Anatomy | Development & Adult Anatomy of the midgut and hindgut (W2)
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
What is the origin of the ventral mesentery?
septum transversum (mesoderm)
What is the ventral mesentery made of?
Falciform ligament + Lesser omentum
What is the lesser omentum made of?
Hepatogastric ligament
Hepatoduodenal ligament
Foregut has both ventral and dorsal mesentery, whereas midgut/hindgut have ___
only dorsal mesentery
What is the dorsal mesentery made of?
Greater omentum, gastrosplenic ligament, splenorenal ligament
The artery supplying the intestine:
Passes through the midgut
Passes through dorsal mesentery
Axis of Rotation for the intestine
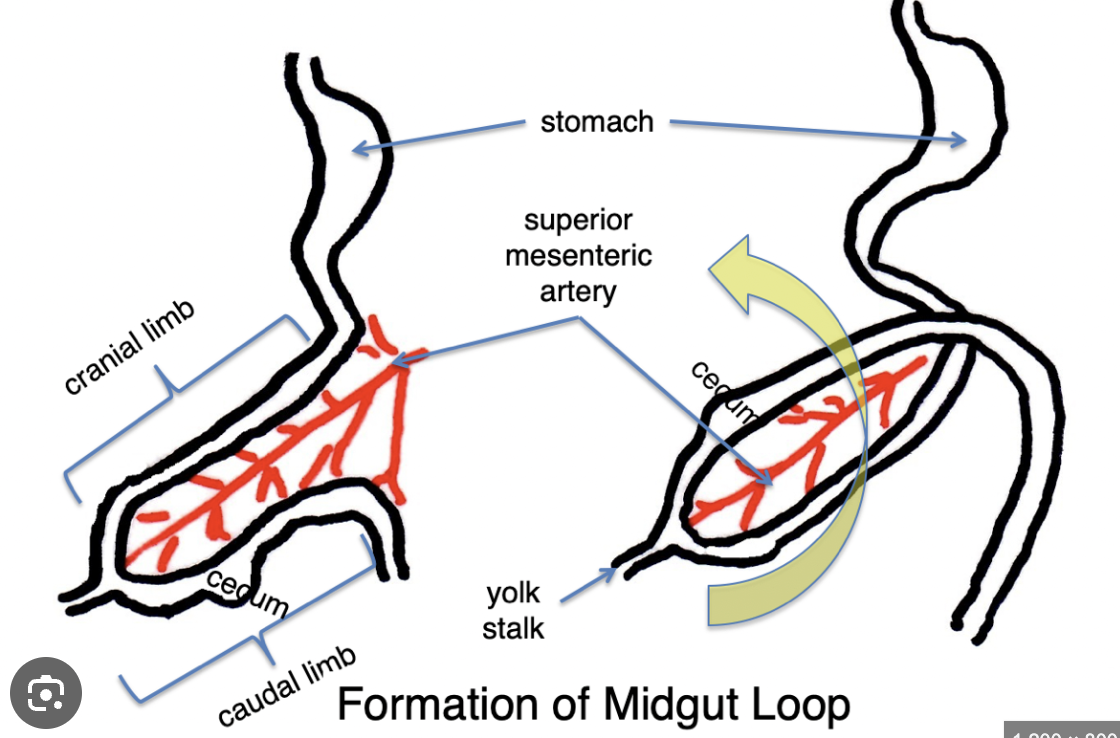
What artery supplies the midgut?
