GALLBLADDER
1/90
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
91 Terms
the gallbladder stores what
bile
diameter of GB should be:
< 4cm
longitudinal of normal GB should be:
< 10cm
normal gb wall thickness should be:
< 3mm
cystic duct should be how long?
4 cm long
CHD DIAMETER
<4MM
CBD DIAMETER
6MM
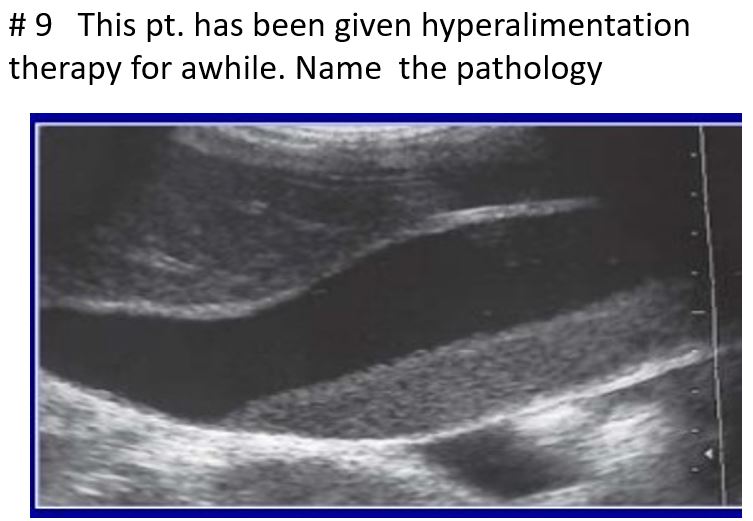
prolonged fasting, hyperalimentation therapy, or with obstruction of the gallbladder.
May be asymptomatic
Gravity dependent
Prominent GB size
Some gallbladders may be so packed with this
Occasionally found in the common duct.
slowly resettle as the patient changes their position
abnormal finding because either a functional or a pathologic abnormality exists when calcium bilirubin or cholesterol precipitates in bile
will not present with gallbladder wall thickening or internal vascularity
may also be seen in combination with cholelithiasis, cholecystitis, and other biliary diseases.
Sludge
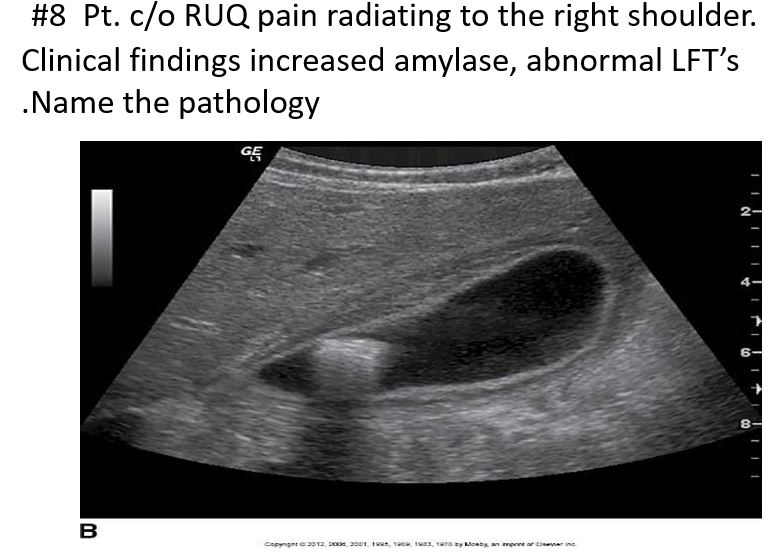
increased Serum amylase / alkaline phosphatase
positive Murphy sign
fever
leukocytosis
found 3x more frequently in females than males over 50, but it has a similar incidence in higher age groups
Abnormal LFTs
gb wall >3mm
Distended gallbladder lumen >4 cm
Gallstones
Pericholecystic fluid collection
Acute Cholecystitis
Repeated episodes of acute cholecystitis
≥ Serum amylase
Abnormal LFTs
No significant tenderness
Symptoms are often milder and may only occur during or after meals (due to gallbladder contraction).
Chronic Cholecystitis
is the most common form of gallbladder inflammation.
Chronic cholecystitis
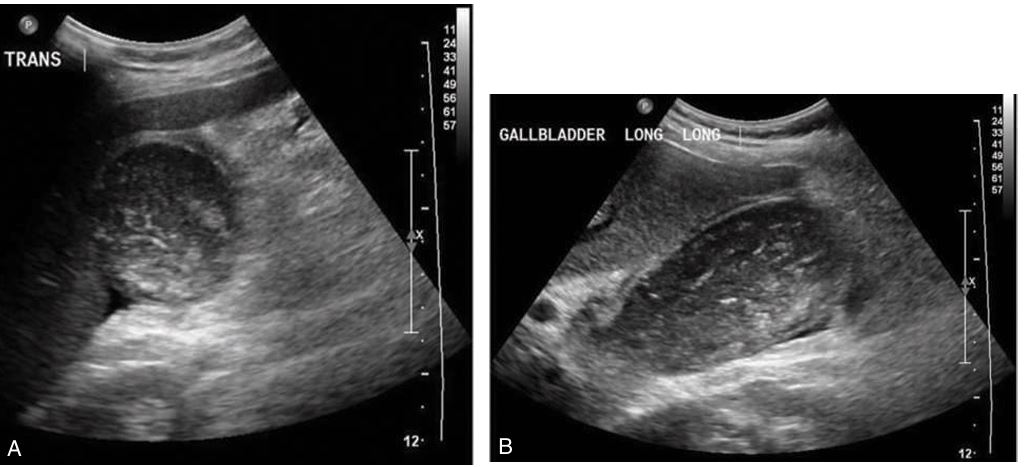
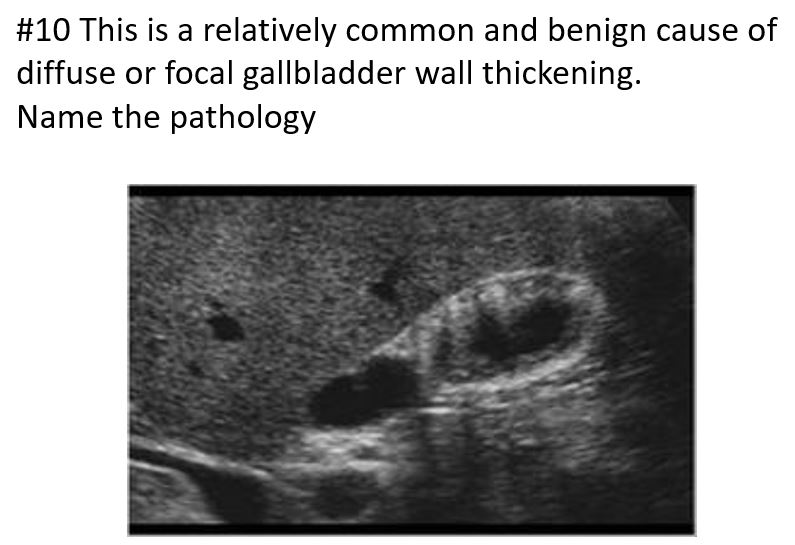
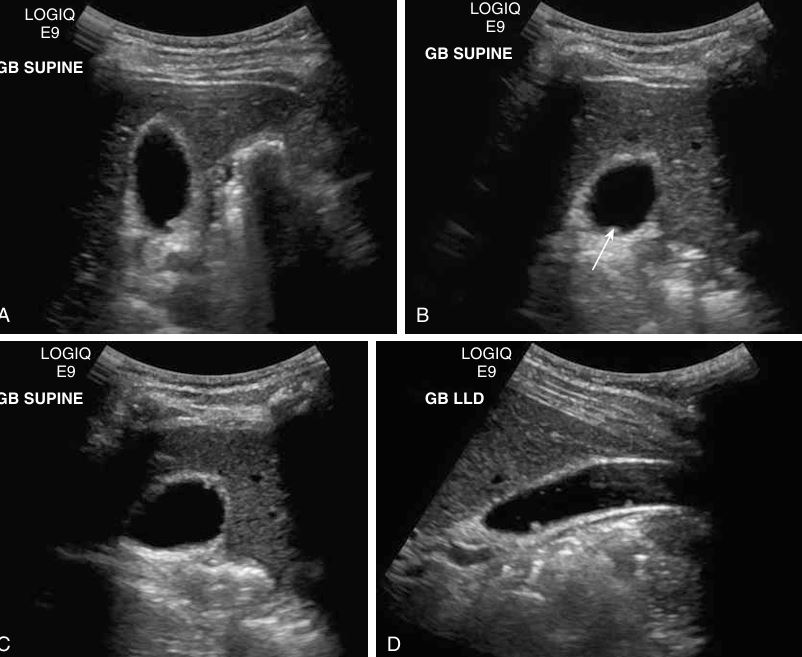
