5- muscular treatment
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
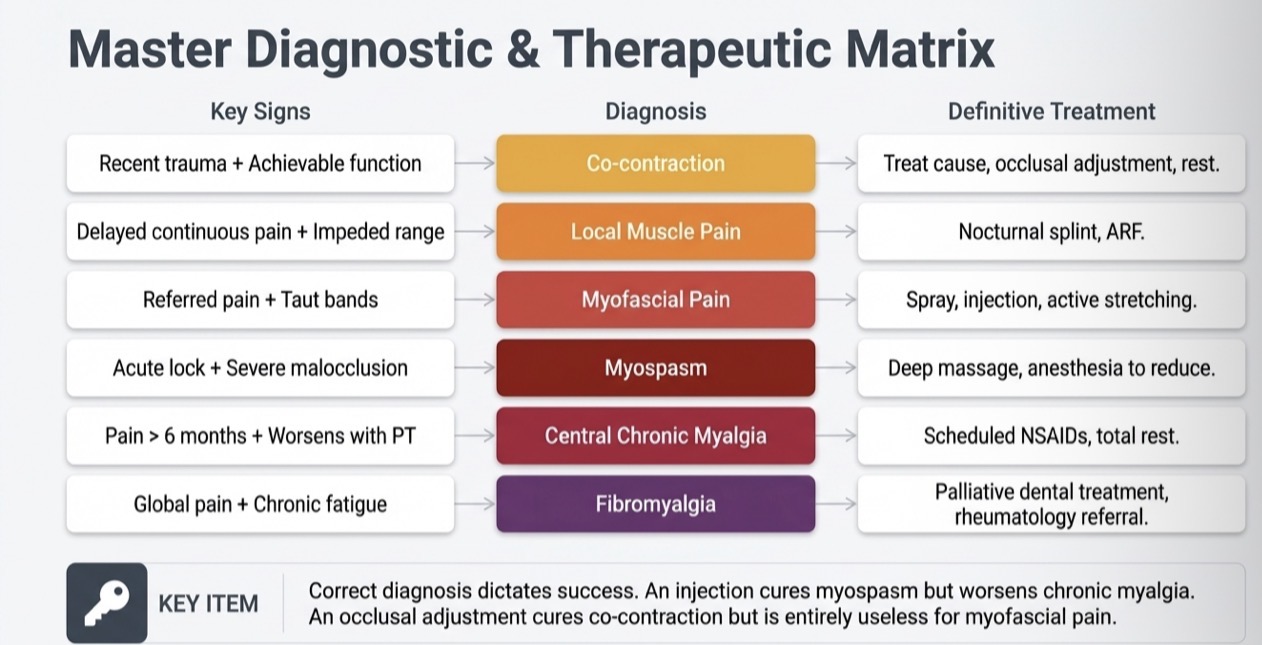
What is the most common and predominant symptom of TMD
Myalgia
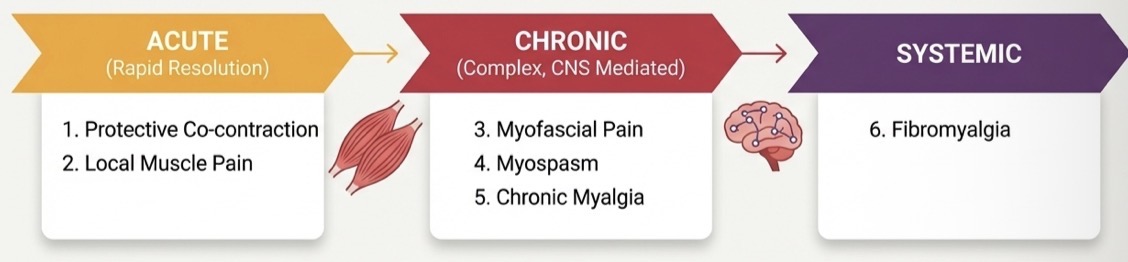
How are muscle disorders classified?
