PSYC 401 - Midterm 2
1/108
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
109 Terms
Krishnamurthy et al. (2004) - competency in psychological assessment
overview of issues related to development of assessment competencies
proposed 8 specific competencies for psychological assessment
8 specific competencies in psychological assessment
background in psychometric theory (statistics, test construction)
knowledge of scientific, theoretical, empirical, contextual bases of assessment (interpreting scores, confounding variables)
knowledge of different psychological theories and their assessment
assess outcomes of treatment/intervention
ability to evaluate roles, contexts that patients and psychologists function in/reciprocal impact of those roles on assessment
establish/maintain collaborative professional relationship
understand relationship between assessment and intervention
technical skills (problem identification, appropriate assessment, systematic data gathering, integrate info, communicate findings, provision of feedback)
psychological assessment
evaluation of an individual who is experiencing some difficulty so that info gleaned can be useful in dealing with the problem using tools such as tests, interviews, case studies, behavioural observation, specially designed apparatuses
goals of psychological assessment
problem explication
formulation
prognosis
treatment issues and recommendations
provision of therapeutic context
communication of findings
problem explication
establishing a formal diagnosis based on classification systems that exist or a description of diagnostic picture without providing a formal diagnosis
diagnosis
assigning diagnostic category or label
generated through structured interviews
uniformity of disorders
classification into categories
formulation
attempt to explain genesis, maintenance, process related info in a person for treatment
generated through psychological assessment
viewed as more important than diagnosis
each person seen as unique
involves the patient
based on theoretical perspective of psychologist
info used in formulation
intraindividual issues (motivation, learning, cognitive styles)
interpersonal issues (relationships)
environmental issues (life events, living situation)
process-related issues (behaviours during interview)
content info (what patient provides/says during interview)
prognosis
expected course, degree and speed of recovery - not always clear solely based on diagnostic info
treatment
based on psychologist’s knowledge of treatments and diagnosis/formulation info
influenced by factors like intelligence and psychological mindedness (ability to observe own internal life, insight)
assessment in research
provide info regarding nature of disorder (severity of symptoms, comorbidity, co-occurrence of other symptoms)
determine efficacy of treatments for specific disorders
actuarial approach to making clinical decisions
scores on measures are used in statistical formulae in making decisions
quantitative
clinical judgement approach to making clinical decisions
clinical experience and clinical intuition are used
qualitative
testing vs. assessment
testing is administering, scoring, interpreting psychological tests
assessment uses many data sources to arrive at conclusions regarding psychological problems (broader)
assessment vs. diagnosis
diagnosis identifies/documents a patient’s symptoms to classify into a category
assessment collects broad info that interact to determine patient’s subjective experiences
psychodiagnostic assessment
gather clinical data on problem experienced, process info, first clinical exposure for people, initiate and develop therapeutic alliance, context for understanding difficulties
clinical interview most common
utilize tests and tools - multimethod approach
data gathered in psychodiagnostic assessment
demographic
presenting problem
history of problem
medical history
current and past living situation
family history
childhood, early adult history
previous treatment
most common clinical tests
clinical interview
Wechsler Adult Intelligence Scale
MMPI-2
sentence completion
thematic apperception test
Rorschach inkblot test