# 1 Pt. c/o RUQ pain, this image looked the same in both supine and LLD positions. Name the pathology
Cholesterolosis showing multiple cholesterol polyps
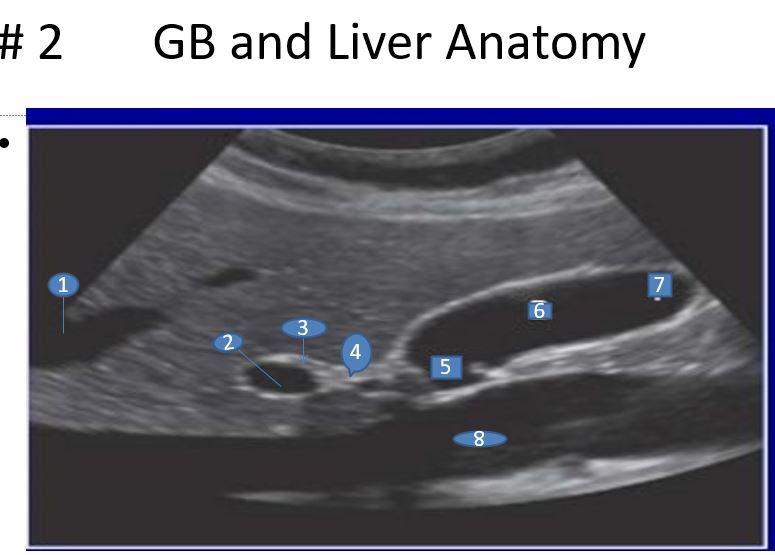
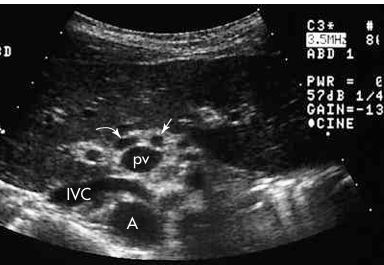
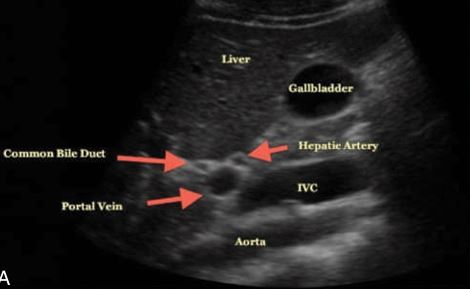
1. Left Hepatic Vein
2. Portal Vein
3. Common Bile Duct
4. Cystic Duct
5. Neck
6. Body
7.Fundus
8. Inferior Vena Cava (IVC)
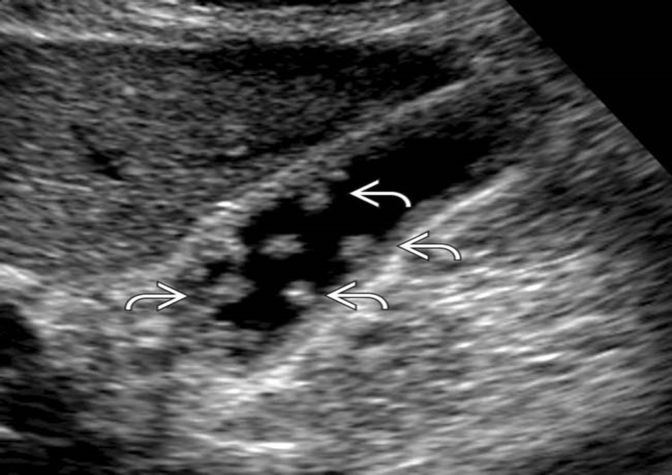
Septations within Gallbladder
HINT: FEVER, positive murphys sign
Acute cholecystitis
Affects more elderly men ; 50% of patients are diabetic
Emphysematous Cholecystitis
all patterns of acute cholecystitis
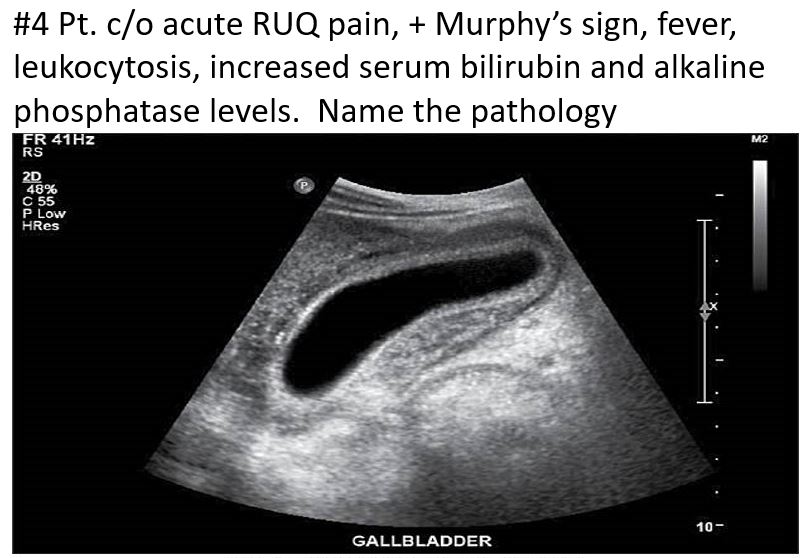
severe right upper quadrant pain, fever, leukocytosis, and elevated bilirubin and alkaline phosphatase
severe and potentially life-threatening complication of acute cholecystitis
result of prolonged infection leading to necrosis of the gallbladder. It is breakdown of the gb wall and the presence of exudates, hemorrhage, and necrotic tissue.
may cause complications like pericholecystic abscesses or peritonitis.
Gallstones or fine gravel occur in 80% to 95% of patients.
This echogenic material has the following three characteristics
Does not cause shadowing
Is not gravity-dependent
Does not show a layering effect
Gangrenous Cholecystitis
Is the acute inflammation of the gallbladder in the absence of cholelithiasis
Is most likely caused by decreased blood flow through the cystic artery
Conditions that produce depressed motility (e.g., trauma, burns, postoperative patients, HIV, etc.) may precede development
Extrinsic compression of the cystic duct by a mass or lymphadenopathy may also cause this condition.
Clinically, the patient has a positive Murphy’s sign.
Acalculous cholecystitis
