3.1 Intro to Health Models in Hearing Rehab
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
what do rehab clinicans do?
educate and empower patient
facilitate communication with patients
partner in patient decisions
implement and optimise hearing technology
improve patient participant and quality of life
what does educating and empowering patients involve?
using a preventative measure rather than an intervention for damaging sounds in the environment.
patient education and counselling and advocacy for the use of hearing plugs in places with high noise exposure.
what does facilitating communication with patients involve?
appropriately communicating to patients if they have hearing impairment, recommending environmental modifications may help people in certain situations.
how does clinicians help in patient decision making?
shared decision making.
counselling patients on their hearing device options.
talking about the advantages and disadvantages of different interventions based on their lifestyle. Individualised treatment plan
how do clinicians implement and optimise hearing aid tech?
Fit devices and make sure they function properly over time and troubleshoot problems with devices (hearing aids, cochlear implants and assistive devices).
how do we improve participation and quality of life patients with hearing loss?
Individualised rehab plan and monitoring outcomes such as making sure interventions are working.
why does hearing rehab matter for hearing loss patients?
- Reduces social isolation
- Improves confidence in communication
- Supports independence
- Protects mental wellbeing
- Restores participation in work family and community life
rehab audiology involves:
- Ongoing relationships across lifespan of patients and changing needs
- Technical problem solving e.g. trouble shooting devices, optimisation of devices and lot of adaptation
- Translating complex technology (making it easier to understand for a client)
- Variety and unpredictability for different appointments
- Lifelong learning e.g. learn new and updated features of hearing aids released by manufacturers
to be a good rehab audiologist:
you need detailed knowledge of communication strategies, a good counselling approach and a broad overview of technology options and the features that are available for reach option.
good technical skills to troubleshoot and verify hearing aids.
as well as good interpersonal skills.
what is at the centre of rehab hearing care?
the person, making a person centred approach to hearing care highly effective.
individualise care.
education of hearing loss involves
explaining the options and their possible benefits and limitations.
setting realistic expectations e.g. hearing aids won’t restore hearing loss fully.
has to be able to be fitted into someone’s life and schedule e.g. if they work etc.
what are health models?
Conceptual frameworks for understanding health and functioning.
what relationship do health models look at?
the relationship between body structures and functions, activities, participation and influence of contextual factors (personal and environmental).
what do health models help clinicians do?
look beyond the impairment alone.
support holistic assessment (focusing on whole person) and intervention.
underpin person centred hearing care.
which health model does WHO use for hearing?
WHO International Classification of Functioning, Disability and Health (ICF) model
what is the ICF model describing?
classify health and health related domains.
what does ICF function as a bridge between?
Functioning as a dynamic interaction between a person’s health condition and their ability to perform tasks, their involvement in life situations, environmental and personal factors.
what does ICF focus on?
a person’s activity limitations and participation restrictions.
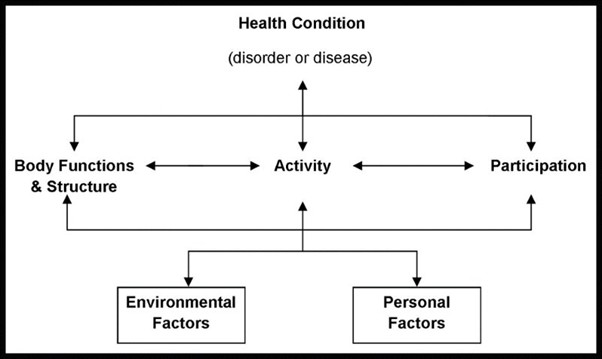
what are the domains of ICF?
Health condition (disorder or disease).
body functions and structure.
activity.
participation.
personal and environmental factors.
body structure and function ICF domain describes:
Body structures are anatomical parts of the body like organs, limbs and their components.
Impairment.
Body functions are physiological functions of body systems, including psychological functions.
sometimes there can be an impairment in structure or function or both.
activity and participation ICF domains describe:
activity
execution of a task or action by an individual.
limitations e.g. inability to run, unable to work, difficulty understanding speech.
participation
involvement in life situation
participation restrictions e.g. unable to participate in fun runs, unable to participate in conversations.
environmental and personal factors ICF domains describe:
Environmental factors
Individual e.g. home, school and workplace.
