Class 10 (February 2nd)
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
"To resist the decline in sexuality of old age, one must combine the body, the mind, and the heart. And to keep these in parallel vigor, one must exercise, study, and love."
Bleasdale
Sexual Health (WHO)
A state of physical, emotional, mental and social wellbeing related to sexuality and not just the absence of disease, dysfunction or infirmity.
Sexuality is a complex concept
Partnerships
Behaviours
Attitudes
Identity
Orientation
Beliefs
Activity
Prevalence of Sexual Activity in Aging
Epidemiology
Epidemiology
Marked decline in sexual activity with age
Sexual activity maintained by some but not all adults later in life
40 – 69 years of age 75% still sexually active (of 2000 women)
40 – 80 years of age 80% of men, 65% of women intercourse in the past year (of 27,500) people
70 - 80 years of age; 53% of men, 21% of women engaged in sexual activity in the past year
75 – 85 years of age who were sexually active
54% have sex 2-3 times/month
¼ have sex on a weekly basis
75 – 85 years of age who were sexually active
54% have sex 2-3 times/month
¼ have sex on a weekly basis
Decline in Sexual Activity with Aging
Access to a partner
Men
Women
Men
Parallels decline in androgen levels
Men with higher testosterone have increased
Erections
Sexual desire
Women
Ovarian Steroids
Estradiol, testosterone, progesterone
Estradiol, testosterone, progesterone
Positive effect on sexual desire
Access to a partner
Older people not in a relationship
22% men, 4% women report having sex in the past year.
Older people not in a relationship