Single, large gallstone or multiple tiny stones
Often asymptomatic
Other factors include pregnancy, diabetes, oral contraceptives, hemolytic diseases, diet-induced weight loss, and total parenteral nutrition (TPN)
After a fatty meal, the gallbladder contracts to release bile; if the outflow tract is blocked by gallstones, then pain results. RUQ Pain, nausea, and vomiting.
The pain can last up to 6 hours
Patients often fall under the category of the “five Fs”: fat, female, forty, fertile, and fair
LAB WORK:AST/ALT MAY BE NORMAL
Elevated bilirubin
Acute Elevated amylase
Elevated ALP
Abnormal LFTs
Cholelithiasis
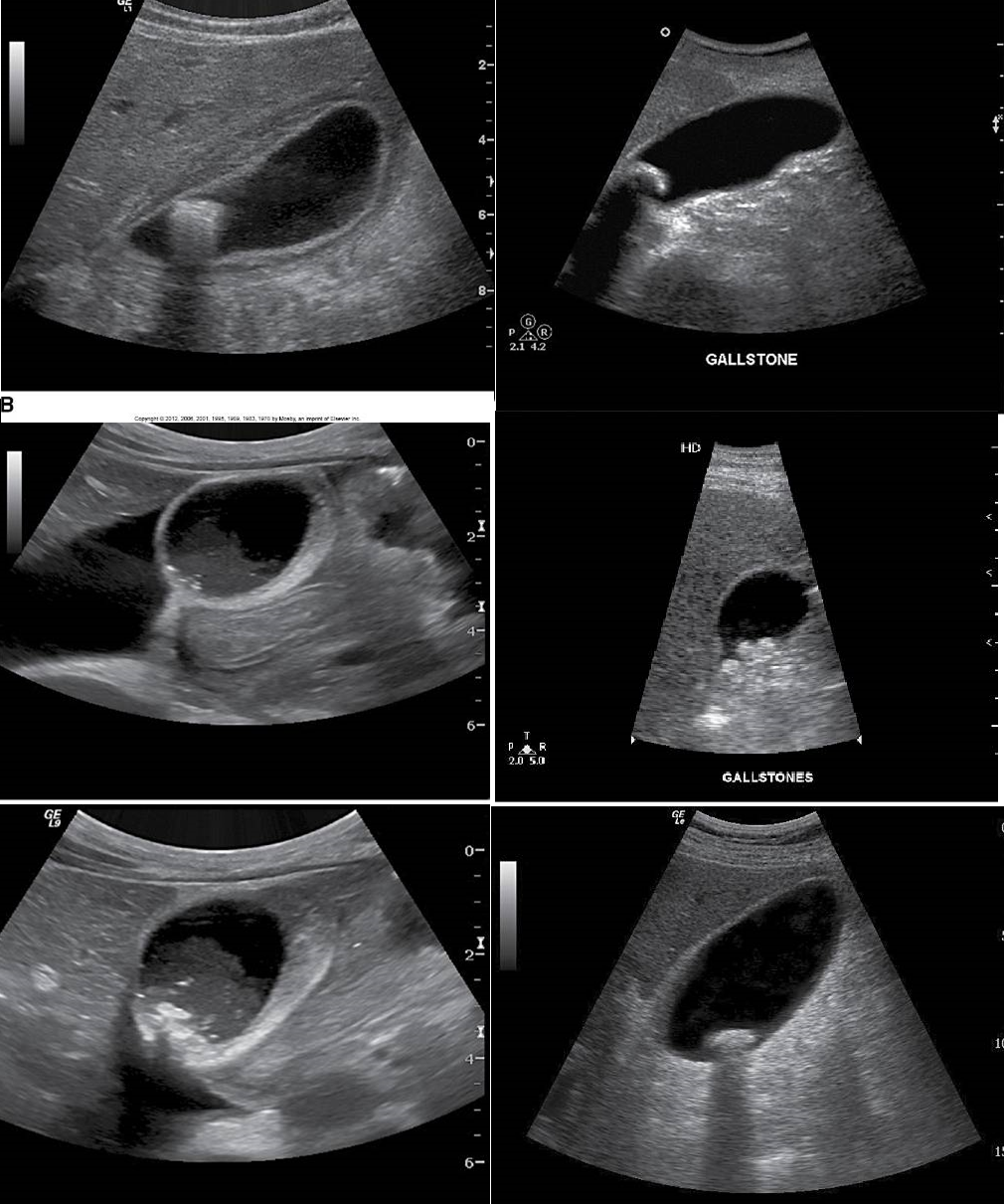
different patterns of cholelithiasis
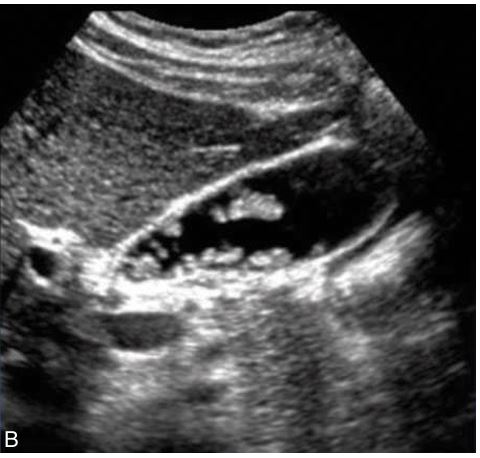
what is this showing
Cholelithiasis w Floating Stones

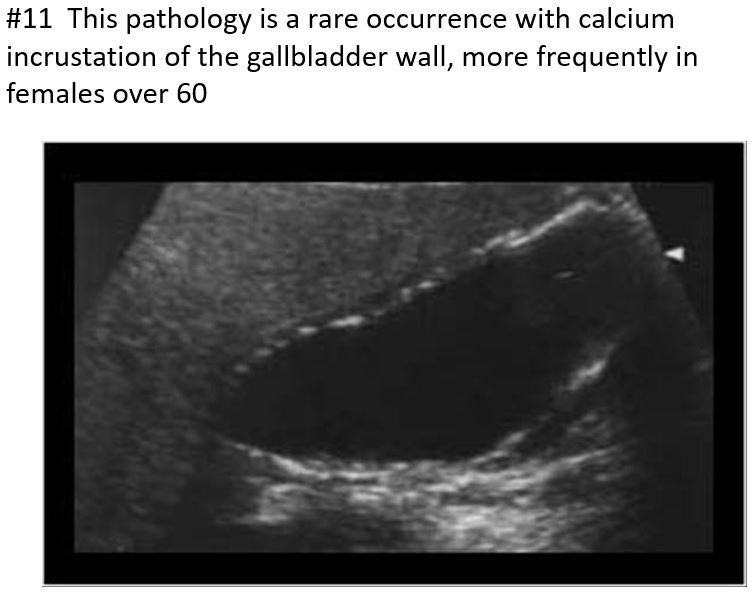
Rare occurrence - calcium incrustation of the gallbladder wall.
often in older female patients over 60
Associated with gallstones, a form of chronic cholecystitis
Significance: 25% of these patients will develop cancer on the gallbladder wall.
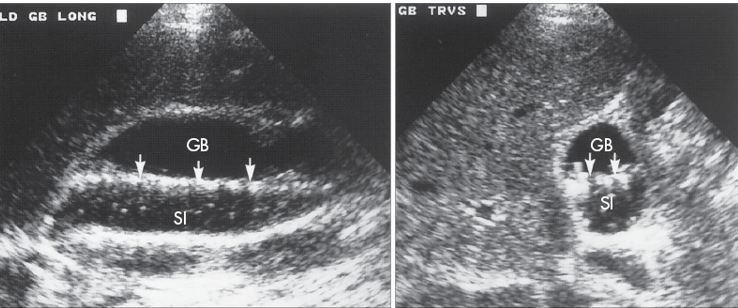
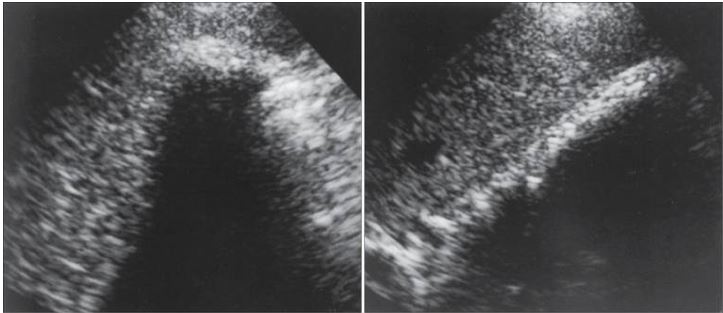
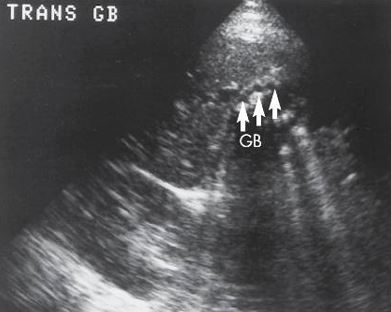
Bright echogenic echo is seen in the region of the gallbladder with posterior shadowing.
The differential will include a packed bag or WES sign.
Porcelain Gallbladder
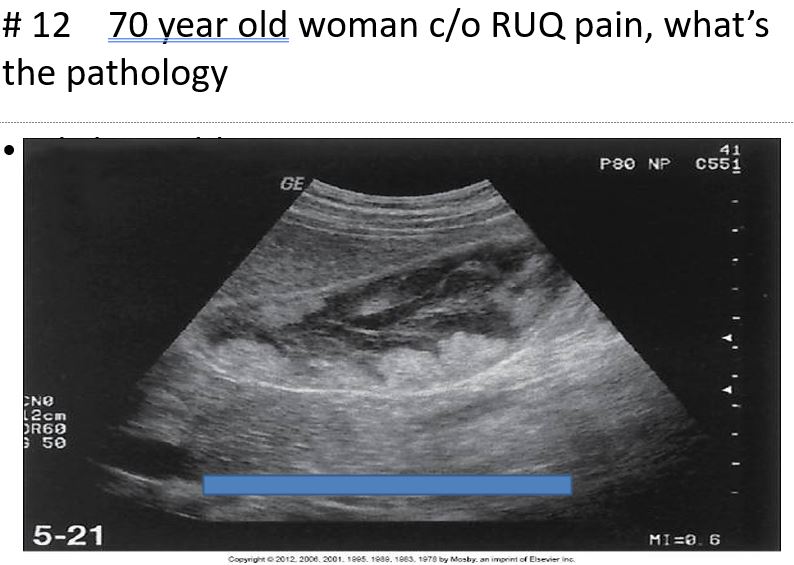
Benign condition that involves a hyperplastic change in the gallbladder wall.
Exaggeration of normal invaginations of the luminal epithelium (called Rokitansky-Aschoff sinuses)
Cholesterol Crystals, Mucosal Hyperplasia, Muscular Thickening, Papillomas
The lesion remains immobile
No Acoustic Shadow
Artifact: comet tail
Adenomyomatosis
what is another name for this ?
