Treatment of Parkinson's disease
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
Signs of Parkinsonism
Tremor at rest
Rigidity
Akinesia or bradykinesia
Postural instability/disturbances
What does the Nigrostriatal pathway do?
Connects substantia nigra to dorsal striatum of basal ganglia
Associated with movement control:
Excites the direct pathway via stimulation of D1 receptors
Inhibits the indirect pathway via stimulation of D2 receptors
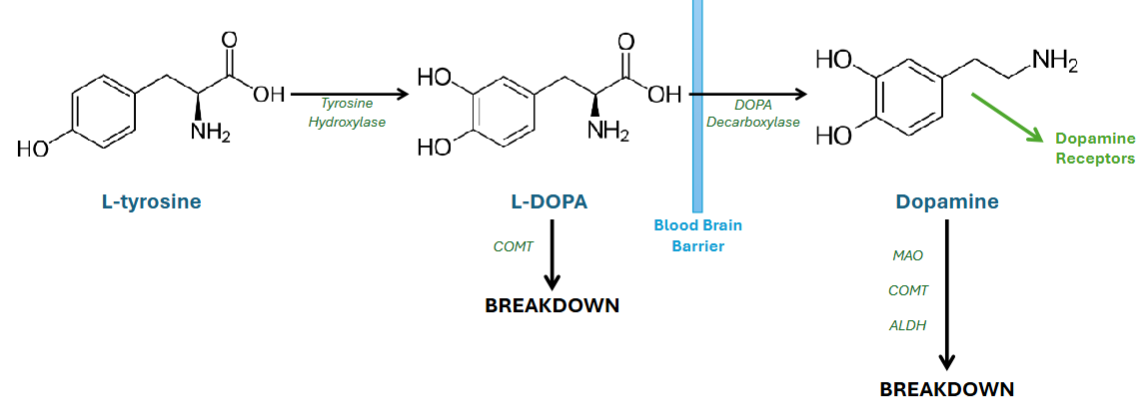
Explain dopamine synthesis
L-tyrosine (first precursor) is converted to L-DOPA via tyrosine hydroxylase
L-DOPA crosses the blood brain barrier (BBB)
L-DOPA is then converted to dopamine via DOPA decarboxylase
Dopamine is packaged and stored in synaptic vesicles by vesicular monoamine transporter (VMAT) and when released binds to post-synaptic dopamine receptors
Dopamine is broken down into inactive metabolites by:
Monoamine oxidase (MAO) →MAO-A and MAO-B
Catechol-O-methyl transferase (COMT) (also involved in peripheral degradation of L-DOPA)
Aldehyde dehydrogenase (ALDH)
** enzymes
What type of neurotransmitter is dopamine?
Catecholamines
** same as adrenaline and noradrenaline
How do D1-like and D2-like receptors work?
D1-like receptors:
Comprising D1 and D5 subtypes
Increase intracellular levels of cAMP by activating adenylate cyclase
D2-like receptors:
Comprising D2, D3, and D4 subtypes
Decrease intracellular levels of cAMP by inhibiting adenylate cyclase
General Pharmacological Management Advice for anti-Parkinsonian medication
Anti-Parkinsonian medications are ‘critical medications’ and are time- sensitive
Patients who miss doses or receive late doses could experience akinesia (freezing)
Suddenly stopping PD medications may also precipitate neuroleptic malignant syndrome, which can be life-threatening
First-line management of Parkinsonian motor symptoms
Levodopa (if motor symptoms affect quality of life)
Dopamine (receptor) agonists (if motor symptoms DON’T affect quality of life)
MAO-B inhibitors (if motor symptoms DON’T affect quality of life)
Adjuvant treatments of motor symptoms:
COMT inhibitors
Amantadine
How does levodopa work?
Similar to the precursor L-DOPA → increase L-DOPA
Levodopa can cross the BBB, allowing for central conversion to dopamine in the CNS
Absorption: well absorbed in small intestine, specifically duodenum
** effectivness dcreaeses with time
What else do you need to prescribe with Levodopa and why?
only 1% of administered levodopa will cross the BBB → so will also have peripheral conversion → causes side effects (i.e. nausea, hypotension)
To counteract this it is given with a dopa decarboxylase inhibitor: Carbidopa / Benserazide
→ Allows for more availability of levodopa in CNS and so lower doses can be used
→ Also reduces peripheral side effects
Adverse effects of levodopa
‘On-Off Phenomenon’ (Rapid Fluctuations in Clinical State):
May have sudden worsening of bradykinesia and rigidity → can last from few minutes to a few hours, then improve again
** Likely related to fluctuating plasma concentration of levodopa
May get hyperkinetic movements: chorea, dystonia, and athetosis (when levodopa levels are high)
Psychiatric Disturbances: Manifests as schizophrenia-like syndrome with delusions and hallucinations + may also have confusion, disorientation, insomnia or nightmares
Peripheral Side Effects: nausea, vomiting and orthostatic hypotension
How do Dopamine Agonists work?