The superior mesenteric artery (intraperitoneal) which branches off from the dorsal aorta (which is retroperitoneal)
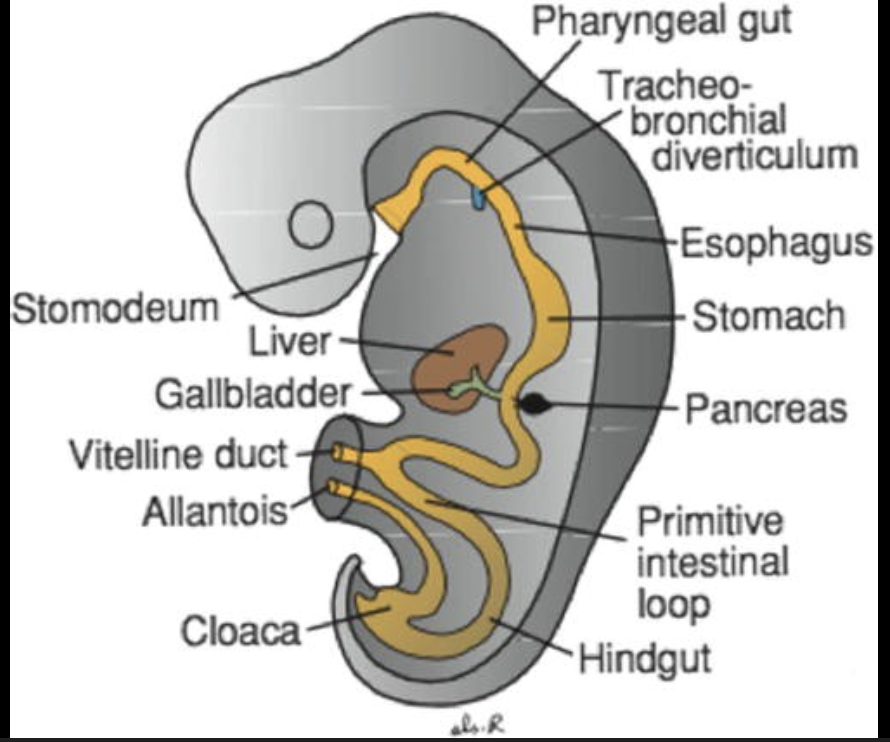
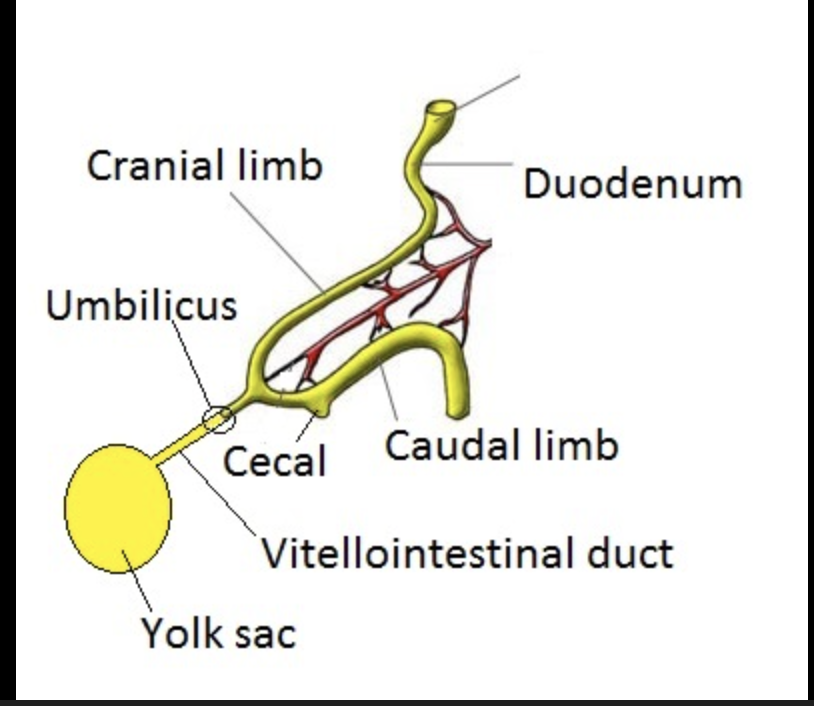
What is the vitello-intestinal duct?
A duct through which the umbilical cord passes.
What is the cranial and caudal limb of the midgut?
Cranial limb is the more superior part of the midgut, whereas the caudal limb is the more inferior.
What is necessary to accommodate the mid-gut loop size?
Herniation. However, if, through development, the midgut remains herniated, you end up with your small intestine outside the anterior abdominal wall.
During development, it is normal to have intestines “outside” of the abdominal cavity. T or F?
True, but they should migrate back inside to the abdominal cavity during development.
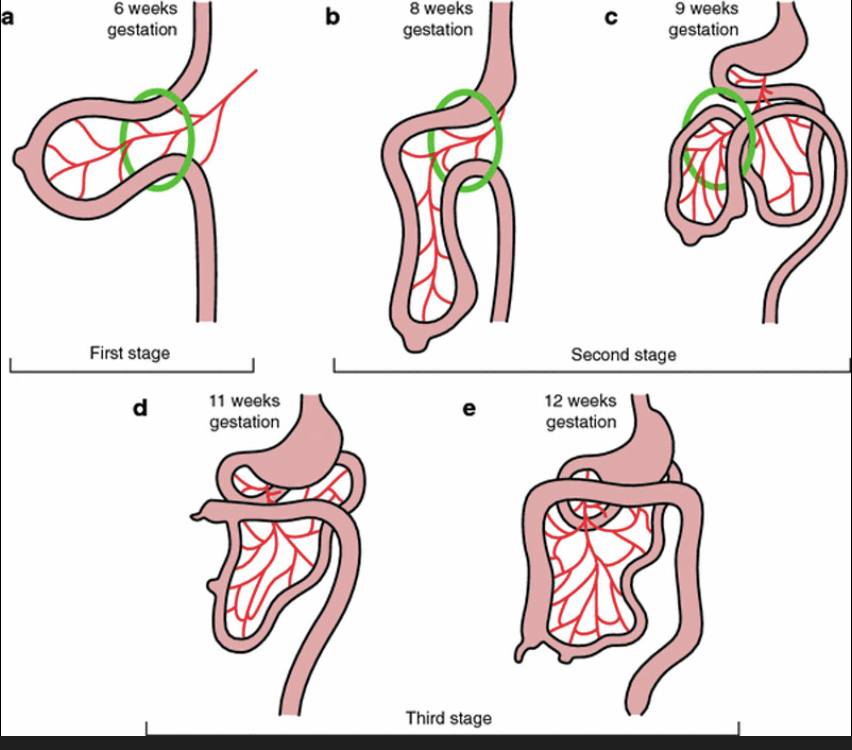
What happens after the herniation of the limbs into the umbilicus?