22% men, 4% women report having sex in the past year.
Sex is unimportant
35% of older women; 12% of older men
Sex is not at all important
57-64 year olds – 15%
65-74 year olds - 25%
75-85 year olds – 41%
What Activities Reflect Sexuality
Closeness
Touching
Exchanging Fantasies
Caressing
Mutual Masterbation
Penetrative Sex (oral, vaginal, anal)
Most research is cis-gender vaginal
Emotionality
Biopsychosocial Model of Changes Related to Sexuality in Later Life
Biological Domain
Social Domain
Psychological domain
Biological Domain
Women – Menopause
Men
Women – Menopause
Depletion of oocytes (egg cells)
Decrease production of Sex Hormones:
Decrease
sexual satisfaction
Vaginal lubrication
Pain with intercourse (dyspareunia)
Atrophy of the vagina
Mood changes/irritability
Anorgasmia (unable to orgasm)
Decrease production of Sex Hormones: (women)
Estradiol
Progesterone
Estrogen
Follicle-stimulating hormone (FSH)
Decrease of sex hormones what happens
sexual satisfaction
Vaginal lubrication
Men (bio domain)
Decreased testosterone
Increased ED causes:
Hormonal
Neurological
Psychological
Vascular (40%) – modifiable by lifestyle
Increased ED causes:
Hormonal
Neurological
Psychological
Vascular (40%) – modifiable by lifestyle
Social Domain
Smaller social network
Access to a partner (or potential to find one)
Societal stigma – assumption that older people are asexual
Social sexual stigma
assumption that older people are asexual
Psychological domain
Identity
Expression of emotions
Eroticism
Fantasy
Self-esteem
Intimacy
Mental health issues leading to lower sexual function
Depression
Anxiety
Chronic stress