packed bag
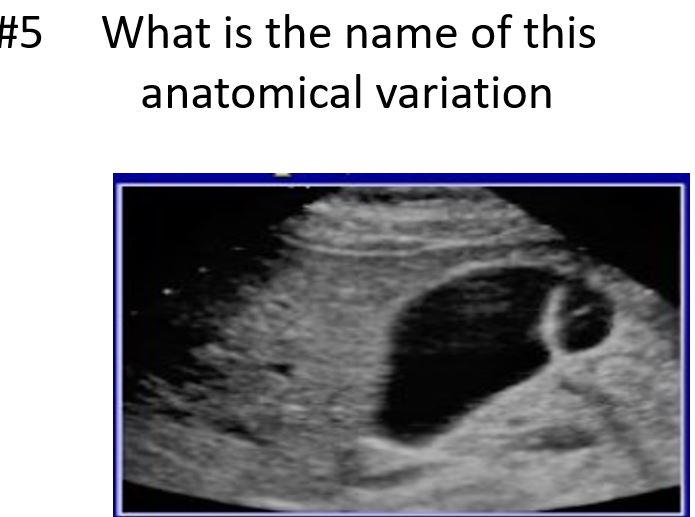
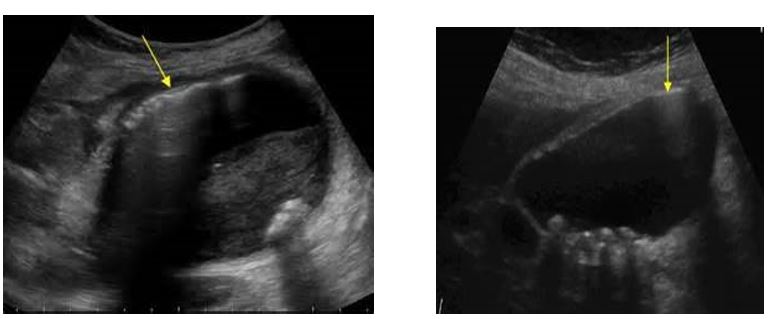
phrygian cap
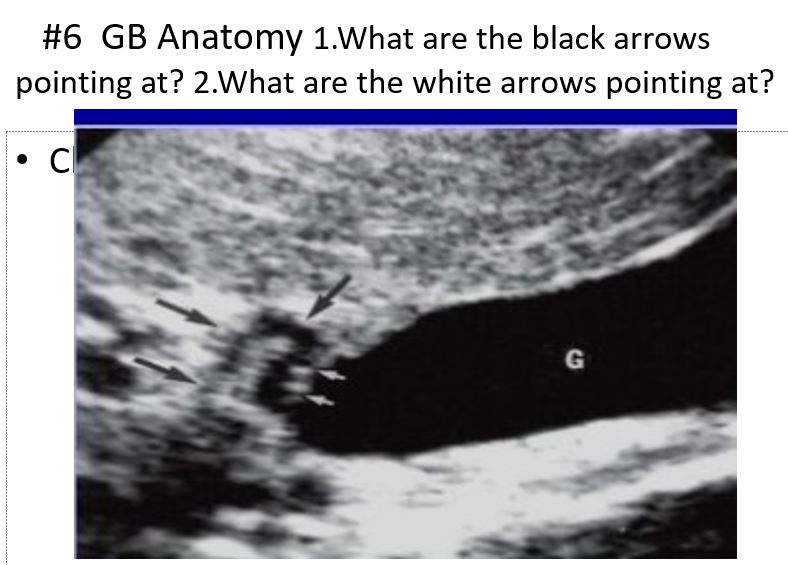
black: cystic duct
white: valves of heister
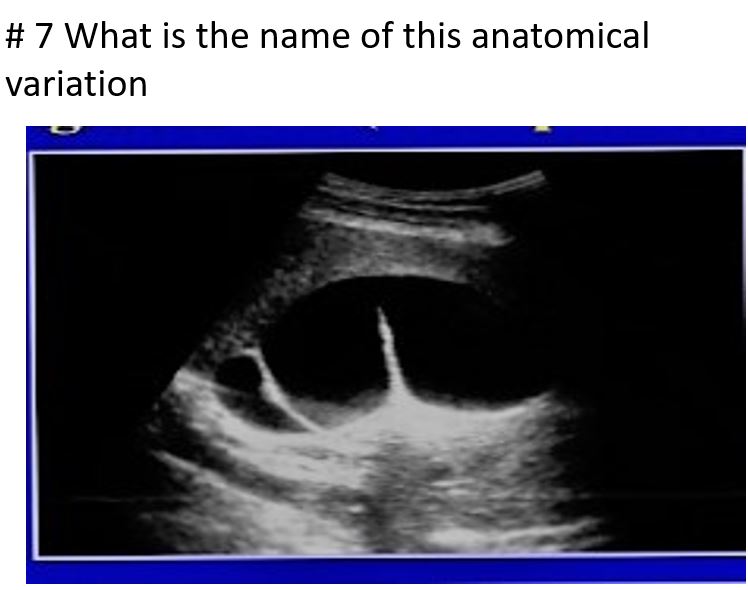
sigmoid gallbladder or junctional folds
HINT: NO FEVER
Cholelithiasis
sludge
Adenomyomatosis
artifact: comet tail
porcelain gallbladder
Adenocarcinoma
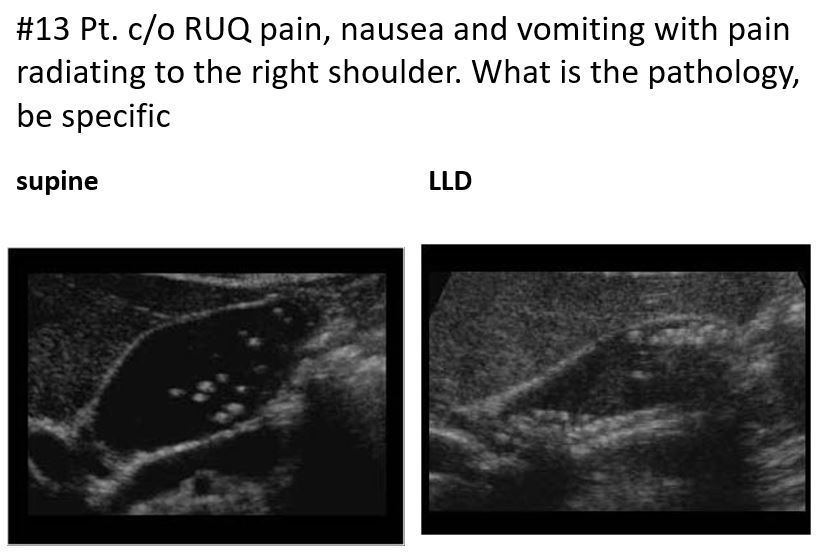
Cholelithiasis showing multiple small floating and
nonfloating gallstones
Choledochal Cyst
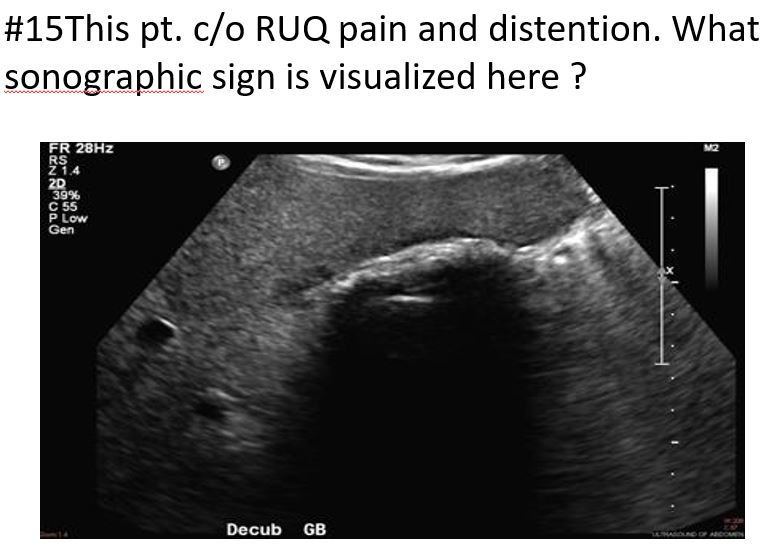
Wall Echo Shadow “WES” Sign
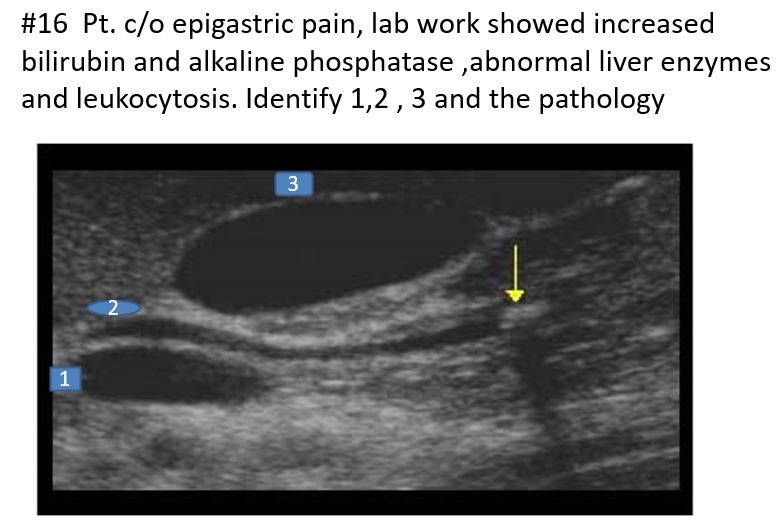
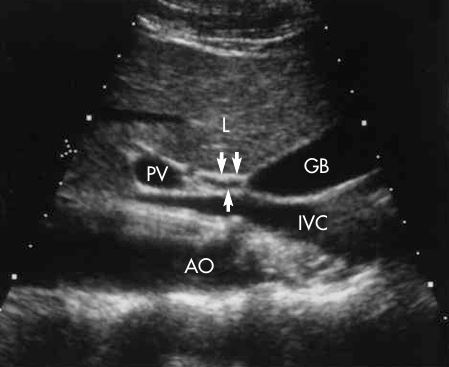
1. Portal Vein
2. Common Bile Duct
3. Gallbladder
Pathology: Choledocholithiasis
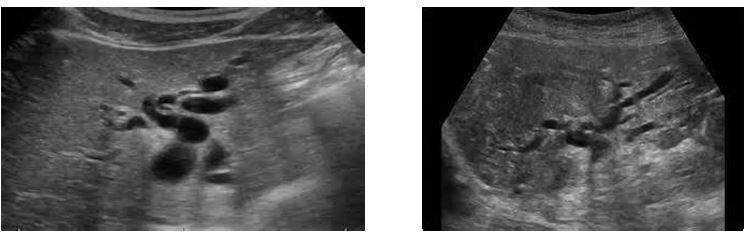
Caroli’s Disease
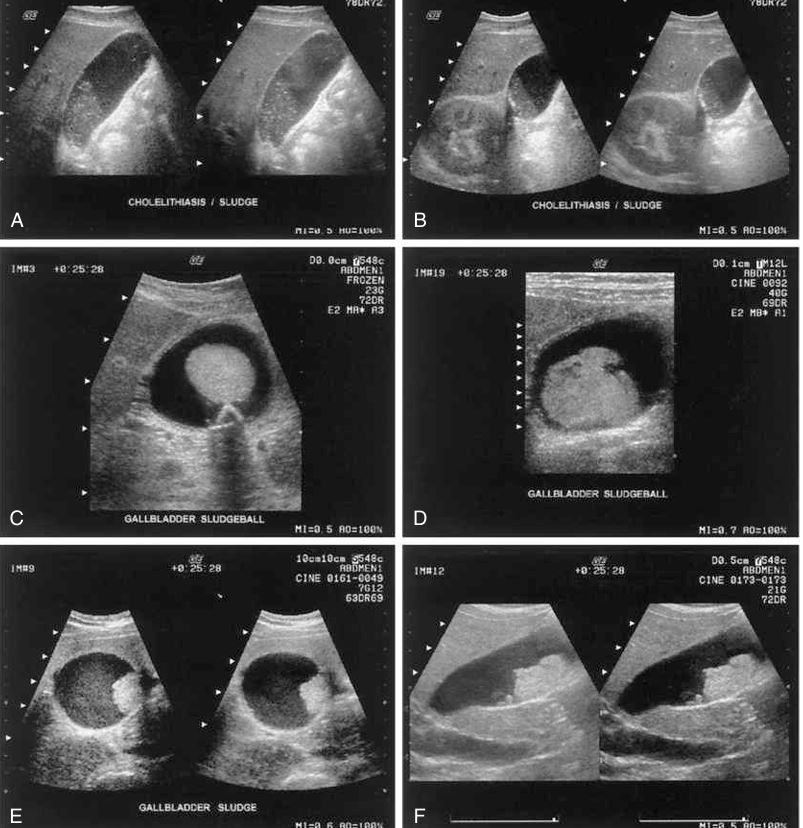
patterns of sludge
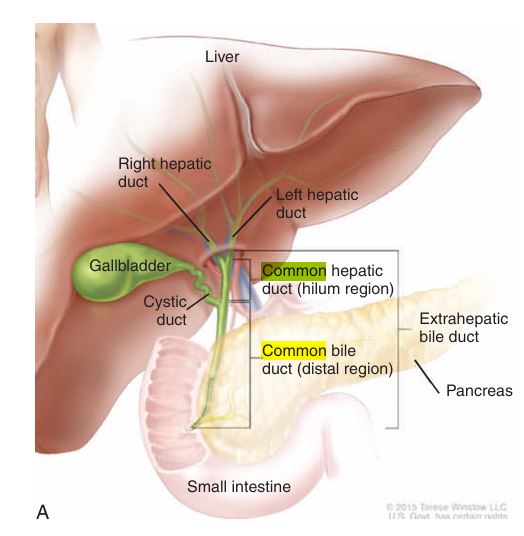
biliary diagram

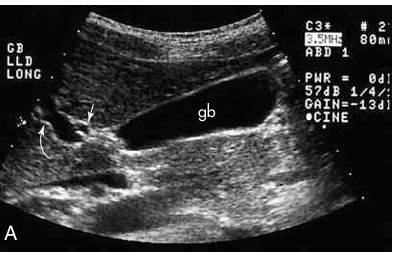