The differential growth of the limbs which causes rotation. The cranial limb grows faster and more exponentially than the caudal limb.
There is 90° counter-clockwise rotation around the SMA, which causes the caudal limb to end up superior to the cranial limb.
The midgut loop becomes the transverse colon
What limits or controls the extent of rotation?
The peritoneum. We do need to limit the amount the midgut rotates, because at the same time this occurs, the foregut is rotating. Too much rotation would lead to a crazy loop.
What are the two retention bands which limit the extent of rotation of the midgut?
Superior Retention Band — Ligament of Treitz
Inferior Retention Band — Phrenico-colic lig
They are each thickenings of the peritoneum.
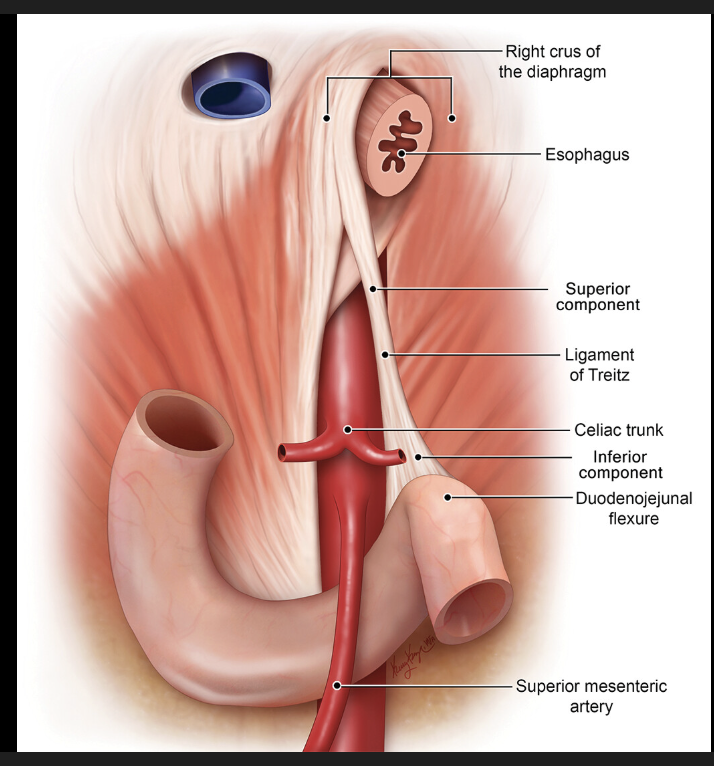
The Ligament of Treitz is the suspensory ligament of the duodenum, and is derived from:
diaphragm (skeletal) and duodenal (smooth) muscle fibers
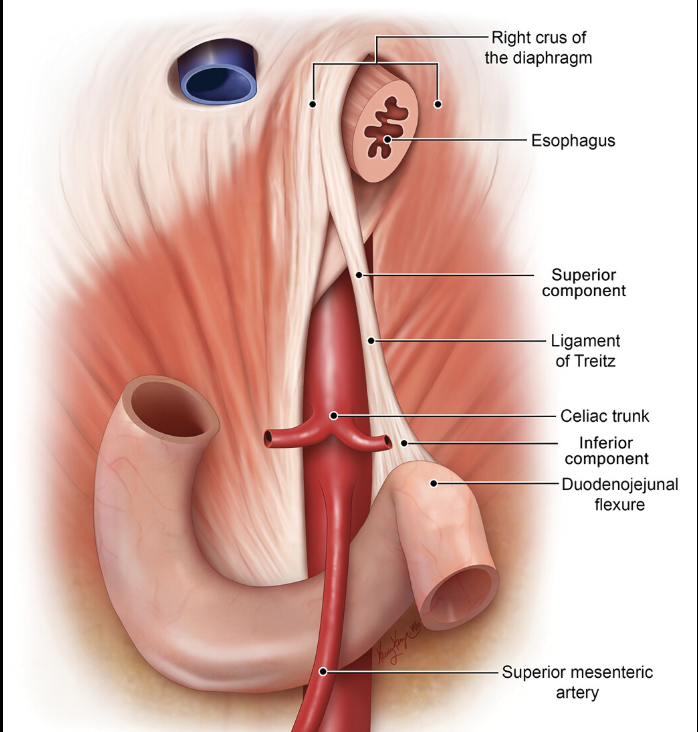
What does the phrenicocolic ligament connect?