Acute, chronic, systemic
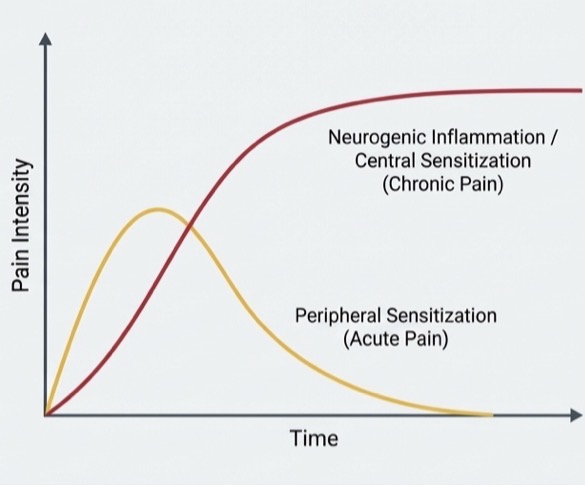
CNS determined how chronic
If acute not resolved quickly CNS- transforms it into chronic- harder to treat
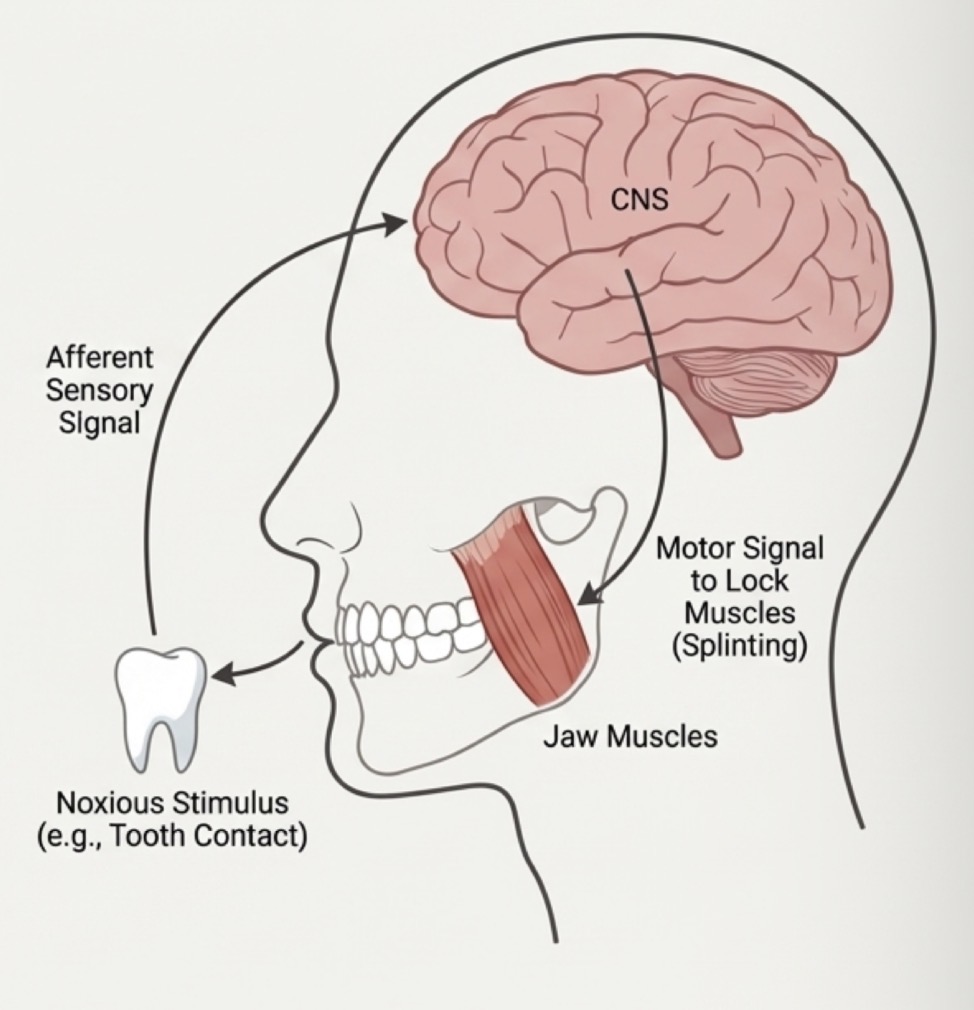
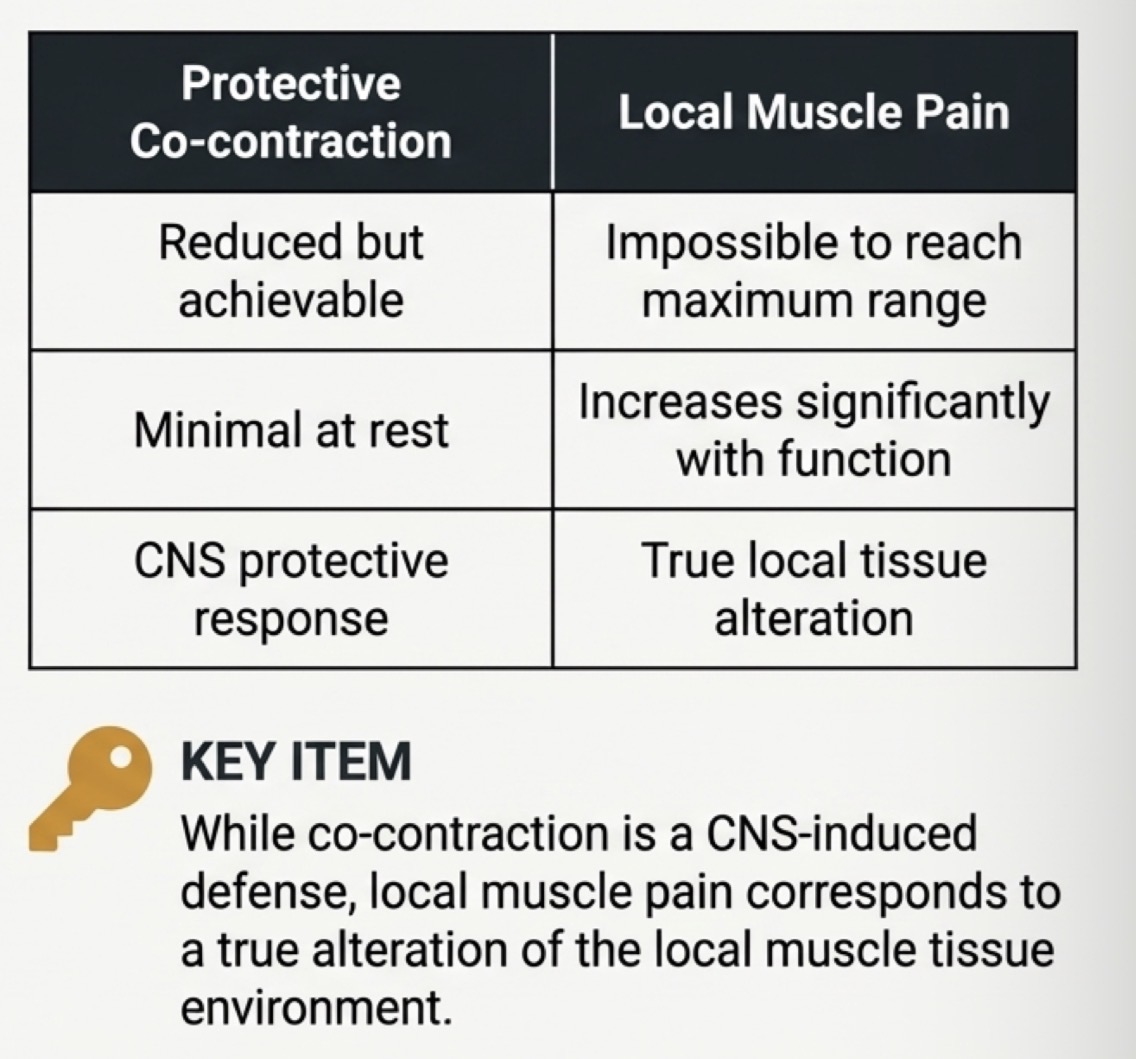
What is protective co contraction- etiology, when, causes, clinical signs
Initial physiological response (muscle splinting) to protect an injured part
Alteration of sensory stimulus, constant deep pain or acute increase in stress
Appears immediately after stimulus, persists for few days
Causes reduced range of motion, but can achieve MO
Minimal pain at rest but increases with function, muscle weakness
How do you treat protective co-contraction?