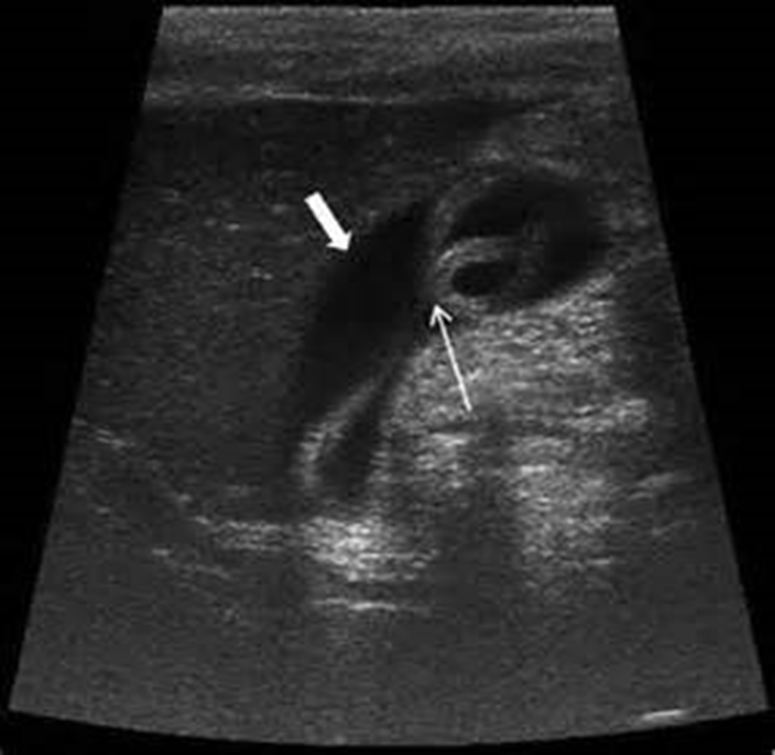
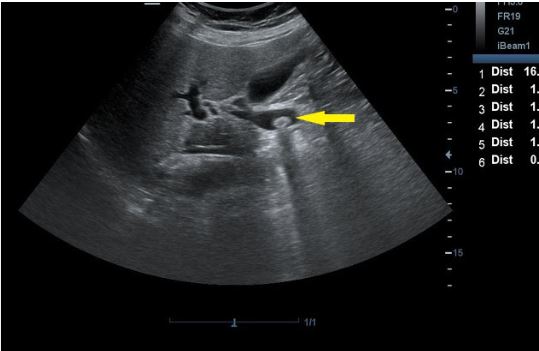
arrow is pointing to?
CBD

hartmann’s pouch

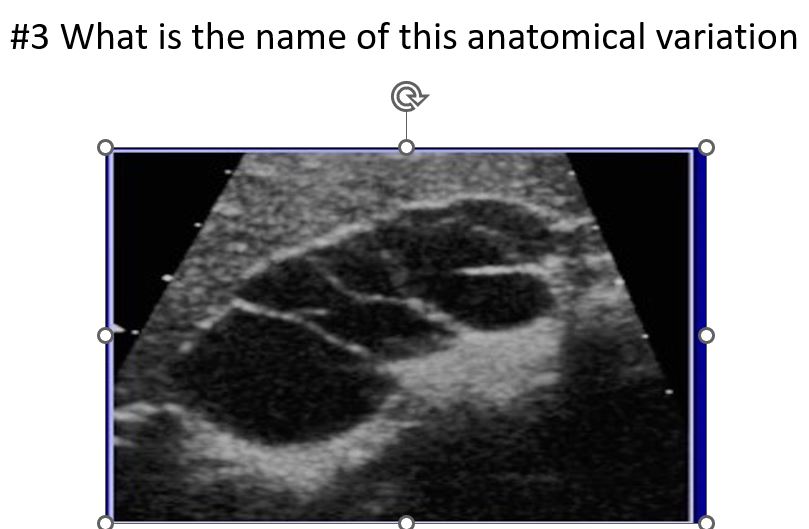
double gallbladder
arrow: MLF
curved arrow: portal vein
arrow: CBD
curved arrow: CBD
arrow: HA
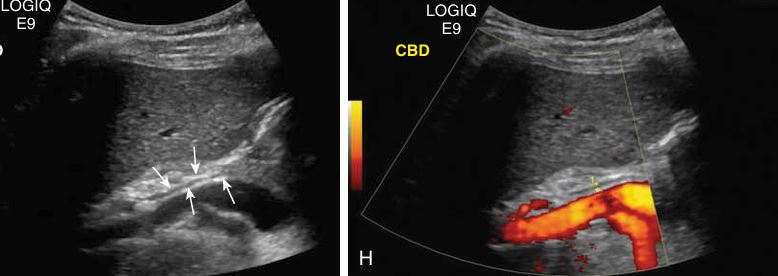
what doesnt catch color
Common Bile Duct doesn’t catch COLOR
Small echogenic Adenoma in GB
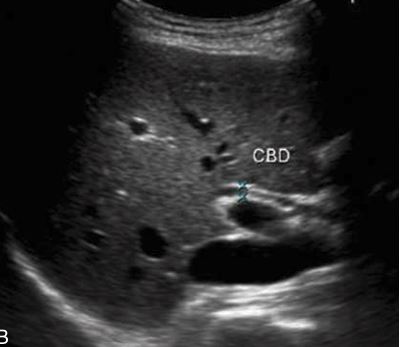
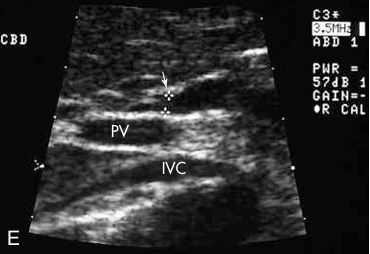
what plane is this and what is it showing
SAG - CBD
what plane is this?
transverse
what are the arrows pointing to?
cystic duct
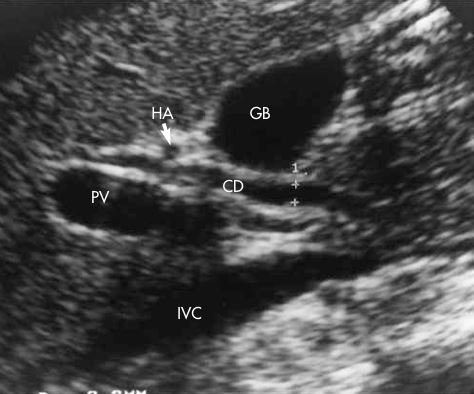
On this sagittal image, the hepatic artery (HA) is shown anterior to the common duct (CD)
the most common cause of this occurs from persistent obstruction of the cystic duct or gallbladder neck by an impacted gallstone.
Acute Cholecystitis
is the most common disease of the gallbladder
Cholelithiasis
is the most common form of gallbladder inflammation.