It is part of the dorsal mesogastrium, and it connects the peritoneal extension of the diaphragm to the colon.
After the end of cranial and caudal limb folding, where do the cranial and caudal limbs end up?
The cranial limb flops to the right and forms the small intestine (+duodenum)
The caudal limb flops to the left and sticks to the posterior abdominal wall. It forms the left 1/3 of the transverse colon & the descending and sigmoid colon
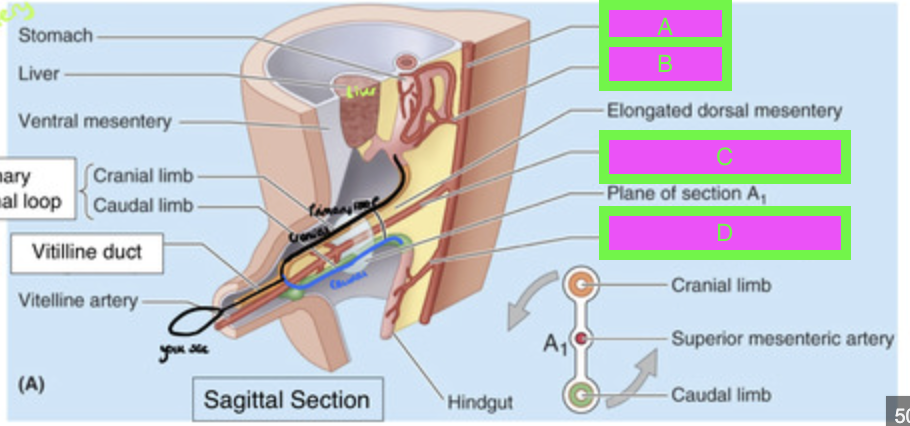
Label A-D
A → aorta (retroperitoneal)
B → celiac trunk
C → Superior Mesenteric Artery (in between the cranial and caudal limbs)
D → Inferior Mesenteric Artery
Portions of the duodenum in the midgut are ___-
Secondarily retroperitoneal (it is posterior body wall)
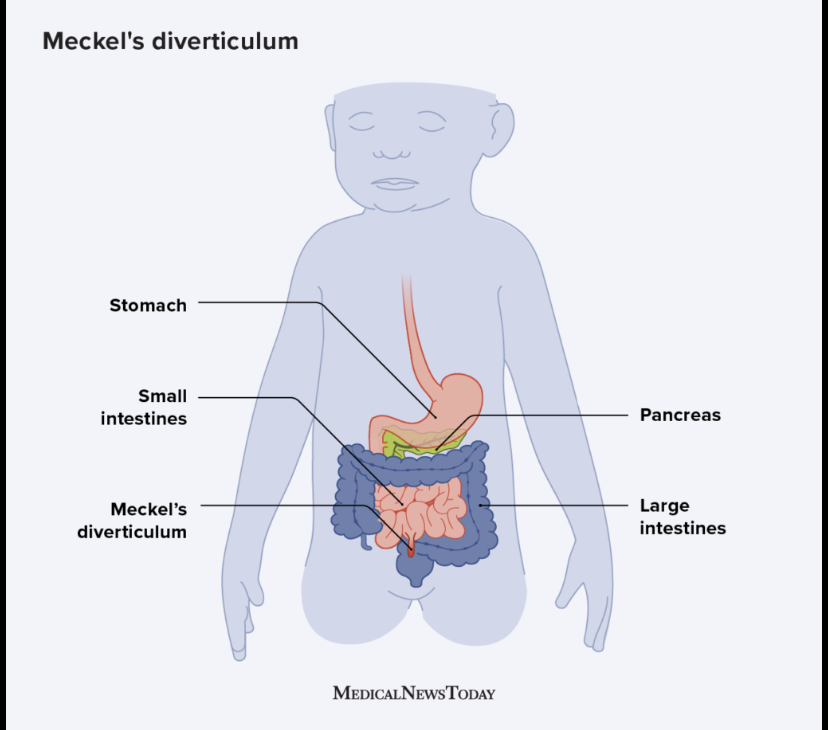
What is Meckel’s Diverticulum?
A continuation or retention of the Vitello-Intestinal duct, which means part of the intestine connects to the umbilicus. Can be painful and dangerous (risk of cutting of blood flow, infection).