Must treat underlying cause- eliminate etiological factor
Restrict mandibular use to painless limits, soft diet
Short term analgesics (NSAIDs) if pain
NO vigorous physical exercise
What is local muscle pain- etiology, when, difference between protective co-contraction?
Primary non inflam pain- 1st response to unresolved co-contraction
Prolonged co contraction, local tissue trauma or chronic emotional stress
Delayed onset- hours or days after an event, injection or excessive MO
How do you treat local muscle pain?
Reduce sensory stimulus reaching CNS to break pain loop
Definitive- Muscle relaxation device (occlusal splint) at night if bruxism suspected
Painless range of motion- but not ABSOLUTE REST, soft diet, teeth apart, passive muscle stretching and massage
NSAIDs 5-7 days
What is myofascial pain- etiology, primary clinical sign, example, diagnosis?
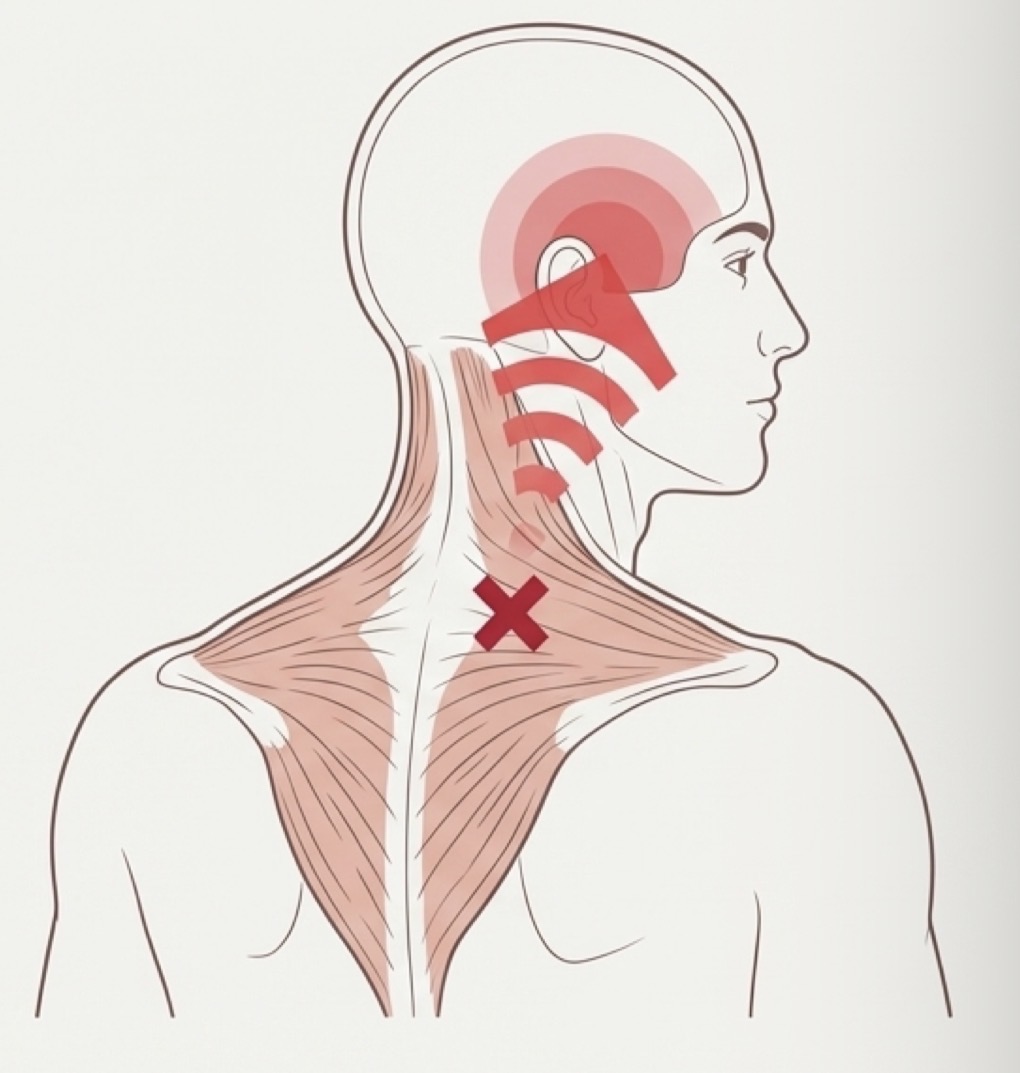
Regional myogenic disorder characterised by hard hypersensitive bands of muscle tissue (trigger points)
Constant deep pain, stress, disturbed sleep, poor posture, fatigue
Central excitatory effects that generate referred pain
E.g traps or neck pain referred upwards perceived as tension headache
Palpating taut muscle band immediately increases referred pain- must treat this not secondary symptom
How do you activate/treat trigger point?
Painless stretching, correct posture and sleep habits
1- spray and stretch- apply vapocoolant spray (fluoromethane) then stretch muscle to full length
2- pressure and massage- up to 9kg for 30-60sec