Stimulates postsynaptic D2 dopamine receptors in the corpus striatum, allowing for normal control of movement via the basal ganglia
Bypasses the need for dopamine
Absorption: absorbed in GI tract, metabolised by liver
** Less motor complications but also less effective than levodopa
What are the 2 Types of Dopamine Agonist and which ones are preferred and why?
Preferred: Non-ergoline Derivatives eg. Bromocriptine, Pergolide, Lisuride, Cabergoline
→ Higher affinity and selectivity for D2-like receptors, little/no interaction with other neurotransmitter receptors
NOT preferred: Ergoline Derivatives eg. Pramipexole, Ropinirole, Rotigotine, Apomorphine
→ less selective
→ more adverse effects: Nausea and vomiting, hallucinations, somnolence + serious risk of developing cardiovalvular, pleuropulmonary, and retroperitoneal fibrosis
Adverse effects of Non-ergoline Derivatives of Dopamine Agonists
Somnolence
Hallucinations
Compulsive behaviours/impulse control disorders: compulsive gambling, compulsive shopping, hypersexuality, and binge eating
→ associated with both dosage and duration of treatment with dopamine agonists
How do MAO-B Inhibitors work?
Inhibits the activity of MAO-B → allows for longer/ more availability of dopamine within the CNS
Absorption: metabolised by liver
** less effective than levodopa
Name some MAO-B Inhibitors
Irreversible MAO-B inhibitors:
Selegiline
Rasagiline
Reversible MAO-B inhibitors:
Safinamide
Adverse effects of MAO-B Inhibitors
Tyramine effect:
An interaction with tyramine, amino acid found in certain foods, can cause rapid and severe increase in blood pressure known as a hypertensive crisis
→ now they are more selective so not as prevelant but longer use increases the chance
Tyramine-rich foods:
Aged cheeses
Cured or smoked meats
Pickled foods
Some fermented products like sauerkraut and soy sauce
Other symptoms:
Nausea
Light headedness
Confusion or hallucinations
How do COMT Inhibitors work?
** Adjuvant treatment for those who have developed dyskinesia or motor fluctuations despite optimal levodopa therapy → used in combination with levodopa
It reversibly inhibits COMT enzyme with the aim of slowing the peripheral breakdown of levodopa → increases the amount available for conversion to dopamine in the brain and reducing the fluctuations in plasma level
Name the 2 types of COMT Inhibitors and what they do
Peripherally Selective COMT Inhibitors:
Do not cross BBB so do not inhibit COMT in the brain
Entacapone or Opicapone
Partially Peripherally Selective COMT Inhibitors:
Cross BBB but exact clinical relevance of inhibiting central COMT in PD is uncertain → most effect is from peripheral inhibition of COMT
Tolcapone
Adverse effects of COMT Inhibitors
May exaggerate some levodopa-related side effects, especially dyskinesia
Confusion
Hallucinations
Discoloration of urine
Diarrhoea
How does Amantadine work?
Adjuvant treatment if dyskinesia remains poorly controlled by other therapies → used in combination with levodopa
Mechanism: poorly understood
Adverse effects of Amantadine
Drowsiness
Light headedness / dizziness
Confusion
Dry mouth
Constipation
Hallucinations (rare)
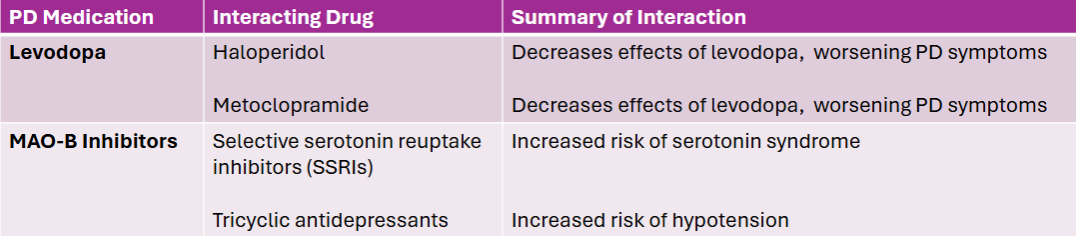
Explain some drug interactions with Levodopa and MAO-B inhibitors
** can also interact with eachother: MAO-B inhibitors which can worsen dyskinesias caused by levodopa