Chronic cholecystitis
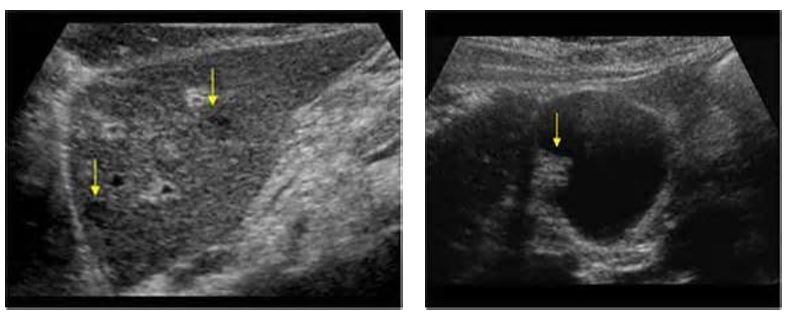
the most common pseudotumor of the gallbladder
Cholesterol polyps
rare and is nearly always a rapidly progressive disease, with a mortality rate approaching 100%.
associated with cholelithiasis in about 80% to 90% of cases
It is twice as common as cancer of the bile ducts and occurs most frequently in women 60 and older
the most common sonographic appearance of the soft tissue mass is a heterogeneous solid or semisolid echo texture.
Gallbladder Carcinoma
two types of Caroli disease: the simple classic form and the more common form associated with
periportal hepatic fibrosis.
The most common cause of biliary ductal system obstruction is the presence of a
tumor or thrombus within the ductal system
Most common cause is the presence of a tumor or thrombus within the ductal system.
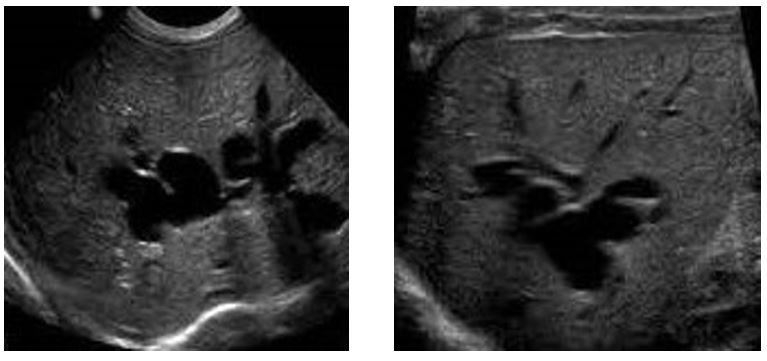
Process may be found in the extrahepatic or intrahepatic ductal pathway.
Obstruction of biliary ductal system is diagnosed by ultrasound when the sonographer finds the presence of ductal dilation.
This finding is called “too many tubes” or “shotgun” sign when intrahepatic ducts are dilated.
Biliary Obstruction
the most common cause for this obstruction is malignancy or adenopathy at this level.
Suprapancreatic Obstruction
Intrahepatic duct stones are less common than
common bile duct stones.
This incidence is uncommon, and the frequency increases with age. The most common risk factor in the Western world is primary sclerosing cholangitis.
Cholangiocarcinoma:
Most cholangiocarcinomas are adenocarcinomas, followed by squamous carcinomas.
The tumors are further divided into subtypes: sclerosing, nodular, and papillary. Nodular sclerosing tumors are the most common.
second most common primary malignancy of the liver.
An increased incidence of this tumor has risen over the past two decades, secondary to an increasing number of patients with liver cirrhosis and hepatitis C infection.
Intrahepatic Cholangiocarcinoma.
the most common tumor sites that can spread to the biliary system are from the
breast, colon, or melanoma.
The most common primary malignancy of the gallbladder is
Adenocarcinoma

Distension (hydrops) of the gallbladder but showing what?
sludge with hydrops
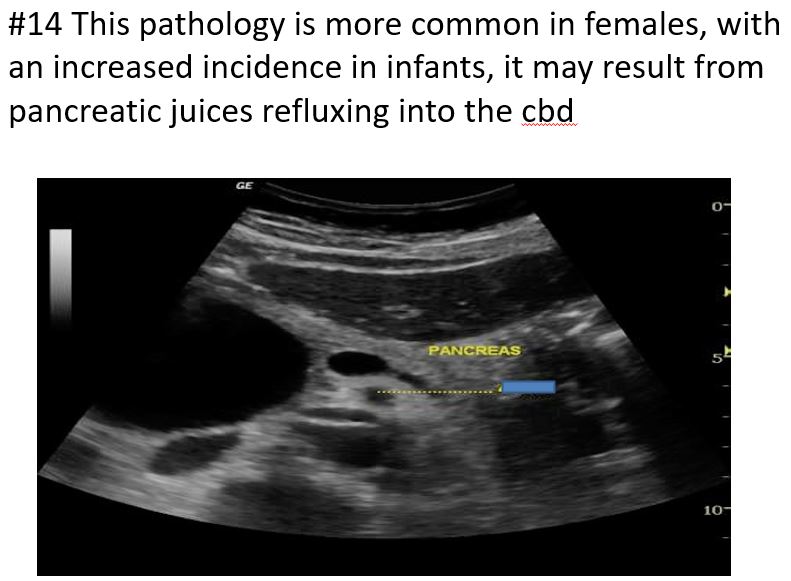
Rare, primarily congenital
More common in women than in men (4:1)
Higher incidence in infants than adults
linked with gallstones, pancreatitis, or cirrhosis, cholangitis
SymptomsAbdominal mass
Pain
Fever
Jaundice
increased BILIRUBIN
Diagnosis may be confirmed with a nuclear medicine hepatobiliary scan
Type I is a fusiform dilation of the common bile duct is Most common, along with type Iva
Choledochal Cysts
rare and primarily limited to cystadenoma and cystadenocarcinoma.
frequently in middle-aged women whose clinical presentation includes abdominal pain or mass or jaundice or both (if the mass is near the porta hepatis).
Sonographic:
Cystic mass with multiple septa and papillary excrescences
Mass may show variations in this pattern and appear as unilocular, calcified, or multiple.
Lesion may be associated with dilation of the intrahepatic ducts.
Differential: hemorrhagic cyst or infection, echinococcal cyst, abscess, or cystic metastasis.
Intrahepatic Biliary Neoplasms
A very rare condition found more often in older women
gallbladder twists along its long axis
mobile gallbladder with a long suspensory mesentery
symptoms resembling acute cholecystitis, such as severe right upper quadrant pain, fever, and nausea.
Sonographic:
Gallbladder massively inflamed and distended
Cystic artery and cystic duct may become twisted
if twisted more than 180 degrees, then a risk of gangrene exists. Surgical intervention is the treatment.
Torsion of the Gallbladder
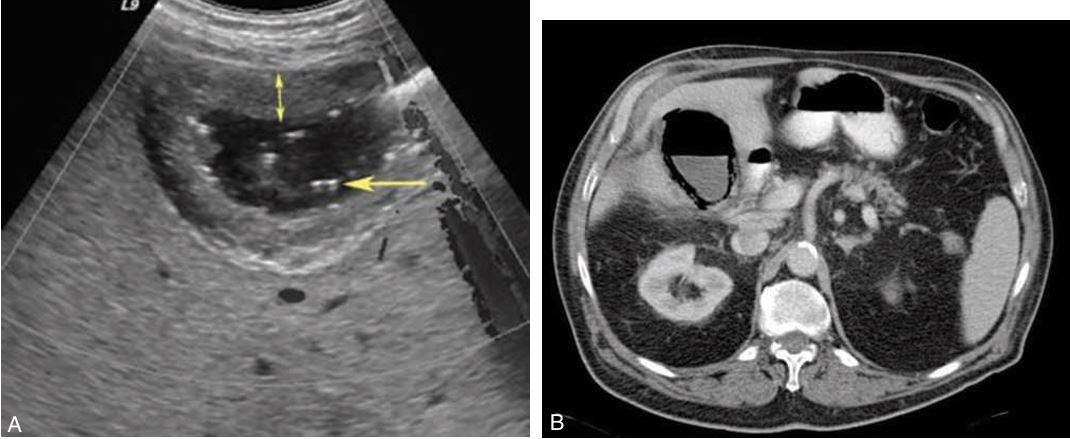
Rare complication of acute cholecystitis
Affects more elderly men ; 50% of patients are diabetic
gas-forming bacteria in the gallbladder wall and lumen with extension into the biliary ducts
bright echo with comet-tail artifact or the WES sign
gallstones may not be present in 30% to 50% of patients
higher risk of perforation, its a surgical emergency.
fatal in 15% of patients
Emphysematous cholecystitis (showing ct scan too)
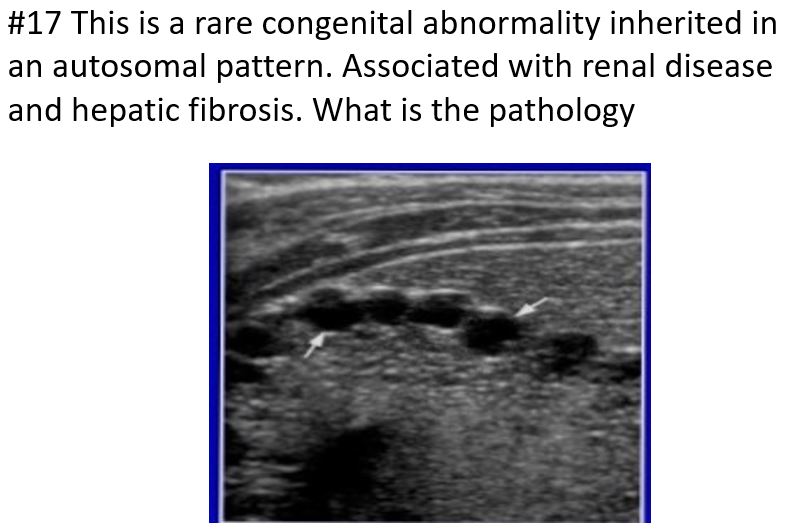
Rare congenital abnormality most likely inherited in an autosomal recessive fashion.