Services and systems.
e.g. work environment, health care systems, laws, informal rules.
Personal factors
e.g. gender, cultural background, other health conditions, motivation, lifestyle, education genetics etc.
why is ICF useful for clinical audiologists?
helps with:
clinical reasoning
case history helps to gather information to make informed rehab plan
readiness of client to go ahead with rehab plan
facilitators as in someone to help with the process e.g. closed one
planning and communication
individualised plans
depth of explanation- explain it in a way that client understands
outcome and evaluation
goal sitting based on participation restrictions
determine efficacy of rehab plan
what is the other determinant of health used by WHO?
Social Determinants of Health (SDH) Model
What are some examples of SDH?
- Income and social protection
- Education
- Unemployment and job insecurity
- Working life conditions
- Food insecurity
- Housing, basic amenities and the environment
- Early childhood development
- Social inclusion and non discrimination
- Structural conflict
- Access to affordable health services of decent quality
What are some of the things to think about when delivering hearing care?
- First nations
- Access to services
- Lower socio economic areas
- Regional and rural (geographically isolated, don’t have services available for access, or with fewer audiologists available)
- Historical barriers (loss of trust in government services due to past experiences)
- Cost and access to funding
- Health literacy (don’t understand the benefits and limitations of treatments options or understand the nature of their hearing loss)
what are some of the negatives of not getting enough access to hearing care?
Social isolation is strongly linked to poor mental and physical health
Low social support and trust are major predictors of poor health
Social disconnection can impact health more than smoking or obesity
Lower socioeconomic status is associated with lower social capital and poorer health outcomes
Case Example: Judy
Judy is a 68-year-old retired university lecturer who lives alone in a retirement village. She presents with increasing difficulty hearing in noisy environments and frequently mishears words in conversation.
She reports:
Missing parts of conversations at social gatherings
Not hearing the phone ring from another room
Turning the TV volume up high enough that neighbours have commented
Over the past year, she has gradually withdrawn from social events and recently resigned as secretary of her local card club because she found meetings “too exhausting.” She still enjoys small one-to-one conversations with close friends.
She is not eligible for government-subsidised hearing devices.
Her general health is good, although she has early macular degeneration and is concerned about her vision declining.
When asked what brought her in today, she says:
“I suppose I’m just getting older… maybe this is normal.”
She mentions that her daughter has suggested hearing aids, but Judy is “not sure she’s ready for that.”
describe ICF domains affected?
Disorder/disease:
Presbycusis age related sensorineural hearing loss.
Body structure and function:
Loss or degradation of sensory hair cells, increased listening effort, reduced speech perception.
Activity:
Cannot hear the phone ringing.
Cannot hear TV at a normal volume
Problems understanding speech in noisy environments.
Participation:
Resigned from the secretary of the local card club.
Withdrawing from social situations, reduced engagement.
Environmental factors
lives alone in a retirement village.
Not eligible for free hearing aid fitting.
Neighbour’s comment on TV volume, has a daughter who suggested aids.
Personal factors
Female 68 years old.
Tertiary educated.
Early macular degeneration.
Potential ambivalence about hearing aids.
which SDH factors affect Judy?
general socio economic, cultural and environmental factors.
Neighbourhood and built environment:
Lives alone in retirement village
Social and community networks:
Less active in community. Resigned from social events and role as secretary of local card club.
Individual lifestyle factors:
Withdrawal from social settings due to reduced hearing.
Health and health care:
Reduced hearing
Early vision issues
Access to some health care for free due to being covered partly by medicare
Economic stability:
No pension
Education:
Retired university lecturer.
How would social determinants of health change what you recommend for Judy?
Technology options and funding pathways.
Appointment structure and follow up.
Communication and counselling approach.
Depending on much funding Judy has it will depend on what hearing aid options are available.
Consider remote (virtual or telehealth) appointments to provide access to hearing care if Judy does not have much access to transport.
Provide an information leaflet on how to use hearing aid, how to put it on, and how to clean it to carers.
Might record things on your phone like how to do certain things so she can show a carer or family member that aspect.
Show the different features of hearing aid.
If rehab is successful for Judy what changes for her?
Reconnected to her social life and more socially engaged.
Might be back at the card club more and at more social events.