Obsessive compulsive disorder
Mental health issues leading to lower sexual function
Depression
Anxiety
Chronic stress
Obsessive compulsive disorder
Prevalence of Sexual Dysfunction in Older Adults
Older men report more frequency and satisfaction with their sexual lives than older women
Dysfunction more common in older women
50% of older adults report at least one bothersome problem associated with sex
Dysfunction in older men:
Dysfunction more common in older women
Sexual desire/interest
Arousal issues
Orgasm issues
Sexual pain
50% in peri/post menopausal women
12-25% have psychological problem associated with sex
Dysfunction in older men
Erectile problems (40-70%)
Premature climax (30-70%)
Inability to climax (20-70%) +ve correlation to increasing age
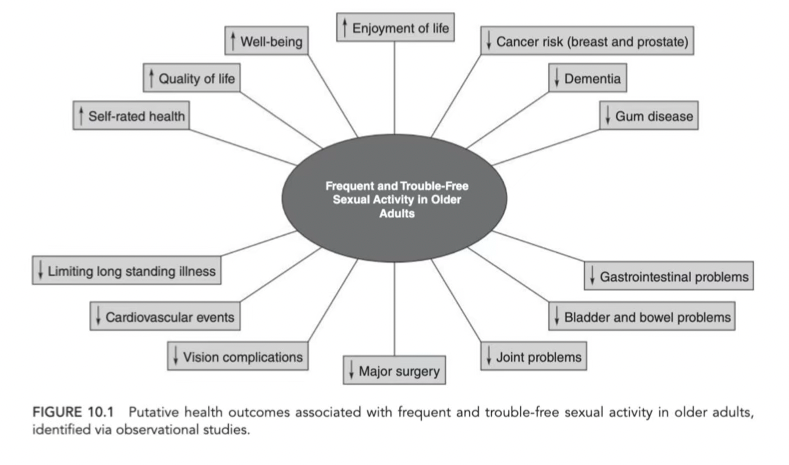
Physical and Mental Health Benefits of a Frequent and Trouble-Free Sex Life in Later Life
Older people do not become “asexual”
Reduces risk of physical and mental disease outcomes
The Role of Physical Activity on Sexuality in Older Adults
Prevention of Erectile Dysfunction
Protective Factor against Female Sexual Dysfunction
Protective against chronic illnesses prevalent in older adults known to have pathophysiological mechanisms that impact sexual health
Prevention of Erectile Dysfunction
Aerobic exercise
Moderate to vigorous intensity
Protective against chronic illnesses prevalent in older adults known to have pathophysiological mechanisms that impact sexual health
Decrease obesity
Improve mental health
Decrease inflammaging
Sexual activity is a form of moderate physical activity
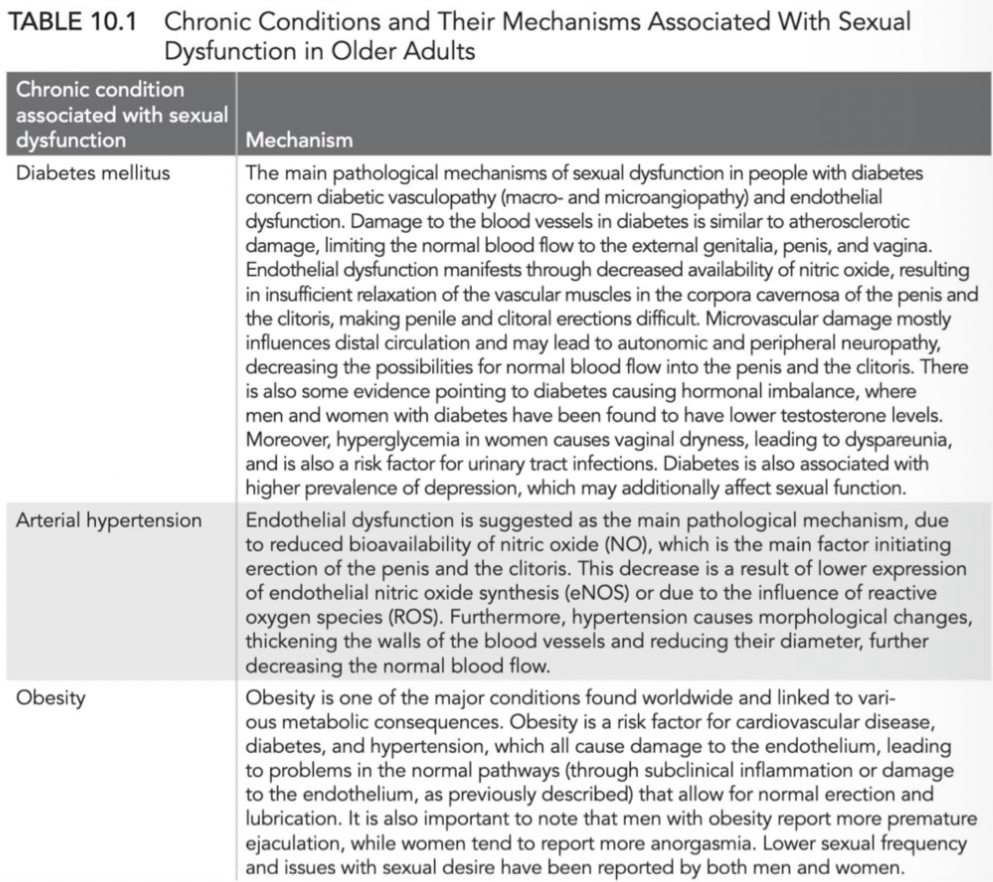