The ascending colon and descending colon are ______ whereas the transverse colon is _______
secondarily retroperitoneal; intraperitoneal
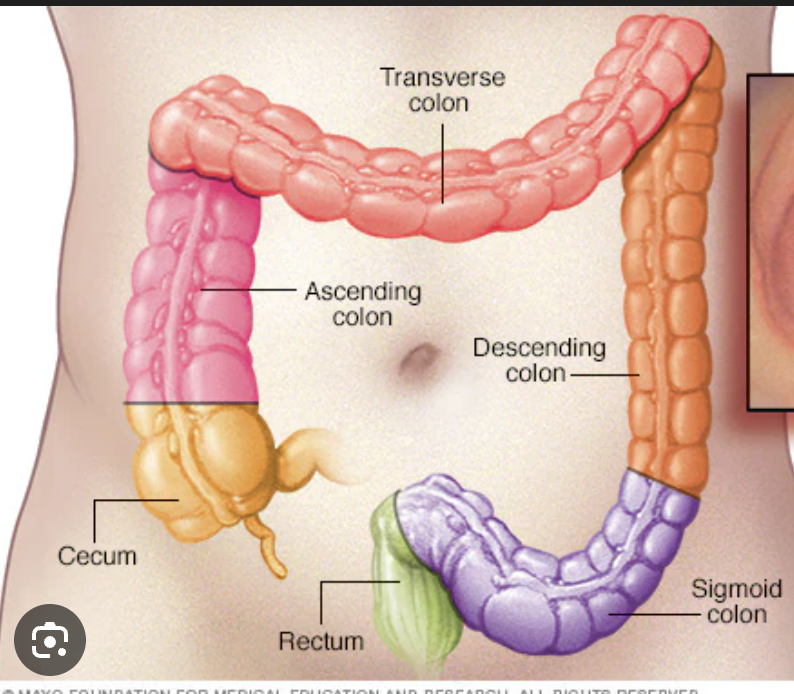
What determines the position of the appendix?
The extent of the growth of the ascending colon inferiorly. The appendix’ position is thus variable.
Appendicular pain is felt ________
Anywhere from the right upper quadrant all the way to the right lower quadrant. Even if the actual adult position of the appendix is in the right lower quadrant, because of the path of its embryological development, pain in the appendix can be referred all the way along the right path.
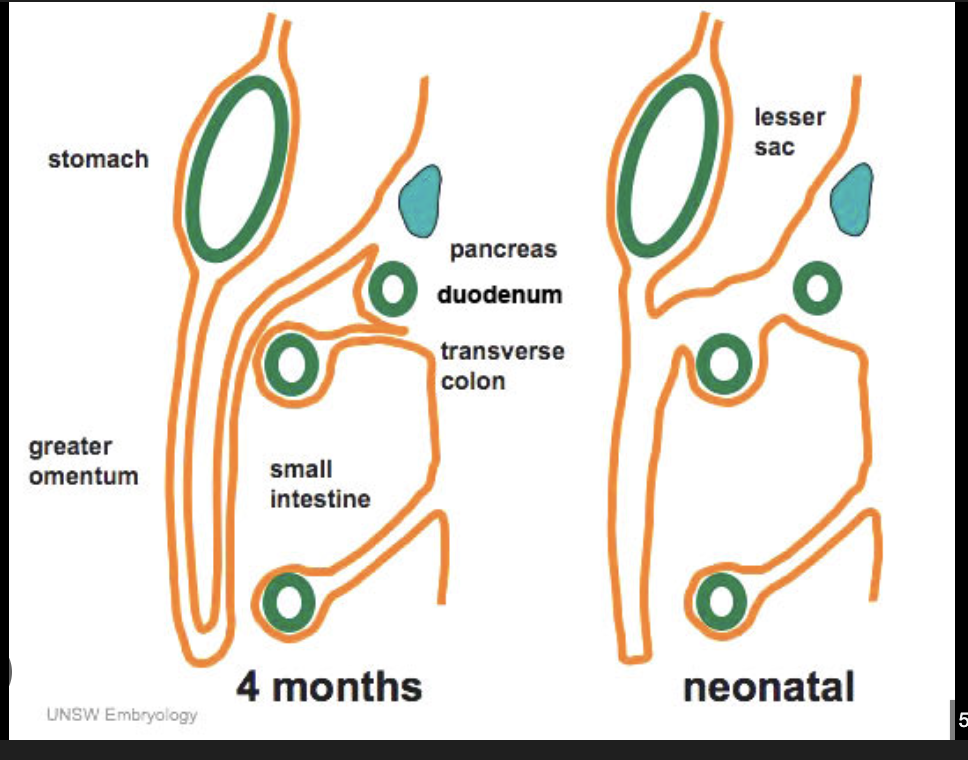
What is the greater omentum?
A large fold of visceral peritoneum that hangs down from the greater curvature of the stomach and transverse colon and covers the small intestine.