Communicating cavernous ectasia of the intrahepatic ducts characterized by congenital segmental saccular cystic dilation of major intrahepatic bile ducts.
Found in the young adult or pediatric population;
may be associated with renal disease or congenital hepatic fibrosis
symptoms
Recurrent cramplike upper abdominal pain, secondary to biliary stasis, ductal stones, cholangitis, and hepatic fibrosis.
Two types of Caroli’s disease
Simple classic form
More common form associated with periportal hepatic fibrosis
Caroli’s Disease (medullary sponge kidney) is strongly associated
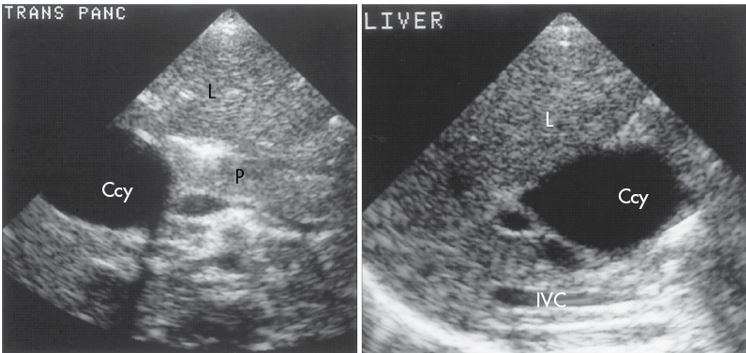
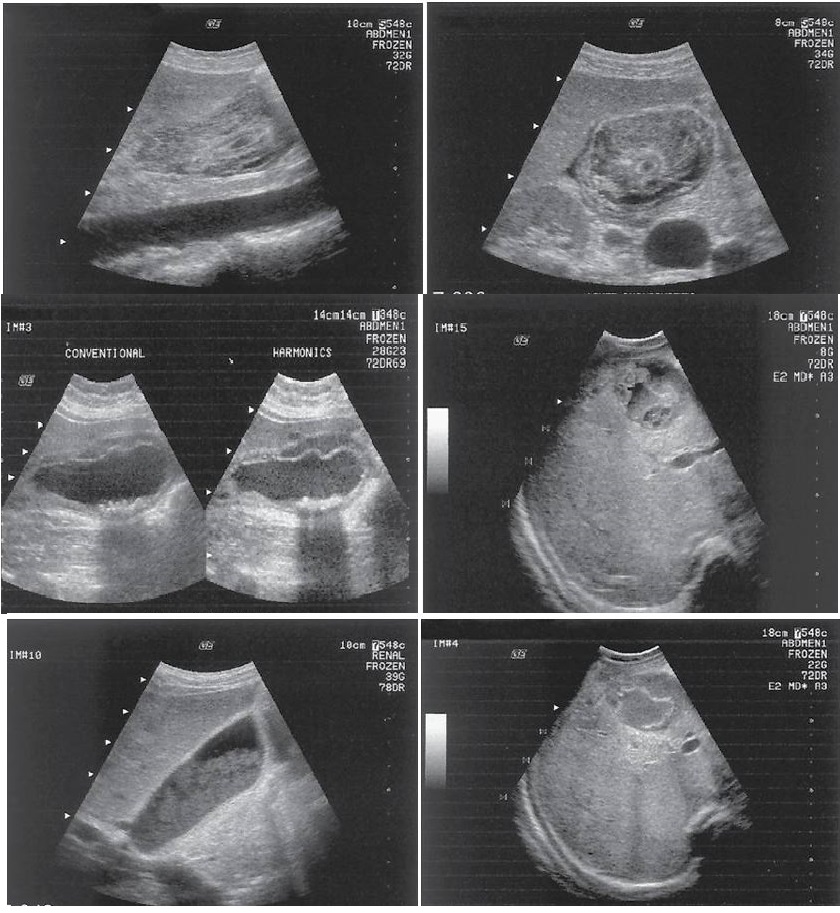
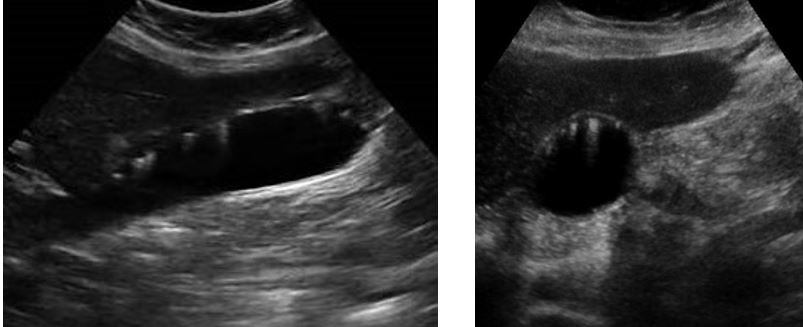
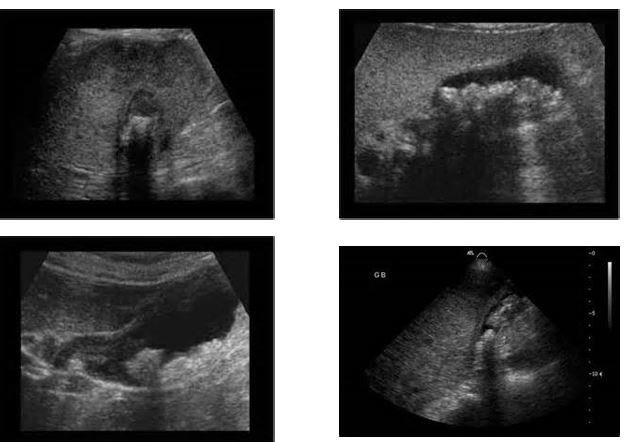
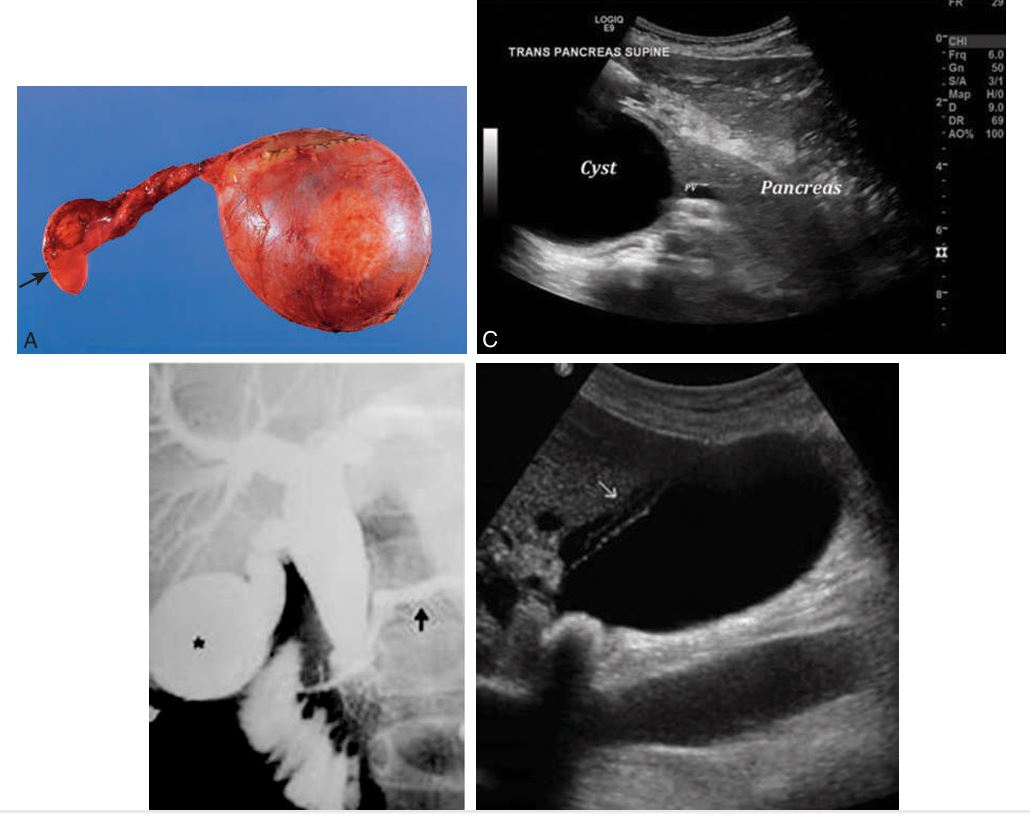
Transverse and longitudinal scan of a young patient with a choledochal cyst (Ccy) in the right upper quadrant.