Chronic conditions and mechanisms associated with sexual dysfunction in older adults 1
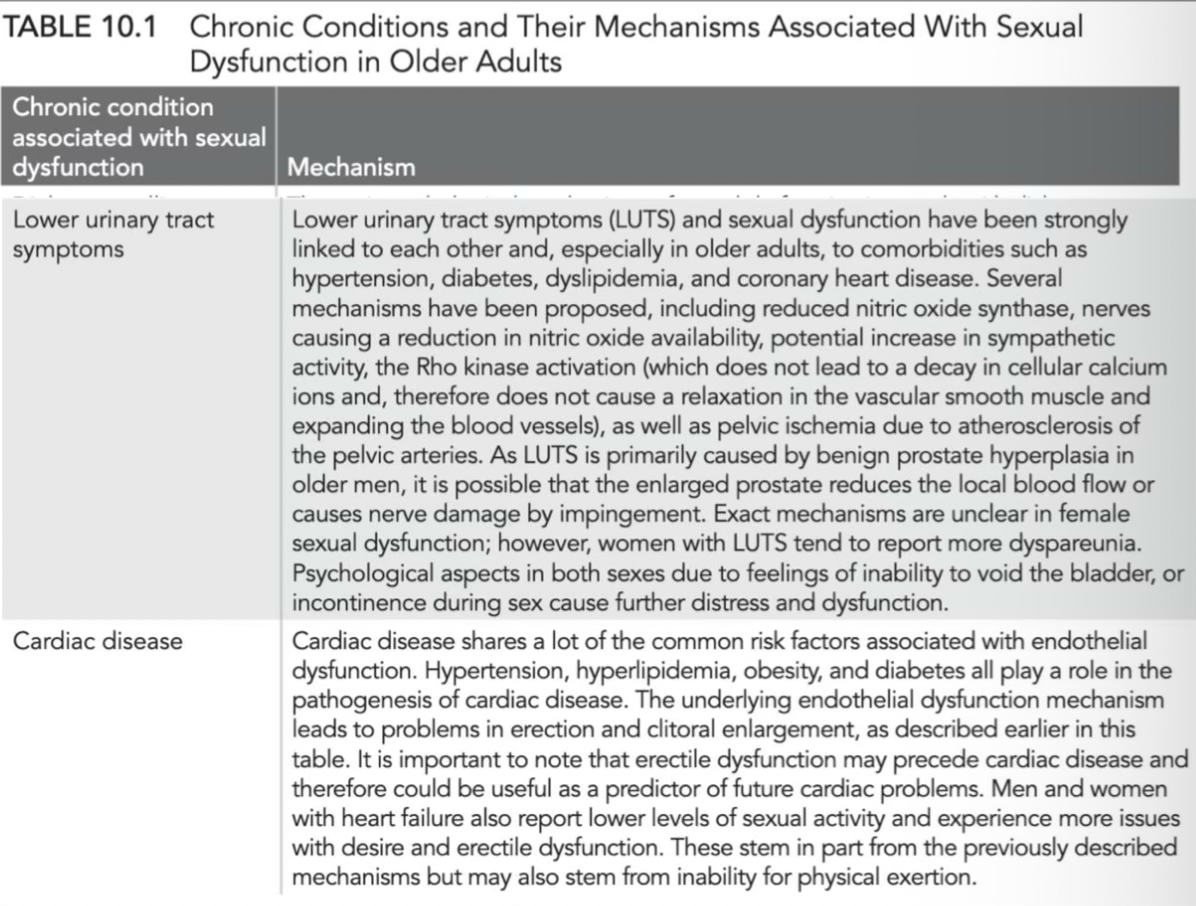
Chronic conditions and mechanisms associated with sexual dysfunction in older adults 2
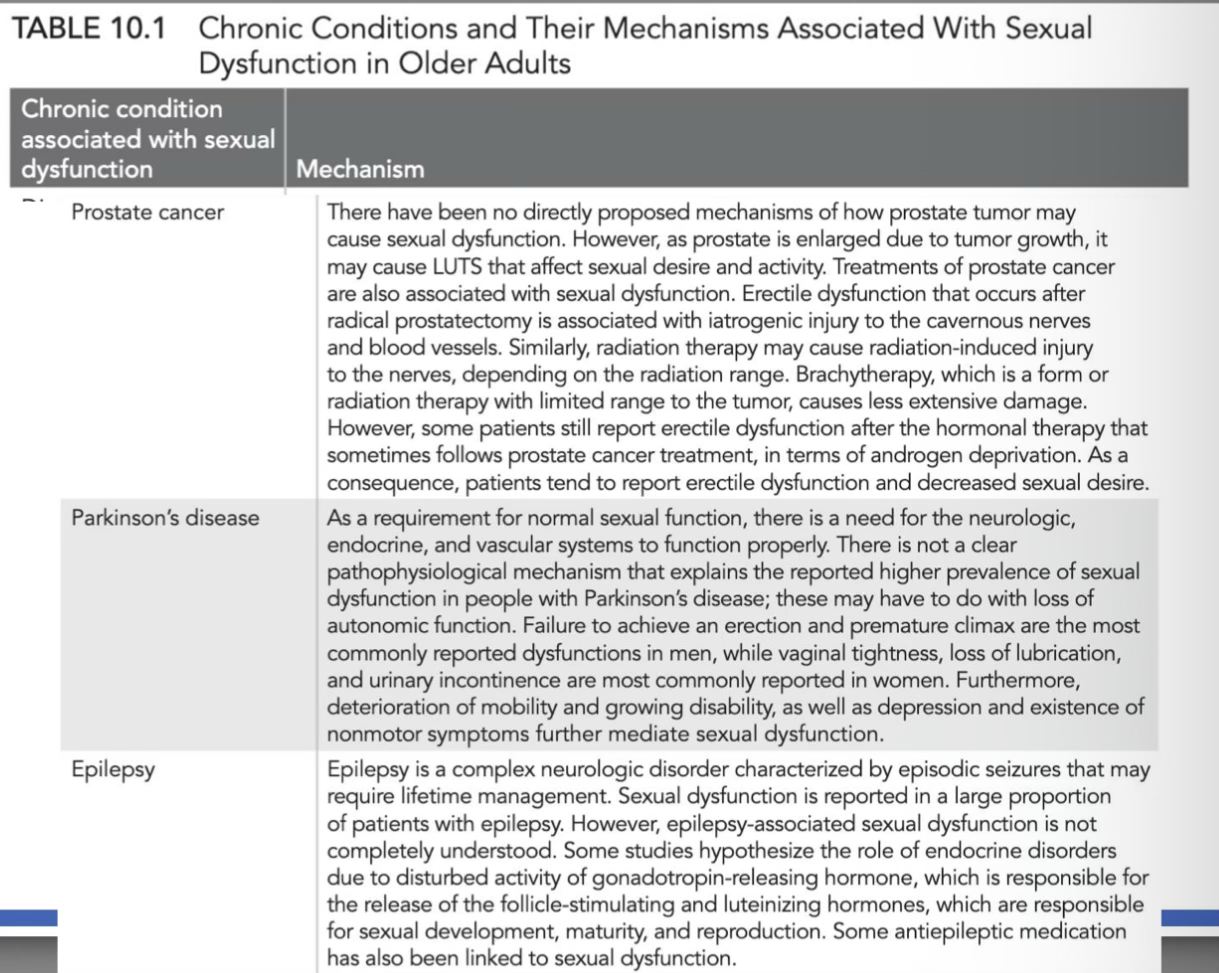
Chronic conditions and mechanisms associated with sexual dysfunction in older adults 3
Chronic conditions and mechanisms associated with sexual dysfunction in older adults 4
Diabetes mellitus
The main pathological mechanisms of sexual dysfunction in people with diabetes concern diabetic vasculopathy (macro- and microangiopathy) and endothelial dysfunction. Damage to the blood vessels in diabetes is similar to atherosclerotic damage, limiting the normal blood flow to the external genitalia, penis, and vagina. Endothelial dysfunction manifests through decreased availability of nitric oxide, resulting in insufficient relaxation of the vascular muscles in the corpora cavernosa of the penis and the clitoris, making penile and clitoral erections difficult. Microvascular damage mostly influences distal circulation and may lead to autonomic and peripheral neuropathy, decreasing the possibilities for normal blood flow into the penis and the clitoris. There is also some evidence pointing to diabetes causing hormonal imbalance, where men and women with diabetes have been found to have lower testosterone levels. Moreover, hyperglycemia in women causes vaginal dryness, leading to dyspareunia, and is also a risk factor for urinary tract infections. Diabetes is also associated with higher prevalence of depression, which may additionally affect sexual function.