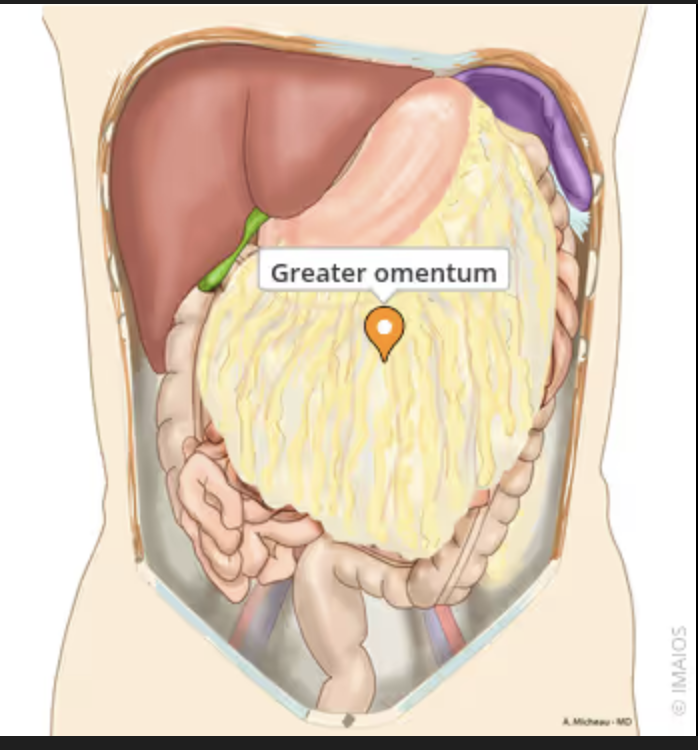
What is the greater omentum comprised of and how many layers is it?
It is comprised of dorsal mesentery.
It is often described as 4x (two double layers) layers (the folding back connecting the stomach and colon, and the two layers of dorsal mesentery growing from the back.
How can the greater omentum respond to infections?
if it senses an infection, it will migrate to that site of infection and wall that site off from the rest of the abdomen. However, the omentum has its own innervation, so as it twists and turns to cover off the site of infection, that can cause pain.
What artery supplies the hindgut?
Inferior Mesenteric Artery
What is the cloaca?
A single pouch that needs to separate anteriorly into the bladder, and posteriorly into the rectum/anus.
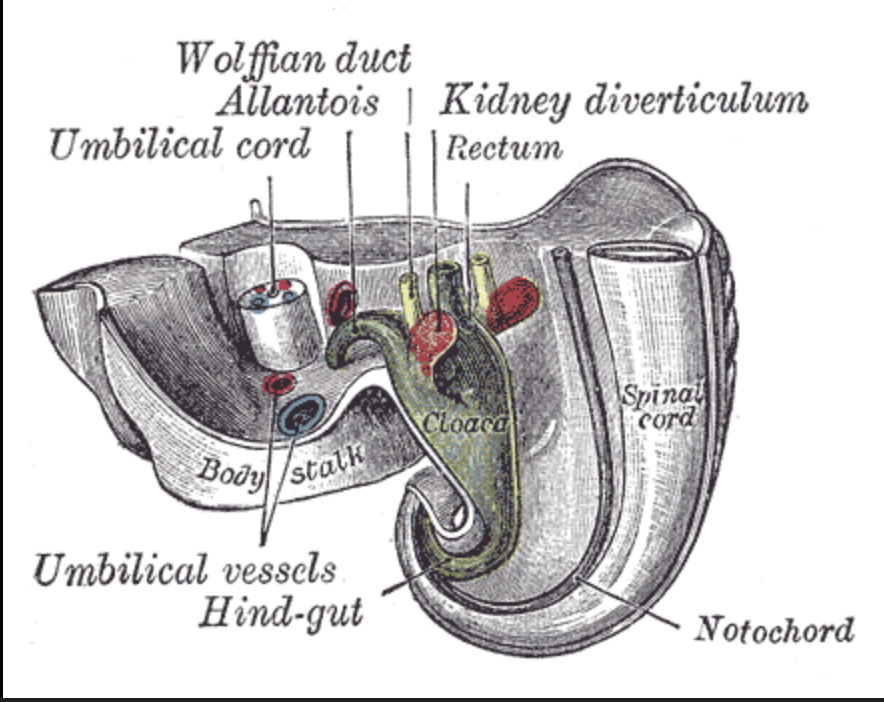
How does the cloaca separate into the bladder and rectum in humans?
Epithelium from the anterior body wall grows in and separates the bladder from the rectum. This epithelium forms what is called the urorectal septum.