3- inject LA (1-2% lidocaine no VC) then stretch
STRETCH most important- spray and needle just prevent triggering a pain reflex
What is a myospasm- acute tonic contraction- etiology, when, causes, exam?
Involuntary CNS induced tonic muscle contraction
Continuous deep pain, severe muscle fatigue, metabolic imbalances
Sudden
Severe restriction of mandibular mobility- acute malocclusion
Feels hard, rigid, difficult to palpate- intense pain even at rest, it’s physiologically locked
How do you treat myospasms?
Pain reduction by deep manual massage with with cool spray or lidocaine injection
Passive stretch after calming pain- full length
Prioritise prevention with muscle rest and electrolyte restoration
If recurrent- Botox A injections- temp paralysis for 3-4 months
What is centrally mediated chronic myalgia- etiology, when, clinical sign, long term risk?
Continuous chronic muscle pain disorder
Prolonged presence of algogenic substances due to neurogenic inflammation
Constant primary pain from unresolved acute pain event
Limited opening, sever pain at rest and palpation
Muscle atrophy or myostatic contracture- longer it goes untreated, higher chance that CNS will develop neuroplasticity and fix pain chronically
How do you treat chronic myalgia?
Strict restriction- limited mandibular opening to minimum, severe soft diet, local moist heat
Caution when taking NSAIDS- ibuprofen 600mg x 4 daily x 2 weeks + use relaxation splint
Avoid local injections and early stretching exercises
What is fibromyalgia- clinical signs, coexist, dental protocol, adjunct drugs?