Arterial hypertension
Endothelial dysfunction is suggested as the main pathological mechanism, due to reduced bioavailability of nitric oxide (NO), which is the main factor initiating erection of the penis and the clitoris. This decrease is a result of lower expression of endothelial nitric oxide synthesis (eNOS) or due to the influence of reactive oxygen species (ROS). Furthermore, hypertension causes morphological changes, thickening the walls of the blood vessels and reducing their diameter, further decreasing the normal blood flow.
Obesity
Obesity is one of the major conditions found worldwide and linked to various metabolic consequences. Obesity is a risk factor for cardiovascular disease, diabetes, and hypertension, which all cause damage to the endothelium, leading to problems in the normal pathways (through subclinical inflammation or damage to the endothelium, as previously described) that allow for normal erection and lubrication. It is also important to note that men with obesity report more premature ejaculation, while women tend to report more anorgasmia. Lower sexual frequency and issues with sexual desire have been reported by both men and women.
Lower urinary tract symptoms
Lower urinary tract symptoms (LUTS) and sexual dysfunction have been strongly linked to each other and, especially in older adults, to comorbidities such as hypertension, diabetes, dyslipidemia, and coronary heart disease. Several mechanisms have been proposed, including reduced nitric oxide synthase, nerves causing a reduction in nitric oxide availability, potential increase in sympathetic activity, the Rho kinase activation (which does not lead to a decay in cellular calcium ions and, therefore does not cause a relaxation in the vascular smooth muscle and expanding the blood vessels), as well as pelvic ischemia due to atherosclerosis of the pelvic arteries. As LUTS is primarily caused by benign prostate hyperplasia in older men, it is possible that the enlarged prostate reduces the local blood flow or causes nerve damage by impingement. Exact mechanisms are unclear in female sexual dysfunction; however, women with LUTS tend to report more dyspareunia. Psychological aspects in both sexes due to feelings of inability to void the bladder, or incontinence during sex cause further distress and dysfunction.
Cardiac disease
Cardiac disease shares a lot of the common risk factors associated with endothelial dysfunction. Hypertension, hyperlipidemia, obesity, and diabetes all play a role in the pathogenesis of cardiac disease. The underlying endothelial dysfunction mechanism leads to problems in erection and clitoral enlargement, as described earlier in this table. It is important to note that erectile dysfunction may precede cardiac disease and therefore could be useful as a predictor of future cardiac problems. Men and women with heart failure also report lower levels of sexual activity and experience more issues with desire and erectile dysfunction. These stem in part from the previously described mechanisms but may also stem from inability for physical exertion.
Prostate cancer
There have been no directly proposed mechanisms of how prostate tumor may cause sexual dysfunction. However, as prostate is enlarged due to tumor growth, it may cause LUTS that affect sexual desire and activity. Treatments of prostate cancer are also associated with sexual dysfunction. Erectile dysfunction that occurs after radical prostatectomy is associated with iatrogenic injury to the cavernous nerves and blood vessels. Similarly, radiation therapy may cause radiation-induced injury to the nerves, depending on the radiation range. Brachytherapy, which is a form or radiation therapy with limited range to the tumor, causes less extensive damage. However, some patients still report erectile dysfunction after the hormonal therapy that sometimes follows prostate cancer treatment, in terms of androgen deprivation. As a consequence, patients tend to report erectile dysfunction and decreased sexual desire.
Parkinson's disease
As a requirement for normal sexual function, there is a need for the neurologic, endocrine, and vascular systems to function properly. There is not a clear pathophysiological mechanism that explains the reported higher prevalence of sexual dysfunction in people with Parkinson's disease; these may have to do with loss of autonomic function. Failure to achieve an erection and premature climax are the most commonly reported dysfunctions in men, while vaginal tightness, loss of lubrication, and urinary incontinence are most commonly reported in women. Furthermore, deterioration of mobility and growing disability, as well as depression and existence of nonmotor symptoms further mediate sexual dysfunction.
Epilepsy
Epilepsy is a complex neurologic disorder characterized by episodic seizures that may require lifetime management. Sexual dysfunction is reported in a large proportion of patients with epilepsy. However, epilepsy-associated sexual dysfunction is not completely understood. Some studies hypothesize the role of endocrine disorders due to disturbed activity of gonadotropin-releasing hormone, which is responsible for the release of the follicle-stimulating and luteinizing hormones, which are responsible for sexual development, maturity, and reproduction. Some antiepileptic medication has also been linked to sexual dysfunction.