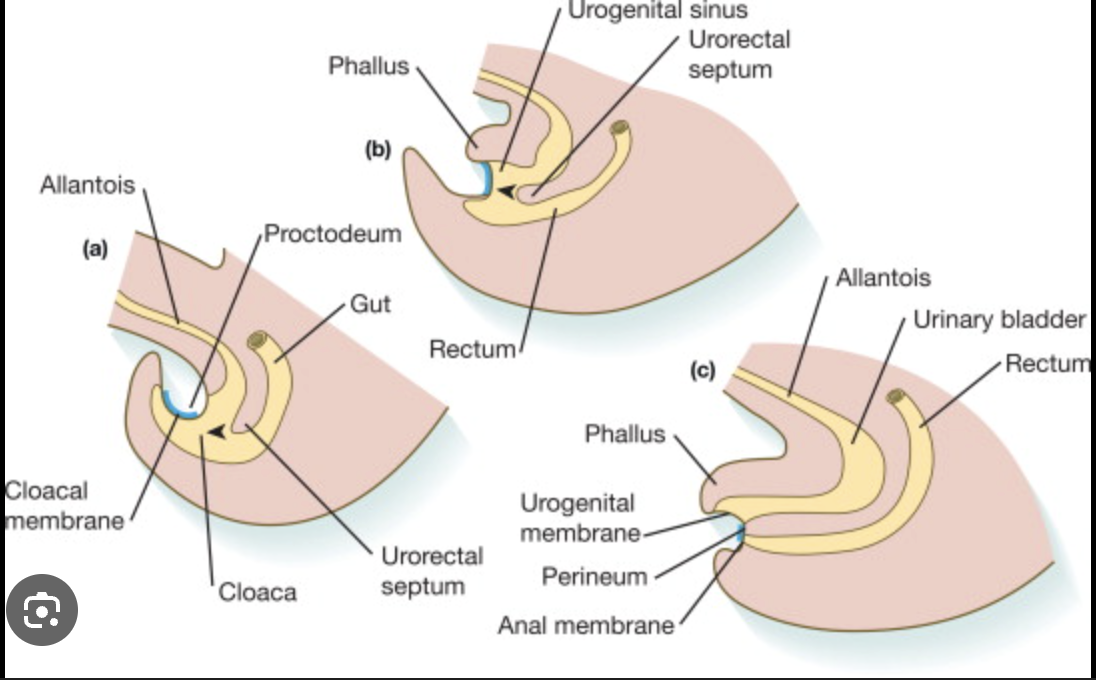
If we don’t separate the cloaca, this leads to ______
Mixing of urine and faeces
If we don’t disconnect the hindgut from the anterior abdominal wall, this leads to _____
Urine dribbling out of the belly button.
What organs make up the hindgut?
Distal 1/3rd of the transverse colon
splenic flexure
descending colon
sigmoid colon
ano-rectal junction
What happens after hindgut development?
The internal gut tube needs to meet the external ectoderm. They do so at the pectinate line, a point where the ectoderm invaginates to meet the endoderm.
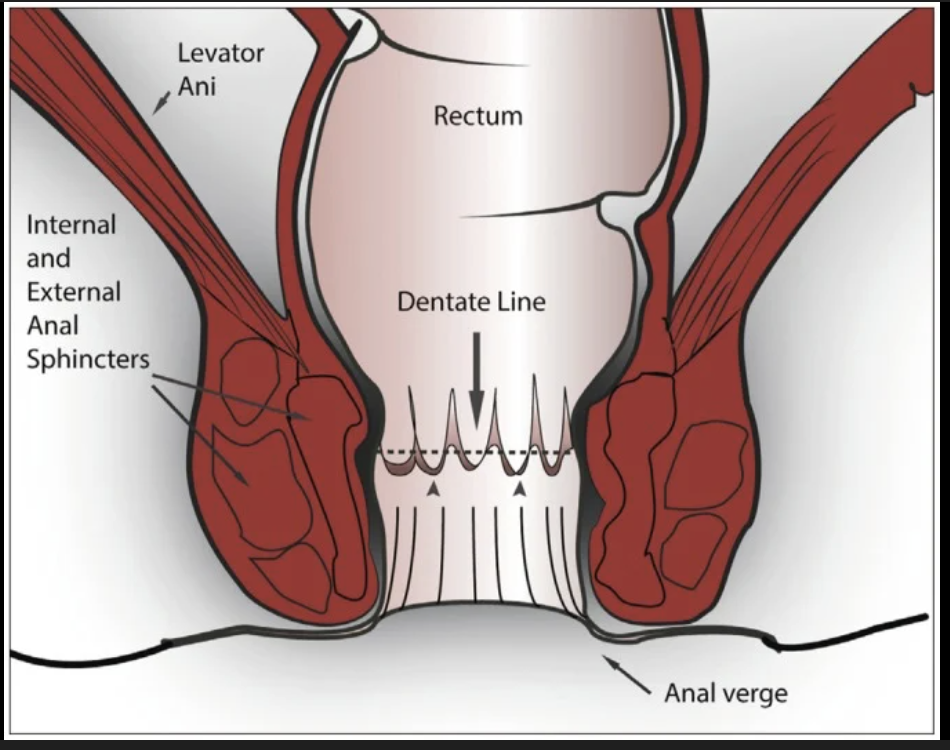
What is the clinical significance of the pectinate/dentate line?