Bender-Gestalt
drawing tests
Beck depression inventory
Wechsler intelligence scale for children
intellectual/cognitive assessment
determination of intellectual and cognitive functioning/strengths
behavioural assessment
determine antecedents, reinforcement histories, maintenance issues for psychological/behavioural problems
health assessments
determine behaviours, personality structures, environmental features that influence patient’s physical health status
psychophysiological assessments
heart rate, skin temperature, muscle control that are factors in physical/psychological health problems
rehabilitative assessments
determine functional capacity of individuals following psychological/physical injuries
forensic assessments
determine factors that may have contributed to criminal behaviour, likelihood of reoffending, treatment of issues pertaining to criminal behaviour
idiographic approach to assessment
understand an individual, couple, family, and psychological issues that pertain to them (specific, detailed)
typically done for treatment planning
nomothetic approach to assessment
assessments done on groups in order to understand broader issues/constructs pertaining to types of problems or treatments
typically done in research
tools of psychological assessment
tests
techniques
techniques
tools that provide relevant clinical info that does not necessarily involve patient reporting on his own behaviour, often compared to norms - help with hypothesis generation
semi/unstructured interviews
projective techniques
behavioural observations
less reliable/valid than tests
purposes of clinical interviews
gathering clinical data on difficulties
info about process-related variables (like how comfortable they are with the therapist)
provides first clinical exposure for many
opportunity to initiate/develop therapeutic relationship
context for understanding nature of difficulties
interview skills
develop rapport
primary active listening (open ended questions, paraphrasing, clarifications, summarizing, minimal leading)
secondary active listening (normalizing, structuring, probing)
nonjudgemental
awareness of nonverbal behaviour/subtle changes
ability to connect disparate kinds of info
psychic determinism
everything has some goal, meaning, purpose, and cause - clinician needs to pay attention to all behaviour that patient exhibits
mental status exam
focuses on patient’s
appearance
behaviour
orientation to time, place, person
memory
sensorium
psychomotor activity
states of consciousness
affect
mood
personality
thought content and process
intellect
judgement of insight
during treatment
non-structured interviews
not trying to diagnose or formal formulation, create a positive interpersonal experience and beneficial internal development for patients
help person feel better main goal
Freudian approaches includes initial unstructured interview
semi-structured interviews
flexibility of interaction between patient and clinician
can talk about whatever issues come up and clinician can probe
clinician does have some info tries to obtain to develop diagnostic and formulation info
pros of semi-structured interviews
rapport
flexibility
modifiable
not limited to certain tools or norms
useful and commonly used
cons of semi-structured interviews
reliability and validity from clinician to clinician (?)
lacks reliability
may be susceptible to clinical biases
not good for research
structured interviews
based on very specific diagnostic criteria from current nomenclature
very highly structured in terms of info sought
purpose is to provide clear diagnosis and really interested in other domains
pros of structured interviews
reliable
good research tool
modules for specific disorders
cons of structured interviews
content constrained by diagnosis
time consuming
no other pertinent info gathered
not as conductive to establish rapport with patient
process info not focused on, just content
major sources of error by clinical psychologists
base rate issue (how common behaviour is)
barnum effect (common statements worded to sound rare)
illusory correlation
preconceived ideas/confirmatory bias (look for evidence that supports ideas)