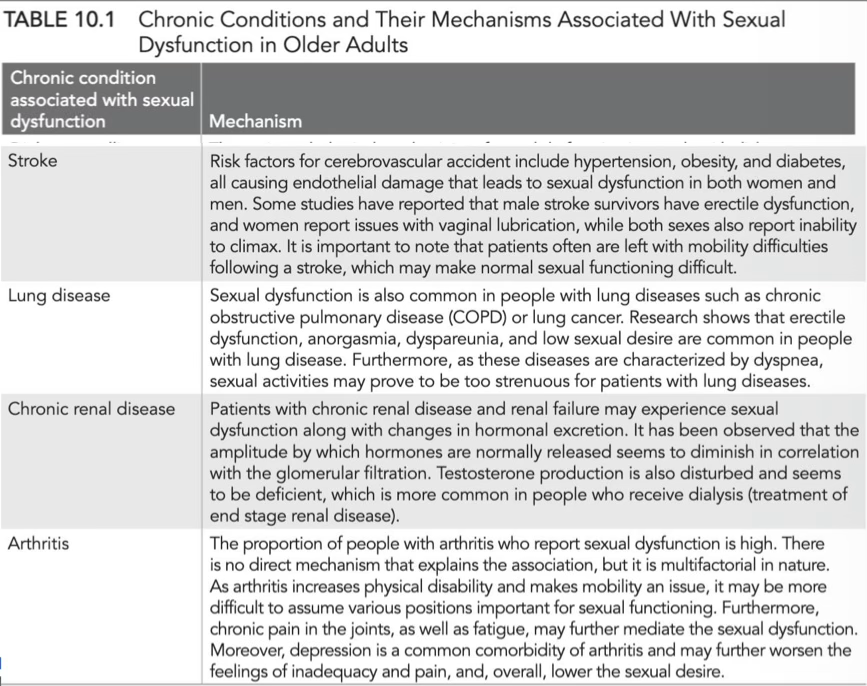
Stroke
Risk factors for cerebrovascular accident include hypertension, obesity, and diabetes, all causing endothelial damage that leads to sexual dysfunction in both women and men. Some studies have reported that male stroke survivors have erectile dysfunction, and women report issues with vaginal lubrication, while both sexes also report inability to climax. It is important to note that patients often are left with mobility difficulties following a stroke, which may make normal sexual functioning difficult.
Lung disease
Sexual dysfunction is also common in people with lung diseases such as chronic obstructive pulmonary disease (COPD) or lung cancer. Research shows that erectile dysfunction, anorgasmia, dyspareunia, and low sexual desire are common in people with lung disease. Furthermore, as these diseases are characterized by dyspnea, sexual activities may prove to be too strenuous for patients with lung diseases.
Chronic renal disease
Patients with chronic renal disease and renal failure may experience sexual dysfunction along with changes in hormonal excretion. It has been observed that the amplitude by which hormones are normally released seems to diminish in correlation with the glomerular filtration. Testosterone production is also disturbed and seems to be deficient, which is more common in people who receive dialysis (treatment of end stage renal disease).
Arthritis
The proportion of people with arthritis who report sexual dysfunction is high. There is no direct mechanism that explains the association, but it is multifactorial in nature.As arthritis increases physical disability and makes mobility an issue, it may be more difficult to assume various positions important for sexual functioning. Furthermore, chronic pain in the joints, as well as fatigue, may further mediate the sexual dysfunction. Moreover, depression is a common comorbidity of arthritis and may further worsen the feelings of inadequacy and pain, and, overall, lower the sexual desire.
Summary
To sum up, popular opinion perpetuates the idea of "asexual" older adults. But this is indeed not the case, although research shows that sexual activity declines with age. In women and men, the aging process increases the risk of sexual dysfunction, which may be partly driven by unfavorable lifestyle behav-iors. These are primarily associated with damage to the endothelium, which is important for normal physiological functioning, in various chronic illnesses (diabetes, obesity, hypertension, etc.) and their prevalence rises with age. There is a growing body of literature that suggests maintaining an active sex life as one ages is beneficial for a plethora of physical and mental health parameters, including a lower risk of early mortality. Physical activity is an emerging correlate of a satisfying and trouble-free sex-life in older adults, and sexual activity itself may be a form of physical activ-ity. Further research is required to elucidate the intricate relationship between physical activity and sexual activity.