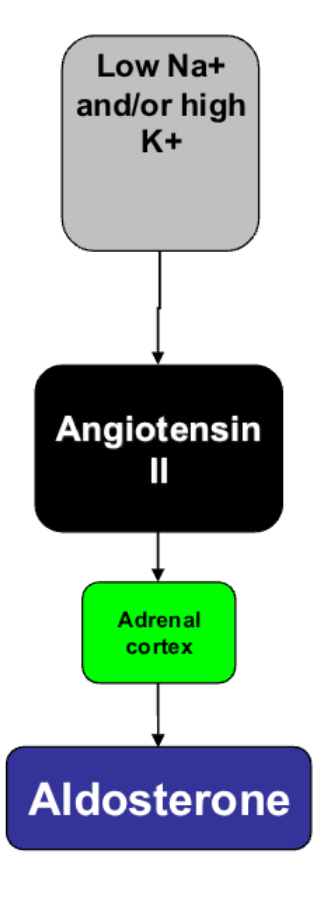
aldosterone
is major mineralocorticoid
• maintains electrolyte balance
• Feedback:
– 1. low plasma Na++ or high K+
– 2. activates renin-angiotensin system
– 3. Angiotensin II increases aldosterone
release from adrenal glands
– 4. acts on distal renal tubules
• increase Na++ & water retention
• increase excretion of K+ & H+ ions
cortisol
Cortisol (hydrocortisone)
• major glucocorticoid in humans
• secretion regulated (diurnal rhythm)
– plays role in stress
– increase blood glucose
– increase blood fatty acids
– control water and electrolyte balance
– anti-inflammatory/immunosuppressive
Feedback:
• negative feedback on hypothalamus (CRH) &
anterior pituitary (ACTH)
sex hormone dhea
Adrenal cortex - secretes both male and female
sex hormones in both sexes
– Dehydroepiandrosterone (DHEA)
• Only adrenal sex hormone that has any biological
importance
• Overpowered by testicular testosterone in males
• Physiologically significant in females where it governs
– Growth of pubic and axillary hair
– Enhancement of pubertal growth spurt
– Development and maintenance of female sex drive
Adrenal cortex
catecholamines
Epinepherine and Norepinerphrine
• Adrenal medulla (modified part of sympathetic nervous
system)
• Primary stimulus: activation of sympathetic nervous
system by stress
• Epinephrine/Adrenaline
– Secreted into blood
– “fight-or-flight” responses
– Maintenance of arterial blood pressure
– Increases blood glucose
– Increases fat metabolism (increase blood fatty acids)
Adrenal medulla
addisons disease
low glucocorticoid (cortisol) & mineralocorticoid
(aldosterone)
Causes
• Primary Addison’s: damage adrenal gland
(TB or autoimmunity)
• Secondary Addison’s: low ACTH release
Symptoms
• hypoglycaemia
• decreased liver glycogen
• fatigue, anorexia, nausea, weight loss, dizziness,
hypotension, psychiatric
• death if untreated
Treatment
• Steroid replacement therapy
cushings disease
Excess glucocorticoids (cortisol)
Causes
• ACTH secreting tumor in pituitary
Symptoms
• hyperglycemia
• elevated blood pressure
• obesity (abdominal fat, thin arms & legs)
• muscle wasting, osteoporosis, cataracts
• poor wound healing
• buffalo hump, moon face, red cheeks
• psychiatric symptoms (depression,
euphoria, hallucinations)
Treatment
• remove tumor
• antiglucocorticoids
• surgical adrenalectomy
Conns syndrome
Excessive mineralocortocoids (aldosterone)
Causes
• primary - tumour
• secondary - excessive renin-angiotensin
action in kidney disease, cirrhosis of liver,
congestive heart failure
Symptoms
• sodium and water retention
• increase in extracellular fluid and hypertension
Treatment
• antagonist of aldosterone (spirono-lactone)
• unilateral adrenalectomy
generalised stress response in the HPA axis versus chronic
generalised stress response
• ↑ epinephrine secretion from adrenal medulla
(chromaffin cells)
• ↑ CRH-ACTH-cortisol (HPA axis) that mobilises
metabolic resources
• ↓ insulin & ↑ glucagon secretion to raise blood
glucose & fatty acids
• ↑ renin-angiotensin-aldosterone system &
vasopressin secretion to maintain blood volume
and blood pressure
chronic stress
• causes heart disease, hypertension,
atherosclerosis, immune-suppression
• prolonged release of CRH causes
anxiety & depression
• CRF1 receptor antagonists may treat
anxiety, depression, drug dependence
and irritable bowel syndrom