inappropriate use of heuristics (cognitive shortcuts)
objective tests
tests where items are presented the same to all and options for responding are the same - measures characteristics that the responder is aware of (surface level)
IQ tests, self-report tests, items describing some behaviour
pros of objective tests
economical
administration and scoring is easy
objective
quite reliable
cons of objective testing
surface or behavioural in nature only
single summary score not representative
transparency in meaning
response sets
patients answering in ways that present a false picture of themselves to the clinician
underreporting or over-reporting of psychopathology
acquiescence or non-aquiescence
carelessness or inconsistency
self-deception
clinical objective test
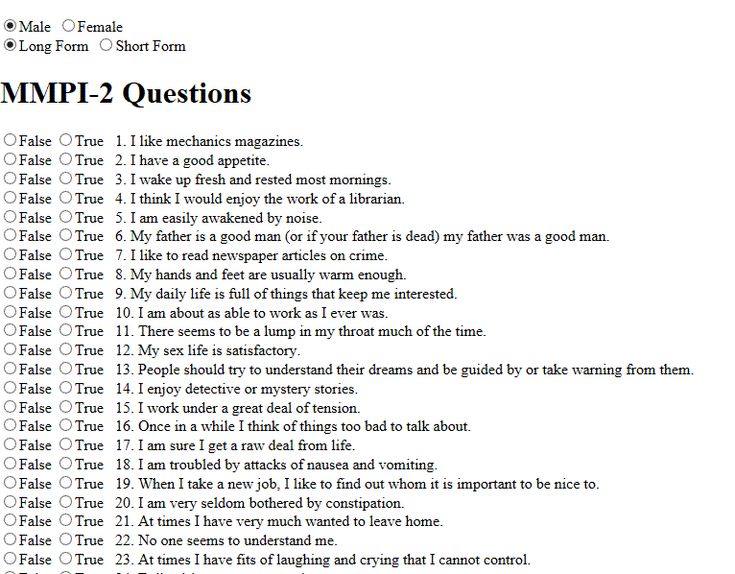
Minnesota Multiphasic Personality Inventory
Personality Assessment Inventory
Millon Clinical Multiaxial Inventory
construct validation test construction
review lit and case studies to understand qualities of test variable
train item writers to write questions that capture different aspects of the variable
use statistical reliability approaches to pare items down
empirical criterion keying test construction
administer a bunch of questions to two different groups and find a question that discriminate the two groups
determine if the questions are able to generate differences
Minnesota Multiphasic Personality Inventory (MMPI)
one of the most frequently used tests
used criterion keying approach
measures personality and psychopathology
13 scales: 3 validity and 10 clinical
use: initial screening for psychopathology, personnel selection, marital therapy, treatment outcome studies
MMPI scales
hypochondriasis (germs/bodily concerns)
depression
hysteria (self-centred, reactive)
psychopathic deviate (asocial/antisocial)
masculinity-femininity (aesthetic interests, confidence)
paranoia
psychasthenia (anxious, obsessive)
schizophrenia
hypomania (excessive activity, lacks direction)
social-introversion
+3 validity scales
MMPI pros
strong empirical basis
body of research
good reliability/validity
well-known/respected
lots of clinical info
ease of administration
objective/comprehensive
MMPI cons
excessive length
standardization sample
not sure if MMPI research can be generalized to new revisions
labels antiquated
normative sample not representative
interpretative process complicated
MMPI validity checks/response biases
L: questions to measure if someone is lying (lie scale)
I: questions to measure if someone isn’t paying attention/exaggerating (unusual/severe psychopathology)
K: questions to measure defensiveness/assertiveness
MMPI clinical scales
Neurotic spectrum: 1,2,3,7
Psychotic spectrum: 6,8,9
Psychopathic: 4
MMPI interpretation
validity (proper conditions for testing established) → pattern interpretation → incorporate with other scales
not simply evaluation equaling diagnosis
MMPI-A
MMPI/MMPI-2 version for adolescents - dropped some items, reworded some items
MCMI
measure of personality and psychopathology
28 subscales
directly accords with DSM criteria
pros of MCMI
developed from comprehensive theory
reflects current DSM and is useful with personality disorders
takes into account base rates
strong test construction approach
easy to administer
shorter to administer
cons of MCMI
imbalance of T/F questions
test is weak in assessing subclinical levels of psychopathology
validity problems
PAI
344-item measure with 22 subscales measuring clinical syndromes and and personality variables - measures symptoms of disorder from mild to severe and underlying pathology
projective tests
use ambiguous stimuli instead of objective - subject has to impose their interpretation (reveal part of themselves)
can have standardized administration, but possible responses not pre-determined
behaviour assessed at deeper level
measures psychological states, personality, underlying psychological makeup (defences, coping)
response determination
a response is not an accident, but a function of subject’s psychological attributes
types of projective tests
association (what visual/auditory stimulus is associated with) - RIT