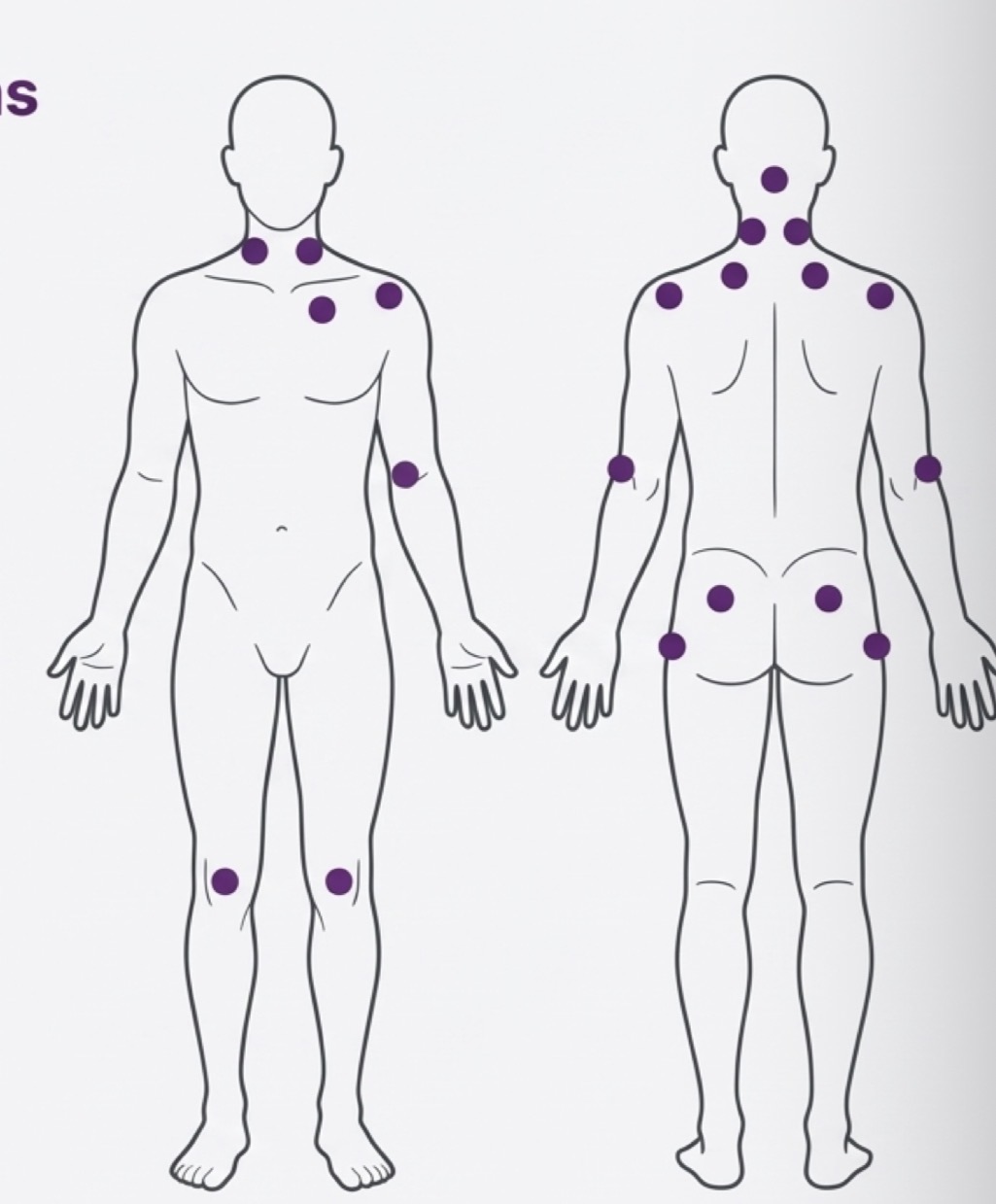
Systemic chronic musculoskeletal pain disorder
Generalised pain, severe fatigue, poor sleep- diagnosed when tenderness in 11-18 specific points
Coexist with chronic masticatory muscle pain
Conservative and palliative care
Low dose tricyclic antidepressants (Amitriptyline 10-50mg) to improve sleep
Refer to rheumatologist
Disuse sequelae will appear after resolving chronic disorders with prolonged immobilisation…what types?
Hypotrophic alterations- loss of strength and amass in elevator muscles
Myostatic contractures- painless shortening of og muscle strength
Rehab phase- introduce activity slowing only after all acute and inflam symptoms gone
Do gentle isometric mandibular exercise against resistance and controlled passive stretching