Innervation and vascularisation of the rectum superior to the pectinate line will be deeper and more visceral, whereas inferior to it will be more superficial (which is more keenly felt).
Hemorrhoids inferior to the line are more painful.
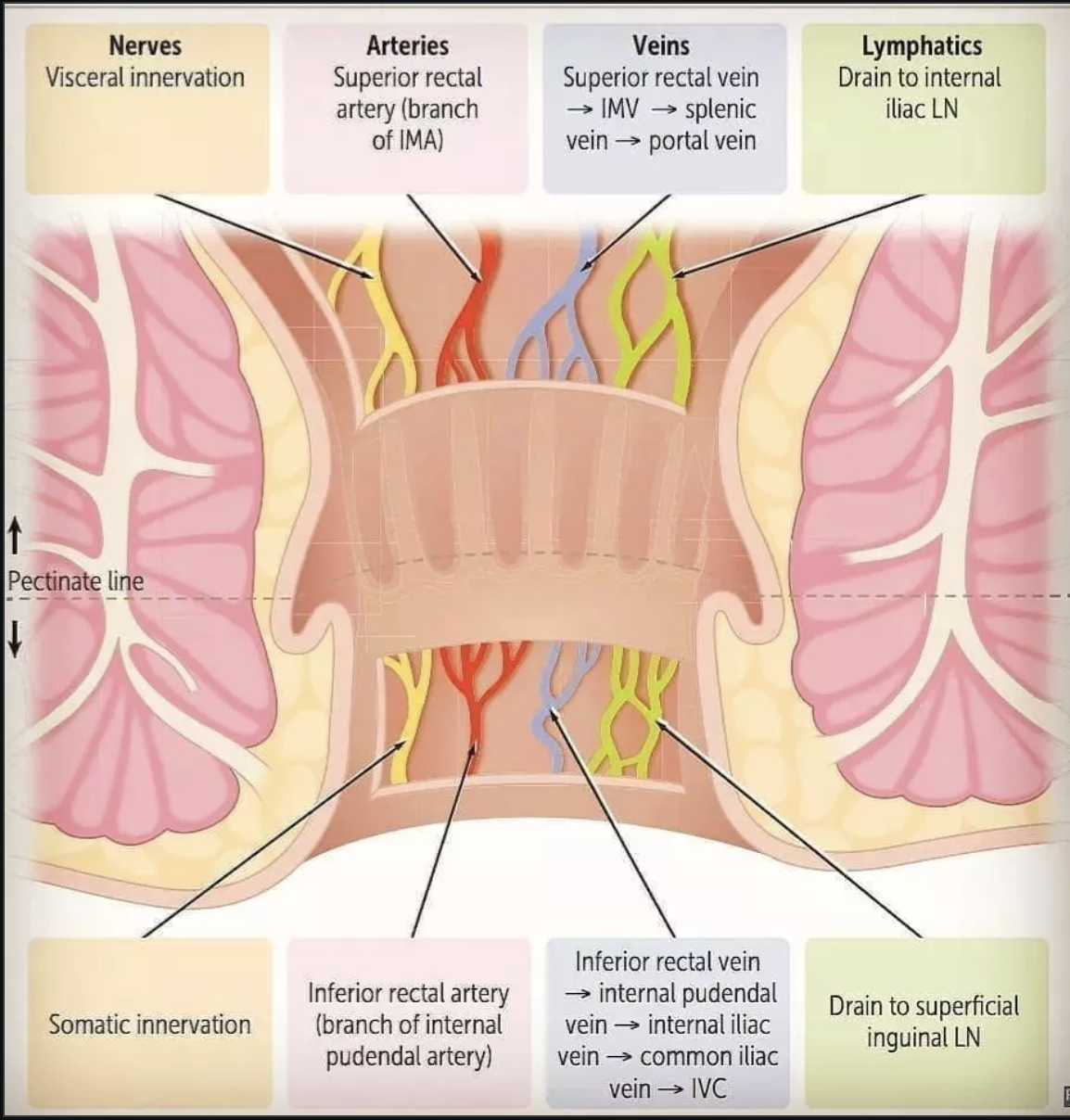
How does lymphatic drainage differ on either side of the pectinate/dentate line?
Superior → internal iliac lymph nodes
Inferior → superficial inguinal lymph nodes
What are the epithelial differences above and below the pectinate line?
Superior → Columnar
Inferior → Stratified Squamous
What are the Arterial Supply differences above and below the pectinate line?
Superior → Superior Rectal artery
Inferior → Inferior Rectal Artery
What are the lymphatic drainage differences above and below the pectinate line?
Superior → internal iliac nodes
Inferior → inguinal nodes
What are the innervation differences above and below the pectinate line?
Superior → visceral (only sensitive to stretching, insensitive to cutting, burning)
Inferior → somatic (very sensitive to pain, touch, temperature)