construction (drawing) - TAT
completion (sentence completion)
choice/ordering (picture arrangement)
expressive (role play)
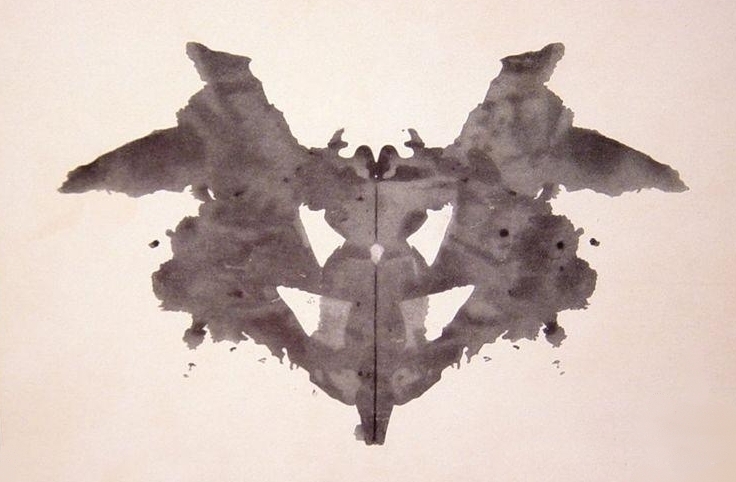
rorschach test
interpretation of ambiguous inkblots
Mirror image score
Free association stage → inquiry stage → interpretation stage
clinically/research validated from Exner’s comprehensive system
rorschach criticisms
poor psychometrics
non-empirical basis for scoring/interpretation
methodological
lack of standardization procedures
rorschach inquiry stage
code
location
determinants
form level (ability to form pictures)
content
popularity of responses
organizational activity
rorschach interpretation stage
assess
info processing
cognitive mediation
ideation
capacity for control/tolerance for stress
affect
self-perception
interpersonal perceptions/relations
rorschach pros
easy to administer
standardized administration, scoring, interpretation
large normative sample
acceptable reliability/validity
taps info not tapped by objective tests
may be resistant to faking
rorschach cons
not developed for purpose currently used for
early research created confusion/bias
lack of research for minorities
additional reliability/validity needed
complex scoring/interpretation

thematic apperception test (TAT)
measures motivational, interpersonal, social-cognitive aspects of functioning - asks participants to interpret photo cards
thought to reflect underlying processes
TAT scoring
not really scored, more themes determined based on a variety of domains (drives, relationships, conflicts, defences, ego strength) - find common themes
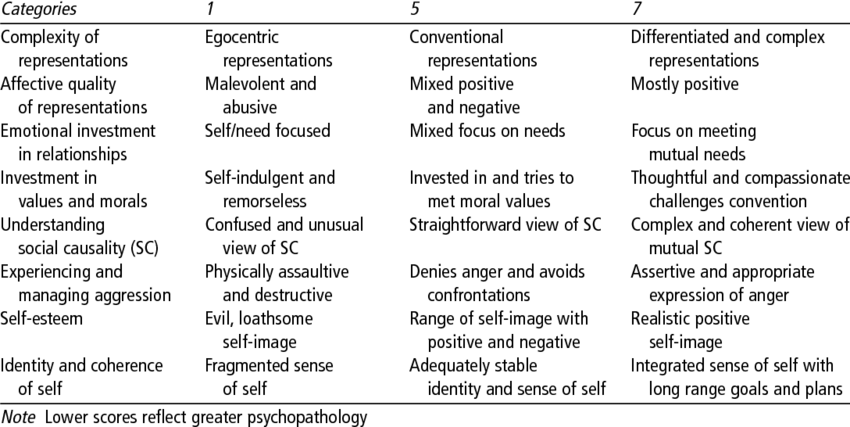
social cognitions and object relations scale
measures complexity of object relations, affect tone, capacity for emotional investment in relationships, understanding social causality
social cognitions and object relations scale pros
potentially valuable to assess deeper aspects of personality
focuses on global aspects of person’s interpersonal and motivational world
aids in development of rapport
adequate reliability and validity of some scoring and interpretive schemes
social cognitions and object relations scale cons
no standardized administration or normative data
general reliability and validity are difficult to establish
subjectivity in scoring and interpretation
drawing tasks
access parts of personality not accessible with objective tests or bypass defences - interpret personality, assess interpersonal relationships
given a paper and asked to draw certain objects, places, people
psychodynamic perspective of therapy
trying to uncover relational features of problems person is experiencing - relations over instincts
need to take info about the person in to diagnose them properly
scientific approach to clinical work
based on info available, develop a model/theory of human behaviour that guides behaviour in attempt to understand
develop hypotheses to test based on the model/design, appropriate means to asses model
alter, accept, refute model
formulation approach to clinical work
develop hypothesis model of unique person seeking help, alter details of model for each person
model guides behaviour of therapist in attempting to understand individual and effecting change
psychodynamic formulation
aim is to increase treatment efficacy
understanding idiosyncratic way individual organizes knowledge, emotions, sensations, experiences, behaviour allows therapist to have more choice
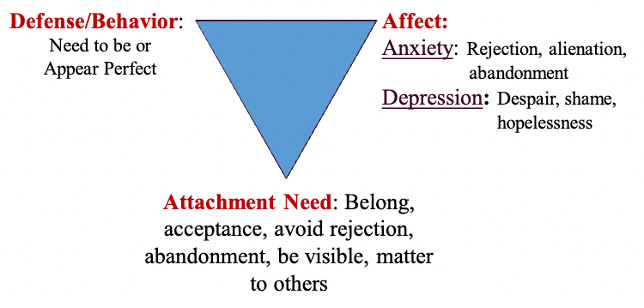
triangle of adaptation
cycle of person’s attachment needs, associated affective states when attachment needs are not satisfied, and the defences/coping mechanisms to cope with lack of satisfaction
triangle of object relations
cycle of relationships a patient goes through while in therapy
current relationships (including self) → past relationships → therapist
foundational assumptions of case formulation
understanding of personality and interpersonal patterns essential to therapeutic work
one’s wishes/needs underlie interpersonal patterns (often unmet with problematic behaviour)
psychodynamic underpinnings of therapy concepts