Localized cystic dilation of the common bile duct
Diverticulum from the common bile duct
Invagination of the common bile duct into the duodenum
Dilation of the entire common bile duct and the common hepatic duct
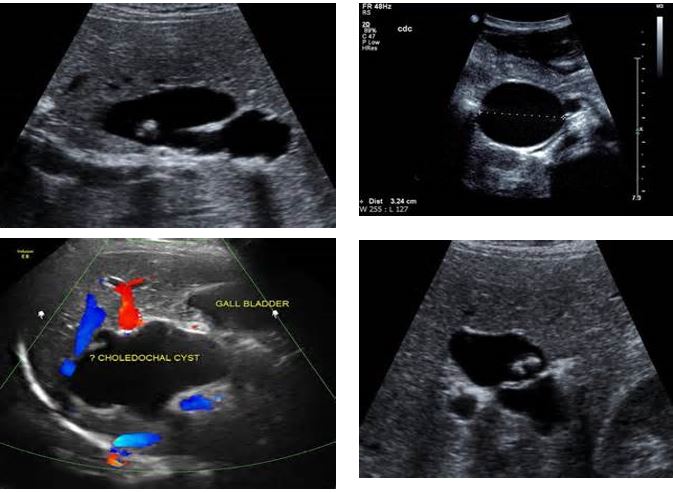
4 pics of Choledochal Cysts
what is this disease associated with…this is carolis disease
MEDULLARY SPONGE KIDNEY
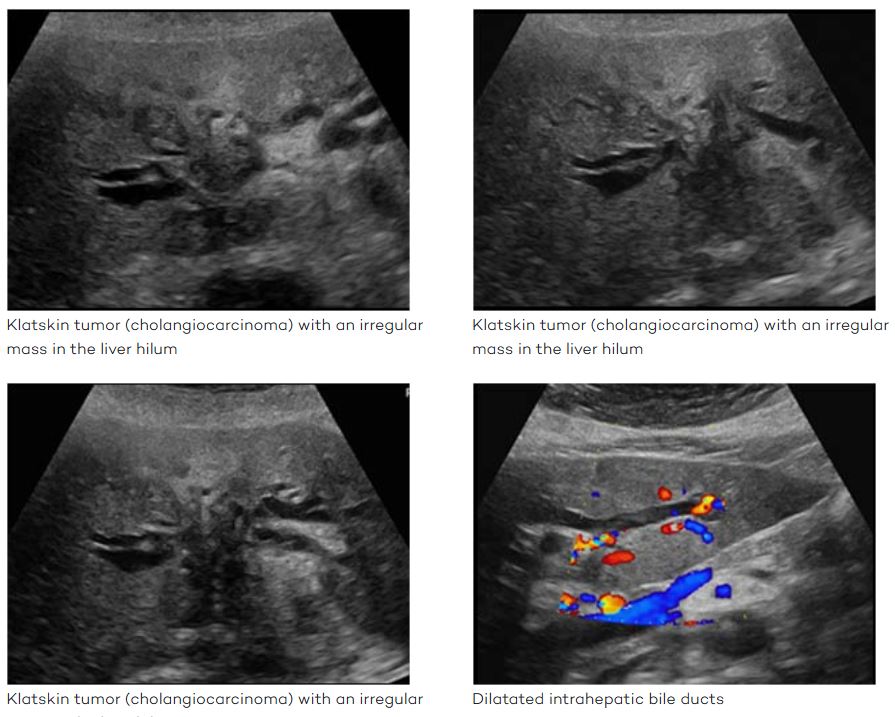
another name for hilar cholangiocarcinoma
Klatskin tumor

is uncommon cause for extrahepatic biliary obstruction as a result of an impacted stone in the cystic duct, which creates extrinsic mechanical compression of the common hepatic duct.
Patient presents with painful jaundice.
Mirizzi Syndrome
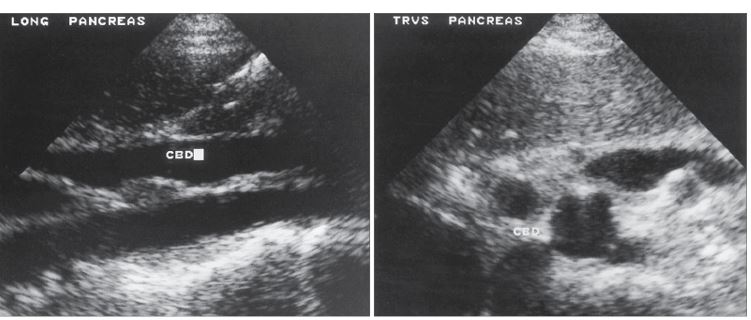
Carcinoma of the head of the pancreas with obstruction of the common bile duct (CBD) is demonstrated
Dilated intrahepatic ducts secondary to a mass in the area of the porta hepatis.
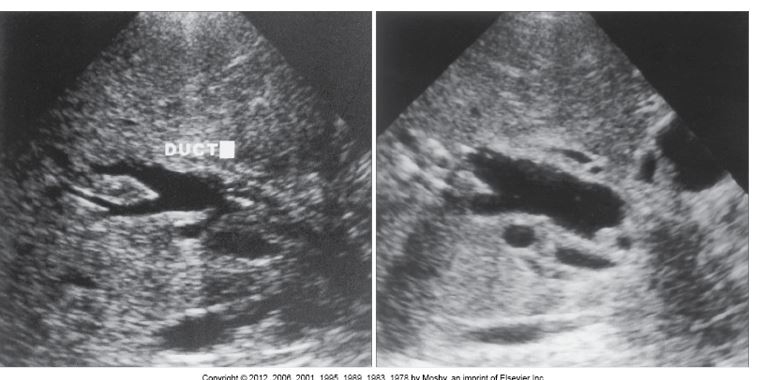
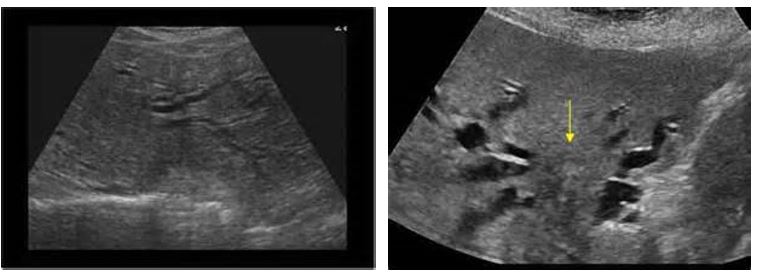
Stones within the common bile duct (CBD)
Primary choledocholithiasis occurs when calcium stones form de novo. This can result from conditions that cause bile duct strictures or dilation, leading to bile stasis. Examples of diseases linked to primary choledocholithiasis include:
Sclerosing cholangitis
Caroli disease
Parasitic infections
Chronic hemolytic diseases
Prior biliary surgery
Secondary choledocholithiasis involves stones migrating from the gallbladder into the common bile duct. This form is typically associated with calculous cholecystitis (gallbladder inflammation due to stones).
Symptoms
Increased direct bilirubin
Leukocytosis
Increased alkaline phosphatase
Abnormal liver enzymes
Choledocholithiasis
May be identified as Oriental sclerosing cholangitis.
Other forms include AIDS cholangitis and acute obstructive suppurative cholangitis.
Patients have malaise and fever, followed by sweating and shivering, right upper quadrant pain, and jaundice.
In severe cases, patient is lethargic, prostrate, and in shock.
Laboratory values show leukocytosis and an elevation of serum alkaline phosphatase and bilirubin.
Cholangitis

Disease is caused by the parasitic roundworm, Ascaris lumbricoides, which uses a fecal-oral route of transmission.
The worms may be 20 to 30 cm long and 6 cm in diameter.
The worms grow in the small bowel before entering the biliary tree through the ampulla of Vater.
Cause acute biliary obstruction
may be symptomatic or have biliary colic, pancreatitis, or biliary symptoms.
Ascariasis
the second most common primary malignancy of the liver
Incidence of this tumor has risen, secondary to increasing number of patients with liver cirrhosis and hepatitis C infection.
These tumors are often unresectable with a poor prognosis.
Intrahepatic Cholangiocarcinoma
specific type of cholangiocarcinoma
jaundice, pruritus, and elevated cholestatic liver parameters.
Begins in the right or left bile duct and then extends into the proximal duct and distally into the common hepatic duct and contralateral bile ducts.
Tumor may extend outside of the ducts to involve the adjacent portal vein and arteries.
Chronic obstruction leads to atrophy of the involved lobe.
Majority of patients die within 1 year of diagnosis
isolated intrahepatic duct dilation.
Hilar Cholangiocarcinoma

Is difficult to distinguish from hilar cholangiocarcinoma; progressive jaundice is seen in the majority of patients.
Tumor mass may be sclerosing or polypoid.
Tumor spread in the superior ductal system and extrahepatic area should be carefully evaluated.
May extend into the adjacent lymph nodes.
Sonographic findings
Sclerosing tumor is nodular with focal irregular ductal constriction and wall thickening.
Has a hypoechoic and hypovascular appearance with poorly defined margins
Distal Cholangiocarcinoma
Metastases to the Biliary Tree
Result from pancreatic juices refluxing into the bile duct because of an connection of the pancreatic duct into the distal common bile duct, causing duct wall abnormality, weakness, and outpouching of the ductal walls
Choledochal Cysts
Benign neoplasms that have a lower premalignant potential compared to colonic adenomas.
typically solitary lesions
to be pedunculated, meaning they are attached by a stalk
Smaller adenomas are generally homogeneously hyperechoic
Larger adenomas tend to become more heterogeneous
Adenoma of GB
what is this showing?
Choledocholithiasis

what are these pics showing?
Cholesterol polyps
What is the most common benign tumor of the gallbladder?
Cholesterol polyps