attachment needs are often unconscious
anxiety/affect are often generated by frustrated/unfulfilled attachment needs
defences are means of coping with unwanted anxiety/affect
concepts of self is related to triangle of adaptation which subsequently shapes relationships in triangle of object relations
defences
manifest themselves as behaviours and can define interpersonal transactions
activated in effort to maintain ego integrity and psychological homeostasis
well-adjusted individuals possess repertoire of defences appropriate to context in which they are applied
use of triangles in treatment
explore past and current relationships
watch for examples of development of perfectionistic behaviour in treatment
explore interpersonal precursors or motivators/fears for perfectionistic behaviour
look for how relationship with therapist is similar to past/current relationships
work towards other ways of attaining interpersonal needs
CBT case formulation
marry unique experience of client with skills, theory, knowledge of therapists to understand/alleviate client’s presenting issues
developed from cognitive model (how we view selves, world, future determines emotions/behaviours)
develop disorders when people have unhelpful patterns on interpretations and behaviours
effective treatment - modifying unrealistic thinking through promoting client strengths/resilience affects emotional wellbeing
contains all of patient’s symptoms, disorders, problems and the mechanisms/precipitants behind them
collaboration between therapist/client is key
developing formulation for problems
list all problems, symptoms, etc - data from multiple sources including clinical interview, structured diagnostic interviews, self-report scales, self-monitoring data provided by patient, observations of patient’s behaviours, reports from family + other
mechanism hypothesis (what maintain symptoms)
developing formulation for mechanisms
heart of formulation
mechanisms/processes/symptoms maintaining disorder - include biological mechanisms, but emphasize and focus on psychological mechanisms
developing formulation for precipitants
determine events, situations that give rise to problems, symptoms, disorders throughout treatment
look for earlier events that might reflect origins
levels of formulation
case
disorder or problem
symptom
5 ps of case conceptualization
presenting
precipitating
perpetuating
predisposing
protective
presenting
present patient problems in terms of emotions, thoughts, behaviours
goes beyond diagnosis and tries to define current problems
define short, medium, long term goals
clarify problems, establish therapeutic connection
precipitating
proximal (close to manifestation of problem) external and internal triggers
introduce cognitive model
initial focus on cognitions
perpetuating
internal and external factors that maintain the problem
focus on interrupting the cycle
quality over quantity
predisposing
distal (contributors to problem occurring at any time) internal and external vulnerability factors
longitudinal understanding of problems
protective
person’s resiliency and strengths
attempts to build on these for treatment
key characteristic of 5 Ps of case conceptualization
based on cognitive model
involves concepts like schemas, assumptions, rules, maintenance cycles of thoughts, emotions, behaviours
formulation in levels from presenting issues to predisposing factors
complementary to diagnoses
when do formal assessment originate?
began in early 1900s - Alfred Binet’s intelligence testing among children, WWII military personnel sorting
where else can you find assessment?
education
neuropsychology
medicine
industrial and forensic psychology
contemporary theories of personality
trait-based (stable behavioural dispositions)
dynamic (unconscious, psychological processes and structures, mental representations)
5 principles of personality tests
core features of personality are relatively stable over time
expression of traits and dynamics varies across gender, culture, age
assessment of traits/dynamic often requires different approaches
traits are dynamic, dynamics are trait like
personality assessment is inextricably interpersonal